

Partner-Inflicted Brain Injury: Intentional, Concurrent, and Repeated Traumatic and Hypoxic Neurologic Insults

 , , , ,
, , , ,
Abstract
1. Introduction
1.1. Prevalence and Health Impact of Intimate Partner Violence (IPV)—Worldwide
1.2. The Prevalence and Health Impact of IPV—A United States (U.S.) Perspective
1.3. Traumatic Brain Injury (TBI) and Hypoxic–Anoxic Brain Injury (HAI)
1.4. The Early Studies of Head Trauma and Strangulation Exposure from IPV
1.5. The Early Studies Naming Traumatic and Hypoxic Partner-Related Injury
1.6. Trauma, Strangulation, and Head Injury in Research and Practice
1.7. Context and Aims of Current Research
2. Materials and Methods
2.1. Survivor Interviews
2.2. Participants
2.3. Instrumentation
2.4. Analysis
3. Results
3.1. Sample Characteristics
3.2. Lifetime Exposure to Strangulation and Intentional Head Trauma—All Sources
3.3. Lifetime Exposure to Both Strangulation and/or Intentional Head Trauma—All Sources
3.4. The Co-Occurrence of Head Trauma and Strangulation by an Intimate Partner
3.5. Probable Partner-Inflicted Brain Injury
4. Discussion
4.1. Reflection on Results
4.2. Partner-Inflicted Brain Injury
4.3. CARE (Connect, Acknowledge, Respond, Evaluate): An Intervention to Address PIBI
- Connect genuinely with survivors;
- Acknowledge that head trauma and strangulation are common forms of IPV assault and can have physical, cognitive, emotional, and behavioral consequences immediately, but also years later;
- Respond by accommodating needs related to brain injury, strangulation, and mental health challenges in services and provide effective, accessible referrals and advocacy for individuals who need additional care;
- Evaluate if accommodations and referrals were effective, reassess needs, and respond accordingly.
- To connect with survivors on the topics of head trauma, strangulation, and mental health concerns (e.g., suicide ideation, emotion lability, and substance use), to facilitate survivors’ self-advocacy and connection to other service systems (e.g., medical and courts), and for self-connection and self-care to address historical and secondary trauma that service providers have experienced;
- To acknowledge and normalize that head trauma, strangulation, and mental health struggles are common experiences among domestic violence survivors and recognize that ongoing education and self-care are necessary for advocates;
- To provide a more holistic approach to trauma-informed care through accommodations within services and referrals to other safety, health, justice, and social service systems so survivors can better access and benefit from services, and self-advocate, often by directly using the CARE Tools.
4.4. The Brain Injury from Violence CARE Alliance: Adapting CARE with the Community
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McGee, R.; Petitt, J. Power, Empowerment and Social Change, 1st ed.; Routledge: London, UK, 2019. [Google Scholar] [CrossRef]
- Collins, P.H. On violence, intersectionality and transversal politics. Ethn. Racial Stud. 2017, 40, 1460–1473. [Google Scholar] [CrossRef]
- Cudd, A.E. 85 Violence as a Force of Oppression. In Analyzing Oppression; Cudd, A.E., Ed.; Oxford University Press: Oxford, UK, 2006. [Google Scholar] [CrossRef]
- World Health Organization. Violence against Women Prevalence Estimates, 2018: Global, Regional and National Prevalence Estimates for Intimate Partner Violence against Women and Global and Regional Prevalence Estimates for Non-Partner Sexual Violence Against Women. World Health Organization: Geneva, Switzerland, 2021. Available online: https://iris.who.int/handle/10665/341337 (accessed on 9 August 2024).
- Sardinha, L.; Maheu-Giroux, M.; Stöckl, H.; Meyer, S.R.; García-Moreno, C. Global, regional, and national prevalence estimates of physical or sexual, or both, intimate partner violence against women in 2018. Lancet 2022, 399, 803–813. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Violence Info: Intimate Partner Violence 1979 Studies. Available online: https://apps.who.int/violence-info/intimate-partner-violence/ (accessed on 4 September 2024).
- Menakem, R. My Grandmother’s Hands: Racialized Trauma and the Pathway to Mending Our Hearts and Bodies. Available online: https://centralrecoverypress.com/product/my-grandmothers-hands-racialized-trauma-and-the-pathway-to-mending-our-hearts-and-bodies-paperback (accessed on 9 August 2024).
- Leemis, R.W.; Friar, N.; Khatiwada, S.; Chen, M.S.; Kresnow, M.J.; Smith, S.G.; Caslin, S.; Basile, K.C. The National Intimate Partner and Sexual Violence Survey: 2016/2017 Report on Intimate Partner Violence. Available online: https://www.cdc.gov/nisvs/documentation/NISVSReportonIPV_2022.pdf (accessed on 9 August 2024).
- Sheridan, D.J.; Nash, K.R. Acute injury patterns of intimate partner violence victims. Trauma Violence Abus. 2007, 8, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Perciaccante, V.J.; Ochs, H.A.; Dodson, T.B. Head, neck, and facial injuries as markers of domestic violence in women. J. Oral Maxillofac. Surg. 1999, 57, 760–762; discussion 762–763. [Google Scholar] [CrossRef]
- Muelleman, R.L.; Lenaghan, P.A.; Pakieser, R.A. Battered women: Injury locations and types. Ann. Emerg. Med. 1996, 28, 486–492. [Google Scholar] [CrossRef]
- Berwick, D.; Bowman, K.; Matney, C. (Eds.) Traumatic Brain Injury: A Roadmap for Accelerating Progress; National Academies Press: Washington, DC, USA, 2022. [Google Scholar] [CrossRef]
- Lacerte, M.; Hays Shapshak, A.; Mesfin, F.B. Hypoxic Brain Injury. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024; Available online: http://www.ncbi.nlm.nih.gov/books/NBK537310/ (accessed on 29 May 2024).
- Silverberg, N.D.; Iverson, G.L.; ACRM Brain Injury Special Interest Group Mild TBI Task Force members; Cogan, A.; Dams-O-Connor, K.; Delmonico, R.; Graf, M.J.P.; Iaccarino, M.A.; Kajankova, M.; Kamins, J.; et al. The American Congress of Rehabilitation Medicine Diagnostic Criteria for Mild Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2023, 104, 1343–1355. [Google Scholar] [CrossRef]
- Mckee, A.C.; Daneshvar, D.H. The neuropathology of traumatic brain injury. Handb. Clin. Neurol. 2015, 127, 45–66. [Google Scholar] [CrossRef]
- Jackson, J.E.; Beres, A.L.; Theodorou, C.M.; Ugiliweneza, B.; Boakye, M.; Nuño, M. Long-term impact of abusive head trauma in young children: Outcomes at 5 and 11 years old. J. Pediatr. Surg. 2021, 56, 2318–2325. [Google Scholar] [CrossRef]
- Jang, S.H. Diagnostic Problems in Diffuse Axonal Injury. Diagnostics 2020, 10, 117. [Google Scholar] [CrossRef]
- Medicherla, C.B.; Lewis, A. The critically ill brain after cardiac arrest. Ann. N. Y. Acad. Sci. 2022, 1507, 12–22. [Google Scholar] [CrossRef]
- Busl, K.M.; Greer, D.M. Hypoxic-ischemic brain injury: Pathophysiology, neuropathology and mechanisms. NeuroRehabilitation 2010, 26, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Budd, S.L. Mechanisms of neuronal damage in brain hypoxia/ischemia: Focus on the role of mitochondrial calcium accumulation. Pharmacol. Ther. 1998, 80, 203–229. [Google Scholar] [CrossRef] [PubMed]
- Monahan, K.; O’Leary, K.D. Head injury and battered women: An initial inquiry. Health Soc. Work. 1999, 24, 269–278. [Google Scholar] [CrossRef]
- Taliaferro, E.; Mills, T.; Walker, S. Walking and talking victims of strangulation. is there a new epidemic? a commentary 1 1 Violence: Recognition, Management, and Prevention is coordinated by Ellen Taliaferro, md, of the University of Texas Southwestern Medical School, Dallas, Texas. J. Emerg. Med. 2001, 21, 293–295. [Google Scholar] [CrossRef]
- Strack, G.B.; McClane, G.E.; Hawley, D. A review of 300 attempted strangulation cases part i: Criminal. J. Emerg. Med. 2001, 21, 303–309. [Google Scholar] [CrossRef]
- McClane, G.E.; Strack, G.B.; Hawley, D. A review of 300 attempted strangulation cases part II: Clinical evaluation of the surviving victim. J. Emerg. Med. 2001, 21, 311–315. [Google Scholar] [CrossRef]
- Hawley, D.A.; McClane, G.E.; Strack, G.B. A review of 300 attempted strangulation cases part III: Injuries in fatal cases. J. Emerg. Med. 2001, 21, 317–322. [Google Scholar] [CrossRef]
- Wilbur, L.; Higley, M.; Hatfield, J.; Surprenant, Z.; Taliaferro, E.; Smith, D.J., Jr.; Paolo, A. Survey results of women who have been strangled while in an abusive relationship. J. Emerg. Med. 2001, 21, 297–302. [Google Scholar] [CrossRef]
- Smith, D.J.; Mills, T.; Taliaferro, E.H. Frequency and relationship of reported symptomology in victims of intimate partner violence: The effect of multiple strangulation attacks. J. Emerg. Med. 2001, 21, 323–329. [Google Scholar] [CrossRef]
- Jackson, H.; Philp, E.; Nuttall, R.L.; Diller, L. Traumatic brain injury: A hidden consequence for battered women. Prof. Psychol. Res. Pract. 2002, 33, 39–45. [Google Scholar] [CrossRef]
- Corrigan, J.D.; Wolfe, M.; Mysiw, W.J.; Jackson, R.D.; Bogner, J.A. Early identification of mild traumatic brain injury in female victims of domestic violence. Am. J. Obstet. Gynecol. 2003, 188, S71–S76. [Google Scholar] [CrossRef] [PubMed]
- Valera, E.M.; Berenbaum, H. Brain injury in battered women. J. Consult. Clin. Psychol. 2003, 71, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Glass, N.; Laughon, K.; Campbell, J.; Block, C.R.; Hanson, G.; Sharps, P.W.; Taliaferro, E. Non-fatal strangulation is an important risk factor for homicide of women. J. Emerg. Med. 2008, 35, 329–335. [Google Scholar] [CrossRef]
- Laughon, K.; Renker, P.; Glass, N.; Parker, B. Revision of the Abuse Assessment Screen to Address Nonlethal Strangulation. J. Obstet. Gynecol. Neonatal Nurs. 2008, 37, 502–507. [Google Scholar] [CrossRef]
- Joshi, M.; Thomas, K.A.; Sorenson, S.B. “I didn’t know I could turn colors”: Health problems and health care experiences of women strangled by an intimate partner. Soc. Work. Health Care 2012, 51, 798–814. [Google Scholar] [CrossRef]
- Sorenson, S.B.; Joshi, M.; Sivitz, E. A systematic review of the epidemiology of nonfatal strangulation, a human rights and health concern. Am. J. Public Health 2014, 104, e54–e61. [Google Scholar] [CrossRef]
- Messing, J.T.; Thaller, J.; Bagwell, M. Factors related to sexual abuse and forced sex in a sample of women experiencing police-involved intimate partner violence. Health Soc. Work. 2014, 39, 181–191. [Google Scholar] [CrossRef]
- Messing, J.T.; Campbell, J.C.; Snider, C. Validation and adaptation of the danger assessment-5: A brief intimate partner violence risk assessment. J. Adv. Nurs. 2017, 73, 3220–3230. [Google Scholar] [CrossRef]
- Messing, J.T.; Patch, M.; Wilson, J.S.; Kelen, G.D.; Campbell, J. Differentiating among Attempted, Completed, and Multiple Nonfatal Strangulation in Women Experiencing Intimate Partner Violence. Women’s Health Issues 2018, 28, 104–111. [Google Scholar] [CrossRef]
- Pritchard, A.J.; Reckdenwald, A.; Nordham, C. Nonfatal Strangulation as Part of Domestic Violence: A Review of Research. Trauma Violence Abus. 2017, 18, 407–424. [Google Scholar] [CrossRef]
- Patch, M.; Anderson, J.C.; Campbell, J.C. Injuries of Women Surviving Intimate Partner Strangulation and Subsequent Emergency Health Care Seeking: An Integrative Evidence Review. J. Emerg. Nurs. 2018, 44, 384–393. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, M.; Strack, G.B. Recognition and Documentation of Strangulation Crimes: A Review. JAMA Otolaryngol.-Head Neck Surg. 2016, 142, 891–897. [Google Scholar] [CrossRef]
- Amoroso, T.; Iverson, K.M. Acknowledging the Risk for Traumatic Brain Injury in Women Veterans. J. Nerv. Ment. 2017, 205, 318. [Google Scholar] [CrossRef]
- Brown, J.; Clark, D.; Pooley, A.E. Exploring the Use of Neurofeedback Therapy in Mitigating Symptoms of Traumatic Brain Injury in Survivors of Intimate Partner Violence. J. Aggress. Maltreatment Trauma 2019, 28, 764–783. [Google Scholar] [CrossRef]
- Iverson, K.M.; Dardis, C.M.; Grillo, A.R.; Galovski, T.E.; Pogoda, T.K. Associations between traumatic brain injury from intimate partner violence and future psychosocial health risks in women. Compr. Psychiatry 2019, 92, 13–21. [Google Scholar] [CrossRef]
- Patch, M.; Farag, Y.M.K.; Anderson, J.C.; Perrin, N.; Kelen, G.; Campbell, J.C. United States ED Visits by Adult Women for Nonfatal Intimate Partner Strangulation, 2006 to 2014: Prevalence and Associated Characteristics. J. Emerg. Nurs. 2021, 47, 437–448. [Google Scholar] [CrossRef]
- Valera, E.M. Increasing Our Understanding of an Overlooked Public Health Epidemic: Traumatic Brain Injuries in Women Subjected to Intimate Partner Violence. J. Women’s Health 2018, 27, 735–736. [Google Scholar] [CrossRef]
- Campbell, J.C.; Anderson, J.C.; McFadgion, A.; Gill, J.; Zink, E.; Patch, M.; Callwood, G.; Campbell, D. The Effects of Intimate Partner Violence and Probable Traumatic Brain Injury on Central Nervous System Symptoms. J Women’s Health 2018, 27, 761–767. [Google Scholar] [CrossRef]
- Haag, H.L.; Sokoloff, S.; MacGregor, N.; Broekstra, S.; Cullen, N.; Colantonio, A. Battered and Brain Injured: Assessing Knowledge of Traumatic Brain Injury Among Intimate Partner Violence Service Providers. J. Women’s Health 2019, 28, 990–996. [Google Scholar] [CrossRef]
- Edwards, C. Partner Inflicted Brain Injury as a Consequence of Intimate Partner Violence. Master’s Thesis, University of Pittsburgh, Pittsburgh, PA, USA, 2017. [Google Scholar]
- Valera, E.M.; Cao, A.; Pasternak, O.; Shenton, M.E.; Kubicki, M.; Makris, N.; Adra, N. White Matter Correlates of Mild Traumatic Brain Injuries in Women Subjected to Intimate-Partner Violence: A Preliminary Study. J. Neurotrauma 2019, 36, 661–668. [Google Scholar] [CrossRef]
- Banks, M.E. Overlooked but critical: Traumatic brain injury as a consequence of interpersonal violence. Trauma Violence Abus. 2007, 8, 290–298. [Google Scholar] [CrossRef] [PubMed]
- Baxter, K.; Hellewell, S.C. Traumatic Brain Injury within Domestic Relationships: Complications, Consequences and Contributing Factors. J. Aggress. Maltreatment Trauma 2019, 28, 660–676. [Google Scholar] [CrossRef]
- Hunnicutt, G.; Murray, C.; Lundgren, K.; Crowe, A.; Olson, L. Exploring Correlates of Probable Traumatic Brain Injury among Intimate Partner Violence Survivors. J. Aggress. Maltreatment Trauma 2019, 28, 677–694. [Google Scholar] [CrossRef]
- Goldin, Y.; Haag, H.L.; Trott, C.T. Screening for History of Traumatic Brain Injury Among Women Exposed to Intimate Partner Violence. PM R. 2016, 8, 1104–1110. [Google Scholar] [CrossRef]
- Zieman, G.; Bridwell, A.; Cárdenas, J.F. Traumatic Brain Injury in Domestic Violence Victims: A Retrospective Study at the Barrow Neurological Institute. J. Neurotrauma 2017, 34, 876–880. [Google Scholar] [CrossRef]
- Crowe, A.; Murray, C.E.; Mullen, P.R.; Lundgren, K.; Hunnicutt, G.; Olson, L. Help-Seeking Behaviors and Intimate Partner Violence-Related Traumatic Brain Injury. Violence Gend. 2019, 6, 64–71. [Google Scholar] [CrossRef]
- Kabat, H.; Anderson, J.P. Acute Arrest of Cerebral Circulation in Man: Lieutenant Ralph Rossen (MC), U.S.N.R. AMA Arch. Neurol. Psychiatry 1943, 50, 510–528. [Google Scholar] [CrossRef]
- Bichard, H.; Byrne, C.; Saville, C.W.N.; Coetzer, R. The neuropsychological outcomes of non-fatal strangulation in domestic and sexual violence: A systematic review. Neuropsychol. Rehabil. 2022, 32, 1164–1192. [Google Scholar] [CrossRef]
- Valera, E.M.; Daugherty, J.C.; Scott, O.; Berenbaum, H. Strangulation as an acquired brain injury in intimate-partner violence and its relationship to cognitive and psychological functioning: A preliminary study. J. Head Trauma Rehabil. 2022, 37, 15–23. [Google Scholar] [CrossRef]
- Adhikari, S.P.; Daugherty, J.C.; Quiroz Molinares, N.; Maldonado-Rodriguez, N.; Wallace, C.; Smirl, J.; Perez-García, M.; De Los Reyes-Aragón, C.J.; Hidalgo-Ruzzante, N.; van Donkelaar, P.; et al. A Four-Country Study of Strangulation-Related Alterations in Consciousness in Women Who Have Experienced Intimate Partner Violence: Co-Occurrence with Traumatic Brain Injuries and Measures of Psychological Distress. J. Neurotrauma 2024, 41, e1666–e1677. [Google Scholar] [CrossRef]
- Nemeth, J.M.; Mengo, C.; Kulow, E.; Brown, A.; Ramirez, R. Provider Perceptions and Domestic Violence (DV) Survivor Experiences of Traumatic and Anoxic-Hypoxic Brain Injury: Implications for DV Advocacy Service Provision. J. Aggress. Maltreatment Trauma 2019, 28, 744–763. [Google Scholar] [CrossRef]
- Nemeth, J.; Ramirez, R.; Debowski, C.; Kulow, E.; Hinton, A.; Wermert, A.; Mengo, C.; Malecki, A.; Glasser, A.; Montgomery, L.; et al. The CARE Health Advocacy Intervention Improves Trauma-Informed Practices at Domestic Violence Service Organizations to Address Brain Injury, Mental Health, and Substance Use. J. Head Trauma Rehabil. 2023, 38, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.K.; Joseph, A.L.C.; Rothman, E.F.; Valera, E.M. The Prevalence of Brain Injury Among Survivors and Perpetrators of Intimate Partner Violence and the Prevalence of Violence Victimization and Perpetration Among People with Brain Injury: A Scoping Review. Curr. Epidemiol. Rep. 2022, 9, 290–315. [Google Scholar] [CrossRef]
- Lansdell, G.T.; Saunders, B.J.; Eriksson, A.; Bunn, R. Strengthening the Connection Between Acquired Brain Injury (ABI) and Family Violence: The Importance of Ongoing Monitoring, Research and Inclusive Terminology. J. Fam. Violence 2022, 37, 367–380. [Google Scholar] [CrossRef]
- Maloney-Wilensky, E.; Gracias, V.; Itkin, A.; Hoffman, K.; Bloom, S.; Yang, W.; Christian, S.; LeRoux, P.D. Brain tissue oxygen and outcome after severe traumatic brain injury: A systematic review. Crit. Care Med. 2009, 37, 2057–2063. [Google Scholar] [CrossRef]
- Cullen, N.K.; Weisz, K. Cognitive correlates with functional outcomes after anoxic brain injury: A case-controlled comparison with traumatic brain injury. Brain Inj. 2011, 25, 35–43. [Google Scholar] [CrossRef]
- Kowalski, R.G.; Haarbauer-Krupa, J.K.; Bell, J.M.; Corrigan, J.D.; Hammond, F.M.; Torbey, M.T.; Hofmann, M.C.; Dams-O’Connor, K.; Miller, A.C.; Whiteneck, G.G. Acute Ischemic Stroke After Moderate to Severe Traumatic Brain Injury: Incidence and Impact on Outcome. Stroke 2017, 48, 1802–1809. [Google Scholar] [CrossRef]
- Lutgendorf, M.A. Intimate Partner Violence and Women’s Health. Obstet. Gynecol. 2019, 134, 470–480. [Google Scholar] [CrossRef]
- Brainkind. Too Many to Count…Brain Injury in the Context of Domestic Abuse. Published Online 2024. Available online: https://brainkind.org/too-many-to-count/form/ (accessed on 2 September 2024).
- Nemeth, J.M.; Glasser, A.M.; Hinton, A.; Macisco, J.M.; Wermert, A.; Smith, R.; Kemble, H.; Sasser, G. Brain Injury Is Prevalent and Precedes Tobacco Use among Youth and Young Adults Experiencing Homelessness. Int. J. Environ. Res. Public Health 2023, 20, 5169. [Google Scholar] [CrossRef]
- Petering, R.; Wenzel, S.; Winetrobe, H. Systematic Review of Current Intimate Partner Violence Prevention Programs and Applicability to Homeless Youth. J. Soc. Soc. Work. Res. 2014, 5, 107–135. [Google Scholar] [CrossRef]
- Tyler, K.A.; Whitbeck, L.B.; Hoyt, D.R.; Cauce, A.M. Risk factors for sexual victimization among male and female homeless and runaway youth. J. Interpers. Violence 2004, 19, 503–520. [Google Scholar] [CrossRef] [PubMed]
- Slesnick, N.; Erdem, G.; Collins, J.; Patton, R.; Buettner, C. Prevalence of Intimate Partner Violence Reported by Homeless Youth in Columbus, Ohio. J. Interpers. Violence 2010, 25, 1579–1593. [Google Scholar] [CrossRef] [PubMed]
- Kemble, H.; Sucaldito, A.; Kulow, E.; Ramirez, R.; Hinton, A.; Glasser, A.; Wermert, A.; Nemeth, J.M. How CARE Tools Are Being Used to Address Brain Injury and Mental Health Struggles with Survivors of Domestic Violence. J. Head Trauma Rehabil. 2022, 37, E39–E47. [Google Scholar] [CrossRef]
- Sucaldito, A.D.; Kemble, H.; Kulow, E.; Ramirez, R.; Nemeth, J.M. How Advocates Use CARE to Accommodate the Needs of Domestic Violence Survivors Seeking Services with Brain Injuries and Mental Health Challenges: A Process Evaluation. Violence Against Women, 2025; 31, 738–749. [Google Scholar] [CrossRef]
- Silverberg, N.D.; Duhaime, A.C.; Iaccarino, M.A. Mild Traumatic Brain Injury in 2019-2020. JAMA 2020, 323, 177–178. [Google Scholar] [CrossRef]
- McCrory, P.; Meeuwisse, W.; Dvorak, J.; Aubry, M.; Bailes, J.; Broglio, S.; Cantu, R.C.; Cassidy, C.; Echemendia, R.J.; Castellani, R.J.; et al. Consensus statement on concussion in sport—The 5th international conference on concussion in sport held in Berlin, October 2016. Br. J. Sports Med. 2017, 51, 838–847. [Google Scholar] [CrossRef]
- Ayton, D.; Pritchard, E.; Tsindos, T. Acquired Brain Injury in the Context of Family Violence: A Systematic Scoping Review of Incidence, Prevalence, and Contributing Factors. Trauma Violence Abus. 2021, 22, 3–17. [Google Scholar] [CrossRef]
- Pritchard, E.; Tsindos, T.; Ayton, D. Practitioner perspectives on the nexus between acquired brain injury and family violence. Health Soc. Care Community 2019, 27, 1283–1294. [Google Scholar] [CrossRef]
- Monahan, K. Intimate Partner Violence (IPV) and Neurological Outcomes: A Review for Practitioners. J. Aggress. Maltreatment Trauma 2019, 28, 807–825. [Google Scholar] [CrossRef]
- US Department of Justice, Office on Violence Against Women. A National Protocol for Intimate Partner Violence Medical Forensic Examinations. Published Online May 2023. Available online: https://www.safeta.org/wp-content/uploads/2023/05/IPVMFEProtocol.pdf (accessed on 4 May 2025).
- Nemeth, J.M.; Ramirez, R. Ohio Domestic Violence Network. CARE CHATS Tool and Advocate Guide. Published online 2018. Available online: https://www.odvn.org/brain-injury/ (accessed on 10 August 2024).

{kind=link}
{kind=link}
| Sample Characteristics (Study Location: Ohio, U.S.). | ||
|---|---|---|
| Service-Seeking IPV Survivors (n = 47) | ||
| Age (mean, SD) [n = 43] | 38.32 | 11.26 |
| Highest grade level (n, %) [n = 46] | ||
| Less than high school | 6 | 13.04 |
| High school diploma/GED | 17 | 36.96 |
| Some college | 11 | 23.91 |
| Associate degree or higher | 12 | 26.09 |
| Current health insurance coverage (n, %) [n = 47] | ||
| None | 8 | 17.02 |
| Medicaid | 20 | 42.55 |
| Other | 19 | 40.43 |
| Lifetime Strangulation and Intentional Head Trauma—All Sources: Exposure, Medical Care, and Brain Injury Diagnosis. | ||
|---|---|---|
| 2.A. Intentional Strangulation–All Sources (e.g., partner, sibling, and peer) * | ||
| How many times in your life have you ever been choked or strangled? (n, %) [n = 47] | ||
| Never | 8 | 17.02 |
| Once | 5 | 10.64 |
| A few times | 18 | 38.30 |
| Too many times to remember | 16 | 34.04 |
| [Among those with lifetime strangulation exposure] have you ever sought medical services after being choked or strangled? (n, %) [n = 39] | ||
| Never | 28 | 71.79 |
| Once | 5 | 12.82 |
| A few times | 4 | 10.26 |
| Too many times to remember | 2 | 5.13 |
| [Among those with lifetime strangulation exposure] how many times have you been diagnosed with a brain injury resulting from being choked or strangled? (n, %) [n = 38] | ||
| Never | 32 | 84.21 |
| Once | 4 | 10.53 |
| A few times | 2 | 5.26 |
| Too many times to remember | 0 | 0.00 |
| Table note. (*) = Due to a skip pattern error, we are not presenting data on who has committed intentional strangulation, asked as the second question in series 2.A. | ||
| 2.B. Intentionally Inflicted Head Trauma—All Sources ** | ||
| How many times in your life have you ever been hit in the head or were made to have your head hit another object? (n, %) [n = 47] | ||
| Never | 6 | 12.77 |
| Once | 5 | 10.64 |
| A few times | 13 | 27.66 |
| Too many times to remember | 23 | 48.94 |
| [Among those with lifetime exposure to intentional head trauma] have you ever sought medical services after you were hit in the head or were made to have your head hit another object? (n, %) [n = 41] | ||
| Never | 22 | 53.66 |
| Once | 9 | 21.95 |
| A few times | 6 | 14.63 |
| Too many times to remember | 4 | 9.76 |
| [Among those who sought medical services] did you receive a concussion screening or neurological exam when you sought medical services? (n, %) [n = 18] | ||
| No | 1 | 5.56 |
| Yes | 17 | 94.44 |
| [Among those with lifetime exposure to intentional head trauma] how many times have you been diagnosed with a concussion or brain injury resulting from being hit in the head or having your head hit another object? (n, %) [n = 41] | ||
| Never | 24 | 58.54 |
| Once | 7 | 17.07 |
| A few times | 6 | 14.63 |
| Too many times to remember | 2 | 4.88 |
| Do not know | 2 | 4.88 |
| Table note. (**) = Due to a skip pattern error, we are not presenting data on who has committed intentional head trauma, originally asked as the second question in series 2.B. | ||
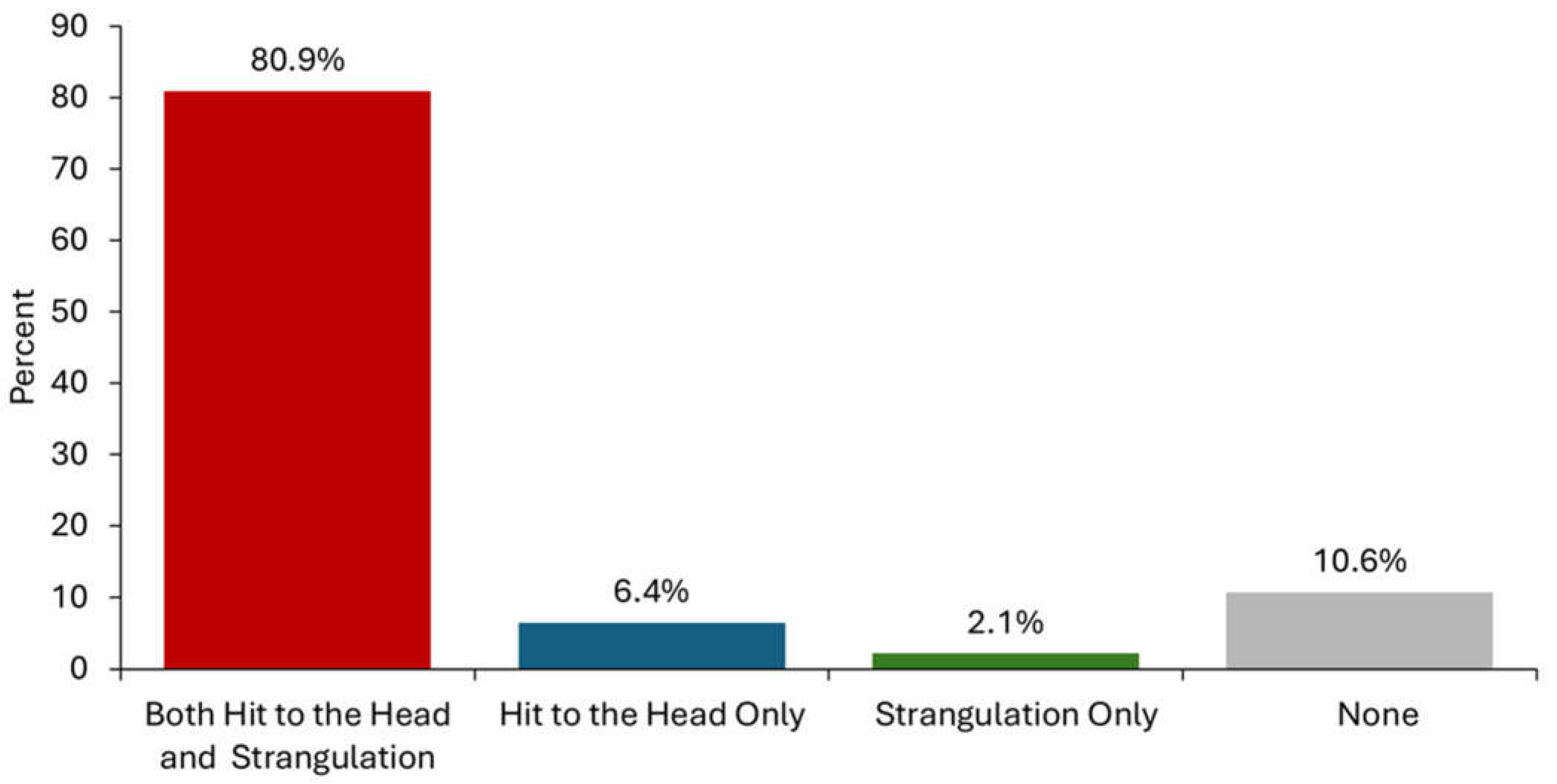
| 2.C. Lifetime Exposures to Events That Can Cause Brain Injury from Violence (BI-V) —All Sources (n, %) [n = 47] | ||
| None | 5 | 10.64 |
| Strangulation Only | 1 | 2.13 |
| Intentional Head Trauma Only | 3 | 6.38 |
| Both Strangulation and Intentional Head Trauma | 38 | 80.85 |
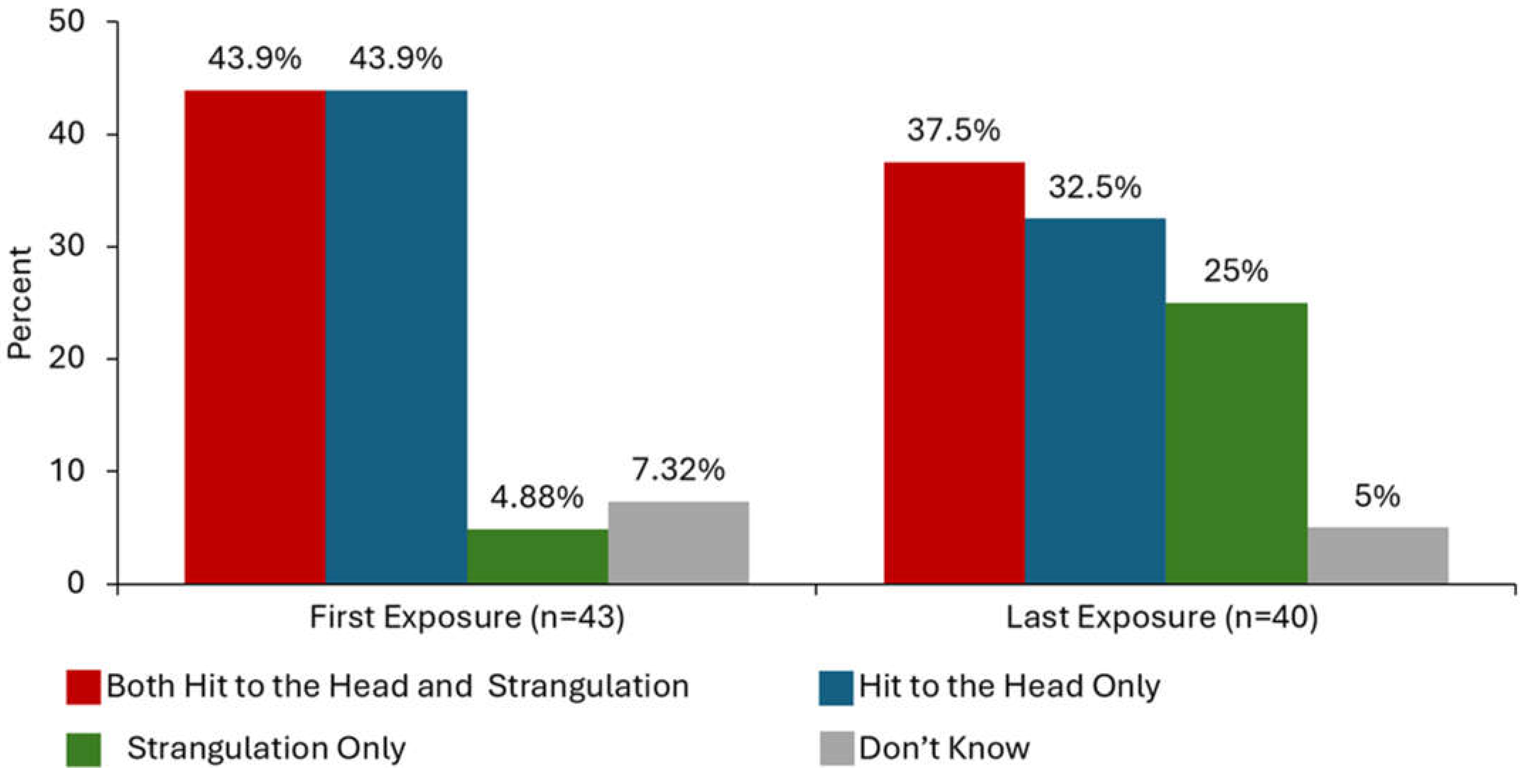
| Partner-Inflicted Head Trauma and Strangulation—First and Last Exposure. | ||
|---|---|---|
| First Exposure to Partner-Inflicted Head Trauma and Strangulation (n, %) [n = 41] | ||
| Hit in the head only | 10 | 24.39 |
| Hit once in the head and choked or strangled at the same time | 7 | 17.07 |
| Hit multiple times in the head only | 8 | 19.51 |
| Hit multiple times in the head and choked or strangled at the same time | 11 | 26.83 |
| Choked or strangled only | 2 | 4.88 |
| Do not know | 3 | 7.32 |
| Age of First Exposure (mean, SD) [n = 38] | ||
| 23.11 | 8.18 | |
| Last Exposure to Partner-Inflicted Head Trauma and Strangulation (n, %) [n = 40] | ||
| Hit in the head only | 7 | 17.50 |
| Hit once in the head and choked or strangled at the same time | 4 | 10.00 |
| Hit multiple times in the head only | 6 | 15.00 |
| Hit multiple times in the head and choked or strangled at the same time | 11 | 27.50 |
| Choked or strangled only | 10 | 25.00 |
| Do not know | 2 | 5.00 |
| Age of Last Exposure (mean, SD) [n = 37] | ||
| 34.73 | 10.39 | |
| Co-Occurrence of Head Trauma and Strangulation by an Intimate Partner During First and/or Last Exposure When the Head or Airway was Targeted (n, %) [n = 45] | ||
| 22 | 48.89 | |
| Brain Injury Severity Assessment (BISA)—Measuring Loss of and Alteration in Consciousness to Assess Probable PIBI Among Service-Seeking Survivors * | ||
| Now I Want You to Think About Times When Your Current or Former Partner Hit Your Head or Strangled You. | Survivors | |
| n | % | |
| After anything your partner has ever done to you, did you ever: Black out or lose consciousness? [n = 45] | ||
| Never | 17 | 37.78 |
| Once | 8 | 17.78 |
| A few times | 14 | 31.11 |
| Too many times to remember | 6 | 13.33 |
| Feel dazed or confused or disoriented? [n = 44] | ||
| Never | 10 | 22.73 |
| Once | 3 | 6.82 |
| A few times | 17 | 38.64 |
| Too many times to remember | 14 | 31.82 |
| Have memory loss about what happened? [n = 45] | ||
| Never | 14 | 31.11 |
| Once | 5 | 11.11 |
| A few times | 18 | 40.00 |
| Too many times to remember | 8 | 17.78 |
| See stars or spots? [n = 44] | ||
| Never | 11 | 25.00 |
| Once | 3 | 6.82 |
| A few times | 18 | 40.91 |
| Too many times to remember | 12 | 27.27 |
| Feel dizzy? [n = 44] | ||
| Never | 11 | 25.00 |
| Once | 5 | 11.36 |
| A few times | 17 | 38.64 |
| Too many times to remember | 11 | 25.00 |
| BISA Indicator [n = 45] | ||
| No indicator | 5 | 11.11 |
| At least one indicator | 40 | 88.89 |
| Probable PIBI [n = 45] | ||
| Loss of Consciousness (LOC) Criterion “Yes” to black out or lose consciousness | 28 | 62.22 |
| Alterations in Consciousness (AICs) Criterion “No” to black out or lose consciousness AND At least two of the below:
| 9 | 20.00 |
| Probable PIBI based on LOC or AIC Criterion | 37 | 82.22 |
| Table note. (*) = Asked of all survivors, regardless of whether they reported experiencing strangulation or direct hits to the head. | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nemeth, J.M.; Decker, C.; Ramirez, R.; Montgomery, L.; Hinton, A.; Duhaney, S.; Smith, R.; Glasser, A.; Bowman, A.; Kulow, E.; et al. Partner-Inflicted Brain Injury: Intentional, Concurrent, and Repeated Traumatic and Hypoxic Neurologic Insults. Brain Sci. 2025, 15, 524. https://doi.org/10.3390/brainsci15050524
Nemeth JM, Decker C, Ramirez R, Montgomery L, Hinton A, Duhaney S, Smith R, Glasser A, Bowman A, Kulow E, et al. Partner-Inflicted Brain Injury: Intentional, Concurrent, and Repeated Traumatic and Hypoxic Neurologic Insults. Brain Sciences. 2025; 15(5):524. https://doi.org/10.3390/brainsci15050524
Chicago/Turabian StyleNemeth, Julianna M., Clarice Decker, Rachel Ramirez, Luke Montgomery, Alice Hinton, Sharefa Duhaney, Raya Smith, Allison Glasser, Abigail (Abby) Bowman, Emily Kulow, and et al. 2025. "Partner-Inflicted Brain Injury: Intentional, Concurrent, and Repeated Traumatic and Hypoxic Neurologic Insults" Brain Sciences 15, no. 5: 524. https://doi.org/10.3390/brainsci15050524
APA StyleNemeth, J. M., Decker, C., Ramirez, R., Montgomery, L., Hinton, A., Duhaney, S., Smith, R., Glasser, A., Bowman, A., Kulow, E., & Wermert, A. (2025). Partner-Inflicted Brain Injury: Intentional, Concurrent, and Repeated Traumatic and Hypoxic Neurologic Insults. Brain Sciences, 15(5), 524. https://doi.org/10.3390/brainsci15050524