


Dissociation between Selecting and Orienting Attentional Reading Deficits: A Study in Adults with Epilepsy
Abstract
1. Introduction
2. Method
2.1. Participants
2.2. Word Experiment
2.2.1. Design
2.2.2. Stimuli
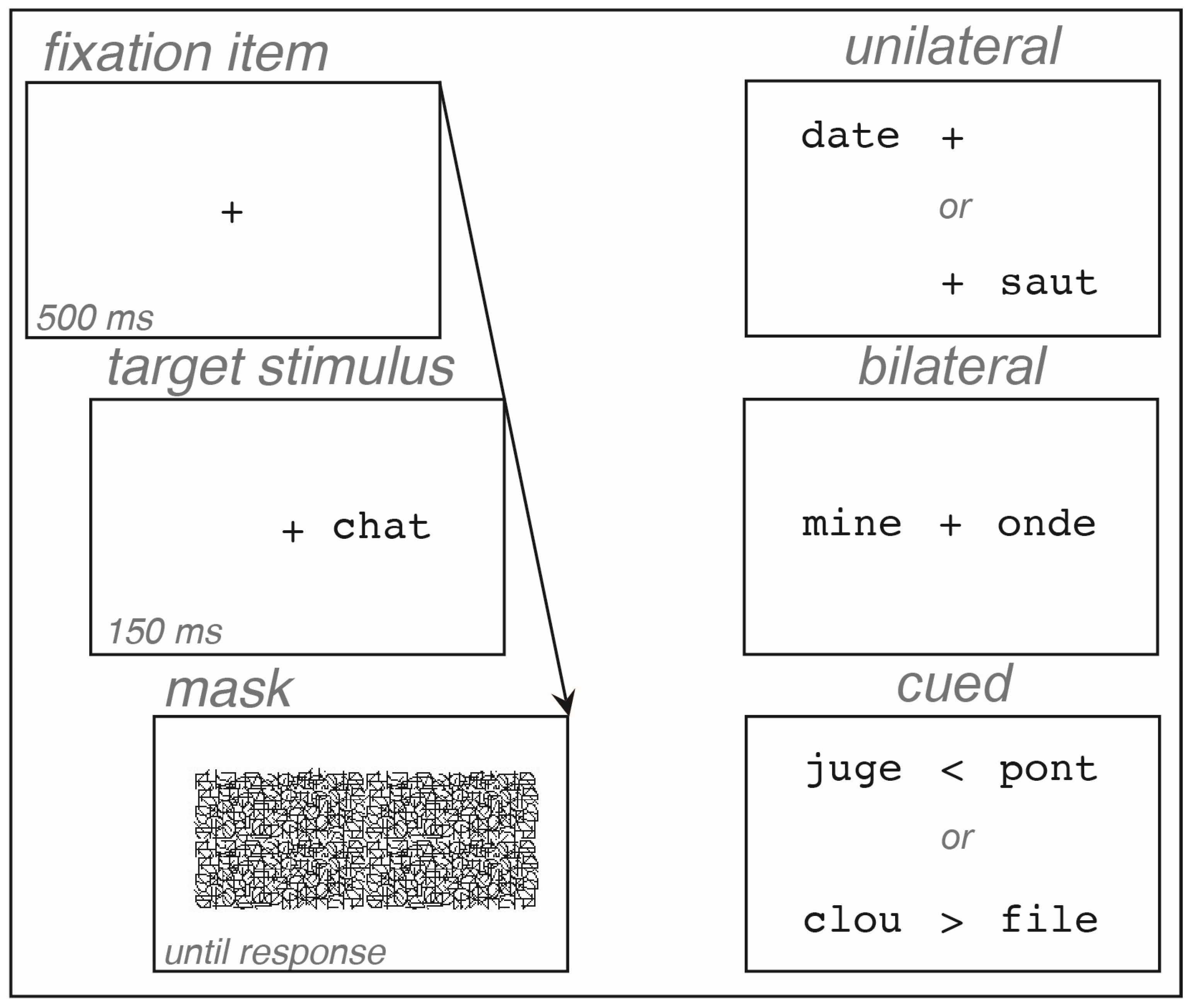
2.2.3. Procedure
2.3. Object Experiment
3. Results
3.1. Global Analyses
3.1.1. Word Experiment
3.1.2. Object Experiment
3.2. Subgroup Analyses
3.2.1. Specific Scores
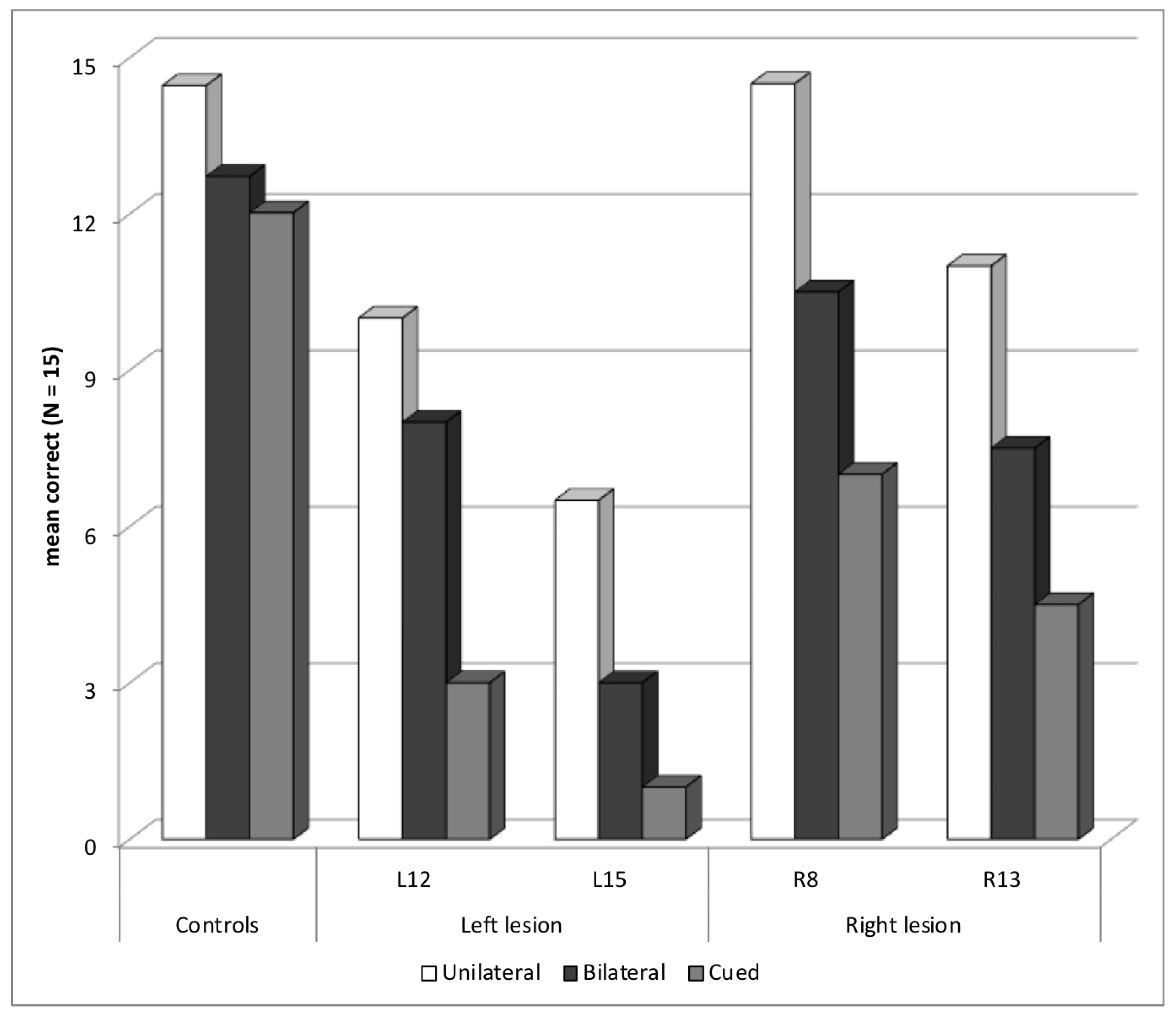
3.2.2. Selection Deficit
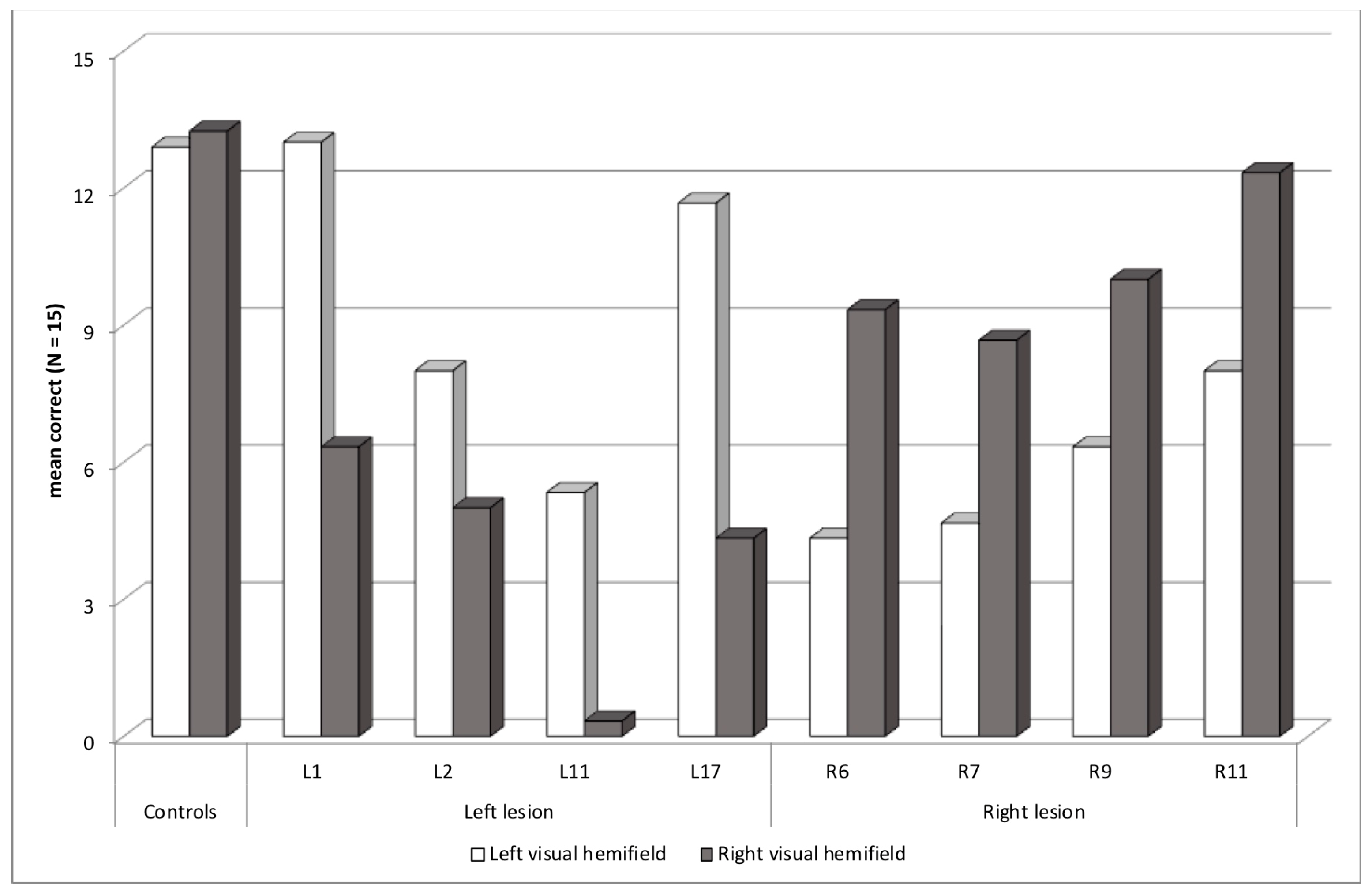
3.2.3. Abnormal Asymmetry: Contralesional Deficit
3.2.4. Abnormal Asymmetry: Ipsilesional Deficit
3.2.5. Other Deficits
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- White, A.T.; Palmer, J.; Boynton, G.M. Evidence of serial processing in visual word recognition. Psychol. Sci. 2018, 29, 1062–1071. [Google Scholar] [CrossRef] [PubMed]
- Snell, J.; Grainger, J. Readers are parallel processors. Trends Cogn. Sci. 2019, 23, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Besner, D.; Risko, E.F.; Stolz, J.A.; White, D.; Reynolds, M.; O’Malley, S.; Robidoux, S. Varieties of attention: Their roles in visual word identification. Curr. Dir. Psychol. Sci. 2016, 25, 162–168. [Google Scholar] [CrossRef]
- LaBerge, D.; Brown, V. Theory of attentional operations in shape identification. Psychol. Rev. 1989, 96, 101–124. [Google Scholar] [CrossRef]
- Wang, C.A.; Inhoff, A.W.; Radach, R. Is attention confined to one word at a time? The spatial distribution of parafoveal preview benefit during reading. Atten. Percept. Psychophys. 2009, 71, 1487–1494. [Google Scholar] [CrossRef]
- Radach, R.; Kennedy, A. Eye movements in reading: Some theoretical context. Q. J. Exp. Psychol. 2013, 66, 429–452. [Google Scholar] [CrossRef]
- Siéroff, E.; Slama, Y. Influence of script direction on word processing modes in left and right visual fields. Laterality 2018, 23, 479–500. [Google Scholar] [CrossRef]
- Siéroff, E. Acquired spatial dyslexia. Ann. Phys. Rehabil. Med. 2017, 60, 155–159. [Google Scholar] [CrossRef]
- Shallice, T.; Warrington, E.K. The possible role of selective attention in acquired dyslexia. Neuropsychologia 1977, 15, 31–41. [Google Scholar] [CrossRef]
- Shallice, T.; Rosazza, C. Patterns of peripheral paralexia: Pure alexia and the forgotten visual dyslexia? Cortex 2006, 42, 892–897. [Google Scholar] [CrossRef]
- Mayall, K.; Humphreys, G.W. Presentation and task effects on migration errors in attentional dyslexia. Neuropsychologia 2002, 40, 1506–1515. [Google Scholar] [CrossRef]
- Siéroff, E. Focusing on/in visual verbal stimuli in patients with parietal lesion. Cogn. Neuropsychol. 1990, 7, 519–554. [Google Scholar] [CrossRef]
- Rich, T.J.; Palmer, J. Neglect dyslexia: Whole-word and within-word errors with parafoveal and foveal viewing. Exp. Brain Res. 2023, 241, 2655–2668. [Google Scholar] [CrossRef]
- Siéroff, E.; Urbanski, M. Conditions of visual verbal extinction: Does the ipsilesional stimulus have to be identified? Brain Cogn. 2002, 48, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Volpe, B.T.; Ledoux, J.E.; Gazzaniga, M.S. Information processing of visual stimuli in an “extinguished” field. Nature 1979, 282, 722–724. [Google Scholar] [CrossRef] [PubMed]
- Daini, R.; Primativo, S.; Albonico, A.; Veronelli, L.; Malaspina, M.; Corbo, M.; Martelli, M.; Arduino, L.S. The focal attention window size explains letter substitution errors in reading. Brain Sci. 2021, 11, 247. [Google Scholar] [CrossRef] [PubMed]
- Weinzierl, C.; Kerkhoff, G.; van Eimeren, L.; Keller, I.; Stenneken, P. Error types and error positions in neglect dyslexia: Comparative analyses in neglect patients and healthy controls. Neuropsychologia 2012, 50, 2764–2772. [Google Scholar] [CrossRef] [PubMed]
- Ptak, R.; Di Pietro, M.; Pignat, J.M. The role of parieto-temporal connectivity in pure neglect dyslexia. Brain Res. 2016, 1648, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Vallar, G.; Burani, C.; Arduino, L.S. Neglect dyslexia: A review of the neuropsychological literature. Exp. Brain Res. 2010, 206, 219–235. [Google Scholar] [CrossRef]
- Beschin, N.; Cisari, C.; Cubelli, R.; Della Sala, S. Prose reading in neglect. Brain Cogn. 2014, 84, 69–75. [Google Scholar] [CrossRef]
- Barban, F.; Zannino, G.D.; Santangelo, V.; Macaluso, E.; Serra, L.; Caltagirone, C.; Carlesimo, G.A. Amblyopic dyslexia: A little investigated reading disorder. Neurocase 2010, 16, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Habekost, T.; Starrfelt, R. Alexia and quadrant-amblyopia: Reading disability after a minor visual field deficit. Neuropsychologia 2006, 44, 2465–2476. [Google Scholar] [CrossRef] [PubMed]
- Cohen, L.; Dehaene, S.; Naccache, L.; Lehéricy, S.; Dehaene-Lambertz, G.; Henaff, M.A.; Michel, F. The visual word form area: Spatial and temporal characterization of an initial stage of reading in normal subjects and posterior split-brain patients. Brain 2000, 123, 291–307. [Google Scholar] [CrossRef]
- Dorff, J.E.; Mirsky, A.F.; Mishkin, M. Effects of unilateral temporal lobe removals in man on tachistoscopic recognition in the left and right visual fields. Neuropsychologia 1965, 3, 39–51. [Google Scholar] [CrossRef]
- Siéroff, E.; Michel, F. Verbal visual extinction in right/left hemisphere lesion patients and the problem of lexical access. Neuropsychologia 1987, 25, 907–918. [Google Scholar] [CrossRef]
- Hunter, Z.R.; Brysbaert, M. Visual half-field experiments are a good measure of cerebral language dominance if used properly: Evidence from fMRI. Neuropsychologia 2008, 46, 316–325. [Google Scholar] [CrossRef]
- Helmstaedter, C.; Witt, J. Epilepsy and cognition: A bidirectional relationship? Seizure 2017, 49, 83–89. [Google Scholar] [CrossRef]
- Chaix, Y.; Laguitton, V.; Lauwers-Cancès, V.; Daquin, G.; Cancès, C.; Démonet, J.F.; Villeneuve, N. Reading abilities and cognitive functions of children with epilepsy: Influence of epileptic syndrome. Brain Dev. 2006, 28, 122–130. [Google Scholar] [CrossRef]
- Lah, S.; Castles, A.; Smith, M.L. Reading in children with temporal lobe epilepsy: A systematic review. Epilepsy Behav. 2017, 68, 84–94. [Google Scholar] [CrossRef]
- Vanasse, C.M.; Béland, R.; Carmant, L.; Lassonde, M. Impact of childhood epilepsy on reading and phonological processing abilities. Epilepsy Behav. 2005, 7, 288–296. [Google Scholar] [CrossRef]
- Breier, J.I.; Fletcher, J.M.; Wheless, J.W.; Clark, A.; Cass, J.; Constantinou, J.E.C. Profiles of cognitive performance associated with reading disability in temporal lobe epilepsy. J. Clin. Exp. Neuropsychol. 2000, 22, 804–816. [Google Scholar] [CrossRef]
- Auclair, L.; Jambaqué, I.; Dulac, O.; LaBerge, D.; Siéroff, E. Deficit of preparatory attention in children with frontal lobe epilepsy. Neuropsychologia 2005, 43, 1701–1712. [Google Scholar] [CrossRef]
- Gascoigne, M.B.; Smith, M.L.; Barton, B.; Webster, R.; Gill, D.; Lah, S. Attention deficits in children with epilepsy: Preliminary findings. Epilepsy Behav. 2017, 67, 7–12. [Google Scholar] [CrossRef]
- Hudson, J.M.; Flowers, K.A.; Walster, K.L. Attentional control in patients with temporal lobe epilepsy. J. Neuropsychol. 2014, 8, 140–146. [Google Scholar] [CrossRef]
- Murphy Kavros, P.; Clarke, T.; Strug, L.J.; Halperin, J.M.; Dorta, N.J.; Pal, D.K. Attention impairment in rolandic epilepsy: Systematic review. Epilepsia 2008, 49, 1570–1580. [Google Scholar] [CrossRef]
- Arduino, L.S.; Vallar, G.; Burani, C. Left neglect dyslexia and the effect of stimulus duration. Neuropsychologia 2006, 44, 662–665. [Google Scholar] [CrossRef]
- Rosen, J.F.; Curcio, F.; Mackavey, W.; Hebert, J. Superior recall of letters in the right visual field with bilateral presentation and partial report. Cortex 1975, 11, 144–154. [Google Scholar] [CrossRef]
- Mishkin, M.; Forgays, D.G. Word recognition as a function of retinal locus. J. Exp. Psychol. 1952, 43, 43–48. [Google Scholar] [CrossRef]
- Fitzgerald, R.E.; Marshall, A.J. Left-right field differences with partial report of letters. Am. J. Psychol. 1967, 80, 370–376. [Google Scholar] [CrossRef]
- Levine, S.C.; Banich, M.T. Possible effects of forced report order on tachistoscopic recognition of bilaterally presented stimuli: A response to Young and Ellis. Brain Lang. 1984, 21, 364–374. [Google Scholar] [CrossRef]
- Wechsler, D. Wechsler Adult Intelligence Scale—Fourth Edition (WAIS–IV); The Psychological Corporation: San Antonio, TX, USA, 2008. [Google Scholar]
- Lutz, M.; Helmstaedter, C. EpiTrack: Tracking cognitive side effects of medication on attention and executive functions in patients with epilepsy. Epilepsy Behav. 2005, 7, 708–714. [Google Scholar] [CrossRef]
- Bilocq, V.; de Partz, M.; De Wilde, V.; Pillon, A.; Seron, X. LEXIS: Tests for the Diagnosis of Lexical Deficits in Aphasic Patients; Solal: Paris, France, 1999. [Google Scholar]
- Jones-Gotman, M.; Zatorre, R.J.; Olivier, A.; Andermann, F.; Cendes, F.; Staunton, H.; McMackin, D.; Siegel, A.M.; Wieser, H.G. Learning and retention of words and designs following excision from medial or lateral temporal-lobe structures. Neuropsychologia 1997, 35, 963–973. [Google Scholar] [CrossRef] [PubMed]
- Lefavrais, P. From the dyslexia diagnosis to the clinical study of reading. A new instrument: The Alouette test. Rev. Psychol. Appl. 1963, 13, 189–207. [Google Scholar]
- Oldfield, R.C. The assessment and analysis of handedness: The Edinburgh inventory. Neuropsychologia 1971, 9, 97–113. [Google Scholar] [CrossRef] [PubMed]
- Content, A.; Mousty, P.; Radeau, M. Brulex. A computerized lexical database for written and spoken French. Annee Psychol. 1990, 90, 551–566. [Google Scholar] [CrossRef]
- New, B.; Pallier, C.; Brysbaert, M.; Ferrand, L. Lexique 2: A new French lexical database. Behav. Res. Methods Instrum. Comput. 2004, 36, 516–524. [Google Scholar] [CrossRef]
- Snodgrass, J.; Vanderwart, M. A standardized set of 260 pictures: Norms for name agreement, image agreement, familiarity, and visual complexity. J. Exp. Psychol. Hum. Learn. Mem. 1980, 6, 174–215. [Google Scholar] [CrossRef]
- Handy, T.C.; Soltani, M.; Mangun, G.R. Perceptual load and visuocortical processing: Event-related potentials reveal sensory-level selection. Psychol. Sci. 2001, 12, 213–218. [Google Scholar] [CrossRef]
- Davis, C.J.; Coltheart, M. Paying attention to reading errors in acquired dyslexia. Trends Cogn. Sci. 2002, 6, 359–361. [Google Scholar] [CrossRef]
- Cao, W.; Zhang, Y.; Hou, C.; Yang, F.; Gong, J.; Jiang, S.; Huang, Y.; Xiao, R.; Luo, C.; Wang, X.; et al. Abnormal asymmetry in benign epilepsy with unilateral and bilateral centrotemporal spikes: A combined fMRI and DTI study. Epilepsy Res. 2017, 135, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Holt, R.L.; Provenzale, J.M.; Veerapandiyan, A.; Moon, W.J.; De Bellis, M.D.; Leonard, S.; Gallentine, W.B.; Grant, G.A.; Egger, H.; Song, A.W.; et al. Structural connectivity of the frontal lobe in children with drug-resistant partial epilepsy. Epilepsy Behav. 2011, 21, 65–70. [Google Scholar] [CrossRef]
- Anneken, K.; Evers, S.; Siawoosh, M.; Schwindt, W.; Deppe, M. Transient lesion in the splenium related to antiepileptic drug: Case report and new pathophysiological insights. Seizure 2008, 17, 654–657. [Google Scholar] [CrossRef]
- Noppeney, U.; Price, C.J.; Duncan, J.S.; Koepp, M.J. Reading skills after left anterior temporal lobe resection: An fMRI study. Brain 2005, 128, 1377–1385. [Google Scholar] [CrossRef]
- Tailby, C.; Weintrob, D.L.; Saling, M.M.; Fitzgerald, C.; Jackson, G.D. Reading difficulty is associated with failure to lateralize temporooccipital function. Epilepsia 2014, 55, 746–753. [Google Scholar] [CrossRef]
- Williamson, J.B.; Lamb, D.G.; Burtis, D.B.; Haque, S.; Zilli, E.M.; Kesayan, T.; Harciarek, M.; Heilman, K.M. Right hemispatial ipsilesional neglect with chronic right hemisphere strokes. J. Clin. Exp. Neuropsychol. 2018, 40, 347–356. [Google Scholar] [CrossRef] [PubMed]
- Saccheti, D.L.; Goedert, K.M.; Foundas, A.L.; Barrett, A.M. Ipsilesional neglect: Behavioral and anatomical correlates. Neuropsychology 2015, 29, 183–190. [Google Scholar] [CrossRef]
- Barton, J.J.S.; Hanif, H.M.; Eklinder Björnström, L.; Hills, C. The word-length effect in reading: A review. Cogn. Neuropsychol. 2014, 31, 378–412. [Google Scholar] [CrossRef]
- Patterson, K.; Kay, J. Letter-by-letter reading: Psychological descriptions of a neurological syndrome. Q. J. Exp. Psychol. Sect. A 1982, 34, 411–441. [Google Scholar] [CrossRef] [PubMed]
- Aldenkamp, A.P.; Overweg-Plandsoen, W.C.G.; Diepman, L.A.M. Factors involved in learning problems and educational delay in children with epilepsy. Child Neuropsychol. 1999, 5, 130–136. [Google Scholar] [CrossRef]
- Binnie, C.D.; Channon, S.; Marton, D. Learning disabilities in epilepsy: Neurophysiological aspects. Epilepsia 1990, 31, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Breier, J.I.; Brookshire, B.L.; Fletcher, J.M.; Thomas, A.B.; Plenger, P.M.; Wheless, J.W.; Willmore, L.J.; Papanicolaou, A. Identification of side of seizure onset in temporal lobe epilepsy using memory tests in the context of reading deficits. J. Clin. Exp. Neuropsychol. 1997, 19, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Broce, I.J.; Bernal, B.; Altman, N.; Bradley, C.; Baez, N.; Cabrera, L.; Hernandez, G.; De Feria, A.; Dick, A.S. Fiber pathways supporting early literacy development in 5–8-year-old children. Brain Cogn. 2019, 134, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Dehaene, S.; Cohen, L. The unique role of the visual word form area in reading. Trends Cogn. Sci. 2011, 15, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Hirshorn, E.A.; Li, Y.; Ward, M.J.; Richardson, R.M.; Fiez, J.A.; Ghuman, A.S. Decoding and disrupting left midfusiform gyrus activity during word reading. Proc. Natl. Acad. Sci. USA 2016, 113, 8162–8167. [Google Scholar] [CrossRef] [PubMed]
- Yeatman, J.D.; Weiner, K.S.; Pestilli, F.; Rokem, A.; Mezer, A.; Wandell, B.A. The vertical occipital fasciculus: A century of controversy resolved by in vivo measurements. Proc. Natl. Acad. Sci. USA 2014, 111, E5214–E5223. [Google Scholar] [CrossRef]
- Yeatman, J.D.; White, A.L. Reading: The confluence of vision and language. Annu. Rev. Vis. Sci. 2021, 7, 487–517. [Google Scholar] [CrossRef]
- Nakagawa, A. Role of anterior and posterior attention networks in hemispheric asymmetries during lexical decisions. J. Cogn. Neurosci. 1991, 3, 313–321. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
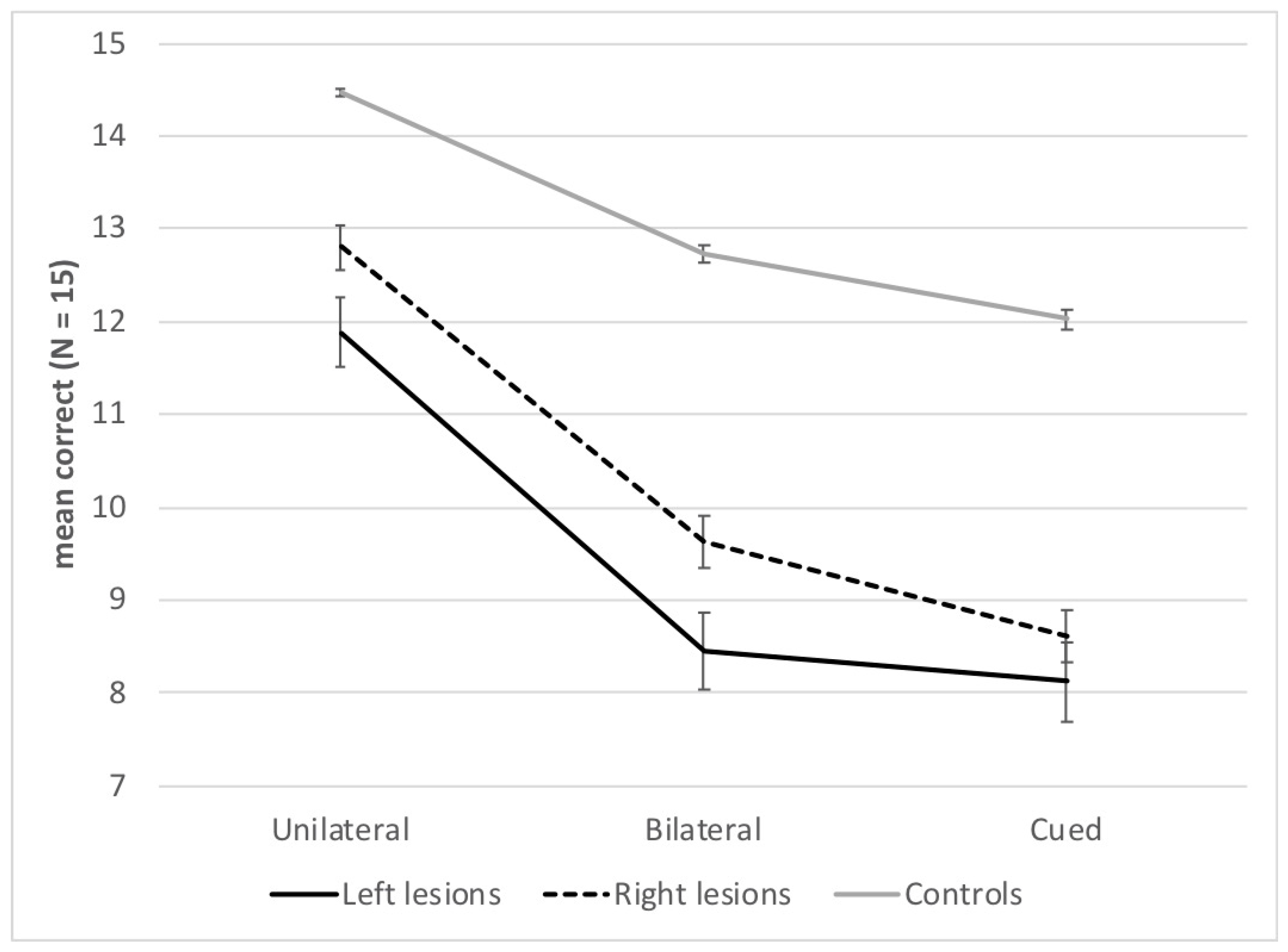
| Unilateral | Bilateral | Cued | ||||
|---|---|---|---|---|---|---|
| LVH | RVH | LVH | RVH | LVH | RVH | |
| Controls (n = 66) | 14.2 ± 0.9 | 14.9 ± 0.3 | 12.9 ± 1.9 | 12.6 ± 1.2 | 10.9 ± 2.1 | 13.7 ± 1.1 |
| Patients with left-sided epilepsy focus (n = 21) | 11.6 ± 3.1 | 12.7 ± 2.4 | 10.5 ± 3.5 | 6.9 ± 4.8 | 7.5 ± 4.4 | 9.1 ± 4.8 |
| Patients with right-sided epilepsy focus (n = 18) | 12.8 ± 2.3 | 14.3 ± 0.9 | 11.3 ± 2.4 | 8.8 ± 2.7 | 7.5 ± 3.4 | 10.2 ± 3.6 |
| Age | Gender | Epilepsy Duration | Language Dominance | Lesion | Surgical Resection | Clinical Deficits | WAIS | IQ | Alouette Reading Test | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| VCI | Accuracy z-Score | Speed z-Score | |||||||||
| Selection deficit | |||||||||||
| L12 | 32 | M | 8 | L | L anterior temporal cavernoma | Yes | language deficit, dyslexia antecedent, executive function deficit | 81 | 83 | –0.3 | –3.1 |
| L15 | 19 | M | 17 | L | L occipitoparietal ependymoma | Yes | lexical access deficit, executive function deficit | 75 | 77 | –0.7 | –3.2 |
| R8 | 30 | F | 9 | R | R temporal | No | 94 | 94 | 0 | –0.3 | |
| R13 | 50 | M | 25 | L | R temporal | No | 83 | 84 | 0.1 | –1.9 | |
| Contralesional deficit | |||||||||||
| L1 | 36 | M | 24 | L | L anterior temporal sclerosis | Yes | right superior quadranopia, memory deficit | 88 | 103 | 0.2 | –1.3 |
| L2 | 17 | M | 6 | R | L opercular and insular | Yes | executive function deficit | 120 | 102 | –0.9 | –0.6 |
| L11 | 42 | F | 1 | NA | L temporoparietal ganglioglioma | Yes | right hemianopia, dyslexia antecedent, lexical access deficit | NA | 69 | –1.5 | –3.7 |
| L17 | 23 | M | 15 | R | L mesial temporal arachnoid cyst | Yes | right superior quadranopia, dyslexia antecedent, depression | 90 | 87 | –1.8 | –2.1 |
| R6 | 48 | F | 18 | L | R temporoparietal, herpes encephalitis | Yes | 124 | 105 | NA | NA | |
| R7 | 19 | M | 15 | bilateral, R | R superior temporal dysplasia | No | dyslexia antecedent, lexical access deficit, verbal memory deficit | 98 | 109 | –1.1 | –1.2 |
| R9 | 37 | M | 23 | L | R occipitotemporal, vascular | No | left superior quadranopia, lexical access deficit, executive function deficit | 71 | 71 | –5.3 | –3.5 |
| R11 | 24 | F | 15 | L | R frontotemporal | Yes | memory deficit, executive function deficit, depression | 69 | 87 | 0.2 | 0.3 |
| Ipsilesional deficit | |||||||||||
| L6 | 19 | M | NA | L | L opercular and insular | Yes | dyslexia antecedent, executive function deficit | 110 | 94 | –3.5 | –3.5 |
| L9 | 29 | M | 20 | NA | L opercular dysplasia | Yes | NA | NA | –0.5 | –1.8 | |
| R1 | 19 | F | 18 | L | R precentral dysplasia | Yes | lexical access deficit | 112 | 100 | 0.1 | –0.5 |
| R10 | 20 | F | 7 | L | R occipital dysplasia | Yes | depression | 128 | 114 | –0.1 | –1.5 |
| Other deficits | |||||||||||
| L8 | 16 | M | 15 | bilateral | L mesial temporal sclerosis | No | memory and intellectual deficits | 63 | 66 | –0.9 | –3.4 |
| L10 | 20 | M | 5 | NA | L mesial temporal sclerosis | No | memory deficit | 94 | 95 | 0.1 | 0 |
| L13 | 21 | F | 10 | bilateral | L temporal | No | NA | NA | –0.7 | –1.6 | |
| L19 | 48 | M | 26 | R | L temporal | No | memory deficit | 84 | 90 | 0.2 | –1.7 |
| R2 | 16 | F | 13 | NA | R central dysplasia | Yes | brachial hemiparesis | 96 | 87 | 0.5 | –0.6 |
| Word Experiment | Object Experiment | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| z-Scores | Number Correct Words (LVH–RVH) (n = 15) | z-Scores | Number Correct Objects (LVH–RVH) (n = 15) | |||||||||
| Global | Sel. | Asym. | Uni. | Bil. | Cued | Global | Sel. | Asym. | Uni. | Bil. | Cued | |
| Selection deficit | ||||||||||||
| L12 | −5.7 | −3.0 | −0.3 | 8–12 | 13–3 | 0–6 | ||||||
| L15 | −8.9 | −2.0 | −0.3 | 5–8 | 3–3 | 1–1 | −3.5 | −1.1 | −2.4 | 11–13 | 11–6 | 12–4 |
| R8 | −2.2 | −3.4 | −0.8 | 14–15 | 11–10 | 8–6 | −1.8 | −1.7 | +0.1 | 14–13 | 10–12 | 10–7 |
| R13 | −5.0 | −2.7 | −0.8 | 9–13 | 8–7 | 7–2 | ||||||
| Contralesional deficit | ||||||||||||
| L1 | −3.2 | −0.4 | −5.4 | 14–11 | 12–2 | 13–6 | ||||||
| L2 | −5.8 | −1.7 | −2.6 | 10–11 | 8–1 | 7–4 | ||||||
| L11 | −9.6 | +2.0 | −4.1 | 4–1 | 6–0 | 6–0 | −7.6 | +1.3 | −9.3 | 13–0 | 9–0 | 13–0 |
| L17 | −4.7 | −1.7 | −6.0 | 13–9 | 12–1 | 10–3 | ||||||
| R6 | −5.8 | −0.4 | +3.6 | 4–13 | 8–5 | 1–10 | −8.0 | +0.7 | −0.2 | 8–4 | 6–5 | 4–6 |
| R7 | −6.0 | −1.7 | +2.8 | 6–14 | 8–2 | 0–10 | −1.6 | −1.1 | −1.9 | 13–14 | 14–7 | 11–8 |
| R9 | −4.6 | −2.0 | +2.6 | 10–14 | 7–5 | 2–11 | ||||||
| R11 | −2.7 | +0.3 | +3.1 | 9–15 | 10–7 | 5–15 | ||||||
| Ipsilesional deficit | ||||||||||||
| L6 | −4.3 | −2.4 | +4.6 | 10–15 | 4–9 | 2–11 | +0.3 | −0.8 | +1.0 | 14–15 | 12–14 | 12–10 |
| L9 | −3.3 | −1.0 | +6.2 | 9–15 | 4–13 | 3–13 | ||||||
| R1 | −2.1 | −2.0 | −4.7 | 15–13 | 14–6 | 12–5 | ||||||
| R10 | −4.9 | +0.3 | −3.6 | 8–10 | 14–1 | 8–6 | −2.7 | +0.1 | −0.2 | 8–13 | 13–10 | 11–6 |
| Other deficits | ||||||||||||
| L8 | −9.9 | −1.4 | −0.5 | 6–5 | 1–1 | 1–1 | −5.5 | −2.9 | +0.7 | 11–11 | 9–7 | 3–5 |
| L10 | −2.4 | −1.7 | −0.5 | 15–14 | 10–5 | 7–12 | −1.2 | −1.4 | −1.3 | 15–13 | 11–11 | 12–7 |
| L13 | −3.6 | −1.0 | +1.0 | 12–13 | 10–3 | 3–14 | ||||||
| L19 | −5.4 | −1.9 | −0.3 | 8–11 | 9–6 | 5–5 | ||||||
| R2 | −2.9 | −0.7 | −0.3 | 11–14 | 10–7 | 9–9 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siéroff, E.; Slama, Y.; Manouvrier, J.; Laurent, A. Dissociation between Selecting and Orienting Attentional Reading Deficits: A Study in Adults with Epilepsy. Brain Sci. 2024, 14, 252. https://doi.org/10.3390/brainsci14030252
Siéroff E, Slama Y, Manouvrier J, Laurent A. Dissociation between Selecting and Orienting Attentional Reading Deficits: A Study in Adults with Epilepsy. Brain Sciences. 2024; 14(3):252. https://doi.org/10.3390/brainsci14030252
Chicago/Turabian StyleSiéroff, Eric, Yael Slama, Jordane Manouvrier, and Agathe Laurent. 2024. "Dissociation between Selecting and Orienting Attentional Reading Deficits: A Study in Adults with Epilepsy" Brain Sciences 14, no. 3: 252. https://doi.org/10.3390/brainsci14030252
APA StyleSiéroff, E., Slama, Y., Manouvrier, J., & Laurent, A. (2024). Dissociation between Selecting and Orienting Attentional Reading Deficits: A Study in Adults with Epilepsy. Brain Sciences, 14(3), 252. https://doi.org/10.3390/brainsci14030252