
Physical, Cognitive, Social, and Functional Health Correlates of Major Depressive Disorder Subtypes: A Systematic Review

 , , ,
, , ,
Abstract
1. Introduction
1.1. Major Depressive Disorder (MDD)
1.2. Purpose of Review
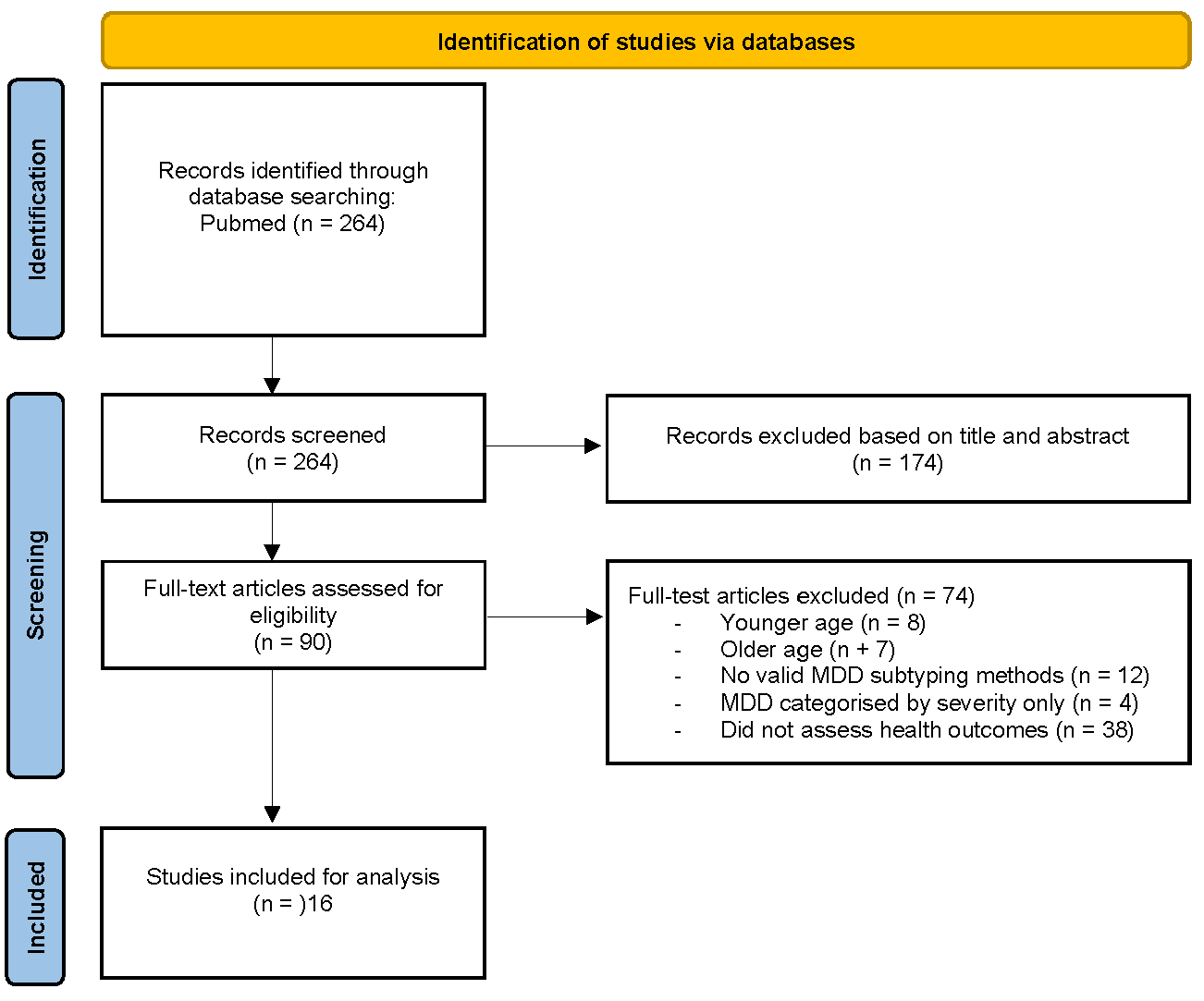
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
2.2. Screening and Data Extraction
2.3. Data Synthesis
3. Results
3.1. Study Characteristics
3.2. Risk of Bias
3.3. Subtyping Methods and Identified MDD Subtypes
3.4. Findings by Health Outcomes
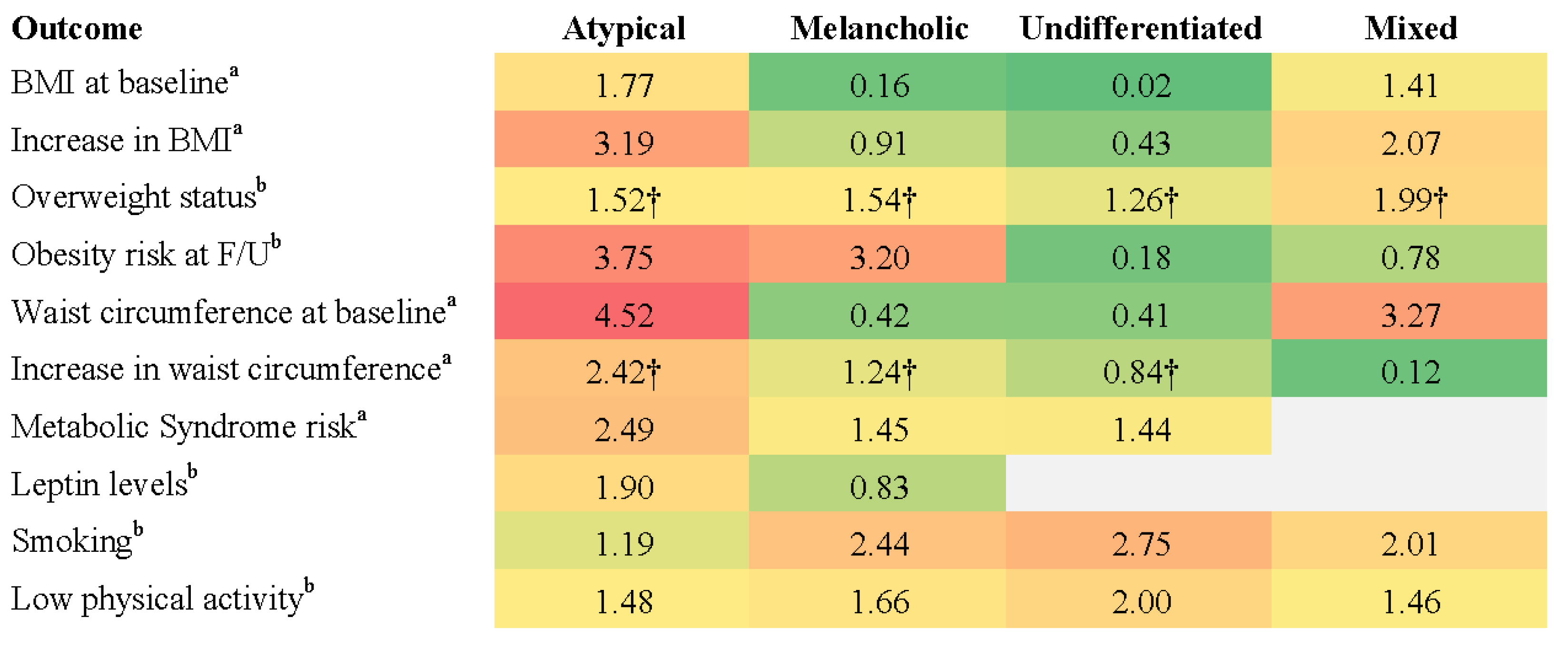
3.4.1. Physical Health
3.4.2. Cognitive Functioning
3.4.3. Social and Functional Outcomes
4. Discussion
4.1. Physical Health and Metabolic Outcomes
4.2. Cognitive Outcomes
4.3. Social and Functional Impairment
4.4. Limitations and Future Directions
4.5. Clinical Implications
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Search Strategy
| Search Term | Field | Yield |
| Title | 80,105 |
| Title | 55,999 |
| Title/Abstract | 5,540,335 |
| Title/Abstract | 2,744,490 |
| 264 |
Appendix B. Inclusion and Exclusion Criteria
| Category | Inclusion Criteria | Exclusion Criteria |
| Population |
|
|
| Subtyping Method |
|
|
| Health Outcomes |
|
|
| Outcome Measures |
|
|
| Study Design |
|
|
| Language |
|
Appendix C. Study Quality Assessment (Newcastle–Ottawa Scale)
| Number of Stars | ||||
| Study (Year) | Selection * | Comparability † | Exposure ‡ | Overall |
| Chan et al. (2023) [55] | 3 | 2 | 1 | 6 |
| Day et al. (2015a) [48] | 4 | 2 | 3 | 9 |
| Day et al. (2015b) [58] | 3 | 2 | 1 | 6 |
| Duan et al. (2021) [49] | 4 | 2 | 3 | 9 |
| Guo et al. (2023) [50] | 4 | 2 | 3 | 9 |
| Lamers et al. (2016) [45] | 4 | 2 | 3 | 9 |
| Lasserre et al. (2014) [46] | 4 | 2 | 3 | 9 |
| Lasserre et al. (2017) [43] | 4 | 2 | 3 | 9 |
| Lin et al. (2014) [51] | 2 | 2 | 1 | 5 |
| Lin et al. (2014b) [57] | 4 | 2 | 3 | 9 |
| Liu et al. (2019) [52] | 2 | 2 | 1 | 5 |
| Lu et al. (2023) [53] | 2 | 2 | 1 | 5 |
| Milaneschi et al. (2017) [44] | 4 | 2 | 1 | 7 |
| Rahe et al. (2016) [47] | 4 | 2 | 1 | 7 |
| Roca et al. (2015) [54] | 3 | 2 | 3 | 8 |
| Zhou et al. (2023) [56] | 2 | 1 | 3 | 6 |
| Average ratings | 3.3 | 1.9 | 2.1 | 7.4 |
References
- World Health Organisation. Depressive Disorder (Depression). Available online: https://www.who.int/news-room/fact-sheets/detail/depression (accessed on 23 February 2025).
- Herrman, H.; Kieling, C.; McGorry, P.; Horton, R.; Sargent, J.; Patel, V. Reducing the global burden of depression: A Lancet-World Psychiatric Association Commission. Lancet 2019, 393, e42–e43. [Google Scholar] [CrossRef] [PubMed]
- Hare, D.L.; Toukhsati, S.R.; Johansson, P.; Jaarsma, T. Depression and cardiovascular disease: A clinical review. Eur. Heart J. 2013, 35, 1365–1372. [Google Scholar] [CrossRef]
- Sartorius, N. Depression and diabetes. Dialogues Clin. Neurosci. 2018, 20, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Deschênes, S.S.; Burns, R.J.; Schmitz, N. Associations between depression, chronic physical health conditions, and disability in a community sample: A focus on the persistence of depression. J. Affect. Disord. 2015, 179, 6–13. [Google Scholar] [CrossRef]
- Baune, B.T.; Miller, R.; McAfoose, J.; Johnson, M.; Quirk, F.; Mitchell, D. The role of cognitive impairment in general functioning in major depression. Psychiatry Res. 2010, 176, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Hirschfeld, R.M.; Montgomery, S.A.; Keller, M.B.; Kasper, S.; Schatzberg, A.F.; Möller, H.J.; Healy, D.; Baldwin, D.; Humble, M.; Versiani, M.; et al. Social functioning in depression: A review. J. Clin. Psychiatry 2000, 61, 268–275. [Google Scholar] [CrossRef]
- Gunnarsson, A.B.; Hedberg, A.K.; Håkansson, C.; Hedin, K.; Wagman, P. Occupational performance problems in people with depression and anxiety. Scand. J. Occup. Ther. 2023, 30, 148–158. [Google Scholar] [CrossRef]
- Hansson, L. Quality of life in depression and anxiety. Int. Rev. Psychiatry 2002, 14, 185–189. [Google Scholar] [CrossRef]
- Hohls, J.K.; König, H.H.; Quirke, E.; Hajek, A. Anxiety, Depression and Quality of Life-A Systematic Review of Evidence from Longitudinal Observational Studies. Int. J. Environ. Res. Public Health 2021, 18, 12022. [Google Scholar] [CrossRef]
- Carragher, N.; Adamson, G.; Bunting, B.; McCann, S. Subtypes of depression in a nationally representative sample. J. Affect. Disord. 2009, 113, 88–99. [Google Scholar] [CrossRef]
- Arnow, B.A.; Blasey, C.; Williams, L.M.; Palmer, D.M.; Rekshan, W.; Schatzberg, A.F.; Etkin, A.; Kulkarni, J.; Luther, J.F.; Rush, A.J. Depression Subtypes in Predicting Antidepressant Response: A Report From the iSPOT-D Trial. Am. J. Psychiatry 2015, 172, 743–750. [Google Scholar] [CrossRef] [PubMed]
- Simmonds-Buckley, M.; Catarino, A.; Delgadillo, J. Depression subtypes and their response to cognitive behavioral therapy: A latent transition analysis. Depress. Anxiety 2021, 38, 907–916. [Google Scholar] [CrossRef] [PubMed]
- Simmons, W.K.; Burrows, K.; Avery, J.A.; Kerr, K.L.; Taylor, A.; Bodurka, J.; Potter, W.; Teague, T.K.; Drevets, W.C. Appetite changes reveal depression subgroups with distinct endocrine, metabolic, and immune states. Mol. Psychiatry 2020, 25, 1457–1468. [Google Scholar] [CrossRef]
- APA. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2022. [Google Scholar]
- World Health Organization. ICD-11: International Classification of Diseases, 11th ed.; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Buch, A.M.; Liston, C. Dissecting diagnostic heterogeneity in depression by integrating neuroimaging and genetics. Neuropsychopharmacology 2021, 46, 156–175. [Google Scholar] [CrossRef]
- Ostergaard, S.; Jensen, S.; Bech, P. The heterogeneity of the depressive syndrome: When numbers get serious. Acta Psychiatr. Scand. 2011, 124, 495–496. [Google Scholar] [CrossRef] [PubMed]
- Parker, G.; Fink, M.; Shorter, E.; Taylor, M.A.; Akiskal, H.; Berrios, G.; Bolwig, T.; Brown, W.A.; Carroll, B.; Healy, D.; et al. Issues for DSM-5: Whither melancholia? The case for its classification as a distinct mood disorder. Am. J. Psychiatry 2010, 167, 745–747. [Google Scholar] [CrossRef] [PubMed]
- Łojko, D.; Rybakowski, J.K. Atypical depression: Current perspectives. Neuropsychiatr. Dis. Treat. 2017, 13, 2447–2456. [Google Scholar] [CrossRef]
- Stewart, J.W.; Thase, M.E. Treating DSM-IV depression with atypical features. J. Clin. Psychiatry 2007, 68, e10. [Google Scholar] [CrossRef]
- Quitkin, F.M. Depression with Atypical Features: Diagnostic Validity, Prevalence, and Treatment. Prim. Care Companion J. Clin. Psychiatry 2002, 4, 94–99. [Google Scholar] [CrossRef]
- Rush, A.J.; Weissenburger, J.E. Melancholic symptom features and DSM-IV. Am. J. Psychiatry 1994, 151, 489–498. [Google Scholar] [CrossRef]
- Hagenaars, J.A.; McCutcheon, A.L. (Eds.) Applied Latent Class Analysis; Cambridge University Press: Cambridge, UK, 2002. [Google Scholar]
- Lange, R.T.; Iverson, G.L.; Senior, G.J.; Chelune, G.J. A primer on cluster analysis applications to cognitive rehabilitation research. J. Cogn. Rehabil. 2002, 20, 16–33. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Taylor-Phillips, S.; Geppert, J.; Stinton, C.; Freeman, K.; Johnson, S.; Fraser, H.; Sutcliffe, P.; Clarke, A. Comparison of a full systematic review versus rapid review approaches to assess a newborn screening test for tyrosinemia type 1. Res. Synth. Methods 2017, 8, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Shea, B.; O’Connell, J. The Newcastle-Ottawa Scale (NOS) for Assessing The Quality of Nonrandomised Studies in Meta-Analyses. Ott. Health Res. Inst. Web Site 2014, 7. [Google Scholar]
- WHO. WHOQOL: Measuring Quality of Life; Department of Mental Health, World Health Organization: Geneva, Switzerland, 1997. [Google Scholar]
- Ware, J.E.; Kosinski, M. SF-36 Physical & Mental Health Summary Scales: A Manual for Users of Version 1; Quality Metric: Lincoln, OR, USA, 2001. [Google Scholar]
- Üstün, T.B. Measuring Health and Disability: Manual for WHO Disability Assessment Schedule WHODAS 2.0; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Skevington, S.M.; Wright, A. Changes in the quality of life of patients receiving antidepressant medication in primary care: Validation of the WHOQOL-100. Br. J. Psychiatry 2001, 178, 261–267. [Google Scholar] [CrossRef]
- Berlim, M.T.; Pavanello, D.P.; Caldieraro, M.A.K.; Fleck, M.P.A. Reliability and validity of the WHOQOL BREF in a sample of Brazilian outpatients with major depression. Qual. Life Res. 2005, 14, 561–564. [Google Scholar] [CrossRef]
- Matcham, F.; Norton, S.; Steer, S.; Hotopf, M. Usefulness of the SF-36 Health Survey in screening for depressive and anxiety disorders in rheumatoid arthritis. BMC Musculoskelet. Disord. 2016, 17, 224. [Google Scholar] [CrossRef]
- Abdin, E.; Seet, V.; Jeyagurunathan, A.; Tan, S.C.; Mok, Y.M.; Verma, S.; Lee, E.S.; Subramaniam, M. Validation of the 12-item World Health Organization Disability Assessment Schedule 2.0 in individuals with schizophrenia, depression, anxiety, and diabetes in Singapore. PLoS ONE 2023, 18, e0294908. [Google Scholar] [CrossRef]
- Frank, P.; Batty, G.D.; Pentti, J.; Jokela, M.; Poole, L.; Ervasti, J.; Vahtera, J.; Lewis, G.; Steptoe, A.; Kivimäki, M. Association Between Depression and Physical Conditions Requiring Hospitalization. JAMA Psychiatry 2023, 80, 690–699. [Google Scholar] [CrossRef]
- Berk, M.; Köhler-Forsberg, O.; Turner, M.; Penninx, B.; Wrobel, A.; Firth, J.; Loughman, A.; Reavley, N.J.; McGrath, J.J.; Momen, N.C.; et al. Comorbidity between major depressive disorder and physical diseases: A comprehensive review of epidemiology, mechanisms and management. World Psychiatry 2023, 22, 366–387. [Google Scholar] [CrossRef]
- Lam, R.W.; Kennedy, S.H.; McLntyre, R.S.; Khullar, A. Cognitive dysfunction in major depressive disorder: Effects on psychosocial functioning and implications for treatment. Can. J. Psychiatry 2014, 59, 649–654. [Google Scholar] [CrossRef]
- Murrough, J.W.; Iacoviello, B.; Neumeister, A.; Charney, D.S.; Iosifescu, D.V. Cognitive dysfunction in depression: Neurocircuitry and new therapeutic strategies. Neurobiol. Learn. Mem. 2011, 96, 553–563. [Google Scholar] [CrossRef] [PubMed]
- Hasselbalch, B.J.; Knorr, U.; Hasselbalch, S.G.; Gade, A.; Kessing, L.V. Cognitive deficits in the remitted state of unipolar depressive disorder. Neuropsychology 2012, 26, 642–651. [Google Scholar] [CrossRef]
- Kupferberg, A.; Bicks, L.; Hasler, G. Social functioning in major depressive disorder. Neurosci. Biobehav. Rev. 2016, 69, 313–332. [Google Scholar] [CrossRef] [PubMed]
- Ustün, B.; Kennedy, C. What is “functional impairment”? Disentangling disability from clinical significance. World Psychiatry 2009, 8, 82–85. [Google Scholar] [CrossRef] [PubMed]
- Lasserre, A.M.; Strippoli, M.F.; Glaus, J.; Gholam-Rezaee, M.; Vandeleur, C.L.; Castelao, E.; Marques-Vidal, P.; Waeber, G.; Vollenweider, P.; Preisig, M. Prospective associations of depression subtypes with cardio-metabolic risk factors in the general population. Mol. Psychiatry 2017, 22, 1026–1034. [Google Scholar] [CrossRef]
- Milaneschi, Y.; Lamers, F.; Bot, M.; Drent, M.L.; Penninx, B.W. Leptin Dysregulation Is Specifically Associated with Major Depression with Atypical Features: Evidence for a Mechanism Connecting Obesity and Depression. Biol. Psychiatry 2017, 81, 807–814. [Google Scholar] [CrossRef]
- Lamers, F.; Beekman, A.T.; van Hemert, A.M.; Schoevers, R.A.; Penninx, B.W. Six-year longitudinal course and outcomes of subtypes of depression. Br. J. Psychiatry 2016, 208, 62–68. [Google Scholar] [CrossRef]
- Lasserre, A.M.; Glaus, J.; Vandeleur, C.L.; Marques-Vidal, P.; Vaucher, J.; Bastardot, F.; Waeber, G.; Vollenweider, P.; Preisig, M. Depression with atypical features and increase in obesity, body mass index, waist circumference, and fat mass: A prospective, population-based study. JAMA Psychiatry 2014, 71, 880–888. [Google Scholar] [CrossRef]
- Rahe, C.; Khil, L.; Wellmann, J.; Baune, B.T.; Arolt, V.; Berger, K. Impact of major depressive disorder, distinct subtypes, and symptom severity on lifestyle in the BiDirect Study. Psychiatry Res. 2016, 245, 164–171. [Google Scholar] [CrossRef]
- Day, C.V.; Gatt, J.M.; Etkin, A.; DeBattista, C.; Schatzberg, A.F.; Williams, L.M. Cognitive and emotional biomarkers of melancholic depression: An iSPOT-D report. J. Affect. Disord. 2015a, 176, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Duan, Y.; Wei, J.; Geng, W.; Jiang, J.; Zhao, X.; Li, T.; Jiang, Y.; Shi, L.; Cao, J.; Zhu, G.; et al. Research on Cognitive Function in Anxious Depression Patients in China. J. Affect. Disord. 2021, 280, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Liu, B.; Wei, X.; Ju, Y.; Wang, M.; Dong, Q.; Lu, X.; Sun, J.; Zhang, L.; Guo, H.; et al. The longitudinal change pattern of cognitive subtypes in medication-free patients with major depressive disorder: A cluster analysis. Psychiatry Res. 2023, 327, 115413. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.; Xu, G.; Lu, W.; Ouyang, H.; Dang, Y.; Lorenzo-Seva, U.; Guo, Y.; Bessonov, D.; Akiskal, H.S.; So, K.F.; et al. Neuropsychological performance in melancholic, atypical and undifferentiated major depression during depressed and remitted states: A prospective longitudinal study. J. Affect. Disord. 2014a, 168, 184–191. [Google Scholar] [CrossRef]
- Liu, W.; Zhou, Y.; Zheng, W.; Wang, C.; Zhan, Y.; Li, H.; Chen, L.; Zhao, C.; Ning, Y. Mediating effect of neurocognition between severity of symptoms and social-occupational function in anxious depression. J. Affect. Disord. 2019, 246, 667–673. [Google Scholar] [CrossRef]
- Lu, W.; Zhang, H.; Zhou, R.; Ding, L.; Wang, Y.; Su, Y.; Wang, X.; Chen, J.; Wu, B.; He, S.; et al. Differences in cognitive functions of atypical and non-atypical depression based on propensity score matching. J. Affect. Disord. 2023, 325, 732–738. [Google Scholar] [CrossRef]
- Roca, M.; Monzón, S.; Vives, M.; López-Navarro, E.; Garcia-Toro, M.; Vicens, C.; Garcia-Campayo, J.; Harrison, J.; Gili, M. Cognitive function after clinical remission in patients with melancholic and non-melancholic depression: A 6 month follow-up study. J. Affect. Disord. 2015, 171, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Chan, R.Y.T.; Hu, H.X.; Wang, L.L.; Chan, M.K.M.; Ho, Z.T.Y.; Cheng, K.M.; Lui, S.S.Y.; Chan, R.C.K. Emotional subtypes in patients with depression: A cluster analysis. Psych. J. 2023, 12, 452–460. [Google Scholar] [CrossRef]
- Zhou, E.; Ma, S.; Kang, L.; Zhang, N.; Wang, P.; Wang, W.; Nie, Z.; Chen, M.; Xu, J.; Sun, S.; et al. Psychosocial factors associated with anxious depression. J. Affect. Disord. 2023, 322, 39–45. [Google Scholar] [CrossRef]
- Lin, C.H.; Wang, F.C.; Lin, S.C.; Chen, C.C.; Huang, C.J. A comparison of inpatients with anxious depression to those with nonanxious depression. Psychiatry Res. 2014b, 220, 855–860. [Google Scholar] [CrossRef]
- Day, C.V.; Rush, A.J.; Harris, A.W.; Boyce, P.M.; Rekshan, W.; Etkin, A.; DeBattista, C.; Schatzberg, A.F.; Arnow, B.A.; Williams, L.M. Impairment and distress patterns distinguishing the melancholic depression subtype: An iSPOT-D report. J. Affect. Disord. 2015b, 174, 493–502. [Google Scholar] [CrossRef] [PubMed]
- First, M.B.; Williams, J.B.W.; Karg, R.S.; Spitzer, R.L. User’s Guide for the SCID-5-CV Structured Clinical Interview for DSM-5® Disorders: Clinical Version; American Psychiatric Publishing, Inc.: Arlington, VA, USA, 2016. [Google Scholar]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59 (Suppl. S20), 22–33; quiz 34–57. [Google Scholar]
- Rush, A.J.; Gullion, C.M.; Basco, M.R.; Jarrett, R.B.; Trivedi, M.H. The Inventory of Depressive Symptomatology (IDS): Psychometric properties. Psychol. Med. 1996, 26, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Parker, G.; McCraw, S. The properties and utility of the CORE measure of melancholia. J. Affect. Disord. 2017, 207, 128–135. [Google Scholar] [CrossRef]
- Bosc, M.; Dubini, A.; Polin, V. Development and validation of a social functioning scale, the Social Adaptation Self-evaluation Scale. Eur. Neuropsychopharmacol. 1997, 7, S57–S70. [Google Scholar] [CrossRef]
- Bennabi, D.; Vandel, P.; Papaxanthis, C.; Pozzo, T.; Haffen, E. Psychomotor retardation in depression: A systematic review of diagnostic, pathophysiologic, and therapeutic implications. BioMed Res. Int. 2013, 2013, 158746. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Physical Health and Metabolic Outcomes | |||||||
|---|---|---|---|---|---|---|---|
| Author (Year) | Country | Study Design | Sample Size | Population Characteristics | MDD Subtypes and Classification Method | Health Outcomes Assessed | Measures Used |
| Lasserre et al. (2017) [43] | Switzerland | Longitudinal cohort study (5.5-year follow-up) | 2813 participants (179 atypical depression, 369 melancholic depression, 685 unspecified depression, 1580 non-MDD) | Adults (35–66 years old) from the CoLaus/PsyCoLaus population-based cohort | Melancholic, atypical, unspecified; DSM-IV criteria (DIGS) and symptom specifiers | Metabolic health, physical health | Fasting glucose, HDL cholesterol, triglycerides, systolic blood pressure, metabolic syndrome, leptin levels (ELISA assay), BMI, waist circumference |
| Milaneschi et al. (2017) [44] | The Netherlands | Cross-sectional observational | 2270 participants (271 current severe typical, 521 current moderate, 270 current severe atypical, 711 remitted MDD, 497 HC) | Adults (18–65 years old) from The Netherlands Study of Depression and Anxiety (NESDA) | Atypical, typical, and moderate; LCA based on symptom profiles | Physical health | Leptin levels (ELISA assay), BMI, waist circumference |
| Lamers et al. (2016) [45] | The Netherlands | Longitudinal observational (6-year follow-up) | 1248 participants (308 severe melancholic, 167 severe atypical, 173 moderate, 600 HC) | Adults (18–65 years old) with MDD (CIDI) recruited from the NESDA cohort | Severe melancholic, severe atypical, and moderate; LCA based on CIDI and IDS-SR symptom profiles | Somatic health, overall functioning | BMI, metabolic syndrome prevalence, waist circumference, fasting glucose, triglycerides, HDL cholesterol, blood pressure, WHODAS |
| Lasserre et al. (2014) [46] | Switzerland | Longitudinal cohort (5.5-year follow-up) | 3054 participants (48 current atypical, 55 current melancholic, 31 current combined, 97 current unspecified, 1121 remitted MDD, 1702 non-MDD) | Adults (35–66 years old) from the CoLaus/PsyCoLaus population-based cohort | Melancholic and atypical; DSM-IV criteria (DIGS) and symptom specifiers | Physical health | BMI, waist circumference, fat mass (bioimpedance) |
| Rahe et al. (2016) [47] | Germany | Cross-sectional observational | 1420 participants (503 melancholic depression, 43 atypical depression, 81 mixed depression, 196 undifferentiated depression, 597 HC) | Adults (35–65 years old) from the BiDirect Study | Melancholic, atypical, mixed, and undifferentiated; DSM-IV criteria (MINI) and IDS items for atypical features | Physical health | BMI, combined lifestyle index (0–4 unhealthy lifestyle factors) |
| Cognitive Outcomes | |||||||
| Author (Year) | Country | Study Design | Sample Size | Population Characteristics | MDD Subtyping Method | Health Outcomes Assessed | Measures Used |
| Day et al. (2015a) [48] | iSPOT (USA, Australia, The Netherlands, New Zealand, South Africa) | Cross-sectional observational | 1344 participants (339 melancholic depression, 669 non-melancholic depression, 336 HC) | Adults (18–65 years old) diagnosed with MDD (DSM-IV, MINI) | Melancholic; DSM-IV criteria and psychomotor disturbance (CORE score ≥ 7) | Cognitive function, emotional function | Standardised cognitive battery |
| Duan et al. (2021) [49] | China | Longitudinal observational (8-week follow-up) | 1048 participants (328 anxious depression, 221 non-anxious depression, 499 HC) | Adults (18–55 years old) with MDD (MINI) | Anxious; HAMD-17 anxiety/somatization factor score ≥ 7 | Cognitive function | HVLT-R, BVMT-R, SCWT, CPT |
| Guo et al. (2023) [50] | China | Longitudinal observational (6-month follow-up) | 295 participants (91 MDD preserved cognition, 62 MDD impaired cognition, 142 HC) | Medication-free adults (18–55 years old) with MDD (SCID) | Cognitive subtypes (preserved vs. impaired cognition); K-means cluster analysis | Cognitive function | DSB, DSF, SCWT, TMT-A, TMT-B, SVF, VMT, WMS |
| Lin et al. (2014a) [51] | China | Prospective longitudinal | 509 participants (142 melancholic depression, 76 atypical depression, 91 undifferentiated depression, 200 HC) | Adults (18–60 years old) with MDD (DSM-IV-TR) | Melancholic, atypical, and undifferentiated; DSM-IV structured clinical interviews | Cognitive function | TMT-A, DSC (WAIS-RC), DSF (WAIS-RC), DSB (WAIS-RC), WCST-M, TMT-B, TOH, AN, IVR (WMS-RC) |
| Liu et al. (2019) [52] | China | Cross-sectional observational | 214 participants (138 anxious depression, 76 non-anxious depression); no HC | Adults (18–65 years old) with MDD (DSM-5) | Anxious; HAMD-17 anxiety/somatization factor score ≥ 7 | Cognitive function, social and occupational function | MCCB, GAF |
| Lu et al. (2023) [53] | China | Cross-sectional observational | 353 participants (101 atypical depression, 252 non-atypical depression); no HC | Adults (16–60 years old) with MDD (MINI) | Atypical; DSM-5 criteria and Inventory of Depressive Symptomatology (IDS-30) | Cognitive function, QoL | MCCB, QOL-6 |
| Roca et al. (2015) [54] | Spain | Longitudinal observational (6-month follow-up) | 88 participants (25 melancholic depression, 63 non-melancholic depression); no HC | Adults (18–55 years old) with MDD (DSM-IV-TR) | Melancholic; DSM-IV-TR, CORE Index for Melancholia, and HAMD-17 score ≥ 17 | Cognitive function | TMT-A, TMT-B, DSF (WAIS-III), DSB (WAIS-III), SCWT, TOL DX, FAS, SVF (Animals), FTT |
| Social and Functional Impairment | |||||||
| Author (Year) | Country | Study Design | Sample Size | Population Characteristics | MDD Subtyping Method | Health Outcomes Assessed | Measures Used |
| Chan et al. (2023) [55] | Hong Kong | Cross-sectional observational | 200 participants (150 MDD patients, 50 controls) | Adults (18–65 years old) with MDD (SCID) | Social subtypes; two-stage cluster analysis based on emotion-related measures (TEPS, TAS, ERQ) | Social functioning | Social Adaptation Self-Evaluation Scale (SASS) |
| Zhou et al. (2023) [56] | China | Cross-sectional observational | 809 participants (326 anxious depression, 483 non-anxious depression); no HC | Adults (19–23 years old) with MDD (MINI) | Anxious; HAMD-17 anxiety/somatization factor score ≥ 7 | Family functioning, social support, interpersonal problems | Family Assessment Device (FAD), Social Support Rating Scale (SSRS), Interpersonal Relationship Integrated Diagnostic Scale (IRIDS) |
| Lin et al. (2014b) [57] | Taiwan | Cross-sectional observational | 174 participants (141 anxious depression, 33 non-anxious depression); no HC | Adult inpatients (18–70 years old) with MDD (SCID) | Anxious and non-anxious depression; (HAMD-17) anxiety/somatization factor score ≥ 7 | Pain, QoL, daily functioning | SF-36 Body Pain Index (BPI), SF-36 Physical Component Summary (PCS), SF-36 Mental Component Summary (MCS), Global Assessment of Functioning (GAF), Work and Social Adjustment Scale (WSAS) |
| Day et al. (2015b) [58] | iSPOT (USA, Australia, The Netherlands, New Zealand, South Africa) | Longitudinal observational study (8-week follow-up) | 1008 MDD participants (339 melancholic, 667 non-melancholic); no HC | Adults (18–65 years old) with MDD (DSM-IV, MINI) | Melancholic; DSM-IV criteria and psychomotor disturbance (CORE score ≥ 7) | Functional capacity, distress and coping, personality, emotion regulation | Social and Occupational Functioning Assessment Scale (SOFAS), World Health Organization Quality of Life (WHOQOL), Brief Risk-Resilience Index for Screening (BRISC), Satisfaction with Life Scale (SWLS), NEO-Five Factor Inventory (NEO-FFI), Emotion Regulation Questionnaire (ERQ) |
| DSM-Defined MDD Subtype | Group Comparison (n) | Outcome | p-Value |
|---|---|---|---|
| Melancholic [54] | Mel. (25) vs. NM (63) | ↓ verbal working memory | |
| DSF | 0.027 | ||
| DSB | 0.049 | ||
| ↓ executive function | |||
| TMT-B | 0.05 | ||
| SCWT-I | 0.031 | ||
| SCWT-II | 0.005 | ||
| ↓ psychomotor speed | |||
| FTT | 0.034 | ||
| ↓ problem-solving | |||
| TOL DX problem-solving | 0.018 | ||
| TOL DX execution | 0.043 | ||
| [48] | Mel. (339) vs. NM (669) | ↓ attention-switching | <0.01 |
| [51] | Mel. (142) vs. Atypical (76); Undiff. (91) | ↓ processing speed | |
| DSC | <0.001 | ||
| TMT-A | <0.001 | ||
| ↑ cognitive inflexibility | |||
| WCST-M | <0.001 | ||
| ↓ semantic fluency | |||
| AN | <0.001 | ||
| Atypical [51] | Atypical (76) vs. Mel. (142); Undiff. (91) | ↑ cognitive inflexibility | |
| WCST-M | 0.001 | ||
| [53] | Atypical (101) vs. Non-atypical (252) | ↓ attention/vigilance | 0.042 |
| ↑ social cognition impairments | 0.035 | ||
| Anxious [49] | Anxious (328) vs. Non-anxious (221) | ↑ verbal memory | |
| HVLT-R | 0.003 | ||
| ↑ visual memory | |||
| BVMT-R | 0.005 |
| MDD Subtype | Group Comparison (n) | Outcome | p-Value |
|---|---|---|---|
| Generalised Emotional Deficits (Data-driven) [55] | Cluster 2 (66) vs. Cluster 1 (50); Cluster 3 (34) | ↓ social adaptation SASS | <0.001 |
| Anxious [56] | Anxious (326) vs. Non-anxious (483) | ↑ interpersonal difficulties engaging in conversations making friends following social norms ↓ social support objective support subjective support support utilisation ↑ family dysfunction problem-solving communication family roles affective responsiveness overall family functioning | <0.001 <0.001 <0.001 0.002 0.002 0.048 <0.001 <0.001 <0.001 0.002 <0.001 |
| Melancholic [58] | Mel. (339) vs. NM (667) | ↓ social relationships ↑ social skill deficits ↑ emotional distress and maladaptive coping strategies negativity bias emotional resilience suppression as an emotion regulation strategy | 0.03 <0.001 0.03 <0.001 <0.001 |
| DSM-Defined MDD Subtype | Group Comparison (n) | Outcome | p-Value |
|---|---|---|---|
| Anxious [57] | Anxious (141) vs. Non-anxious (33) | ↓ global functioning ↑ work-related impairment ↑ psychological impairment ↓ physical functioning ↑ bodily pain | 0.029 0.011 0.020 <0.001 0.001 |
| Melancholic [58] | Mel. (339) vs. NM (667) | ↑ impairments in social and occupational functioning ↓ overall QoL ↓ physical health ↓ psychological well-being | <0.001 <0.001 0.01 <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McKeough, J.E.; Sharpley, C.F.; Vessey, K.A.; Bitsika, V.; Williams, R.J.; Odierna, G.L.; Evans, I.D. Physical, Cognitive, Social, and Functional Health Correlates of Major Depressive Disorder Subtypes: A Systematic Review. Brain Sci. 2025, 15, 525. https://doi.org/10.3390/brainsci15050525
McKeough JE, Sharpley CF, Vessey KA, Bitsika V, Williams RJ, Odierna GL, Evans ID. Physical, Cognitive, Social, and Functional Health Correlates of Major Depressive Disorder Subtypes: A Systematic Review. Brain Sciences. 2025; 15(5):525. https://doi.org/10.3390/brainsci15050525
Chicago/Turabian StyleMcKeough, Jen E., Christopher F. Sharpley, Kirstan A. Vessey, Vicki Bitsika, Rebecca J. Williams, G. Lorenzo Odierna, and Ian D. Evans. 2025. "Physical, Cognitive, Social, and Functional Health Correlates of Major Depressive Disorder Subtypes: A Systematic Review" Brain Sciences 15, no. 5: 525. https://doi.org/10.3390/brainsci15050525
APA StyleMcKeough, J. E., Sharpley, C. F., Vessey, K. A., Bitsika, V., Williams, R. J., Odierna, G. L., & Evans, I. D. (2025). Physical, Cognitive, Social, and Functional Health Correlates of Major Depressive Disorder Subtypes: A Systematic Review. Brain Sciences, 15(5), 525. https://doi.org/10.3390/brainsci15050525