

Effects of Probiotic Supplementation on Depressive Symptoms, Sleep Quality, and Modulation of Gut Microbiota and Inflammatory Biomarkers: A Randomized Controlled Trial


Abstract
1. Introduction
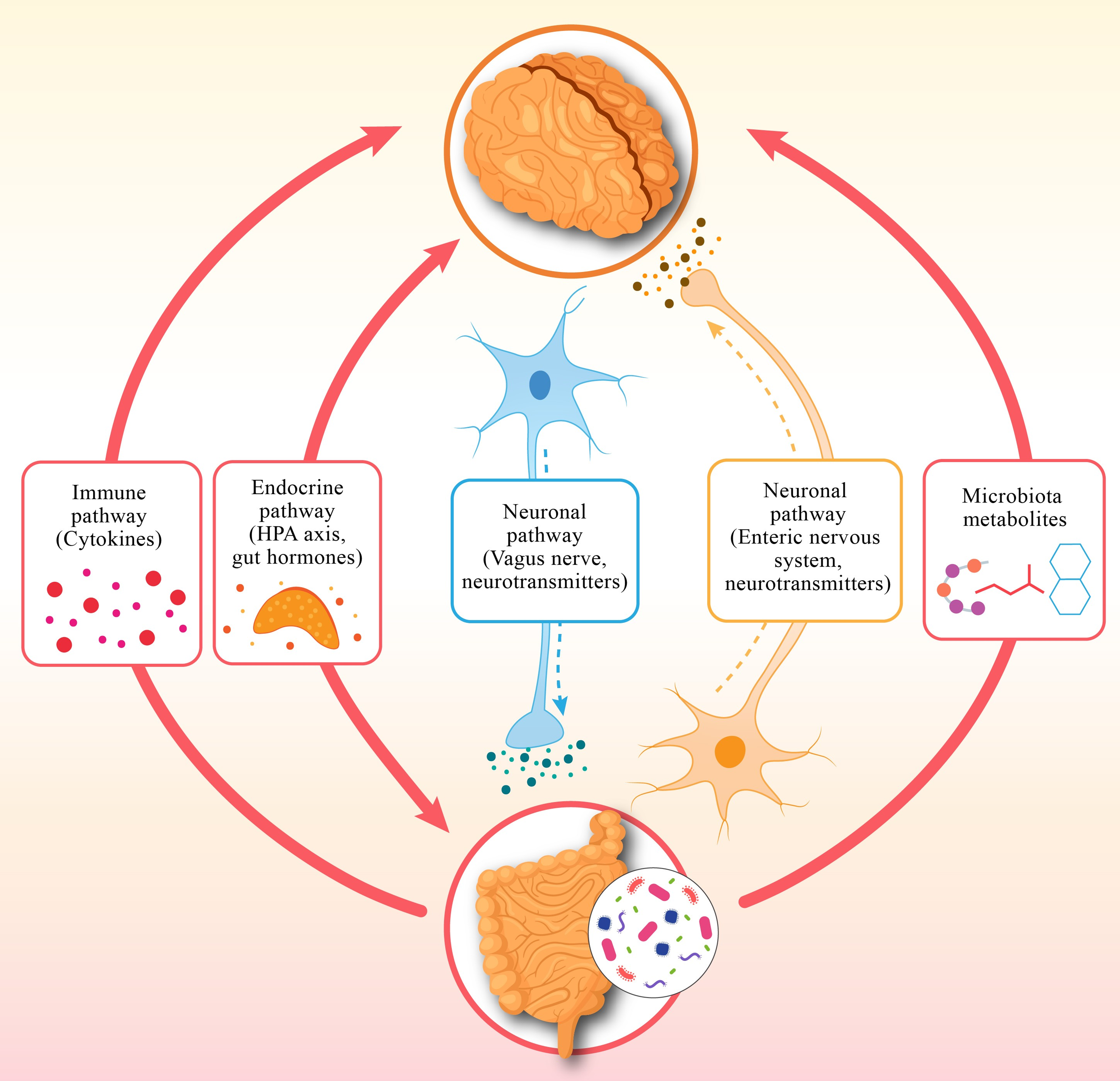
1.1. The Gut Microbiome: A Crucial Factor in Mental Well-Being
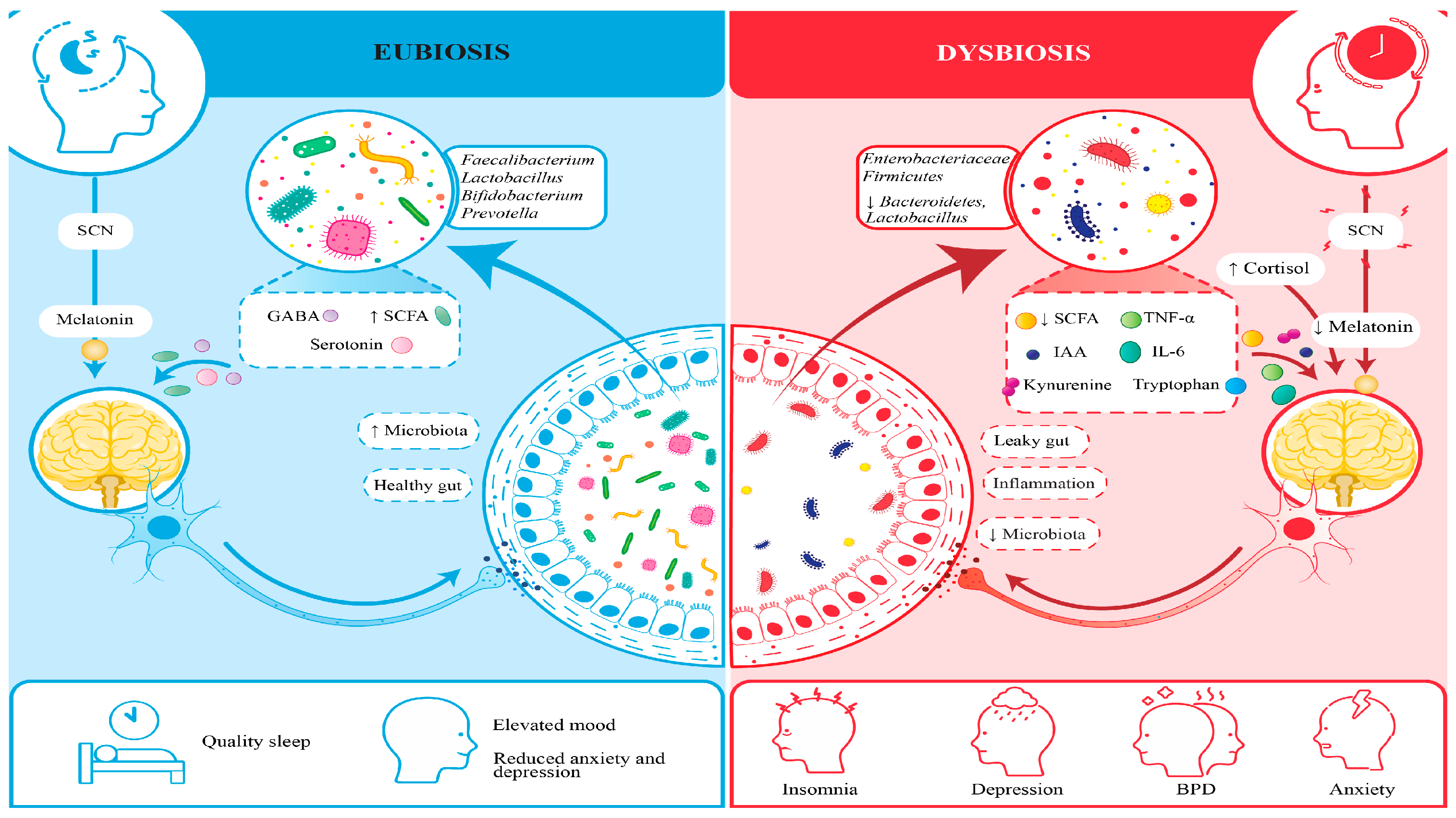
1.2. Circadian Rhythms and Their Role in Health
1.3. Sleep: A Vital Element of the Gut–Sleep–Brain Axis
1.4. The Interconnection Between the Gut Microbiome, Circadian Rhythms, and Sleep
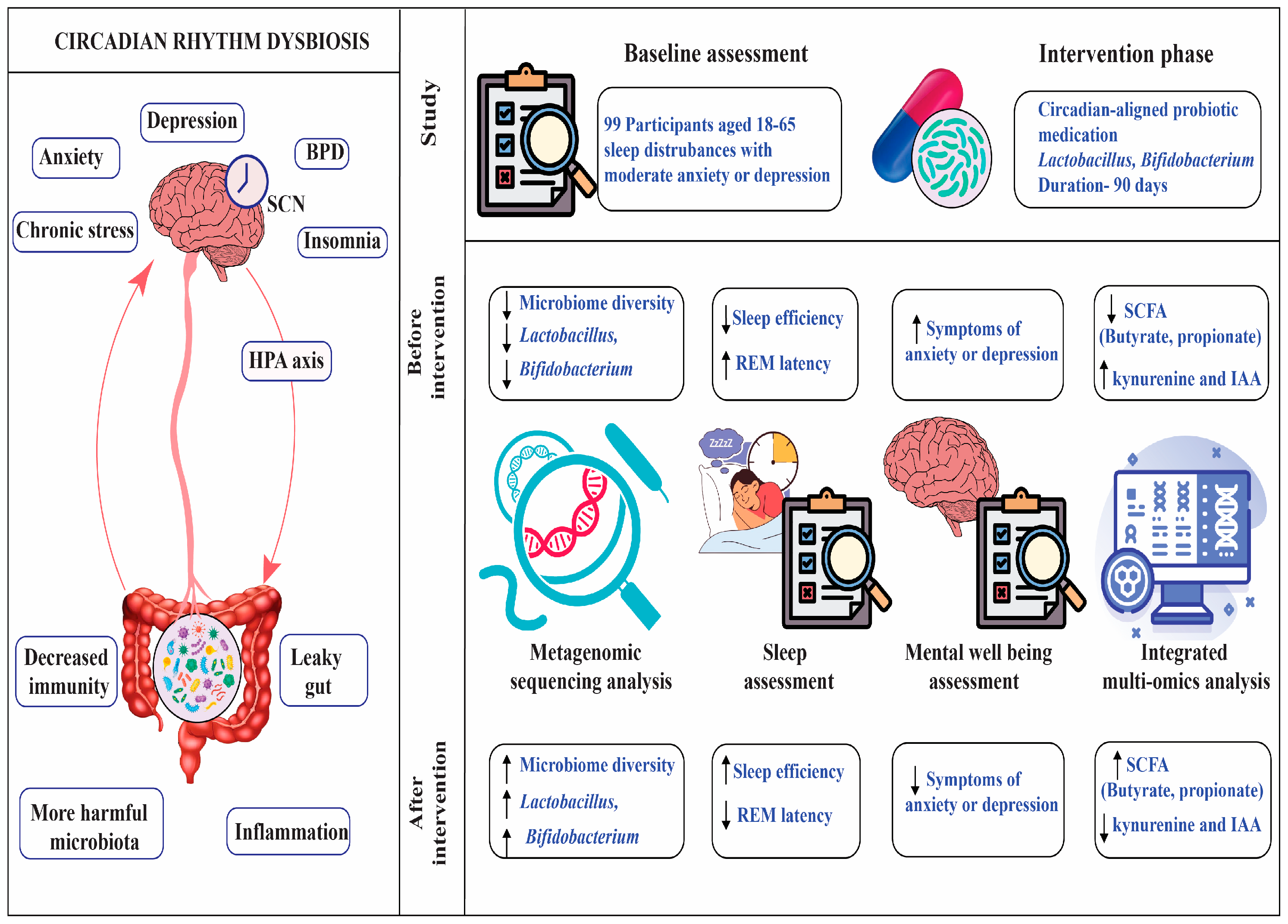
2. Materials and Methods
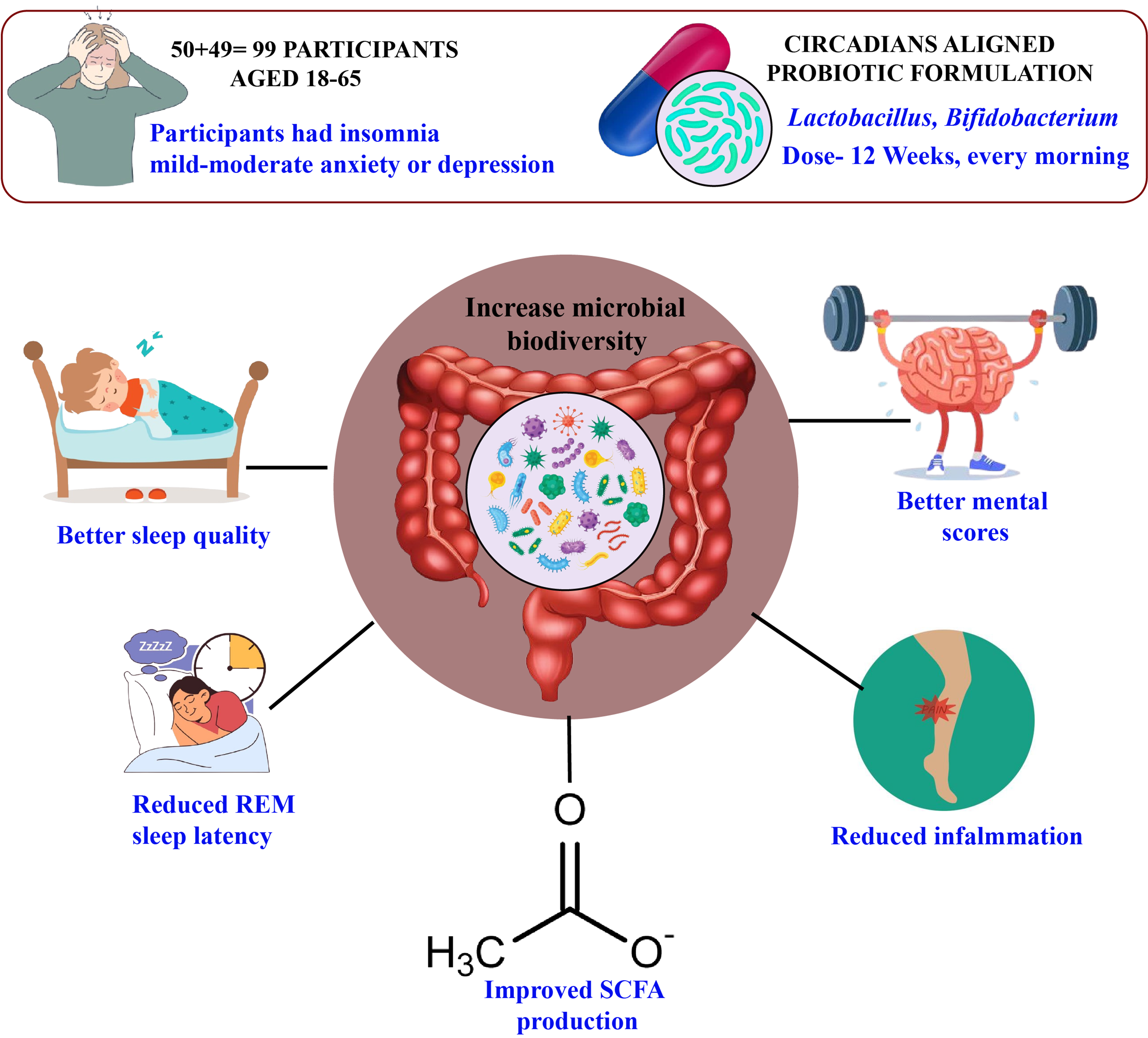
2.1. Participants
Participants Were Randomized into Two Groups
2.2. Experimetnal Procedure
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Intervention Details
2.5.1. Administration
2.5.2. Randomization
2.6. Study Design
2.6.1. Study Timeline and Stool Sample Collection
Pre-Interventional Period (Baseline)
Interventional Period
Post-Intervention Period
2.7. Sleep and Mental Health Assessment
2.7.1. Sleep Assessments
Subjective Measures
2.7.2. Mental Health Assessments
2.7.3. Polysomnography (PSG)
- ❖
- Avoid caffeine, alcohol, nicotine, and recreational drugs for 48 h prior to each session.
- ❖
- Refrain from strenuous physical exercise and naps for 24 h before PSG.
- ❖
- Maintain a consistent sleep–wake schedule (within ±1 h) for 7 days prior, verified via sleep diaries and actigraphy.
- ❖
- Consume a standardized light meal (500–600 kcal, low in sugar and fat) at least 4 h before PSG to minimize gastrointestinal interference with sleep.
Scoring
- ❖
- Sleep Stages: Wake, N1 (light sleep), N2 (light sleep with spindles/K-complexes), N3 (slow-wave sleep), and REM (rapid eye movement sleep), based on EEG, EOG, and EMG patterns.
- ❖
- Respiratory Events: Apneas (cessation of airflow ≥10 s), hypopneas (≥30% airflow reduction with ≥3% oxygen desaturation or arousal), and respiratory effort-related arousals (RERAs).
- ❖
- Arousals: Abrupt EEG frequency shifts (≥3 s) in alpha, theta, or higher frequencies, accompanied by EMG activation in REM sleep.
- ❖
- Periodic Limb Movements: Repetitive leg EMG bursts (0.5–10 s, ≥4 in a 90 s period).
2.7.4. Actigraphy
Data Collection and Metrics
- ❖
- Total Sleep Time (TST): Total minutes classified as sleep within the sleep period (from sleep onset to final awakening), excluding periods of wakefulness.
- ❖
- Sleep Onset Latency (SOL): Time (minutes) from the event-marked lights-off to the first epoch classified as sleep, based on reduced movement and heart rate.
- ❖
- Sleep Efficiency (SE): Percentage of TST divided by the time in bed (TIB, from lights-off to lights-on), calculated as SE = (TST/TIB) × 100.
- ❖
- Wake After Sleep Onset (WASO): Total minutes classified as wake after sleep onset, reflecting sleep fragmentation.
- ❖
- Circadian Rhythm Amplitude: The difference between peak and trough activity levels within a 24 h period, derived from cosinor analysis to quantify circadian rhythm strength.
- ❖
- Sleep Midpoint: The midpoint of the sleep period (e.g., 3:00 AM for a 11:00 PM–7:00 AM sleep window), used to assess circadian phase stability.
- ❖
- Sleep Diaries: Completed daily for one week at each assessment point.
- ❖
- Questionnaires (PSQI, ESS): Administered at baseline, midpoint (week 6), and post-intervention.
2.7.5. Mental Health Assessments
HDRS, GAD-7, PHQ-9
2.8. Data Analysis
- ❖
- Statistical Tests: Mixed-effects ANOVA and paired t-tests compared pre- and post-intervention differences in sleep (PSG, actigraphy), mental health (BDI-II, PHQ-9, GAD-7), and microbiome metrics (Shannon index, SCFAs) between groups. Regression models assessed associations between microbial changes, sleep, and psychiatric symptoms, adjusting for age, sex, and city.
- ❖
- Bioinformatics: QIIME2, Mothur, and HUMAnN2 analyzed 16S rRNA sequencing (alpha diversity: Shannon index; beta diversity: Bray–Curtis dissimilarity) and LC–MS metabolomics (SCFAs, tryptophan derivatives). Alpha diversity compared probiotic vs. placebo groups, and beta diversity assessed microbial shifts post-intervention.
- ❖
- Machine Learning: Random Forest and Support Vector Machine (SVM) models identified microbial biomarkers predictive of sleep and mental health outcomes, trained with 5-fold cross-validation. Performance was evaluated via AUC (target >0.70), with feature importance ranked by mean decrease in accuracy.
- ❖
- Missing Data: Missing data (<10% of records, e.g., incomplete diaries, failed PSG) were handled using multiple imputation by chained equations (MICE) in R, with sensitivity analyses excluding imputed data to assess bias.
2.9. Validated Psychiatric Tools for Evaluating Participants’ Mental Health
3. Results
3.1. Gut Microbiome and Circadian Disruption Correlation
3.2. Gut Microbiome Dysbiosis and Sleep Structure
3.3. Influence of Microbial Metabolites on Mental Well-Being
3.4. Probiotic Supplementation Aligned with Circadian Rhythms
3.5. Post-Intervention Microbiome Changes
3.6. Two-Way Interactions Among Circadian Cycles, Gut Microbiome, and Psychological Well-Being
3.7. Predictive Value of Microbial Metabolites for Mental Health Outcomes
3.7.1. Predictive Value
3.7.2. Butyrate (AUC = 0.82, p = 0.005 for Depression)
3.7.3. Kynurenine (AUC = 0.84, p = 0.007 for Anxiety)
3.7.4. Key Points About Predictive Value
Biomarker Potential
Statistical Significance
Clinical Implications
Simplified Analogy
4. Discussion
Limitation of the Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Besedovsky, L.; Lange, T.; Born, J. Sleep and immune function. Pflüg. Arch.-Eur. J. Physiol. 2019, 471, 387–397. [Google Scholar] [CrossRef] [PubMed]
- Silva, Y.P.; Bernardi, A.; Frozza, R.L. The role of short-chain fatty acids from gut microbiota in gut-brain communication. Front. Endocrinol. 2020, 11, 25. [Google Scholar] [CrossRef] [PubMed]
- Milosavljevic, T.; Ghelfi, F.; Sinagra, G.; Bano, G. The Microbiota–Gut–Brain Axis in Metabolic Syndrome and Sleep Disorders: A Systematic Review. Nutrients 2024, 16, 390. [Google Scholar]
- Smith, L.; Jacob, L.; Yakkundi, A.; McDermott, D.; Armstrong, N.C.; Barnett, Y.; López-Sánchez, G.F.; Martin, S.; Butler, L.; Tully, M.A. Correlates of symptoms of anxiety and depression and mental wellbeing associated with COVID-19: A cross-sectional study of UK-based respondents. Psychiatry Res. 2020, 291, 113138. [Google Scholar] [CrossRef]
- Yano, J.M.; Yu, K.; Donaldson, G.P.; Shastri, G.G.; Ann, P.; Ma, L.; Nagler, C.R.; Ismagilov, R.F.; Mazmanian, S.K.; Hsiao, E.Y. Indigenous bacteria from the gut microbiota regulate host serotonin biosynthesis. Cell 2015, 161, 264–276. [Google Scholar] [CrossRef]
- Chen, X.; Yang, C.; Zhang, L. Probiotics and Circadian Rhythm: Potential for Improving Sleep and Mood Disorders. Nutrients 2025, 17, 234. [Google Scholar]
- Voigt, R.M.; Forsyth, C.B.; Green, S.J.; Mutlu, E.; Keshavarzian, A. Circadian rhythm and the gut microbiome. Int. Rev. Neurobiol. 2016, 131, 193–205. [Google Scholar] [CrossRef]
- Liang, X.; FitzGerald, G.A. Chronobiology and the Microbiome: Implications for Mental Health. Biology 2023, 12, 612. [Google Scholar]
- Rogers, G.B.; Keating, D.J.; Young, R.L.; Wong, M.L.; Licinio, J.; Wesselingh, S. From gut dysbiosis to altered brain function and mental illness: Mechanisms and pathways. Mol. Psychiatry 2016, 21, 738–748. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Koh, A.; De Vadder, F.; Kovatcheva-Datchary, P.; Bäckhed, F. From dietary fiber to host physiology: Short-chain fatty acids as key bacterial metabolites. Cell 2016, 165, 1332–1345. [Google Scholar] [CrossRef]
- Anderson, J.R.; Carroll, I.; Azcarate-Peril, M.A.; Rochette, A.D.; Heinberg, L.J.; Peat, C.; Kennedy, A.; Gunstad, J. A preliminary examination of gut microbiota, sleep, and cognitive flexibility in healthy older adults. Sleep Med. 2017, 38, 104–107. [Google Scholar] [CrossRef] [PubMed]
- Benedict, C.; Vogel, H.; Jonas, W.; Woting, A.; Blaut, M.; Schürmann, A.; Cedernaes, J. Gut microbiota and sleep-wake regulation. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 571–576. [Google Scholar] [CrossRef]
- Arendt, J. Melatonin and human rhythms. Chronobiol. Int. 2019, 36, 189–210. [Google Scholar] [CrossRef]
- Aylwin, C.F.; Lomniczi, A. Circadian misalignment and metabolic disorders: From mechanisms to treatments. Curr. Opin. Endocr. Metab. Res. 2020, 13, 41–47. [Google Scholar] [CrossRef]
- Huang, R.; Wang, K.; Hu, J. Circadian Disruption and Gut Dysbiosis: A Pathway to Mental Health Disorders. Biology 2025, 13, 345. [Google Scholar]
- Wulff, K.; Gatti, S.; Wettstein, J.G.; Foster, R.G. Sleep and circadian rhythm disruption in psychiatric and neurodegenerative disease. Nat. Rev. Neurosci. 2010, 11, 589–599. [Google Scholar] [CrossRef] [PubMed]
- Berry, R.; Quan, S.; Abreu, A. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications; Version 2.6; American Academy of Sleep Medicine: Darien, GA, USA, 2020. [Google Scholar]
- Zee, P.C.; Turek, F.W. Sleep, circadian rhythms, and health: A new frontier in medicine. Sleep Med. Clin. 2021, 16, 203–215. [Google Scholar] [CrossRef]
- Boivin, D.B.; Boudreau, P.; Kosmadopoulos, A. Disturbance of the Circadian System in Shift Work and Its Health Impact. J. Biol. Rhythms 2022, 37, 3–28. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhou, L.; Kang, L.; Xiao, X.; Jia, L.; Zhang, Q.; Deng, M. "Gut Microbiota-Circadian Clock Axis" in Deciphering the Mechanism Linking Early-Life Nutritional Environment and Abnormal Glucose Metabolism. Int. J. Endocrinol. 2019, 2019, 5893028. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ting, E.Y.; Yang, A.C.; Tsai, S.J. Role of Interleukin-6 in Depressive Disorder. Int. J. Mol. Sci. 2020, 21, 2194. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Miller, A.H.; Maletic, V.; Raison, C.L. Inflammation and its discontents: The role of cytokines in the pathophysiology of major depression. Biol. Psychiatry 2009, 65, 732–741. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cho, H.J.; Eisenberger, N.I.; Olmstead, R.; Breen, E.C.; Irwin, M.R. Preexisting mild sleep disturbance as a vulnerability factor for inflammation-induced depressed mood: A human experimental study. Transl. Psychiatry 2016, 6, e750. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, C.N.; Sammer, G.; Neumann, E.; Blecker, C.; Gründer, G.; Adolphi, H.; Pedraz-Petrozzi, B. Functional resting state connectivity is differentially associated with IL-6 and TNF-α in depression and in healthy controls. Sci. Rep. 2025, 15, 1769. [Google Scholar] [CrossRef]
- Brymer, K.J.; Romay-Tallon, R.; Allen, J.; Caruncho, H.J.; Kalynchuk, L.E. Exploring the Potential Antidepressant Mechanisms of TNF_ Antagonists. Front. Neurosci. 2019, 13, 98. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Q | Participants (n) | Intervention Content | Dosage/Day | Duration | Compliance Checks |
|---|---|---|---|---|---|
| Probiotic | 50 | L. rhamnosus GG + B. longum | 15B CFU | 12 weeks | Capsule counts + weekly telehealth |
| Placebo | 49 | Maltodextrin (matched appearance) | N/A | 12 weeks | Capsule counts + weekly telehealth |
| Taxonomic Level | Circadian Misalignment (%) | p-Value |
|---|---|---|
| Bacteroidetes | 35.2 ± 4.8 | 0.003 |
| Firmicutes | 50.1 ± 6.0 | 0.012 |
| Lactobacillus | 1.8 ± 0.6 | <0.001 |
| Bifidobacterium | 2.1 ± 0.5 | <0.001 |
| Prevotella | 5.3 ± 1.4 | 0.021 |
| Akkermansia | 0.9 ± 0.4 | 0.045 |
| Sleep Metric | Dysbiosis Group (Mean ± SD) | Healthy Microbiome Group (Mean ± SD) | p-Value |
|---|---|---|---|
| Sleep Efficiency (%) | 78.3 ± 7.1 | 85.7 ± 6.6 | <0.001 |
| REM Sleep Latency (min) | 120.5 ± 17.8 | 90.4 ± 14.9 | <0.001 |
| REM Sleep Duration (min) | 70.2 ± 9.4 | 85.6 ± 9.1 | <0.001 |
| WASO (min) | 45.6 ± 11.9 | 30.3 ± 10.2 | 0.002 |
| N3 Sleep Duration (min) | 80.5 ± 10.8 | 85.2 ± 10.2 | 0.045 |
| Total Sleep Time (h) | 6.5 ± 0.8 | 7.2 ± 0.7 | 0.004 |
| Sleep Onset Latency (min) | 25.3 ± 6.2 | 18.7 ±5.5 | 0.012 |
| Metabolite | Depressive Symptoms (Mean ± SD) | Anxiety Symptoms (Mean ± SD) | Healthy Controls (Mean ± SD) | p-Value |
|---|---|---|---|---|
| Butyrate (µg/mL) | 12.3 ± 2.5 | 14.5 ± 2.7 | 18.7 ± 2.9 | <0.001 |
| Propionate (µg/mL) | 8.5 ± 2.0 | 9.2 ± 2.2 | 12.4 ± 2.4 | 0.003 |
| Kynurenine (ng/mL) | 45.6 ± 6.0 | 55.3 ± 7.0 | 35.4 ± 5.5 | <0.001 |
| Indole-3-acetic acid (ng/mL) | 22.3 ± 3.6 | 28.7 ± 4.0 | 18.5 ± 3.3 | 0.001 |
| Metric | Probiotic Baseline (Mean ± SD) | Probiotic Post-Intervention (Mean ± SD) | Placebo Baseline (Mean ± SD) | Placebo Post-Intervention Mean ± SD) | p-Value * |
|---|---|---|---|---|---|
| Sleep Efficiency (%) | 78.5 ± 7.0 | 86.2 ± 6.5 | 78.7 ± 6.9 | 79.3 ± 6.8 | <0.001 |
| REM Sleep Latency (min) | 118.4 ± 16.0 | 92.3 ± 14.4 | 118.0 ± 15.8 | 115.6 ± 15.5 | <0.001 |
| Depression Score (PHQ-9) | 12.3 ± 3.7 | 7.8 ± 3.0 | 12.1 ± 3.6 | 11.5 ± 3.6 | <0.001 |
| Anxiety Score (GAD-7) | 10.5 ± 3.2 | 6.2 ± 2.5 | 10.3 ± 3.1 | 9.8 ± 3.1 | <0.001 |
| Metric | Probiotic Baseline (Mean ± SD) | Probiotic Post-Intervention (Mean ± SD) | Placebo Post-Intervention (Mean ± SD) | p-Value * |
|---|---|---|---|---|
| Shannon Index | 3.8 ± 0.6 | 4.2 ± 0.5 | 3.9 ± 0.6 | 0.002 |
| Lactobacillus (%) | 1.8 ± 0.6 | 3.5 ± 0.8 | 1.9 ± 0.7 | <0.001 |
| Bifidobacterium (%) | 2.1 ± 0.5 | 4.8 ± 0.9 | 2.2 ± 0.6 | <0.001 |
| Butyrate (µg/mL) | 12.3 ± 2.5 | 16.5 ± 2.7 | 12.5 ± 2.6 | <0.001 |
| Propionate (µg/mL) | 8.5 ± 2.0 | 10.8 ± 2.1 | 10.8 ± 2.1 | 0.005 |
| Pathway | Standardized Beta Coefficient | p-Value |
|---|---|---|
| Circadian Misalignment → Dysbiosis | 0.45 | 0.005 |
| Dysbiosis → Sleep Disturbances | 0.38 | 0.012 |
| Sleep Disturbances → Mental Health | 0.52 | 0.002 |
| Probiotic Intervention → Circadian Alignment | 0.41 | 0.015 |
| Circadian Alignment → Microbial Balance | 0.37 | 0.020 |
| Metabolite | AUC (Depression) | AUC (Anxiety) | p-Value |
|---|---|---|---|
| Butyrate | 0.82 | 0.75 | 0.005 |
| Kynurenine | 0.78 | 0.84 | 0.007 |
| Indole-3-acetic acid | 0.71 | 0.69 | 0.025 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmad, S.R.; AlShahrani, A.M.; Kumari, A. Effects of Probiotic Supplementation on Depressive Symptoms, Sleep Quality, and Modulation of Gut Microbiota and Inflammatory Biomarkers: A Randomized Controlled Trial. Brain Sci. 2025, 15, 761. https://doi.org/10.3390/brainsci15070761
Ahmad SR, AlShahrani AM, Kumari A. Effects of Probiotic Supplementation on Depressive Symptoms, Sleep Quality, and Modulation of Gut Microbiota and Inflammatory Biomarkers: A Randomized Controlled Trial. Brain Sciences. 2025; 15(7):761. https://doi.org/10.3390/brainsci15070761
Chicago/Turabian StyleAhmad, S Rehan, Abdullah M. AlShahrani, and Anupriya Kumari. 2025. "Effects of Probiotic Supplementation on Depressive Symptoms, Sleep Quality, and Modulation of Gut Microbiota and Inflammatory Biomarkers: A Randomized Controlled Trial" Brain Sciences 15, no. 7: 761. https://doi.org/10.3390/brainsci15070761
APA StyleAhmad, S. R., AlShahrani, A. M., & Kumari, A. (2025). Effects of Probiotic Supplementation on Depressive Symptoms, Sleep Quality, and Modulation of Gut Microbiota and Inflammatory Biomarkers: A Randomized Controlled Trial. Brain Sciences, 15(7), 761. https://doi.org/10.3390/brainsci15070761