


Artificial Intelligence as A Complementary Tool for Clincal Decision-Making in Stroke and Epilepsy
Abstract
1. Introduction
2. Basic Terminology and Concepts of AI
Reinforcement Learning
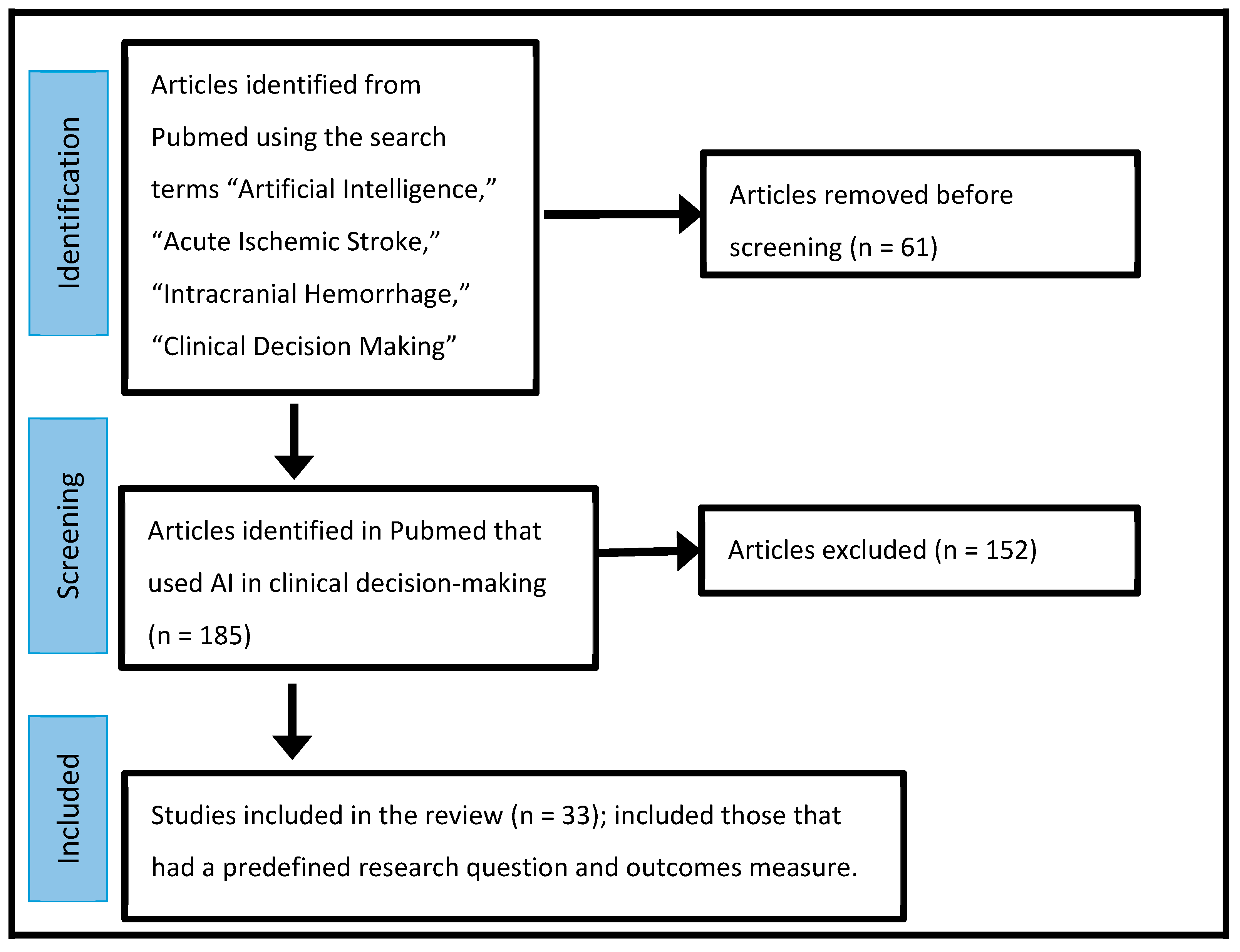
3. Methods
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Auger, S.D.; Jacobs, B.M.; Dobson, R.; Marshall, C.R.; Noyce, A.J. Big data, machine learning and artificial intelligence: A neurologist’s guide. Pract. Neurol. 2020, 21, 4–11. [Google Scholar] [CrossRef]
- Singh, A.; Velagala, V.R.; Kumar, T.; Dutta, R.R.; Sontakke, T. The Application of Deep Learning to Electroencephalograms, Magnetic Resonance Imaging, and Implants for the Detection of Epileptic Seizures: A Narrative Review. Cureus 2023, 15, e42460. [Google Scholar] [CrossRef]
- Torrente, A.; Maccora, S.; Prinzi, F.; Alonge, P.; Pilati, L.; Lupica, A.; Di Stefano, V.; Camarda, C.; Vitabile, S.; Brighina, F. The Clinical Relevance of Artificial Intelligence in Migraine. Brain Sci. 2024, 14, 85. [Google Scholar] [CrossRef]
- Vinny, P.; Vishnu, V.; Srivastava, M.P. Artificial Intelligence shaping the future of neurology practice. Med. J. Armed. Forces India 2021, 77, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Miceli, G.; Basso, M.G.; Rizzo, G.; Pintus, C.; Cocciola, E.; Pennacchio, A.R.; Tuttolomondo, A. Artificial Intelligence in Acute Ischemic Stroke Subtypes According to Toast Classification: A Comprehensive Narrative Review. Biomedicines 2023, 11, 1138. [Google Scholar] [CrossRef]
- Koza, J.R.; Bennett, F.H.; Andre, D.; Keane, M.A. Automated Design of Both the Topology and Sizing of Analog Electrical Circuits Using Genetic Programming. In Artificial Intelligence in Design ’96; Gero, J.S., Sudweeks, F., Eds.; Springer: Dordrecht, The Netherlands, 1996; pp. 151–170. ISBN 978-94-010-6610-5. [Google Scholar] [CrossRef]
- Mohri, M.; Rostamizadeh, A.; Talwalkar, A. Foundations of Machine Learning; The MIT Press: Cambridge, MA, USA, 2012; ISBN 9780262018258. [Google Scholar]
- Buhmann, J.; Kuhnel, H. Unsupervised and supervised data clustering with competitive neural networks. In Proceedings of the IJCNN International Joint Conference on Neural Networks, Baltimore, MD, USA, 7–11 June 1992; Volume 4, pp. 796–801. [Google Scholar] [CrossRef]
- Brahme, A. Comprehensive Biomedical Physics; Elsevier: Boca Raton, FL, USA, 2014; p. 1. ISBN 978-0-444-53633-4. [Google Scholar]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Venkatesan, R.; Li, B. Convolutional Neural Networks in Visual Computing: A Concise Guide; CRC Press: Boca Raton, FL, USA, 2017; ISBN 978-1-351-65032-8. [Google Scholar]
- Field, N.C.; Entezami, P.; Boulos, A.S.; Dalfino, J.; Paul, A.R. Artificial intelligence improves transfer times and ischemic stroke workflow metrics. Interv. Neuroradiol. 2023; epub ahead of print. [Google Scholar] [CrossRef]
- Zhou, X.-Z.; Lu, K.; Zhai, D.-C.; Cui, M.-M.; Liu, Y.; Wang, T.-T.; Shi, D.; Fan, G.-H.; Ju, S.-H.; Cai, W. The image quality and diagnostic performance of CT perfusion-derived CT angiography versus that of conventional CT angiography. Quant. Imaging Med. Surg. 2023, 13, 7294–7303. [Google Scholar] [CrossRef]
- Wu, Y.-P.; Xiang, S.-F.; Su, Y.; Li, S.-Y.; Yang, S.-J. Application of Computed Tomography Perfusion Imaging-guided Mechanical Thrombectomy in Ischemic Stroke Patients with Large Vessel Occlusion beyond the Therapeutic Time Window. Curr. Med. Imaging, 2023; epub ahead of print. [Google Scholar] [CrossRef]
- Du, B.; Yin, S.; Cao, S.; Mo, Y.; Liu, Y.; Zhang, Y.; Qiu, B.; Wu, X.; Hu, P.; Wang, K.; et al. Intracranial Atherosclerotic Stenosis Is Associated with Cognitive Impairment in Patients with Non-Disabling Ischemic Stroke: A pCASL-Based Study. Brain Connect. 2023, 13, 508–518. [Google Scholar] [CrossRef] [PubMed]
- Nazari-Farsani, S.; Yu, Y.; Armindo, R.D.; Lansberg, M.; Liebeskind, D.S.; Albers, G.; Christensen, S.; Levin, C.S.; Zaharchuk, G. Predicting final ischemic stroke lesions from initial diffusion-weighted images using a deep neural network. NeuroImage Clin. 2023, 37, 103278. [Google Scholar] [CrossRef]
- Kossen, T.; Madai, V.I.; Mutke, M.A.; Hennemuth, A.; Hildebrand, K.; Behland, J.; Aslan, C.; Hilbert, A.; Sobesky, J.; Bendszus, M.; et al. Image-to-image generative adversarial networks for synthesizing perfusion parameter maps from DSC-MR images in cerebrovascular disease. Front. Neurol. 2023, 13, 1051397. [Google Scholar] [CrossRef] [PubMed]
- Le, H.L.; Roh, H.G.; Kim, H.J.; Kwak, J.T. A 3D Multi-task Regression and Ordinal Regression Deep Neural Network for Collateral Imaging from Dynamic Susceptibility Contrast-Enhanced MR perfusion in Acute Ischemic Stroke. Comput. Methods Programs Biomed. 2022, 225, 107071. [Google Scholar] [CrossRef] [PubMed]
- Neves, G.; Warman, P.; Bueso, T.; Duarte-Celada, W.; Windisch, T. Identification of successful cerebral reperfusions [mTICI ≥ 2b] using an artificial intelligence strategy. Neuroradiology 2022, 64, 991–997. [Google Scholar] [CrossRef] [PubMed]
- Grosser, M.; Gellißen, S.; Borchert, P.; Sedlacik, J.; Nawabi, J.; Fiehler, J.; Forkert, N.D. Localized prediction of tissue outcome in acute ischemic stroke patients using diffusion- and perfusion-weighted MRI datasets. PLoS ONE 2020, 15, e0241917. [Google Scholar] [CrossRef] [PubMed]
- Sathish, R.; Rajan, R.; Vupputuri, A.; Ghosh, N.; Sheet, D. Adversarially Trained Convolutional Neural Networks for Semantic Segmentation of Ischaemic Stroke Lesion using Multisequence Magnetic Resonance Imaging. In Proceedings of the2019 41st Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 1010–1013. [Google Scholar]
- Reid, M.; Famuyide, A.O.; Forkert, N.D.; Talai, A.S.; Evans, J.W.; Sitaram, A.; Hafeez, M.; Najm, M.; Menon, B.K.; Demchuk, A.; et al. Accuracy and Reliability of Multiphase CTA Perfusion for Identifying Ischemic Core. Clin. Neuroradiol. 2019, 29, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, A.; Hansen, M.B.; Tietze, A.; Mouridsen, K. Prediction of Tissue Outcome and Assessment of Treatment Effect in Acute Ischemic Stroke Using Deep Learning. Stroke 2018, 49, 1394–1401. [Google Scholar] [CrossRef] [PubMed]
- Ho, K.C.; Speier, W.; El-Saden, S.; Arnold, C.W. Classifying Acute Ischemic Stroke Onset Time using Deep Imaging Features. AMIA Annu. Symp. Proc. 2018, 2017, 892–901. [Google Scholar]
- Yu, Y.; Guo, D.; Lou, M.; Liebeskind, D.S.; Scalzo, F. Prediction of Hemorrhagic Transformation Severity in Acute Stroke from Source Perfusion MRI. IEEE Trans. Biomed. Eng. 2017, 65, 2058–2065. [Google Scholar] [CrossRef]
- Tian, X.; Zeng, D.; Zhang, S.; Huang, J.; Zhang, H.; He, J.; Lu, L.; Xi, W.; Ma, J.; Bian, Z. Robust low-dose dynamic cerebral perfusion CT image restoration via coupled dictionary learning scheme. J. X-ray Sci. Technol. 2016, 24, 837–853. [Google Scholar] [CrossRef]
- Fang, R.; Chen, T.; Sanelli, P.C. Towards robust deconvolution of low-dose perfusion CT: Sparse perfusion deconvolution using online dictionary learning. Med. Image Anal. 2013, 17, 417–428. [Google Scholar] [CrossRef]
- Mendrik, A.; Vonken, E.; van Ginneken, B.; Smit, E.; Waaijer, A.; Bertolini, G.; Viergever, M.A.; Prokop, M. Automatic segmentation of intracranial arteries and veins in four-dimensional cerebral CT perfusion scans. Med. Phys. 2010, 37, 2956–2966. [Google Scholar] [CrossRef]
- Meyer-Baese, A.; Lange, O.; Wismueller, A.; Hurdal, M.K. Analysis of Dynamic Susceptibility Contrast MRI Time Series Based on Unsupervised Clustering Methods. IEEE Trans. Inf. Technol. Biomed. 2007, 11, 563–573. [Google Scholar] [CrossRef]
- Feng, H.; Wang, X.; Wang, W.; Zhao, X. Risk factors and a prediction model for the prognosis of intracerebral hemorrhage using cerebral microhemorrhage and clinical factors. Front. Neurol. 2023, 14, 1268627. [Google Scholar] [CrossRef]
- Maghami, M.; Sattari, S.A.; Tahmasbi, M.; Panahi, P.; Mozafari, J.; Shirbandi, K. Diagnostic test accuracy of machine learning algorithms for the detection intracranial hemorrhage: A systematic review and meta-analysis study. Biomed. Eng. Online 2023, 22, 114. [Google Scholar] [CrossRef]
- Vacek, A.; Mair, G.; White, P.; Bath, P.M.; Muir, K.W.; Salman, R.A.-S.; Martin, C.; Dye, D.; Chappell, F.M.; von Kummer, R.; et al. Evaluating artificial intelligence software for delineating hemorrhage extent on CT brain imaging in stroke. J. Stroke Cerebrovasc. Dis. 2024, 33, 107512. [Google Scholar] [CrossRef]
- Chen, Y.; Jiang, C.; Chang, J.; Qin, C.; Zhang, Q.; Ye, Z.; Li, Z.; Tian, F.; Ma, W.; Feng, M.; et al. An artificial intelligence-based prognostic prediction model for hemorrhagic stroke. Eur. J. Radiol. 2023, 167, 111081. [Google Scholar] [CrossRef] [PubMed]
- MacIntosh, B.J.; Liu, Q.; Schellhorn, T.; Beyer, M.K.; Groote, I.R.; Morberg, P.C.; Poulin, J.M.; Selseth, M.N.; Bakke, R.C.; Naqvi, A.; et al. Radiological features of brain hemorrhage through automated segmentation from computed tomography in stroke and traumatic brain injury. Front. Neurol. 2023, 14, 1244672. [Google Scholar] [CrossRef] [PubMed]
- Kotovich, D.; Twig, G.; Itsekson-Hayosh, Z.; Klug, M.; Ben Simon, A.; Yaniv, G.; Konen, E.; Tau, N.; Raskin, D.; Chang, P.J.; et al. The impact on clinical outcomes after 1 year of implementation of an artificial intelligence solution for the detection of intracranial hemorrhage. Int. J. Emerg. Med. 2023, 16, 50. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.-L.; Chen, C.; Zhang, L.-J.; Zheng, Y.-N.; Lv, X.-N.; Zhao, L.-B.; Li, Q.; Lv, F.-J. Prediction of Early Perihematomal Edema Expansion Based on Noncontrast Computed Tomography Radiomics and Machine Learning in Intracerebral Hemorrhage. World Neurosurg. 2023, 175, e264–e270. [Google Scholar] [CrossRef]
- Matsoukas, S.; Scaggiante, J.; Schuldt, B.R.; Smith, C.J.; Chennareddy, S.; Kalagara, R.; Majidi, S.; Bederson, J.B.; Fifi, J.T.; Mocco, J.; et al. Accuracy of artificial intelligence for the detection of intracranial hemorrhage and chronic cerebral microbleeds: A systematic review and pooled analysis. Radiol. Med. 2022, 127, 1106–1123. [Google Scholar] [CrossRef]
- Lim, M.J.R.; Quek, R.H.C.; Ng, K.J.; Loh, N.-H.W.; Lwin, S.; Teo, K.; Nga, V.D.W.; Yeo, T.T.; Motani, M. Machine Learning Models Prognosticate Functional Outcomes Better than Clinical Scores in Spontaneous Intracerebral Haemorrhage. J. Stroke Cerebrovasc. Dis. 2021, 31, 106234. [Google Scholar] [CrossRef]
- Heit, J.; Coelho, H.; Lima, F.; Granja, M.; Aghaebrahim, A.; Hanel, R.; Kwok, K.; Haerian, H.; Cereda, C.; Venkatasubramanian, C.; et al. Automated Cerebral Hemorrhage Detection Using RAPID. Am. J. Neuroradiol. 2020, 42, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Xu, Y.; Zhou, Y.; Su, R.; Tao, L.; Wang, Z.; Chen, C.; Chen, W. Prognostic Analysis of KCNQ2 Patients via Combining EEG Deep Features and Machine Learning Classifiers. In Proceedings of the 2023 45th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Sydney, Australia, 24–27 July 2023; pp. 1–4. [Google Scholar]
- Wang, H.; Hu, Z.; Jiang, D.; Lin, R.; Zhao, C.; Zhao, X.; Zhou, Y.; Zhu, Y.; Zeng, H.; Liang, D.; et al. Predicting Antiseizure Medication Treatment in Children with Rare Tuberous Sclerosis Complex–Related Epilepsy Using Deep Learning. Am. J. Neuroradiol. 2023, 44, 1373–1383. [Google Scholar] [CrossRef] [PubMed]
- Asadi-Pooya, A.A.; Fattahi, D.; Abolpour, N.; Boostani, R.; Farazdaghi, M.; Sharifi, M. Epilepsy classification using artificial intelligence: A web-based application. Epilepsia Open 2023, 8, 1362–1368. [Google Scholar] [CrossRef] [PubMed]
- Tveit, J.; Aurlien, H.; Plis, S.; Calhoun, V.D.; Tatum, W.O.; Schomer, D.L.; Arntsen, V.; Cox, F.; Fahoum, F.; Gallentine, W.B.; et al. Automated Interpretation of Clinical Electroencephalograms Using Artificial Intelligence. JAMA Neurol. 2023, 80, 805–812. [Google Scholar] [CrossRef]
- Torres-Gaona, G.; Aledo-Serrano, Á.; García-Morales, I.; Toledano, R.; Valls, J.; Cosculluela, B.; Munsó, L.; Raurich, X.; Trejo, A.; Blanquez, D.; et al. Artificial intelligence system, based on mjn-SERAS algorithm, for the early detection of seizures in patients with refractory focal epilepsy: A cross-sectional pilot study. Epilepsy Behav. Rep. 2023, 22, 100600. [Google Scholar] [CrossRef]
- QA for Machine Learning Models With the PDCA Cycle. Available online: https://dzone.com/articles/qa-for-machine-learning-models-with-the-pdca-cycle (accessed on 1 February 2024).
- Khandelwal, N. CT perfusion in acute stroke. Indian J. Radiol. Imaging 2008, 18, 281–286. [Google Scholar] [CrossRef]

{kind=link}
| Year | Authors | Research Question | Outcomes Measures/Conclusions |
|---|---|---|---|
| 2023 [12] | Field N. et al. | Does supplying an LVO detection algorithm notification to the thrombectomy team’s cell phone improve ischemic stroke workflow? | Transfer time and Mechanical Thrombectomy [MT] Initiation time decreased. |
| 2023 [13] | Zhaou X. et al. | Does CTA derived from CT Perfusion [CTA-DF-CTP] give better image quality and diagnostic accuracy than traditional CTA in AIS? | CTA derived from CTA-DF-CTP had diagnostic accuracy comparable to traditional CTA and CTA-DF-CTP. |
| 2023 [14] | Xiang et al. | Is it feasible to apply computed tomography perfusion [CTP] imaging-guided mechanical thrombectomy in acute ischemic stroke patients with LVO beyond the therapeutic time window? | NIHSS of MT group-CTP guided [at 6 h, 24 h, 7 days, and 30 days] was significantly better [p < 0.05]; however, infarct core volume approximation was too high or too low for this group. |
| 2023 [15] | Du B. et al. | In patients with ICAS [Intracranial Atherosclerotic Stenosis] in the anterior circulation, is AI based on CBF [Cerebral Blood Flow] or sCoV [Spatial Coefficient of Variation] better for predicting vascular cognitive impairment? | Cognitive impairment seems better predicted by AI analysis of sCoV than CBF. |
| 2023 [16] | Farsani S. et al. | Can AG-DCNN [Attention Gated Deep Convoluted Neural Network] predict infarct volume and size? | AG-DCNN, using only admission DWI, predicted infarct volumes at 3–7 days after stroke onset with accuracy like models using DWI and PWI. |
| 2022 [17] | Kossen T. et al. | How can modern machine learning methods such as generative adversarial networks [GANs] automate perfusion map generation from [DSC-MR] Dynamic Susceptibility Contrasted MR in AIS on an expert level without manual validation? | DSC-MR using machine learning can speed up patient stratification by perfusion mapping in AIS. |
| 2022 [18] | Long Le et al. | Can an advanced deep learning-based method accurately and rapidly assess collateral perfusion in AIS by automatically generating a multiphase collateral imaging map from dynamic susceptibility contrast-enhanced MR perfusion [DSC-MRP] images? | DSC-Enhanced MR Perfusion improved accuracy and sped the assessment of the collateral perfusion. |
| 2021 [19] | Neeves G et al. | Can a machine-learning [ML] algorithm grade digital subtraction angiograms [DSA] by the mTICI scale? | ML of complete cerebral DSA predicted mTICI scores following EVT of MCA occlusions. |
| 2020 [20] | Grosser M. et al. | In AIS patients, how do predictions of machine learning models based on local [regional] tissue susceptibility to ischemia compare with those of machine learning models based on global brain imaging? | Compared to single global machine learning models, locally trained machine learning models can lead to better prediction of lesion outcomes in AIS patients. |
| 2019 [21] | Satish R. et al. | Can Convolutional Neural Network analysis of Multisequence MRI in AIS predict the ischemic core and penumbra? | CNN analysis experimentally confirmed local changes. |
| 2019 [22] | Reid M. et al. | For detecting early severe ischemia, how does NCCT compare with multiphase computed tomography angiography [mCTA] regional leptomeningeal score [mCTA-rLMC] and an mCTA venous [mCTA-venous] perfusion lesion? | An assessment blinded to clinical information in patients undergoing endovascular therapy [EVT] showed that mCTA-venous more accurately detected early ischemia and predicted clinical outcomes than NCCT and the mCTA-rLMC score. |
| 2018 [23] | Nielsen A. et al. | In AIS, can Deep Learning improve Tissue Outcome and Treatment Effect predictions? | Deep Learning improves predictions of final neurological outcome and lesion volume. |
| 2018 [24] | Chung-Ho. et al. | Can imaging features and advanced machine learning use the TSS [Time Since Stroke] classification to characterize the Acute Ischemic Stroke Onset Time? | Demonstrates the potential benefit of using advanced machine learning methods in TSS classification. |
| 2017 [25] | Yu. Y. et al. | Can machine learning models trained on perfusion-weighted magnetic resonance imaging [PWI] and diffusion-weighted MRI scans predict HT [hemorrhagic transformation] occurrence and location in AIS? | HT prediction was a machine-learning problem. Specifically, the model learned to extract imaging markers of HT directly from source PWI images. |
| 2016 [26] | Tian X. et al. | Can clinically acceptable PCT [dynamic cerebral Perfusion Computed Tomography] images be created from low-dose CT images restored with a coupled dictionary learning [CDL] method in chronic and AIS patients? | CDL increased kinetic enhanced details and improved diagnostic hemodynamic parameter maps |
| 2013 [27] | Fang R. et al. | Will the robust sparse perfusion deconvolution method [SPD] accurately estimate cerebral blood flow [CBF] in CTP performed at a low radiation dose? | SPD was superior to existing methods for CBF and helped differentiate normal and ischemic brain tissue. |
| 2010 [28] | Mendrick A. et al. | Can the diagnostic yield of CTP in cerebrovascular diseases be expanded by combining arterial and venous segmentation and vessel-enhanced volume? | This artery and vein segmentation method was accurate for arteries and veins with normal perfusion. Combining the artery and vein segmentation with the vessel-enhanced volume produced an arteriogram and venogram, extending the diagnostic yield of CTP scans and making a CTA scan unnecessary. |
| 2007 [29]. | Meyer-Baese A. et al. | Do five unsupervised clustering techniques help analyze dynamic susceptibility contrast MRI time series? | Clustering is a valuable tool for analyzing and visualizing brain regional perfusion properties. |
| Year | Authors | Research Question | Outcome Measures/Conclusions |
|---|---|---|---|
| 2023 [30] | Feng H. et al. | Can AI use the GCS score, NIH stroke scale, INR, BUN, hemorrhage location, hematoma volume, modified Rankin score, and other risk factors to construct a prediction model for the prognosis of ICH at discharge, 3 months, and 12 months? | The study showed that prediction models for modified Rankin scores showed a relatively high predictive performance. Also, the study found risk factors and constructed a prediction model to predict poor modified-Rankin score outcomes and mortality at discharge, 3 months, and 12 months in ICH patients. |
| 2023 [31] | Maghami M. et al. | Are machine learning methods for detecting ICH from non-contrast CT scans sufficiently precise to be considered acceptable diagnostic tests of accuracy [DTA]? | This meta-analysis showed that assessing noncontract CT scans using ML algorithms for detecting ICH had acceptable DTA. |
| 2023 [32] | Vacek A. et al. | Can E-ASPECTS delineate the extent and distribution of ICH from brain CT? | AI software-Brainomix Ltd. (Oxford, UK) excellently delineated ICH extent- on stroke CTs by AI software in about 71% of cases. ICH extent was more likely to be over or underestimated when ICH was extensive, intraventricular, or extra-axial. |
| 2023 [33] | Chen Y. et al. | Can a convolutional neural network [CNN] create a clinical imaging perfusion model predicting the short-term neurological outcomes of ICH patients? | The CNN prognostication prediction model was more effective than ICH scales in predicting neurological outcomes and ICH patients at discharge. Predictions improved slightly after including clinical data. |
| 2023 [34] | MacIntosh B. et al. | Can Viola AI estimate the number and volume of hematoma clusters in traumatic brain injury and ICH patients? | The automated total hemorrhage volume estimate correlated with the per-participant hemorrhage cluster count. This tool may help evaluate various types of ICH in the future. |
| 2023 [35] | Kotovich D. et al. | Did implementing a commercial artificial intelligence solution in a level 1 trauma center emergency room affect ICH’s clinical outcome? | Artificial intelligence computer-aided triage and prioritization software in the emergency room setting was associated with a significant reduction in 30 day and 120 day all-cause mortality and morbidity in ICH patients. It was also associated with a significant reduction in modified Rankin score on discharge. |
| 2023 [36] | Li. Y. et al. | Can ML predict early perihematomal edema expansion [PHE] from non-contrast CT scan data in patients with spontaneous ICH? | This model was the best marker for predicting prior hematoma edema expansion in patients with ICH. It could predict early perihematomal edema expansion and improve the discrimination of early identification of spontaneous ICH in patients at risk of PHE expansion. |
| 2023 [37] | Mastoukas S., et al. | What are AI methods’ reported sensitivity, specificity, and accuracy for detecting ICH and chronic cerebral microbleeds? | In 40 studies, overall sensitivity, specificity, and accuracy were more than 90% for ICH and cerebral microbleed detection. AI algorithms were developed from large data sets, volumetric analysis of imaging examinations, fine-tuning, and false-positivity reduction. |
| 2022 [38] | Lim M. et al. | How do deep neural networks [DNN] and support vector machines [SVM] compare with clinical prognostic scores for prognosticating 30-day mortality and 90-day poor functional outcome [PFO] in spontaneous intracerebral hemorrhage [SICH]? | The SVM model performed significantly better than clinical prognostic scores in predicting 90-day PFO in SICH. |
| 2021 [39] | Heit J. et al. | What is the accuracy of RAPID ICH, 2D/3D, a volitional neural network application designed to detect ICH, in detecting and measuring ICH volume? | Rapid ICH was highly accurate in detecting ICH and quantifying the volume of intraparenchymal and intraventricular hemorrhages. |
| Year | Authors | Research Questions | Outcome Measures/Conclusions |
|---|---|---|---|
| 2023 [40] | Zheng Z. et al. | Can EEG Deep Features and Machine Learning Classifiers assess and prognostically analyze KCNQ2 patients by combining the two well-trained models, RESNET-15 and RESNET-18, to extract deep features of EEG? | An outcome of 79% accuracy was reported in pediatric patients. |
| 2023 [41] | Wang H. et al. | Can the multi-technique deep learning method WAE-Net use clinical data and multi-contrast MR imaging [T2WI and FLAIR images combined as FLAIR3 images] to forecast antiseizure medication treatment in a retrospective study involving 300 children with tuberous sclerosis complex-related epilepsy? | The hybrid technique of FLAIR3 could accurately localize tuberous sclerosis complex lesions, and the proposed method achieved the best performance [area under the curve = 0.908 and accuracy of 0.847] in the testing cohort among the compared methods. |
| 2023 [42] | Asadi-Pooya A. et al. | Can AI machine learning methods reliably differentiate idiopathic generalized epilepsy from focal epilepsy using easily accessible and applicable clinical history and physical examination data? | This algorithm aimed at easing epilepsy classification for individuals whose epilepsy began at age 10 and older. The stacking classifier led to better results than the base classifier in general. Precision was 81%, sensitivity was 81%, and specificity was close to 77%. |
| 2023 [43] | Tveit J. et al. | Can the artificial intelligence program SCORE-AI [Standardized Computer-based Organizing Reporting of EEG] be developed and validated to distinguish abnormal from normal EEGs, detect focal epilepsy epileptiform discharges and generalized epilepsy, and distinguish focal nonepileptiform and diffuse nonepileptiform EEGs? | SCORE-AI accuracy approached human expert-level and fully automated interpretation of routine EEGs. Accuracy was approximately 88.3%, significantly higher than the three previously published models comparing EEG interpretation to human experts. |
| 2023 [44] | Gustavo T. et al. | In patients diagnosed with epilepsy wearing the mjn-SERAS brain activity sensor, can AI create a personalized mathematical model for the programmed recognition of oncoming seizures before they start using patient-specific EEG training data? | The AI program accurately detected pre- and interictal EEG segments in drug-resistant epilepsy patients. |
| Extrapolation of PDCA in AI |
|---|
| Plan Explore and discuss the question, assess the potential solution, and make use of the various machine learning models or methods as described above, set the endpoint in the objectives and goals, identify the potential metrics to use for implementation and quality measurement, prepare the action plan which includes implementation along with a potential route to reevaluate as needed. |
| Do Evaluate earlier models; train or retrain and test different machine learning models; assess and see if known machine learning solutions and components of the AI protocol can be improved or changed; test the overall solution to assess its integrity; review the code and filter out older ML models which did not work. |
| Check Monitor the model for fairness; assess for bias and variance; monitor the stability precisely to ascertain clarity and results; implement split testing of two methodologies; compare them head-to-head and assess to see which performs better. |
| Act The goal is standardization and continuous improvement, deploying the solution and continuing to monitor for biasing and variance, evaluating for areas of improvement in active machine learning algorithms and machine learning components, standardizing data, and features, and continuing the PDCA cycle accordingly. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shah, S.P.; Heiss, J.D. Artificial Intelligence as A Complementary Tool for Clincal Decision-Making in Stroke and Epilepsy. Brain Sci. 2024, 14, 228. https://doi.org/10.3390/brainsci14030228
Shah SP, Heiss JD. Artificial Intelligence as A Complementary Tool for Clincal Decision-Making in Stroke and Epilepsy. Brain Sciences. 2024; 14(3):228. https://doi.org/10.3390/brainsci14030228
Chicago/Turabian StyleShah, Smit P., and John D. Heiss. 2024. "Artificial Intelligence as A Complementary Tool for Clincal Decision-Making in Stroke and Epilepsy" Brain Sciences 14, no. 3: 228. https://doi.org/10.3390/brainsci14030228
APA StyleShah, S. P., & Heiss, J. D. (2024). Artificial Intelligence as A Complementary Tool for Clincal Decision-Making in Stroke and Epilepsy. Brain Sciences, 14(3), 228. https://doi.org/10.3390/brainsci14030228