
Relational, Ethical, and Care Challenges in ALS: A Systematic Review and Qualitative Metasynthesis of Nurses’ Perspectives

 ,
,  , , and
, , and
Abstract
1. Background
2. Materials and Methods
2.1. Study Design
2.2. Formulation of the Research Question
2.3. Search Strategy and Eligibility Criteria
2.4. Data Selection and Extraction
2.5. Quality Evaluation of the Studies
2.6. Data Analysis and Synthesis
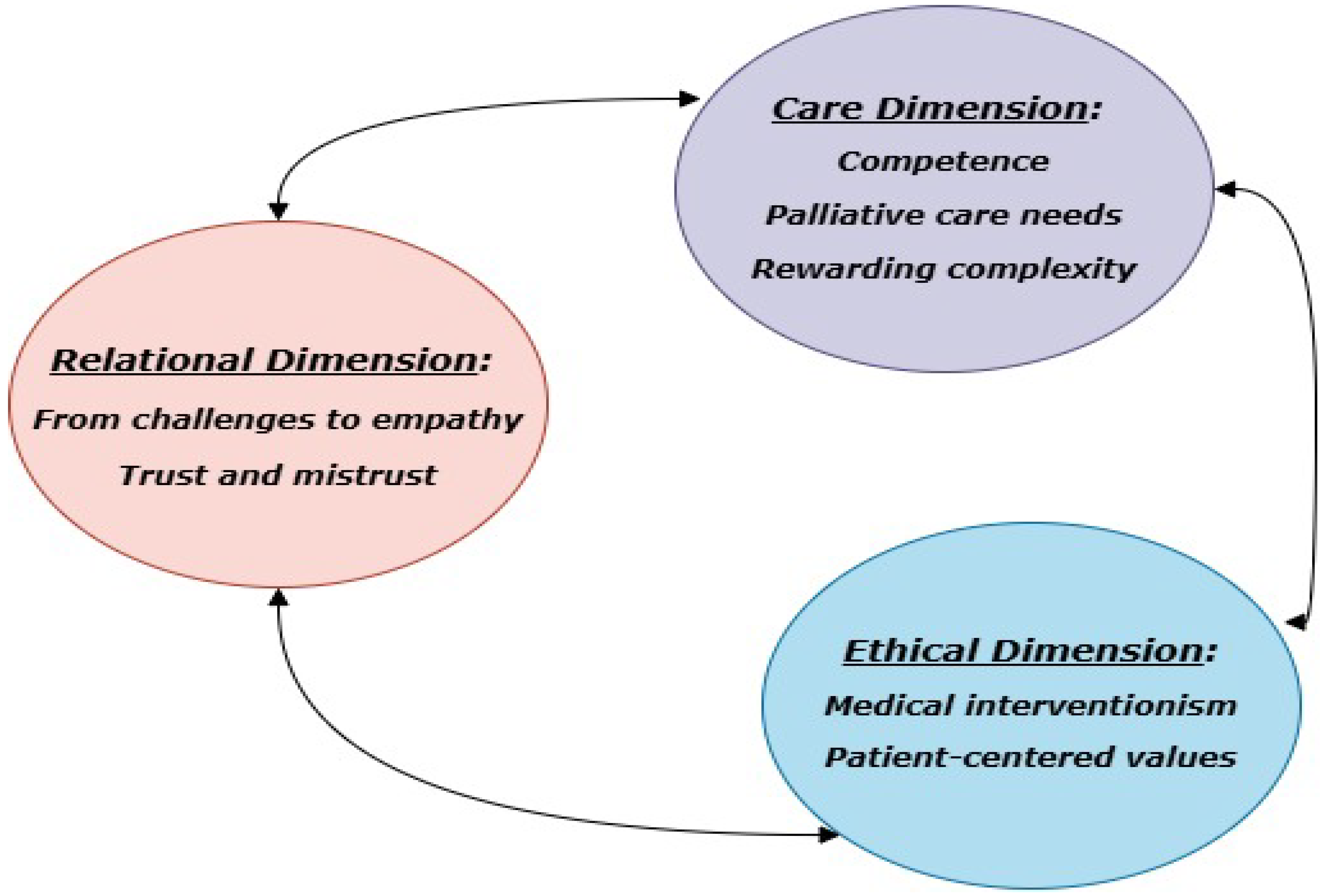
3. Results
3.1. Theme 1. Relational Dimension
3.2. Theme 2. Care Dimension
3.3. Theme 3. Ethical Dimension
4. Discussion
4.1. Relational Dimension
4.2. Care Dimension
4.3. Ethical Dimension
4.4. Strengths, Limitations, and Future Research Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Chen, L.; Zhang, S.; Liu, S.; Gao, S. Amyotrophic Lateral Sclerosis Mechanism: Insights from the Caenorhabditis elegans Models. Cells 2024, 13, 99. [Google Scholar] [CrossRef] [PubMed]
- Aktekin, M.; Uysal, H. Epidemiology of amyotrophic lateral sclerosis. Turk. J. Neurol. 2020, 26, 187–196. [Google Scholar] [CrossRef]
- Cook, S.F.; Rhodes, T.; Schlusser, C.; Han, S.; Chen, C.; Zach, N.; Murthy, V.; Davé, S. A descriptive review of global real world evidence efforts to advance drug discovery and clinical development in amyotrophic lateral sclerosis. Front. Neurol. 2021, 12, 770001. [Google Scholar] [CrossRef] [PubMed]
- Feldman, E.L.; Goutman, S.A.; Petri, S.; Mazzini, L.; Savelieff, M.G.; Shaw, P.J.; Sobue, G. Amyotrophic lateral sclerosis. Lancet 2022, 400, 1363–1380. [Google Scholar] [CrossRef]
- Corcia, P.; Beltran, S.; Bakkouche, S.E.; Couratier, P. Therapeutic news in ALS. Rev. Neurol. 2021, 177, 544–549. [Google Scholar] [CrossRef]
- Calvo, A.; Moglia, C.; Canosa, A.; Manera, U.; Vasta, R.; Grassano, M.; Daviddi, M.; De Mattei, F.; Matteoni, E.; Gallone, S.; et al. High Frequency of Cognitive and Behavioral Impairment in Amyotrophic Lateral Sclerosis Patients with SOD1 Pathogenic Variants. Ann. Neurol. 2024, 96, 150–158. [Google Scholar] [CrossRef]
- Sommers-Spijkerman, M.; Kruitwagen-van Reenen, E.; Kruithof, W.; Visser-Meily, J.M.A.; Scholten, E.; Beelen, A. Quality of Life of People with Neuromuscular Diseases: The Role of Stigma. Muscle Nerve 2025. [Google Scholar] [CrossRef]
- Serizawa, S. Exploration of the Factors Impacting Sustained Clinical Care by Multidisciplinary Professionals for Amyotrophic Lateral Sclerosis. Tokai J. Exp. Clin. Med. 2024, 49, 110–116. [Google Scholar]
- Mercadante, S.; Al-Husinat, L. Palliative care in amyotrophic lateral sclerosis. J. Pain Symptom Manag. 2023, 66, e485–e499. [Google Scholar] [CrossRef]
- Yu, Y.; Zeng, L.; Wu, M.; Li, C.; Qiu, Y.; Liu, J.; Yang, F.; Xia, P. Exploring amyotrophic lateral sclerosis patients’ experiences of psychological distress during the disease course in China: A qualitative study. BMJ Open 2024, 14, e082398. [Google Scholar] [CrossRef]
- Katz, L.; Gur, A. Psychosocial Intervention for Family Caregivers of ALS Patients: A Systematic Review. Healthcare 2024, 12, 1171. [Google Scholar] [CrossRef] [PubMed]
- Bublitz, S.K.; Eham, M.; Ellrott, H.; Littger, B.; Richter, J.; Lorenzl, S. Homecare amyotrophic lateral sclerosis (ALS): A multidisciplinary, home-based model of care for patients with ALS and their caregivers. Muscle Nerve 2024, 70, 937–943. [Google Scholar] [CrossRef] [PubMed]
- Gamskjaer, T.; Werlauff, U.; Handberg, C. Investigating job satisfaction in palliative rehabilitation: Reflections and perspectives of health professionals working with amyotrophic lateral sclerosis. J. Eval. Clin. Pract. 2022, 28, 108–119. [Google Scholar] [CrossRef] [PubMed]
- Alanazi, M.A.; Shaban, M.M.; Ramadan, O.M.E.; Zaky, M.E.; Mohammed, H.H.; Amer, F.G.M.; Shaban, M. Navigating end-of-life decision-making in nursing: A systematic review of ethical challenges and palliative care practices. BMC Nurs. 2024, 23, 467. [Google Scholar] [CrossRef]
- Povedano-Jiménez, M.; Ropero-Padilla, C.; Rodriguez-Arrastia, M.; García-Caro, M.P. Personal and emotional factors of nursing professionals related to coping with end-of-life care: A cross-sectional study. Int. J. Environ. Res. Public Health 2021, 18, 9515. [Google Scholar] [CrossRef]
- Lee, C.N.; Lee, G.; Aw, F.C.; Zulkifle, N.B.; Tan, Y.S.; Amanulla, M.; Chua, E.H.H.; Koh, W.Z.; Lee, J.E.H.; Woong, N.L. Enhancing end-of-life care nursing competency: A nursing education quality improvement project in general medical wards. BMJ Open Qual. 2025, 14, e003228. [Google Scholar] [CrossRef]
- Sandelowski, M.; Barroso, J.; Voils, C.I. Using qualitative metasummary to synthesize qualitative and quantitative descriptive findings. Res. Nurs. Health 2007, 30, 99–111. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Tong, A.; Flemming, K.; McInnes, E.; Oliver, S.; Craig, J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med. Res. Methodol. 2012, 12, 181. [Google Scholar] [CrossRef]
- Cooke, A.; Smith, D.; Booth, A. Beyond PICO: The SPIDER Tool for Qualitative Evidence Synthesis. Qual. Health Res. 2012, 22, 1435–1443. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Porritt, K.; Gomersall, J.; Lockwood, C. JBI’s Systematic Reviews: Study Selection and Critical Appraisal. AJN Am. J. Nurs. 2014, 114, 47. [Google Scholar] [CrossRef] [PubMed]
- Daneau, S.; Bourbonnais, A.; Allard, É.; Asri, M.; Ummel, D.; Bolduc, E. ‘Intensive palliative care’: A qualitative study of issues related to nurses’ care of people with amyotrophic lateral sclerosis at end-of-life. Palliat. Care Soc. Pract. 2023, 17, 26323524231170881. [Google Scholar] [CrossRef] [PubMed]
- McConigley, R.; Kristjanson, L.J.; Aoun, S.M.; Oldham, L.; Currow, D.C.; O’Connor, M.; Holloway, K. Staying just one step ahead: Providing care for patients with motor neurone disease. BMJ Support. Palliat. Care 2014, 4, 38–42. [Google Scholar] [CrossRef]
- Lerum, S.V.; Solbrække, K.N.; Frich, J.C. Healthcare professionals’ accounts of challenges in managing motor neurone disease in primary healthcare: A qualitative study. Health Soc. Care Community 2017, 25, 1355–1363. [Google Scholar] [CrossRef]
- Beyermann, A.; Asp, M.; Godskesen, T.; Söderman, M. Nurses’ challenges when supporting the family of patients with ALS in specialized palliative home care: A qualitative study. Int. J. Qual. Stud. Health Well-Being 2023, 18, 2238984. [Google Scholar] [CrossRef]
- Ushikubo, M. Circumstances and signs of approaching death in patients with amyotrophic lateral sclerosis undergoing noninvasive ventilation in home care settings. J. Neurosci. Nurs. 2018, 50, 182–186. [Google Scholar] [CrossRef]
- Ushikubo, M.; Nashiki, E.; Ohtani, T.; Kawabata, H. Practical measures for dealing with the struggles of nurses caring for people with amyotrophic lateral sclerosis comorbid with cognitive impairment in Japan. Front. Psychol. 2021, 12, 752461. [Google Scholar] [CrossRef]
- Cipolletta, S.; Reggiani, M. End-of-life care after the legal introduction of advance directives: A qualitative study involving healthcare professionals and family caregivers of patients with amyotrophic lateral sclerosis. Palliat. Med. 2021, 35, 209–218. [Google Scholar] [CrossRef]
- Phelps, K.; Regen, E.; Oliver, D.; McDermott, C.; Faull, C. Withdrawal of ventilation at the patient’s request in MND: A retrospective exploration of the ethical and legal issues that have arisen for doctors in the UK. BMJ Support. Palliat. Care 2017, 7, 189–196. [Google Scholar] [CrossRef]
- Shoesmith, C. Chapter 9—Palliative care principles in ALS. In Handbook of Clinical Neurology; Miyasaki, J.M., Kluger, B.M., Eds.; Elsevier: Amsterdam, The Netherlands, 2023; Volume 191, pp. 139–155. [Google Scholar] [CrossRef]
- Kluger, B.M.; Hudson, P.; Hanson, L.C.; Bužgovà, R.; Creutzfeldt, C.J.; Gursahani, R.; Sumrall, M.; White, C.; Oliver, D.J.; Pantilat, S.Z.; et al. Palliative care to support the needs of adults with neurological disease. Lancet Neurol. 2023, 22, 619–631. [Google Scholar] [CrossRef] [PubMed]
- Oliver, D.J.; Borasio, G.D.; Caraceni, A.; de Visser, M.; Grisold, W.; Lorenzl, S.; Veronese, S.; Voltz, R. A consensus review on the development of palliative care for patients with chronic and progressive neurological disease. Eur. J. Neurol. 2016, 23, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Hagan, T.L.; Xu, J.; Lopez, R.P.; Bressler, T. Nursing’s role in leading palliative care: A call to action. Nurse Educ. Today 2018, 61, 216–219. [Google Scholar] [CrossRef] [PubMed]
- Hogden, A.; Foley, G.; Henderson, R.D.; James, N.; Aoun, S.M. Amyotrophic lateral sclerosis: Improving care with a multidisciplinary approach. J. Multidiscip. Healthc. 2017, 10, 205–215. [Google Scholar] [CrossRef]
- Brizzi, K.; Paganoni, S.; Zehm, A.; De Marchi, F.; Berry, J.D. Integration of a palliative care specialist in an amyotrophic lateral sclerosis clinic: Observations from one center. Muscle Nerve. Agosto 2019, 60, 137–140. [Google Scholar] [CrossRef]
- Veronese, S.; Gallo, G.; Valle, A.; Cugno, C.; Chiò, A.; Calvo, A.; Cavalla, P.; Zibetti, M.; Rivoiro, C.; Oliver, D.J. Specialist palliative care improves the quality of life in advanced neurodegenerative disorders: NE-PAL, a pilot randomised controlled study. BMJ Support. Palliat. Care 2017, 7, 164–172. [Google Scholar] [CrossRef]
- Gaertner, J.; Siemens, W.; Meerpohl, J.J.; Antes, G.; Meffert, C.; Xander, C.; Stock, S.; Mueller, D.; Schwarzer, G.; Becker, G. Effect of specialist palliative care services on quality of life in adults with advanced incurable illness in hospital, hospice, or community settings: Systematic review and meta-analysis. BMJ 2017, 357, j2925. Available online: https://www.bmj.com/content/357/bmj.j2925.short (accessed on 6 May 2025). [CrossRef]
- Washington, K.T.; Mechling, C.A.; Pitzer, K.A.; Maiser, S.; Mehta, A.K. Identifying the Unmet Needs of People Living with Amyotrophic Lateral Sclerosis: A National Survey to Inform Interdisciplinary Palliative Care. Am. J. Hosp. Palliat. Med.® 2025, 42, 326–333. [Google Scholar] [CrossRef]
- Brandstötter, C.; Büssing, A.; Eham, M.; Littger, B.; Lorenzl, S.; Memmel, M.; Paal, P.; Bublitz, S.K. Assessment of the Spiritual Needs of People With Amyotrophic Lateral Sclerosis and Their Caregivers. J. Pain Symptom Manag. 2025, 69, 507–514. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Authors | ITEM 1 | ITEM 2 | ITEM 3 | ITEM 4 | ITEM 5 | ITEM 6 | ITEM 7 | ITEM 8 | ITEM 9 | ITEM 10 | Inclusion | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Beyermann et al., 2023 | NS | Y | Y | Y | Y | Y | U | U | Y | U | Y | Included |
| LG | Y | Y | Y | Y | Y | U | U | Y | U | Y | ||
| Daneau et al., 2023 | NS | Y | Y | Y | Y | Y | N | U | Y | Y | Y | Included |
| LG | Y | Y | Y | Y | Y | N | U | Y | Y | Y | ||
| Phelps et al., 2022 | NS | Y | Y | Y | Y | Y | N | N | Y | Y | Y | Included |
| LG | Y | Y | Y | Y | Y | N | N | Y | Y | Y | ||
| Ushikubo et al., 2021 | NS | Y | Y | Y | Y | Y | N | U | Y | Y | Y | Included |
| LG | Y | Y | Y | Y | Y | N | U | Y | Y | Y | ||
| Cipolletta and Reggiani 2021 | NS | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Included |
| LG | Y | Y | Y | Y | Y | U | N | Y | Y | Y | ||
| Ushikubo, 2018 | NS | Y | Y | Y | Y | Y | U | U | Y | Y | Y | Included |
| LG | Y | Y | Y | Y | Y | U | U | Y | Y | Y | ||
| Lerum et al., 2017 | NS | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Included |
| LG | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | ||
| McConigley et al., 2013 | NS | Y | Y | Y | Y | Y | U | U | Y | Y | Y | Included |
| LG | Y | Y | Y | Y | Y | U | U | Y | Y | Y |
| Study | Country | Setting | Study Aim | Study Design | Sample Size (Sex) | Themes | Conclusions |
|---|---|---|---|---|---|---|---|
| Beyermann et al., 2023 | Sweden | Specialized palliative home care | To explore RNs’ experiences of supporting families of ALS patients | Qualitative study | 11 nurses (10 F; 1 M) | (i) “To support in an increasingly difficult everyday life”; (ii) “To support in emotionally challenging situations” | RNs play a vital role in emotional and daily life support for families. |
| Daneau et al., 2023 | Canada | Home care, hospital, palliative care homes | To explore nurses’ experience in end-of-life ALS care | Qualitative multiple-case study | 24 nurses (20 F; 4 M) | (i) identifying the end-of life period, (ii) communication issues, (iii) supporting the need for control, (iv) accompanying in the fight culture, and (v) the extent of the need for care | ALS care requires better staffing, recognition of family involvement, and resources. |
| Phelps et al., 2022 | UK | Hospitals and hospices | To explore experiences of relatives and healthcare professionals during withdrawal of assisted ventilation in ALS. | Retrospective qualitative study | 26 healthcare professionals (Not specified) | (i) Emotional intensity, (ii) ethical/legal ambiguity, (iii) lack of professional guidance, (iv) teamwork importance | Withdrawal of ventilation requires clearer guidelines and training to reduce distress and ensure safe, ethical practice. |
| Ushikubo et al., 2021 | Japan | Home care, hospital, public health centers | To identify practical strategies for nurses caring for ALS patients | Qualitative study | 58 nurses (57 F; 1 M) | (i) “Patients’ strong persistency on specific requirements for nursing assistance in their daily lives”, (ii) “Patients’ problematic behaviors toward nurses”, and (iii) “Struggles in communicating with and understanding patients’ wishes.” | Practical tools and shared experiences improve confidence and care quality. |
| Cipolletta & Reggiani, 2021 | Italy | Various healthcare services and patient associations | To explore end-of-life care after the legal introduction of advance directives. | Qualitative study | 24 healthcare professionals (16 F; 8 M) | (i) Lack of organization, (ii) collaboration and continuity on the part of healthcare services and professionals, (iii) a lack of information on palliative care, (iv) advance care planning, and (v) advance directives | Legal introduction not sufficient without structural and training support. |
| Ushikubo et al., 2018 | Japan | Home care with non-invasive ventilation | To explore circumstances and signs of approaching death in ALS | Retrospective qualitative study | 6 nurses (Not specified) | (i) Difficulties with knowing about approaching death, (ii) several signs and symptoms of knowing about approaching death, (iii) importance of feeling prepared and provision of palliative care to die at home, (iv) death caused by accident, and (v) fate determined by the caregiver’s ability | Recognizing death signs is crucial for timely and preferred end-of-life care. |
| Lerum et al., 2017 | Norway | Home care | To explore challenges in managing ALS in the community | Qualitative study | 18 healthcare professionals (Not specified) | (i) building relationships with those giving and receiving care in the home; (ii) preventing caregiver burnout and breakdown; (iii) providing tailored care; (iv) ensuring good working conditions in patients’ homes; (v) recruiting and retaining qualified nursing assistants. | Home-based ALS care is emotionally challenging and requires better support. |
| McConigley et al., 2013 | Australia | Community and hospital settings | To examine nurses’ perceptions of caring for ALS patients | Qualitative study | 31 healthcare professionals (Not specified) | (i) Just One Step Ahead; (ii) Expertise in MSD and bespoke communication | Palliative care should start early; team communication is critical. |
| Theme | Subtheme | Quote |
|---|---|---|
| Relational dimension | From challenges to empathy | “I think that you don’t need to talk to experience the transpersonal caring relationship. You can experience sadness and pain without necessarily having to express it verbally. When we know that it’s the spirit that’s not ok, we deduce the rest and we feel the sorrow together. At the beginning of my training, it was important for me to do something, to say something, but with the passage of time, I realized that silence has its place in a therapeutic relationship. Now, I can say that I am really comfortable, completely comfortable, with saying nothing and simply existing in the presence of someone else and getting them to express their suffering in ways other than talking” (Daneau et al., 2023) |
| “Well, there’s also the psychological side with the person, but there are barriers all the time, because of communication problems. You know? What is a good therapeutic approach to take with someone who doesn’t communicate 100% verbally? That’s what gets complicated too, because you can’t understand them” (Daneau et al., 2023) | ||
| “You really need to learn to have some empathy and also be quite comfortable talking about end-of-life issues and just how we go about educating some of those things I think is a real challenge because I think some of that has to come through life experience” (McConigley et al., 2013) | ||
| Trust and mistrust | “Day by day, we [were] learning a little bit more about the patient’s routine, and day by day, she gave us a little more room, so she could free herself from the caregiver role and be the spouse again, if you will, to take some breaks” (Daneau et al., 2023) | |
| “She [the individual with ALS] wanted to get it done quickly. Our task was to wash around the PEG, which was something that needed to be done, get the food and finish the visit. Nothing more. Never any talk, never sitting down and sharing a cup of coffee or something like that. Not by either of them [the two with ALS in that region]. And there is very little of that, generally, in the services. […] maybe they have realised that we don’t have the time”(Lerum et al., 2017) | ||
| “I think the support for them the family can be any thing from that I think above all, to show that you see what you see” (Beyermann et al., 2023) | ||
| Care dimension | Competence | “Eventually one has to use assistive devices and medical equipment; all personnel need to be able to use that. This requires a high level of skill and you need to feel confident using it. They [persons with ALS] get respiratory problems, and you need to suck them for mucus. Using cough assist and BiPAP. To be honest, this municipality was not prepared. If there is much uncertainty and insecurity it does not work out. Then it turns into chaos” (Lerum et al., 2017) |
| “Often re-explaining medication management to them because morphine affects breathing too. Sometimes people forget that, so it’s about repeating it, reteaching it, and reassuring them. You know, some people are afraid to take morphine for breathing, but it helps so much. So, it’s about reassuring them, removing the fears and false beliefs if you will” (Daneau et al., 2023) | ||
| Palliative care needs | “I think that, yes, it’s a terrible disease, but I think that we have the means—or the capacity—as nurses to do wonderful things with these patients as well: you just have to take the time. Of course, experience helps, but you have to take the time” (Daneau et al., 2023) | |
| “Home care nurses visited him/her once a week and experienced difficulties assessing symptom aggravation” (Ushikubo, 2018) | ||
| “I would say that sometimes it takes weeks for the patient’s acceptance to arrive, and also, I think, for us to accept that ‘they’re there’. Because I really think we want to fight with them. I think there’s this pattern in our heads, and I would also like to say that, in terms of diet, for example, the step from ‘normal’ to ‘bite-sized’ is not so bad, but when you go from ‘bite-sized’ to ‘minced’, then the step seems to be HUGE, and no one wants to take it. It’s like putting them [the patient] in front of a fait accompli” (Daneau et al., 2023) | ||
| Rewarding complexity | “You know, I have no choice but to be with this patient, because he’s the one who takes up most of my time. But my stroke patient, who is also being tube fed and is panicking because he doesn’t understand the instructions even though his brain is working, I neglect him. So, I always neglect two or three of them because of the ALS workload” (Daneau et al., 2023) | |
| “Some patients frequently press the nurse call button to request fine, millimetric repositioning no matter what time” (Ushikubo et al., 2021) | ||
| “Well, it’s like, I saw this as fair. Not equal, you understand—it’s not the same level of attention, but it’s what the person needs” (Ushikubo et al., 2021) | ||
| Ethical dimension | Medical Interventionism | “The purpose of the wife was to take care of her husband in any condition, using any device to stay alive” (Cipolletta and Reggiani 2021) |
| “I find myself even now, with patients coming from the emergency room and maybe the family members saying ‘No, we don’t want more things interventions’, and instead the young doctor can’t get away from it… so we call for resuscitators, we administer important drugs, we improperly use instruments” (Cipolletta and Reggiani 2021) | ||
| “We have asked for help for this… that is, help us understand how can we relate to these people here. How can you tell someone ‘your life is about to end’?” (Cipolletta and Reggiani 2021) | ||
| “Morally and ethically, I think it was absolutely the right thing and I’m really chuffed we somehow pulled it out of the bag and did it so quickly …” (Phelps et al., 2022) | ||
| Patient-centered values | “We thought that the cognitive decline and the progression of ALS would make it difficult for family caregivers to confirm the patient’s preferences for ventilator use…” (Ushikubo et al., 2021) | |
| “She [the GP] said she was going to have absolutely nothing to do with removing the ventilator or touching the settings or…which made it very difficult because I couldn’t guarantee that I was going to be available around the clock to do it, whereas she could have been, more so, or she could have, perhaps, interacted with me” (Phelps et al., 2022) | ||
| “If that story had been in the news, how would that have been perceived? And would it be the case that some local newspaper would then suddenly say ‘palliative care nurses can now help you die’. And you know, if it’s a tabloid they’re not going to want to engage in the ethics of it, yeah. So I think that was something that was on my mind a little bit” (Phelps et al., 2022) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Artioli, G.; Guardamagna, L.; Succi, N.; Guasconi, M.; Diamanti, O.; Dellafiore, F. Relational, Ethical, and Care Challenges in ALS: A Systematic Review and Qualitative Metasynthesis of Nurses’ Perspectives. Brain Sci. 2025, 15, 600. https://doi.org/10.3390/brainsci15060600
Artioli G, Guardamagna L, Succi N, Guasconi M, Diamanti O, Dellafiore F. Relational, Ethical, and Care Challenges in ALS: A Systematic Review and Qualitative Metasynthesis of Nurses’ Perspectives. Brain Sciences. 2025; 15(6):600. https://doi.org/10.3390/brainsci15060600
Chicago/Turabian StyleArtioli, Giovanna, Luca Guardamagna, Nicole Succi, Massimo Guasconi, Orejeta Diamanti, and Federica Dellafiore. 2025. "Relational, Ethical, and Care Challenges in ALS: A Systematic Review and Qualitative Metasynthesis of Nurses’ Perspectives" Brain Sciences 15, no. 6: 600. https://doi.org/10.3390/brainsci15060600
APA StyleArtioli, G., Guardamagna, L., Succi, N., Guasconi, M., Diamanti, O., & Dellafiore, F. (2025). Relational, Ethical, and Care Challenges in ALS: A Systematic Review and Qualitative Metasynthesis of Nurses’ Perspectives. Brain Sciences, 15(6), 600. https://doi.org/10.3390/brainsci15060600