
Impact of the Anticholinergic Burden on Disease-Specific Symptoms in Parkinsonian Syndromes
 , ,
, , 
Abstract
1. Introduction
2. Methods
2.1. Participants
2.2. Anticholinergic Burden Measures
2.3. Clinical Assessments
2.4. Analyses
3. Results
3.1. Patient Characteristics
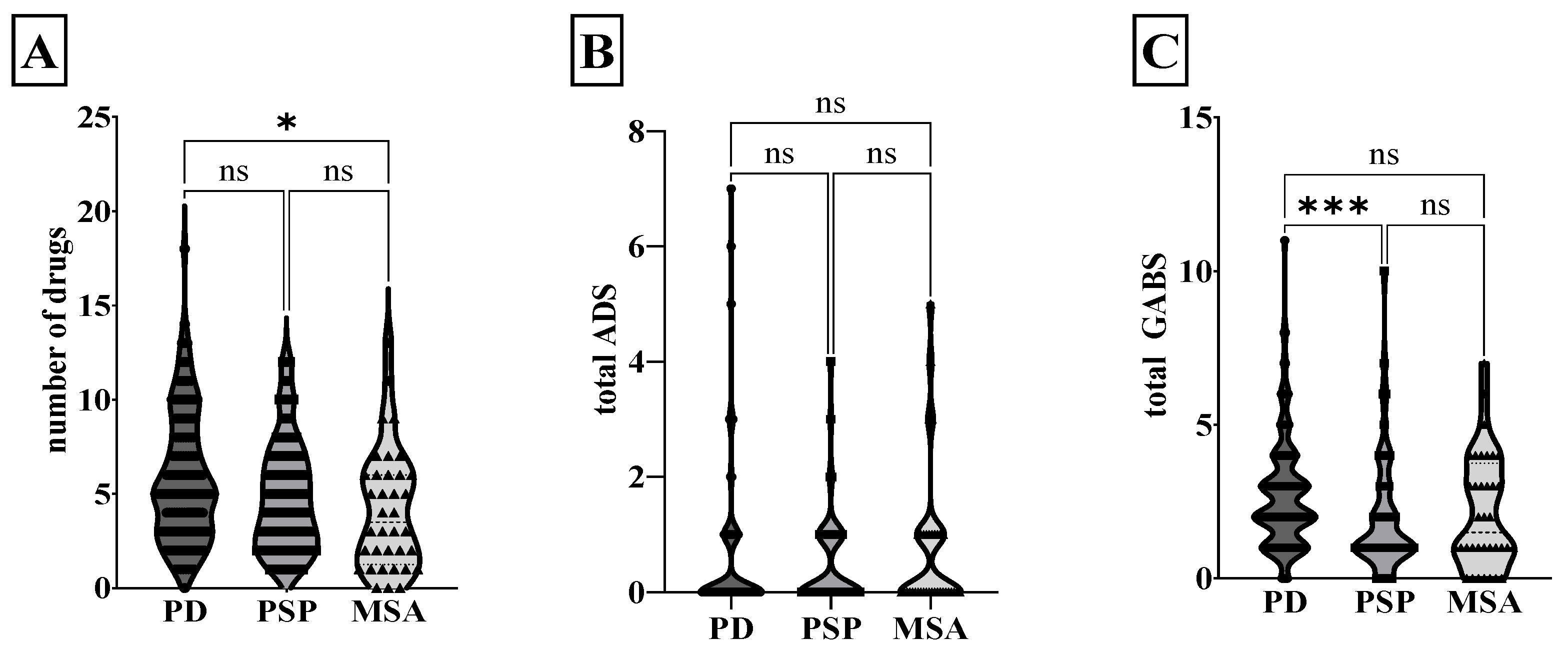
3.2. Anticholinergic Burden in Parkinsonian Syndromes
3.3. Influence of Anticholinergic Burden on Clinical Symptoms in PD
3.4. Influence of Anticholinergic Burden on Clinical Symptoms in Atypical Parkinsonian Syndromes
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lampela, P.; Paajanen, T.; Hartikainen, S.; Huupponen, R. Central Anticholinergic Adverse Effects and Their Measurement. Drugs Aging 2015, 32, 963–974. [Google Scholar] [CrossRef] [PubMed]
- Egberts, A.; Moreno-Gonzalez, R.; Alan, H.; Ziere, G.; Mattace-Raso, F.U. Anticholinergic Drug Burden and Delirium: A Systematic Review. J. Am. Med. Dir. Assoc. 2021, 22, 65–73.e4. [Google Scholar] [CrossRef] [PubMed]
- Feinberg, M. The Problems of Anticholinergic Adverse Effects in Older Patients. Drugs Aging 1993, 3, 335–348. [Google Scholar] [CrossRef] [PubMed]
- Fox, C.; Richardson, K.; Maidment, I.D.; Savva, G.M.; Matthews, F.E.; Smithard, D.; Coulton, S.; Katona, C.; Boustani, M.A.; Brayne, C. Anticholinergic Medication Use and Cognitive Impairment in the Older Population: The Medical Research Council Cognitive Function and Ageing Study. J. Am. Geriatr. Soc. 2011, 59, 1477–1483. [Google Scholar] [CrossRef] [PubMed]
- Ancelin, M.L.; Artero, S.; Portet, F.; Dupuy, A.-M.; Touchon, J.; Ritchie, K. Non-degenerative mild cognitive impairment in elderly people and use of anticholinergic drugs: Longitudinal cohort study. BMJ 2006, 332, 455–459. [Google Scholar] [CrossRef] [PubMed]
- Klietz, M.; Greten, S.; Wegner, F.; Höglinger, G.U. Safety and Tolerability of Pharmacotherapies for Parkinson’s Disease in Geriatric Patients. Drugs Aging 2019, 36, 511–530. [Google Scholar] [CrossRef]
- Gerretsen, P.; Pollock, B.G. Rediscovering Adverse Anticholinergic Effects. J. Clin. Psychiatry 2011, 72, 869–870. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Bali, V.; Carnahan, R.M.; Chen, H.; Johnson, M.L.; Aparasu, R.R. Anticholinergic burden and risk of cognitive impairment in elderly nursing home residents with depression. Res. Soc. Adm. Pharm. 2020, 16, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Lampela, P.; Lavikainen, P.; Garcia-Horsman, J.A.; Bell, J.S.; Huupponen, R.; Hartikainen, S. Anticholinergic Drug Use, Serum Anticholinergic Activity, and Adverse Drug Events Among Older People: A Population-Based Study. Drugs Aging 2013, 30, 321–330. [Google Scholar] [CrossRef]
- Tysnes, O.-B.; Storstein, A. Epidemiology of Parkinson’s disease. J. Neural Transm. Vienna Austria 1996 2017, 124, 901–905. [Google Scholar] [CrossRef]
- Respondek, G.; Stamelou, M.; Kurz, C.; Ferguson, L.W.; Rajput, A.; Chiu, W.Z.; van Swieten, J.C.; Troakes, C.; al Sarraj, S.; Gelpi, E.; et al. The phenotypic spectrum of progressive supra-nuclear palsy: A retrospective multicenter study of 100 definite cases. Mov. Disord. Off. J. Mov. Disord. Soc. 2014, 29, 1758–1766. [Google Scholar] [CrossRef] [PubMed]
- Poewe, W.; Stankovic, I.; Halliday, G.; Meissner, W.G.; Wenning, G.K.; Pellecchia, M.T.; Seppi, K.; Palma, J.-A.; Kaufmann, H. Multiple system atrophy. Nat. Rev. Dis. Primers 2022, 8, 56. [Google Scholar] [CrossRef] [PubMed]
- Greten, S.; Müller-Funogea, J.I.; Wegner, F.; Höglinger, G.U.; Simon, N.; Junius-Walker, U.; Gerbel, S.; Krause, O.; Klietz, M. Drug safety profiles in geriatric patients with Parkinson’s disease using the FORTA (Fit fOR The Aged) classification: Results from a mono-centric retrospective analysis. J. Neural Transm. 2021, 128, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Greten, S.; Wegner, F.; Jensen, I.; Krey, L.; Rogozinski, S.; Fehring, M.; Heine, J.; Doll-Lee, J.; Pötter-Nerger, M.; Zeitzschel, M.; et al. The comorbidity and co-medication profile of patients with progressive supranuclear palsy. J. Neurol. 2024, 271, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Ye, L.; Greten, S.; Wegner, F.; Doll-Lee, J.; Krey, L.; Heine, J.; Gandor, F.; Vogel, A.; Berger, L.; Gruber, D.; et al. The comorbidity profiles and medication issues of patients with multiple system atrophy: A systematic cross-sectional analysis. J. Neurol. 2024, 271, 2639–2648. [Google Scholar] [CrossRef]
- Okudur, S.K.; Dokuzlar, O.; Aydin, A.E.; Kocyigit, S.E.; Soysal, P.; Isik, A.T. The Evaluation of Relationship Between Polypharmacy and Anticholinergic Burden Scales. North. Clin. Istanb. 2021, 8, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Wong, H.L.; Weaver, C.; Marsh, L.; Mon, K.O.; Dapito, J.M.; Amin, F.R.; Chauhan, R.; Mandal, A.K.J.; Missouris, C.G. Polypharmacy and cumulative anticholinergic burden in older adults hospitalized with fall. Aging Med. 2023, 6, 116–123. [Google Scholar] [CrossRef]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS clinical diagnostic criteria for Parkinson’s disease: MDS-PD Clinical Diagnostic Criteria. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef] [PubMed]
- Höglinger, G.U.; Respondek, G.; Stamelou, M.; Kurz, C.; Josephs, K.A.; Lang, A.E.; Mollenhauer, B.; Müller, U.; Nilsson, C.; Whitwel, J.L.; et al. Clinical diagnosis of progressive supranuclear palsy: The movement disorder society criteria: MDS Clinical Diagnostic Criteria for PSP. Mov. Disord. 2017, 32, 853–864. [Google Scholar] [CrossRef]
- Gilman, S.; Wenning, G.; Low, P.A.; Brooks, D.; Mathias, C.J.; Trojanowski, J.Q.; Wood, N.; Colosimo, C.; Durr, A.; Fowler, C.J.; et al. Second consensus statement on the diagnosis of multiple system atrophy. Neurology 2008, 71, 670–676. [Google Scholar] [CrossRef]
- Carnahan, R.M.; Lund, B.C.; Perry, P.J.; Pollock, B.G.; Culp, K.R. The Anticholinergic Drug Scale as a measure of drug-related anti-cholinergic burden: Associations with serum anticholinergic activity. J. Clin. Pharmacol. 2006, 46, 1481–1486. [Google Scholar] [CrossRef] [PubMed]
- Kiesel, E.K.; Hopf, Y.M.; Drey, M. An anticholinergic burden score for German prescribers: Score development. BMC Geriatr. 2018, 18, 239. [Google Scholar] [CrossRef]
- Carnahan, R.M.; Lund, B.C.; Perry, P.J.; Culp, K.R.; Pollock, B.G. The relationship of an anticholinergic rating scale with serum anti-cholinergic activity in elderly nursing home residents. Psychopharmacol. Bull. 2002, 36, 14–19. [Google Scholar] [PubMed]
- Pazan, F.; Wehling, M. Polypharmacy in older adults: A narrative review of definitions, epidemiology and consequences. Eur. Geriatr. Med. 2021, 12, 443–452. [Google Scholar] [CrossRef]
- Pont, L.G.; Nielen, J.T.H.; McLachlan, A.J.; Gnjidic, D.; Chan, L.; Cumming, R.G.; Taxis, K. Measuring anticholinergic drug exposure in older community-dwelling Australian men: A comparison of four different measures. Br. J. Clin. Pharmacol. 2015, 80, 1169–1175. [Google Scholar] [CrossRef] [PubMed]
- Ramaker, C.; Marinus, J.; Stiggelbout, A.M.; van Hilten, B.J. Systematic evaluation of rating scales for impairment and disability in Parkinson’s disease. Mov. Disord. 2002, 17, 867–876. [Google Scholar] [CrossRef] [PubMed]
- Jenkinson, C.; Peto, V.; Fitzpatrick, R.; Greenhall, R.; Hyman, N. Self-reported Functioning and Well-being in Patients with Parkin-son’s Disease: Comparison of the Short-form Health Survey (SF-36) and the Parkinson’s Disease Questionnaire (PDQ-39). Age Ageing 1995, 24, 505–509. [Google Scholar] [CrossRef] [PubMed]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Martinez-Martin, P.; Frades-Payo, B.; Agüera-Ortiz, L.; Ayuga-Martinez, A. A short Scale for Evaluation of Neuropsychiatric Dis-orders in Parkinson’s Disease: First psychometric approach. J. Neurol. 2012, 259, 2299–2308. [Google Scholar] [CrossRef]
- Wenning, G.K.; Tison, F.; Seppi, K.; Sampaio, C.; Diem, A.; Yekhlef, F.; Ghorayeb, I.; Ory, F.; Galitzky, M.; Scaravilli, T.; et al. Development and validation of the Unified Multiple System Atrophy Rating Scale (UMSARS). Mov. Disord. 2004, 19, 1391–1402. [Google Scholar] [CrossRef]
- Golbe, L.I.; Ohman-Strickland, P.A. A clinical rating scale for progressive supranuclear palsy. Brain 2007, 130, 1552–1565. [Google Scholar] [CrossRef] [PubMed]
- Nawaz, H.; Sargent, L.; Quilon, H.; Cloud, L.J.; Testa, C.M.; Snider, J.D.; Lageman, S.K.; Baron, M.S.; Berman, B.D.; Zimmerman, K.; et al. Anticholinergic Medication Burden in Parkinson’s Disease Outpatients. J. Park. Dis. 2022, 12, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Sumbul-Sekerci, B.; Bilgic, B.; Pasin, O.; Emre, M.; Hanagasi, H.A. Anticholinergic Burden, Polypharmacy, and Cognition in Par-kinson’s Disease Patients with Mild Cognitive Impairment: A Cross-Sectional Observational Study. Dement. Geriatr. Cogn. Disord. 2022, 51, 386–395. [Google Scholar] [CrossRef] [PubMed]
- Rajan, R.; Saini, A.; Verma, B.; Choudhary, N.; Gupta, A.; Vishnu, V.Y.; Bhatia, R.; Singh, M.B.; Srivastava, A.K.; Srivastava, M.V.P. Anticholinergics May Carry Significant Cognitive and Gait Burden in Parkinson’s Disease. Mov. Disord. Clin. Pract. 2020, 7, 803–809. [Google Scholar] [CrossRef]
- Crispo, J.A.G.; Willis, A.W.; Thibault, D.P.; Fortin, Y.; Hays, H.D.; McNair, D.S.; Bjerre, L.M.; Kohen, D.E.; Perez-Lloret, S.; Mattison, D.R.; et al. Associations between Anticholinergic Burden and Adverse Health Outcomes in Parkinson Disease. PLoS ONE 2016, 11, e0150621. [Google Scholar] [CrossRef]
- Pfistermeister, B.; Tümena, T.; Gaßmann, K.-G.; Maas, R.; Fromm, M.F. Anticholinergic burden and cognitive function in a large German cohort of hospitalized geriatric patients. PLoS ONE 2017, 12, e0171353. [Google Scholar] [CrossRef] [PubMed]
- Litvan, I.; Goldman, J.G.; Tröster, A.I.; Schmand, B.A.; Weintraub, D.; Petersen, R.C.; Mollenhauer, B.; Adler, C.H.; Marder, K.; Williams-Gray, C.H.; et al. Diagnostic criteria for mild cognitive im-pairment in Parkinson’s disease: Movement Disorder Society Task Force guidelines. Mov. Disord. Off. J. Mov. Disord. Soc. 2012, 27, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Zia, A.; Kamaruzzaman, S.; Myint, P.K.; Tan, M. Anticholinergic burden is associated with recurrent and injurious falls in older individuals. Maturitas 2016, 84, 32–37. [Google Scholar] [CrossRef]
- Stewart, C.; Taylor-Rowan, M.; Soiza, R.L.; Quinn, T.J.; Loke, Y.K.; Myint, P.K. Anticholinergic burden measures and older people’s falls risk: A systematic prognostic review. Ther. Adv. Drug Saf. 2021, 12. [Google Scholar] [CrossRef]
- Bloem, B.R.; Grimbergen, Y.A.M.; Cramer, M.; Willemsen, M.; Zwinderman, A.H. Prospective assessment of falls in Parkinson’s disease. J. Neurol. 2001, 248, 950–958. [Google Scholar] [CrossRef] [PubMed]
- Crouse, J.J.; Phillips, J.R.; Jahanshahi, M.; Moustafa, A.A. Postural instability and falls in Parkinson’s disease. Rev. Neurosci. 2016, 27, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Giagkou, N.; Höglinger, G.U.; Stamelou, M. Progressive supranuclear palsy. Int. Rev. Neurobiol. 2019, 149, 49–86. [Google Scholar] [PubMed]
- Wenning, G.K.; Ebersbach, G.; Verny, M.; Chaudhuri, K.R.; Jellinger, K.; McKee, A.; Poewe, W.; Litvan, I. Progression of falls in postmortem-confirmed Parkinsonian disorders. Mov. Disord. 1999, 14, 947–950. [Google Scholar] [CrossRef] [PubMed]
- Xie, T.; Kang, U.J.; Kuo, S.-H.; Poulopoulos, M.; Greene, P.; Fahn, S. Comparison of clinical features in pathologically confirmed PSP and MSA patients followed at a tertiary center. NPJ Park. Dis. 2015, 1, 15007. [Google Scholar] [CrossRef] [PubMed]
- Lisibach, A.; Benelli, V.; Ceppi, M.G.; Waldner-Knogler, K.; Csajka, C.; Lutters, M. Quality of anticholinergic burden scales and their impact on clinical outcomes: A systematic review. Eur. J. Clin. Pharmacol. 2021, 77, 147–162. [Google Scholar] [CrossRef] [PubMed]
- Krüger, C.; Schäfer, I.; Bussche, H.v.D.; Bickel, H.; Fuchs, A.; Gensichen, J.; König, H.-H.; Maier, W.; Mergenthal, K.; Riedel-Heller, S.G.; et al. Anticholinergic drug burden according to the anticholinergic drug scale and the German anticholinergic burden and their impact on cognitive function in multimorbid elderly German people: A multicentre observational study. BMJ Open 2021, 11, e044230. [Google Scholar] [CrossRef]
- Rudolph, J.L.; Salow, M.J.; Angelini, M.C.; McGlinchey, R.E. The Anticholinergic Risk Scale and Anticholinergic Adverse Effects in Older Persons. Arch. Intern. Med. 2008, 168, 508–513. [Google Scholar] [CrossRef]
- Naples, J.G.; Marcum, Z.A.; Perera, S.; Gray, S.L.; Newman, A.B.; Simonsick, E.M.; Yaffe, K.; Shorr, R.I.; Hanlon, J.T.; the Health, Aging and Body Composition Study. Concordance Between Anticholinergic Burden Scales. J. Am. Geriatr. Soc. 2015, 63, 2120–2124. [Google Scholar] [CrossRef]
- Brombo, G.; Bianchi, L.; Maietti, E.; Malacarne, F.; Corsonello, A.; Cherubini, A.; Ruggiero, C.; Onder, G.; Volpato, S. Association of Anticholinergic Drug Burden with Cognitive and Functional Decline Over Time in Older Inpatients: Results from the CRIME Project. Drugs Aging 2018, 35, 917–924. [Google Scholar] [CrossRef]
- Suh, Y.; Ah, Y.-M.; Han, E.; Jun, K.; Hwang, S.; Choi, K.H.; Lee, J.-Y. Dose response relationship of cumulative anticholinergic exposure with incident dementia: Validation study of Korean anticholinergic burden scale. BMC Geriatr. 2020, 20, 265. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| PD (n = 151) | PSP (n = 63) | MSA (n = 36) | |
|---|---|---|---|
| Age in years, mean ± SD | 67 ± 10.96 ** | 69.4 ± 8.5 *** | 61.9 ± 8.8 |
| Sex, female, n (%) | 63 (41.7) | 29 (46.0) | 20 (55.6) |
| Disease duration in years, mean ± SD | 6.16 ± 6.54 *** | 0.5 ± 0.9 | 1.1 ± 1.7 |
| Clinical phenotype, n (%) | |||
| PD Tremor-dominant | 23 (15.2) | ||
| PD Akinetic-rigid | 76 (50.3) | ||
| PD Equivalent | 51 (33.8) | ||
| PSP-Richardson Syndrome | 50 (79.4) | ||
| PSP non-Richardson Syndrome | 7 (11.1) | ||
| MSA-P | 19 (52.8) | ||
| MSA-C | 15 (41.7) | ||
| Missing | 1 (0.7) | 6 (9.5) | 2 (5.6) |
| Number of drugs, mean ± SD | 5.8 ± 3.4 | 4.9 ± 2.9 | 4.1 ± 3.2 * |
| Patients with polypharmacy, n (%) | 91 (60.3) | 31 (49.2) | 16 (44.4) |
| Anticholinergic exposure, ADS, n (%) | |||
| absent | 111 (73.5) | 42 (66.7) | 22 (61.1) |
| low | 30 (19.9) | 19 (30.1) | 10 (28.8) |
| high | 10 (6.6) | 2 (3.2) | 4 (11.1) |
| Anticholinergic exposure, GABS, n (%) | |||
| absent | 5 (3.3) | 8 (12.7) | 7 (19.4) |
| low | 77 (51.0) | 39 (61.9) | 14 (38.9) |
| high | 69 (45.7) | 16 (25.4) | 15 (41.7) |
| Age | Disease Duration | MoCA | UPDRS I | UPDRS II | UPDRS III | UPDRS Total | SEND-Psycho | SEND-PD Total | GDS-15 | PDQ-8 | Number of Drugs | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of drugs | 0.431 ** | 0.167 ** | −0.302 ** | 0.341 ** | 0.340 ** | 0.396 ** | 0.438 ** | 0.167 | 0.130 | 0.160 | 0.218 * | |
| ADS | 0.011 | 0.172 * | −0.108 | 0.169 | 0.169 | 0.038 | 0.134 | 0.021 | 0.111 | 0.033 | 0.046 | 0.374 ** |
| GABS | 0.133 | 0.296 ** | −0.153 | 0.357 ** | 0.344 ** | 0.248 ** | 0.374 ** | 0.267 ** | 0.262 ** | 0.156 | 0.252 ** | 0.517 ** |
| Age | Disease Duration | MoCA | PSPRS | SEND-Psycho | SEND-PD Total | GDS-15 | PDQ-8 | Number of Drugs | |
|---|---|---|---|---|---|---|---|---|---|
| Number of drugs | −0.022 | 0.064 | 0.032 | −0.066 | −0.082 | −0.2 | −0.024 | 0.147 | |
| ADS | −0.058 | 0.163 | −0.037 | −0.134 | −0.010 | 0.139 | −0.091 | 0.163 | 0.435 ** |
| GABS | −0.011 | 0.057 | −0.053 | −0.024 | −0.065 | 0.125 | −0.154 | 0.24 | 0.389 ** |
| Age | Disease Duration | MoCA | UMSARS I + II | SEND-Psycho | SEND-PD Total | GDS-15 | PDQ-8 | Number of Drugs | |
|---|---|---|---|---|---|---|---|---|---|
| Number of drugs | 0.231 | 0.151 | −0.331 | 0.327 | 0.182 | −0.012 | −0.486 ** | −0.009 | |
| ADS | 0.087 | 0.079 | −0.197 | 0.386 * | 0.074 | 0.036 | 0.062 | −0.78 | 0.442 ** |
| GABS | 0.106 | 0.349 * | −0.182 | 0.305 | 0.014 | 0.055 | −0.228 | 0.098 | 0.704 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahmoudi, R.; Greten, S.; Veith Sanches, L.; Krey, L.; Ulaganathan, S.; Höglinger, G.U.; Heck, J.; Wegner, F.; Klietz, M. Impact of the Anticholinergic Burden on Disease-Specific Symptoms in Parkinsonian Syndromes. Brain Sci. 2024, 14, 805. https://doi.org/10.3390/brainsci14080805
Mahmoudi R, Greten S, Veith Sanches L, Krey L, Ulaganathan S, Höglinger GU, Heck J, Wegner F, Klietz M. Impact of the Anticholinergic Burden on Disease-Specific Symptoms in Parkinsonian Syndromes. Brain Sciences. 2024; 14(8):805. https://doi.org/10.3390/brainsci14080805
Chicago/Turabian StyleMahmoudi, Romina, Stephan Greten, Linda Veith Sanches, Lea Krey, Sarana Ulaganathan, Günter U. Höglinger, Johannes Heck, Florian Wegner, and Martin Klietz. 2024. "Impact of the Anticholinergic Burden on Disease-Specific Symptoms in Parkinsonian Syndromes" Brain Sciences 14, no. 8: 805. https://doi.org/10.3390/brainsci14080805
APA StyleMahmoudi, R., Greten, S., Veith Sanches, L., Krey, L., Ulaganathan, S., Höglinger, G. U., Heck, J., Wegner, F., & Klietz, M. (2024). Impact of the Anticholinergic Burden on Disease-Specific Symptoms in Parkinsonian Syndromes. Brain Sciences, 14(8), 805. https://doi.org/10.3390/brainsci14080805