Gambling Problems and Alexithymia: A Systematic Review


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Search Strategy
2.2. Selection Criteria
2.3. Selection Procedure, Data Extraction and Data Management
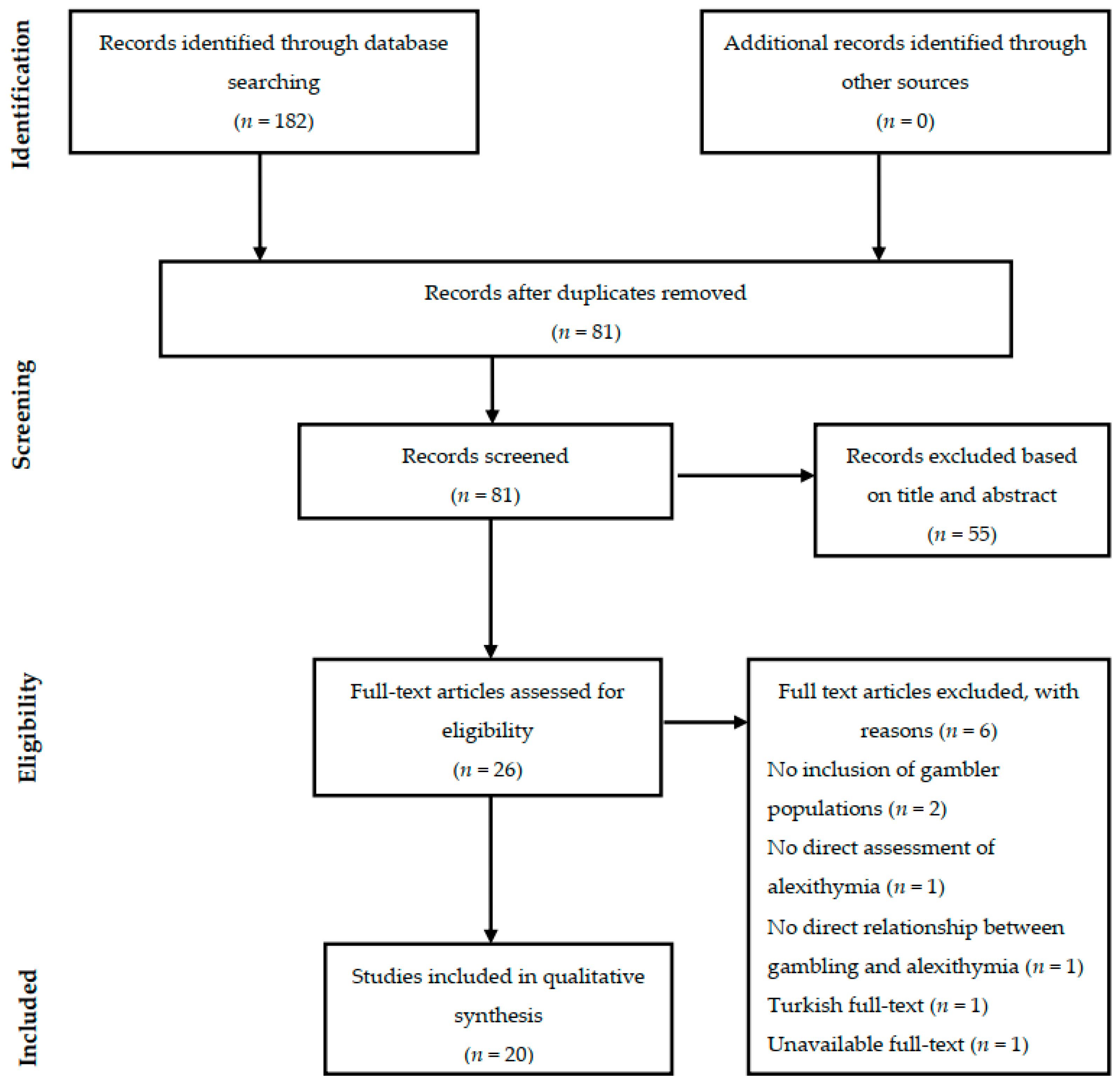
3. Results
3.1. Studies in Community Samples
3.2. Studies in Clinical Samples
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 3rd ed.; American Psychiatric Association: Washington, DC, USA, 1980. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Hodgins, D.C.; Stea, J.N.; Grant, J.E. Gambling disorders. Lancet 2011, 378, 1874–1884. [Google Scholar] [CrossRef]
- Petry, N.M.; Ginley, M.K.; Rash, C.J. A systematic review of treatments for problem gambling. Psychol. Addict. Behav. 2017, 31, 951–961. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, M.; Blaszczynski, A. The longitudinal relationships between psychiatric disorders and gambling disorders. Int. J. Ment. Health Addict. 2018, 16, 16–44. [Google Scholar] [CrossRef]
- Stucki, S.; Rihs-Middel, M. Prevalence of adult problem and pathological gambling between 2000 and 2005: An update. J. Gambl. Stud. 2007, 23, 245–257. [Google Scholar] [CrossRef] [PubMed]
- Dowling, N.; Merkouris, S.; Greenwood, C.; Oldenhof, E.; Toumbourou, J.; Youssef, G. Early risk and protective factors for problem gambling: A systematic review and meta-analysis of longitudinal studies. Clin. Psychol. Rev. 2017, 51, 109–124. [Google Scholar] [CrossRef] [PubMed]
- Johansson, A.; Grant, J.E.; Kim, S.; Odlang, B.L.; Götestam, K.G. Risk factors for problematic gambling: A critical literature review. J. Gambl. Stud. 2009, 25, 67–92. [Google Scholar] [CrossRef]
- Marchetti, D.; Whelan, J.P.; Verrocchio, M.C.; Ginley, M.K.; Fulcheri, M.; Relyea, G.E.; Meyers, A.W. Psychometric evaluation of the Italian translation of the gamblers’ beliefs questionnaire. Int. Gambl. Stud. 2016, 16, 17–30. [Google Scholar] [CrossRef]
- Olsen, V.V.; Lugo, R.G.; Sutterlin, S. The somatic marker theory in the context of addiction: Contributions to understanding development and maintenance. Psychol. Res. Behav. Manag. 2015, 8, 187–200. [Google Scholar] [CrossRef]
- Taylor, G.J.; Bagby, R.M.; Parker, J.D.A. Disorders of Affect Regulation: Alexithymia in Medical and Psychiatric Illness; Cambridge University Press: Cambridge, UK, 1997. [Google Scholar]
- Luminet, O.; Taylor, G.J.; Bagby, R.M. Alexithymia. Advances in Research, Theory, and Clinical Practice; Cambridge University Press: Cambridge, UK, 2018. [Google Scholar]
- Bucci, W. Symptoms and symbols. A multiple code theory of somatization. Psychoanal. Inq. 1997, 17, 151–172. [Google Scholar] [CrossRef]
- Fonagy, P.; Gergely, G.; Jurist, E.L.; Target, M. Affect Regulation, Mentalization and the Development of the Self; Other Press: New York, NY, USA, 2002. [Google Scholar]
- Parker, J.D.A.; Taylor, G.J.; Bagby, R.M. The relationship between emotional intelligence and alexithymia. Personal. Individ. Differ. 2001, 30, 107–115. [Google Scholar] [CrossRef]
- Goerlich, K.S.; Aleman, A. Neuroimaging studies of alexithymia. In Alexithymia: Advances in Research, Theory, and Clinical Practice; Luminet, O., Bagby, R.M., Taylor, G.J., Eds.; Cambridge University Press: Cambridge, UK, 2018; pp. 207–249. [Google Scholar]
- Porcelli, P.; Taylor, G.J. Alexithymia and Physical Illness: A Psychosomatic Approach. In Alexithymia: Advances in Research, Theory, and Clinical Practice; Luminet, O., Bagby, R.M., Taylor, G.J., Eds.; Cambridge University Press: Cambridge, UK, 2018; pp. 105–126. [Google Scholar]
- Lumley, M.A.; Neely, L.C.; Burger, A.J. The assessment of alexithymia in medical settings: Implications for understanding and treating health problems. J. Personal. Assess. 2007, 89, 230–246. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Cosenza, M.; Baldassarre, I.; Matarazzo, O.; Nigro, G. Youth at stake: Alexithymia, cognitive distortions, and problem gambling in late adolescents. Cogn. Comput. 2014, 6, 652–660. [Google Scholar] [CrossRef]
- Noël, X.; Saeremans, M.; Kornreich, C.; Bechara, A.; Jaafari, N.; Fantini-Hauwel, C. On the processes underlying the relationship between alexithymia and gambling severity. J. Gambl. Stud. 2018, 34, 1049–1066. [Google Scholar] [CrossRef]
- Sekely, A.; Bagby, R.M.; Porcelli, P. Assessment of the alexithymia construct. In Alexithymia: Advances in Research, Theory, and Clinical Practice; Luminet, O., Bagby, R.M., Taylor, G.J., Eds.; Cambridge University Press: Cambridge, UK, 2018; pp. 17–32. [Google Scholar]
- Aïte, A.; Barrault, S.; Cassotti, M.; Borst, G.; Bonnaire, C.; Houdé, O.; Varescon, I.; Moutier, S. The impact of alexithymia on pathological gamblers’ decision making: A preliminary study of gamblers recruited in “sportsbook” casinos. Cogn. Behav. Neurol. 2014, 27, 59–67. [Google Scholar] [CrossRef]
- Bonnaire, C.; Bungener, C.; Varescon, I. Subtypes of french pathological gamblers: Comparison of sensation seeking, alexithymia and depression scores. J. Gambl. Stud. 2009, 25, 455–471. [Google Scholar] [CrossRef]
- Bonnaire, C.; Varescon, I.; Bungener, C. Slot machine gamblers in a french population: Study of depression, alexithymia and sensation seeking [Joueurs de machines à sous dans une population française: Étude de la dépression, de l’alexithymie et de la recherche de sensations]. Ann. Med. Psychol. 2010, 168, 350–356. [Google Scholar] [CrossRef]
- Bonnaire, C.; Bungener, C.; Varescon, I. Alexithymia and gambling: A risk factor for all gamblers? J. Gambl. Stud. 2013, 29, 83–96. [Google Scholar] [CrossRef]
- Bonnaire, C.; Barrault, S.; Aïte, A.; Cassotti, M.; Moutier, S.; Varescon, I. Relationship between pathological gambling, alexithymia, and gambling type. Am. J. Addict. 2017, 26, 152–160. [Google Scholar] [CrossRef]
- Di Nicola, M.; Ferri, V.R.; Moccia, L.; Panaccione, I.; Strangio, A.M.; Tedeschi, D.; Grandinetti, P.M.; Callea, A.; De-Giorgio, F.; Martinotti, G.; et al. Gender differences and psychopathological features associated with addictive behaviors in adolescents. Front. Psychiatry 2017, 8, 256. [Google Scholar] [CrossRef]
- Di Trani, M.; Renzi, A.; Vari, C.; Zavattini, G.C.; Solano, L. Gambling disorder and affect regulation: The role of alexithymia and attachment style. J. Gambl. Stud. 2017, 33, 649–659. [Google Scholar] [CrossRef]
- Gori, A.; Craparo, G.; Caretti, V.; Giannini, M.; Iraci-Sareri, G.; Bruschi, A.; Janiri, L.; Ponti, L.; Tani, F. Impulsivity, alexithymia and dissociation among pathological gamblers in different therapeutic settings: A multisample comparison study. Psychiatry Res. 2016, 246, 789–795. [Google Scholar] [CrossRef]
- Grall-Bronnec, M.; Bouju, G.; Landréat-Guillou, M.; Vénisse, J.L. Socio-demographic and clinical assessment, and trajectory of a sample of french pathological gamblers. [Évaluation sociodémographique, clinique et du parcours de jeu d’un échantillon de joueurs pathologiques franais]. Encephale 2010, 36, 452–460. [Google Scholar] [CrossRef]
- Lumley, M.A.; Roby, K.J. Alexithymia and pathological gambling. Psychother. Psychosom. 1995, 63, 201–206. [Google Scholar] [CrossRef]
- Maniaci, G.; Picone, F.; Dimarco, T.; Lipari, A.; Brancato, A.; Cannizzaro, C. Psychodiagnostic assessment of pathological gamblers: A focus on personality disorders, clinical syndromes and alexithymia. Int. J. Ment. Health Addict. 2015, 13, 728–739. [Google Scholar] [CrossRef]
- Maniaci, G.; Picone, F.; van Holst, R.J.; Bolloni, C.; Scardina, S.; Cannizzaro, C. Alterations in the emotional regulation process in gambling addiction: The role of anger and alexithymia. J. Gambl. Stud. 2017, 33, 633–647. [Google Scholar] [CrossRef]
- Montel, S.; Ducroz, E.; Davidson, C. Impulsivity and internet gambling: What is the link? A preliminary study. Addict. Disord. Treat. 2014, 13, 190–198. [Google Scholar] [CrossRef]
- Parker, J.D.A.; Wood, L.M.; Bond, B.J.; Shaughnessy, P. Alexithymia in young adulthood: A risk factor for pathological gambling. Psychother. Psychosom. 2005, 74, 51–55. [Google Scholar] [CrossRef]
- Toplak, M.E.; Liu, E.; Macpherson, R.; Toneatto, T.; Stanovich, K.E. The reasoning skills and thinking dispositions of problem gamblers: A dual-process taxonomy. J. Behav. Decis. Mak. 2007, 20, 103–124. [Google Scholar] [CrossRef]
- Mitrovic, D.V.; Brown, J. Poker mania and problem gambling: A study of distorted cognitions, motivation and alexithymia. J. Gambl. Stud. 2009, 25, 489–502. [Google Scholar] [CrossRef]
- Bibby, P.A.; Ross, K.E. Alexithymia predicts loss chasing for people at risk for problem gambling. J. Behav. Addict. 2017, 6, 630–638. [Google Scholar] [CrossRef]
- Toneatto, T.; Lecce, J.; Bagby, M. Alexithymia and pathological gambling. J. Addict. Dis. 2009, 28, 193–198. [Google Scholar] [CrossRef]
- Dorard, G.; Berthoz, S.; Haviland, M.G.; Phan, O.; Corcos, M.; Bungener, C. Multimethod alexithymia assessment in adolescents and young adults with a cannabis use disorder. Compr. Psychiatry 2008, 49, 585–592. [Google Scholar] [CrossRef]
- Thorberg, F.A.; Young, R.M.; Sullivan, K.A.; Lyvers, M. Alexithymia and alcohol use disorders: A critical review. Addict. Behav. 2009, 34, 237–245. [Google Scholar] [CrossRef]
- Scimeca, G.; Bruno, A.; Cava, L.; Pandolfo, G.; Muscatello, M.R.A.; Zoccali, R. The relationship between alexithymia, anxiety, depression and internet addiction severity in a sample of Italian school students. Sci. World J. 2014, 2014, 504376. [Google Scholar] [CrossRef]
- Rose, P.; Segrist, D.J. Difficulty identifying feelings, distress tolerance and compulsive buying: Analyzing the associations to inform therapeutic strategies. Int. J. Ment. Health Addict. 2012, 10, 927–935. [Google Scholar] [CrossRef]
- Sutherland, M.T.; Carroll, A.J.; Salmeron, B.J.; Ross, T.J.; Stein, E.A. Insula’s functional connectivity with ventromedial prefrontal cortex mediates the impact of trait alexithymia on state tobacco craving. Psychopharmacology 2013, 228, 143–155. [Google Scholar] [CrossRef]
- Thorberg, F.A.; Young, R.M.; Sullivan, K.A.; Lyyers, M.; Connor, J.P.; Freeney, G.F. Alexithymia, craving and attachment in a heavy drinking population. Addict. Behav. 2011, 36, 427–430. [Google Scholar] [CrossRef][Green Version]
- Saladin, M.E.; Santa Ana, E.J.; LaRowe, S.D.; Simpson, A.N.; Tolliver, B.K.; Price, K.L.; McRae-Clark, A.L.; Brady, K.T. Does alexithymia explain variation in cue-elicited craving reported by methamphetamine-dependent individuals? Am. J. Addict. 2012, 21, 130–135. [Google Scholar] [CrossRef]
- Morie, K.P.; Ridout, N. Alexithymia and Maladaptive Regulatory Behaviors in Substance Use Disorders and Eating Disorders. In Alexithymia: Advances in Research, Theory, and Clinical Practice; Luminet, O., Bagby, R.M., Taylor, G.J., Eds.; Cambridge University Press: Cambridge, UK, 2018; pp. 158–173. [Google Scholar]
- Woodman, T.; Huggins, M.; Le Scanff, C.; Cazenave, N. Alexithymia determines the anxiety experienced in skydiving. J. Affect. Disord. 2009, 116, 134–138. [Google Scholar] [CrossRef]
- Lesieur, H.R. Cluster analysis of types of inpatient pathological gamblers. Diss. Abstr. Int. Sect. B Sci. Eng. 2001, 62, 2065. [Google Scholar]
- Blaszczynski, A.; Nower, L. A pathways model of problem and pathological gambling. Addiction 2002, 97, 487–499. [Google Scholar] [CrossRef]
- Ledgerwood, D.M.; Petry, N.M. Subtyping pathological gamblers based on impulsivity, depression, and anxiety. Psychol. Addict. Behav. 2010, 24, 680–688. [Google Scholar] [CrossRef]
- Ogrodniczuk, J.S.; Kealy, D.; Hadjinpsvlou, G.A.; Cameron, K. Therapeutic Issues. In Alexithymia: Advances in Research, Theory, and Clinical Practice; Luminet, O., Bagby, R.M., Taylor, G.J., Eds.; Cambridge University Press: Cambridge, UK, 2018; pp. 190–206. [Google Scholar]
- Rogier, G.; Velotti, P. Conceptualizing gambling disorder with the process model of emotion regulation. J. Behav. Addict. 2018, 7, 239–251. [Google Scholar] [CrossRef]


{kind=link}
| Authors | Country | Study Design | Sample | Assessment of Gambling | Assessment of Alexithymia | Other Relevant Variables | Main Results |
|---|---|---|---|---|---|---|---|
| Lumley and Roby (1995) [32] | USA | Cross-sectional |
| - SOGS | TAS-26 |
|
|
| Parker et al. (2005) [36] | Canada | Cross-sectional |
| - SOGS | TAS-20 | - Mood | - Between-group comparisons showed that PG subjects scored significantly higher on the TAS total as well as DDF and EOT than HC, either unadjusted or after controlling for mood scores. |
| Toplak et al. (2007) [37] | Canada | Cross-sectional |
|
| TAS-20 | - Cognitive ability | - PG subjects scored higher to the TAS than HC (F(2, 104) = 11.03, p < 0.001), even after controlling for age and cognitive ability (F(2, 104) = 7.61, p < 0.001). TAS-20 accounted for the most unique variance of gambling behavior (R2 Change = 0.104, F = 15.53, p < 0.001) in hierarchical regression, after age and cognitive ability were partialled out. |
| Toneatto et al. (2009) [40] | Canada | Cross-sectional |
| - DSM-IV criteria | TAS-20 |
|
|
| Mitrovic and Brown (2009) [38] | Australia | Cross-sectional |
| - CPGI | TAS-20 |
|
|
| Bonnaire et al. (2010) [25] | France | Cross-sectional |
|
| TAS-20 |
| - The prevalence of alexithymia was significantly higher among participants classified as PG (44%) than RG (28%) and NRG (5%) (χ2 = 13.2, p < 0.001). |
| Bonnaire et al. (2013) [26] | France | Cross-sectional |
|
| TAS-20 |
|
|
| Cosenza et al. (2014) [20] | Italy | Cross-sectional |
| - SOGS-RA | TAS-20 | - Gambling-related cognitions |
|
| Aïte et al. (2014) [23] | France | Cross-sectional |
|
| TAS-20 |
|
|
| Montel et al. (2014) [35] | France | Cross-sectional |
| - SOGS | TAS-20 | - No significant differences were found on alexithymia scores between online PG, PrG, and HC. | |
| Bibby and Ross (2017) [39] | United Kingdom | Cross-sectional |
| - PGSI | TAS-20 | - Loss-chasing behavior |
|
| Di Nicola et al. (2017) [28] | Italy | Cross-sectional |
| - SOGS-RA | TAS-20 |
| - No association was found between gambling problems and alexithymia when impulsivity, anhedonia, and dissociation variables were controlled for. |
| Bonnaire et al. (2017) [27] | France | Cross-sectional |
|
| TAS-20 |
|
|
| Noël et al. (2018) [21] | Belgium | Cross-sectional |
| - CPGI | TAS-20 |
| - Alexithymia was a significant predictor of gambling severity and its effect was fully mediated by distress and impulsivity (indirect effect: β = 0.29; 95% bootstrap CI = 0.13, 0.44). |
| Authors | Country | Study Design | Sample | Assessment of Gambling | Assessment of Alexithymia | Other Relevant Variables | Main Results |
|---|---|---|---|---|---|---|---|
| Bonnaire et al. (2009) [24] | France | Cross-sectional |
|
| TAS-20 |
|
|
| Grall-Bronnec et al. (2010) [31] | France | Cross-sectional |
|
| TAS-20 | - Two third of participants (66.7%) scored in the alexithymia range (TAS-20 > 56). | |
| Maniaci et al. (2015) [33] | Italy | Cross-sectional, case-control study |
| - SOGS | TAS-20 |
|
|
| Gori et al. (2016) [30] | Italy | Cross-sectional, case-control study |
| - SOGS | TAS-20 |
|
|
| Maniaci et al. (2017) [34] | Italy | Cross-sectional, case-control study |
| - SOGS | TAS-20 | - Anger expression |
|
| Di Trani et al. (2017) [29] | Italy | Cross-sectional |
|
| TAS-20 | - Attachment style |
|
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marchetti, D.; Verrocchio, M.C.; Porcelli, P. Gambling Problems and Alexithymia: A Systematic Review. Brain Sci. 2019, 9, 191. https://doi.org/10.3390/brainsci9080191
Marchetti D, Verrocchio MC, Porcelli P. Gambling Problems and Alexithymia: A Systematic Review. Brain Sciences. 2019; 9(8):191. https://doi.org/10.3390/brainsci9080191
Chicago/Turabian StyleMarchetti, Daniela, Maria Cristina Verrocchio, and Piero Porcelli. 2019. "Gambling Problems and Alexithymia: A Systematic Review" Brain Sciences 9, no. 8: 191. https://doi.org/10.3390/brainsci9080191
APA StyleMarchetti, D., Verrocchio, M. C., & Porcelli, P. (2019). Gambling Problems and Alexithymia: A Systematic Review. Brain Sciences, 9(8), 191. https://doi.org/10.3390/brainsci9080191