
The Role of Lurasidone in Managing Depressive Symptoms in People with Schizophrenia: A Review


 ,
,  ,
,  ,
, 
Abstract
1. Introduction
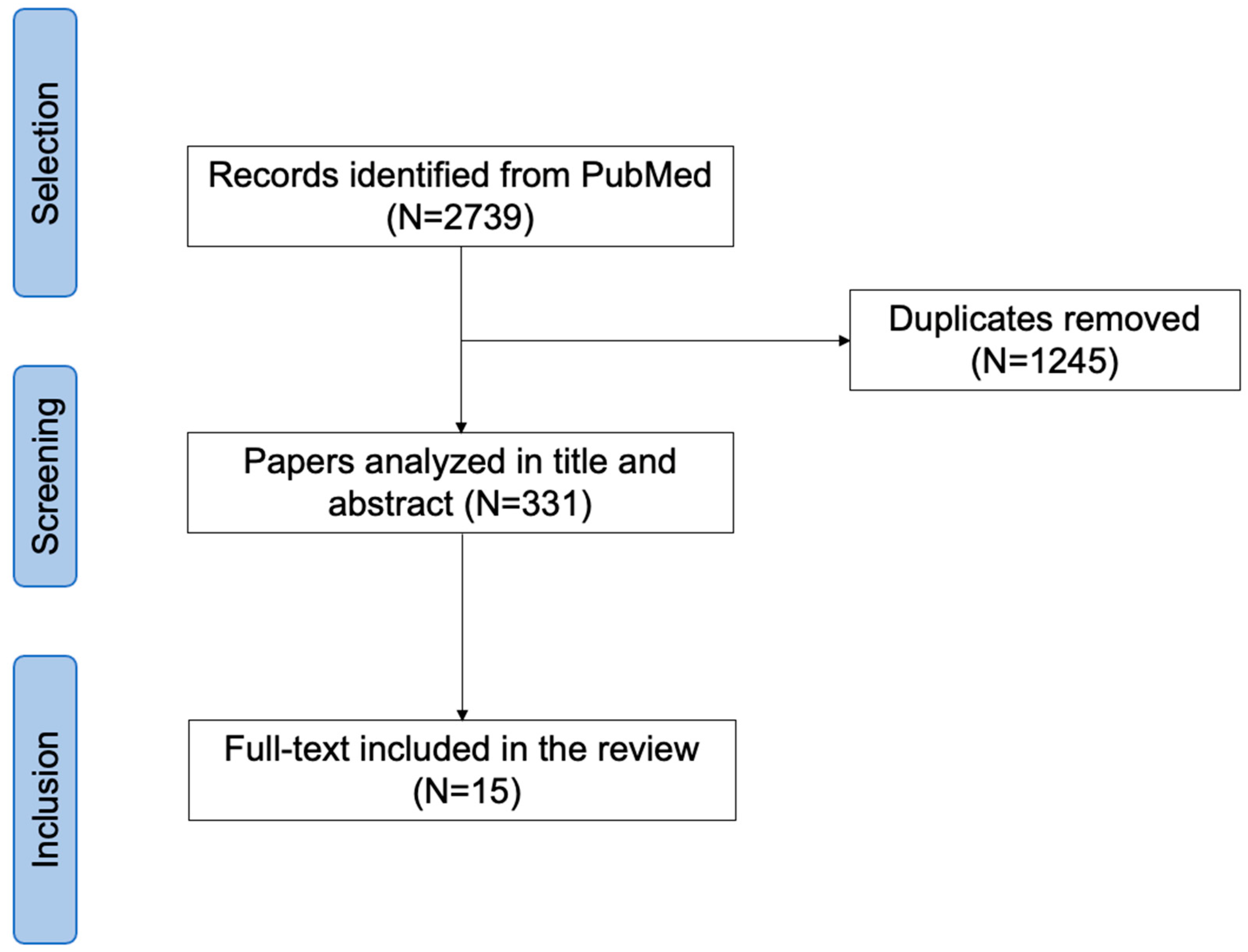
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mesholam-Gately, R.I.; Johnston, D.; Keshavan, M.S. What’s in the name “schizophrenia”? A clinical, research and lived experience perspective. World Psychiatry 2023, 22, 156–157. [Google Scholar] [CrossRef]
- Kanchanatawan, B.; Thika, S.; Anderson, G.; Galecki, P.; Maes, M. Affective symptoms in schizophrenia are strongly associated with neurocognitive deficits indicating disorders in executive functions, visual memory, attention and social cognition. Prog. Neuropsychopharmacol. Biol. Psychiatry 2018, 80 Pt C, 168–176. [Google Scholar] [CrossRef]
- Rybakowski, J.K. 120th Anniversary of the Kraepelinian Dichotomy of Psychiatric Disorders. Curr. Psychiatry Rep. 2019, 21, 65. [Google Scholar] [CrossRef] [PubMed]
- Wakefield, J.C. Klerman’s “credo” reconsidered: Neo-Kraepelinianism, Spitzer’s views, and what we can learn from the past. World Psychiatry 2022, 21, 4–25. [Google Scholar] [CrossRef] [PubMed]
- Leichsenring, F.; Steinert, C.; Rabung, S.; Ioannidis, J.P.A. The efficacy of psychotherapies and pharmacotherapies for mental disorders in adults: An umbrella review and meta-analytic evaluation of recent meta-analyses. World Psychiatry 2022, 21, 133–145. [Google Scholar] [CrossRef] [PubMed]
- Maj, M. Understanding depression beyond the “mind-body” dichotomy. World Psychiatry 2023, 22, 349–350. [Google Scholar] [CrossRef] [PubMed]
- Thornicroft, G. Psychiatric diagnosis and treatment in the 21st century: Paradigm shifts or power shifts? World Psychiatry 2022, 21, 334–335. [Google Scholar] [CrossRef] [PubMed]
- Stein, D.J.; Shoptaw, S.J.; Vigo, D.V.; Lund, C.; Cuijpers, P.; Bantjes, J.; Sartorius, N.; Maj, M. Psychiatric diagnosis and treatment in the 21st century: Paradigm shifts versus incremental integration. World Psychiatry 2022, 21, 393–414. [Google Scholar] [CrossRef] [PubMed]
- Lake, C.R.; Hurwitz, N. Schizoaffective disorders are psychotic mood disorders; there are no schizoaffective disorders. Psychiatry Res. 2006, 143, 255–287. [Google Scholar] [CrossRef]
- Malhi, G.S.; Green, M.; Fagiolini, A.; Peselow, E.D.; Kumari, V. Schizoaffective disorder: Diagnostic issues and future recommendations. Bipolar Disord. 2008, 10 Pt 2, 215–230. [Google Scholar] [CrossRef]
- Gratz, K.L.; Tull, M.T. A clinically useful conceptualization of emotion regulation grounded in functional contextualism and evolutionary theory. World Psychiatry 2022, 21, 460–461. [Google Scholar] [CrossRef] [PubMed]
- First, M.B.; Yousif, L.H.; Clarke, D.E.; Wang, P.S.; Gogtay, N.; Appelbaum, P.S. DSM-5-TR: Overview of what’s new and what’s changed. World Psychiatry 2022, 21, 218–219. [Google Scholar] [CrossRef] [PubMed]
- Arrasate, M.; González-Ortega, I.; García-Alocén, A.; Alberich, S.; Zorrilla, I.; González-Pinto, A. Prognostic Value of Affective Symptoms in First-Admission Psychotic Patients. Int. J. Mol. Sci. 2016, 17, 1039. [Google Scholar] [CrossRef] [PubMed]
- Sartorius, N. Community care for people with mental illness: Challenges emerging in the 2020s and consequent recommendations. World Psychiatry 2023, 22, 388–389. [Google Scholar] [CrossRef] [PubMed]
- Bergé, D.; Mané, A.; Salgado, P.; Cortizo, R.; Garnier, C.; Gomez, L.; Diez-Aja, C.; Bulbena, A.; Pérez, V. Predictors of Relapse and Functioning in First-Episode Psychosis: A Two-Year Follow-Up Study. Psychiatr. Serv. 2016, 67, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Hoertnagl, C.M.; Kaufmann, A.; Yalcin-Siedentopf, N.; Pfaffenberger, N.M.; Frajo-Apor, B.; Pardeller, S.; Kemmler, G.; Hofer, A. Premorbid Social Functioning and Affective Symptoms Predict Subjective Outcome Among Outpatients With Schizophrenia. Front. Psychiatry 2020, 11, 570857. [Google Scholar] [CrossRef] [PubMed]
- Almuqrin, A.; Georgiades, A.; Mouhitzadeh, K.; Rubinic, P.; Mechelli, A.; Tognin, S. The association between psychosocial stress, interpersonal sensitivity, social withdrawal and psychosis relapse: A systematic review. Schizophrenia 2023, 9, 22. [Google Scholar] [CrossRef] [PubMed]
- Starzer, M.; Hansen, H.G.; Hjorthøj, C.; Albert, N.; Nordentoft, M.; Madsen, T. 20-year trajectories of positive and negative symptoms after the first psychotic episode in patients with schizophrenia spectrum disorder: Results from the OPUS study. World Psychiatry 2023, 22, 424–432. [Google Scholar] [CrossRef]
- Leucht, S.; Schneider-Thoma, J.; Burschinski, A.; Peter, N.; Wang, D.; Dong, S.; Huhn, M.; Nikolakopoulou, A.; Salanti, G.; Davis, J.M. Long-term efficacy of antipsychotic drugs in initially acutely ill adults with schizophrenia: Systematic review and network meta-analysis. World Psychiatry 2023, 22, 315–324. [Google Scholar] [CrossRef]
- Bornheimer, L.A.; Martz, M.E.; Suzuki, T.; Tso, I.F.; Burton, C.Z.; Li Verdugo, J.; Grove, T.; Heitzeg, M.M.; Taylor, S.F. Affective Dysregulation Precedes Emergence of Psychosis-Like Experiences in a Community Sample of Young Adults. Schizophr. Bull. 2022, 48, 664–672. [Google Scholar] [CrossRef]
- Hunter, R.; Barry, S. Negative symptoms and psychosocial functioning in schizophrenia: Neglected but important targets for treatment. Eur. Psychiatry 2012, 27, 432–436. [Google Scholar] [CrossRef]
- Jimmy, B.; Jose, J. Patient medication adherence: Measures in daily practice. Oman Med. J. 2011, 26, 155–159. [Google Scholar] [CrossRef]
- Kestel, D. Transforming mental health for all: A critical role for specialists. World Psychiatry 2022, 21, 333–334. [Google Scholar] [CrossRef]
- Krueger, R.F. Incremental integration of nosological innovations is improving psychiatric diagnosis and treatment. World Psychiatry 2022, 21, 416–417. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Fan, L.; Wang, H.; Yu, J.; Lu, D.; Qi, J.; Nie, F.; Luo, Z.; Liu, Z.; Cheng, J.; et al. Structure-based design of a novel third-generation antipsychotic drug lead with potential antidepressant properties. Nat. Neurosci. 2022, 25, 39–49. [Google Scholar] [CrossRef]
- Fiorillo, A.; Cuomo, A.; Sampogna, G.; Albert, U.; Calò, P.; Cerveri, G.; De Filippis, S.; Masi, G.; Pompili, M.; Serafini, G.; et al. Lurasidone in adolescents and adults with schizophrenia: From clinical trials to real-world clinical practice. Expert Opin. Pharmacother. 2022, 23, 1801–1818. [Google Scholar] [CrossRef]
- Correll, C.U.; Solmi, M.; Croatto, G.; Schneider, L.K.; Rohani-Montez, S.C.; Fairley, L.; Smith, N.; Bitter, I.; Gorwood, P.; Taipale, H.; et al. Mortality in people with schizophrenia: A systematic review and meta-analysis of relative risk and aggravating or attenuating factors. World Psychiatry 2022, 21, 248–271. [Google Scholar] [CrossRef]
- McCutcheon, R.A.; Pillinger, T.; Efthimiou, O.; Maslej, M.; Mulsant, B.H.; Young, A.H.; Cipriani, A.; Howes, O.D. Reappraising the variability of effects of antipsychotic medication in schizophrenia: A meta-analysis. World Psychiatry 2022, 21, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Dong, S.; Schneider-Thoma, J.; Bighelli, I.; Siafis, S.; Wang, D.; Burschinski, A.; Schestag, K.; Samara, M.; Leucht, S. A network meta-analysis of efficacy, acceptability, and tolerability of antipsychotics in treatment-resistant schizophrenia. Eur. Arch. Psychiatry Clin. Neurosci. 2023, Epub ahead of print. [Google Scholar] [CrossRef]
- Ostuzzi, G.; Bertolini, F.; Tedeschi, F.; Vita, G.; Brambilla, P.; Del Fabro, L.; Gastaldon, C.; Papola, D.; Purgato, M.; Nosari, G.; et al. Oral and long-acting antipsychotics for relapse prevention in schizophrenia-spectrum disorders: A network meta-analysis of 92 randomized trials including 22,645 participants. World Psychiatry 2022, 21, 295–307. [Google Scholar] [CrossRef] [PubMed]
- Correll, C.U.; Solmi, M.; Cortese, S.; Fava, M.; Højlund, M.; Kraemer, H.C.; McIntyre, R.S.; Pine, D.S.; Schneider, L.S.; Kane, J.M. The future of psychopharmacology: A critical appraisal of ongoing phase 2/3 trials, and of some current trends aiming to de-risk trial programmes of novel agents. World Psychiatry 2023, 22, 48–74. [Google Scholar] [CrossRef]
- Burschinski, A.; Schneider-Thoma, J.; Chiocchia, V.; Schestag, K.; Wang, D.; Siafis, S.; Bighelli, I.; Wu, H.; Hansen, W.P.; Priller, J.; et al. Metabolic side effects in persons with schizophrenia during mid- to long-term treatment with antipsychotics: A network meta-analysis of randomized controlled trials. World Psychiatry 2023, 22, 116–128. [Google Scholar] [CrossRef]
- Feng, Y.; Shi, J.; Wang, L.; Zhang, X.; Tan, Y.; Zhao, J.; Ning, Y.; Xie, S.; Liu, X.; Liu, Q.; et al. Randomized, double-blind, 6-week non-inferiority study of lurasidone and risperidone for the treatment of schizophrenia. Psychiatry Clin. Neurosci. 2020, 74, 336–343. [Google Scholar] [CrossRef] [PubMed]
- Miura, I.; Watabe, K.; Sakaguchi, R.; Okamoto, K.; Maruyama, H. Effectiveness of Lurasidone 80 mg in Patients with Schizophrenia: Results of an Open-Label, 12-Week Extension Study. Neuropsychiatr. Dis. Treat. 2022, 18, 2627–2637. [Google Scholar] [CrossRef]
- Patel, P.J.; Weidenfeller, C.; Jones, A.P.; Nilsson, J.; Hsu, J. Long-Term Assessment of Lurasidone in Schizophrenia: Post Hoc Analysis of a 12-Month, Double Blind, Active-Controlled Trial and 6-Month Open-Label Extension Study. Neurol. Ther. 2021, 10, 121–147. [Google Scholar] [CrossRef]
- Mattingly, G.W.; Haddad, P.M.; Tocco, M.; Xu, J.; Phillips, D.; Pikalov, A.; Loebel, A. Switching to Lurasidone following 12 months of treatment with Risperidone: Results of a 6-month, open-label study. BMC Psychiatry 2020, 20, 199. [Google Scholar] [CrossRef]
- Harvey, P.D.; Siu, C.O.; Loebel, A.D. Insight and Treatment Outcomes in Schizophrenia: Post-hoc Analysis of a Long-term, Double-blind Study Comparing Lurasidone and Quetiapine XR. Innov. Clin. Neurosci. 2017, 14, 23–29. [Google Scholar]
- Oguchi, Y.; Nakagawa, A.; Kocha, H. A case of postpsychotic depression improved by switching antipsychotic monotherapy. Neuropsychopharmacol. Rep. 2023, 43, 146–149. [Google Scholar] [CrossRef] [PubMed]
- Ricci, V.; Martinotti, G.; De Berardis, D.; Maina, G. Lurasidone use in Cannabis-Induced Psychosis: A Novel Therapeutic Strategy and Clinical Considerations in Four Cases Report. Int. J. Environ. Res. Public Health 2022, 19, 16057. [Google Scholar] [CrossRef] [PubMed]
- Citrome, L.; Weiden, P.J.; McEvoy, J.P.; Correll, C.U.; Cucchiaro, J.; Hsu, J.; Loebel, A. Effectiveness of lurasidone in schizophrenia or schizoaffective patients switched from other antipsychotics: A 6-month, open-label, extension study. CNS Spectr. 2014, 19, 330–339. [Google Scholar] [CrossRef]
- Iyo, M.; Ishigooka, J.; Nakamura, M.; Sakaguchi, R.; Okamoto, K.; Mao, Y.; Tsai, J.; Fitzgerald, A.; Takai, K.; Higuchi, T. Safety and Effectiveness of Lurasidone in Patients with Schizophrenia: A 12-Week, Open-Label Extension Study. Neuropsychiatr. Dis. Treat. 2021, 17, 2683–2695. [Google Scholar] [CrossRef] [PubMed]
- Correll, C.U.; Cucchiaro, J.; Silva, R.; Hsu, J.; Pikalov, A.; Loebel, A. Long-term safety and effectiveness of lurasidone in schizophrenia: A 22-month, open-label extension study. CNS Spectr. 2016, 21, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Nasrallah, H.A.; Cucchiaro, J.B.; Mao, Y.; Pikalov, A.A.; Loebel, A.D. Lurasidone for the treatment of depressive symptoms in schizophrenia: Analysis of 4 pooled, 6-week, placebo-controlled studies. CNS Spectr. 2015, 20, 140–147. [Google Scholar] [CrossRef]
- McEvoy, J.P.; Citrome, L.; Hernandez, D.; Cucchiaro, J.; Hsu, J.; Pikalov, A.; Loebel, A. Effectiveness of lurasidone in patients with schizophrenia or schizoaffective disorder switched from other antipsychotics: A randomized, 6-week, open-label study. J. Clin. Psychiatry 2013, 74, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Loebel, A.; Cucchiaro, J.; Sarma, K.; Xu, L.; Hsu, C.; Kalali, A.H.; Pikalov, A.; Potkin, S.G. Efficacy and safety of lurasidone 80 mg/day and 160 mg/day in the treatment of schizophrenia: A randomized, double-blind, placebo- and active-controlled trial. Schizophr. Res. 2013, 145, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Ricci, V.; Di Salvo, G.; Maina, G. Lurasidone in first-episode psychosis with predominant depressive symptoms: A case report. Int. Clin. Psychopharmacol. 2023, 38, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Olivola, M.; Arienti, V.; Bassetti, N.; Giovanna, G.; Brondino, N. Lurasidone Augmentation of Clozapine in Refractory Schizophrenia: A Case Series. J. Clin. Psychopharmacol. 2023, 43, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Morrissette, D.B.; Stahl, S.M. Affective symptoms in schizophrenia. Drug Discov. Today Ther. Strateg. 2011, 8, 3–9. [Google Scholar] [CrossRef]
- Pompili, M.; Giordano, G.; Luciano, M.; Lamis, D.A.; Del Vecchio, V.; Serafini, G.; Sampogna, G.; Erbuto, D.; Falkai, P.; Fiorillo, A. Unmet Needs in Schizophrenia. CNS Neurol. Disord. Drug Targets 2017, 16, 870–884. [Google Scholar] [CrossRef]
- Upthegrove, R.; Marwaha, S.; Birchwood, M. Depression and Schizophrenia: Cause, Consequence, or Trans-diagnostic Issue? Schizophr. Bull 2017, 43, 240–244. [Google Scholar] [CrossRef]
- Häfner, H. Schizophrenia: Still Kraepelin’s dementia praecox? Epidemiol. Psichiatr. Soc. 2004, 13, 99–112. [Google Scholar] [CrossRef] [PubMed]
- Emsley, R. The future of psychopharmacology: Challenges beyond efficacy and tolerability. World Psychiatry 2023, 22, 82–83. [Google Scholar] [CrossRef] [PubMed]
- Levinson, D.F.; Umapathy, C.; Musthaq, M. Treatment of schizoaffective disorder and schizophrenia with mood symptoms. Am. J. Psychiatry 1999, 156, 1138–1148. [Google Scholar] [CrossRef] [PubMed]
- Vakalopoulos, C. A new nosology of psychosis and the pharmacological basis of affective and negative symptom dimensions in schizophrenia. Ment. Illn. 2010, 2, e7. [Google Scholar] [CrossRef] [PubMed]
- Dondé, C.; Vignaud, P.; Poulet, E.; Brunelin, J.; Haesebaert, F. Management of depression in patients with schizophrenia spectrum disorders: A critical review of international guidelines. Acta Psychiatr. Scand. 2018, 138, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Mulholland, C.; Cooper, S. The symptom of depression in schizophrenia and its management. Adv. Psychiatr. Treat. 2000, 6, 169–177. [Google Scholar] [CrossRef]
- Gregory, A.; Mallikarjun, P.; Upthegrove, R. Treatment of depression in schizophrenia: Systematic review and meta-analysis. Br. J. Psychiatry 2017, 211, 198–204. [Google Scholar] [CrossRef]
- Peuskens, J.; Demily, C.; Thibaut, F. Treatment of cognitive dysfunction in schizophrenia. Clin. Ther. 2005, 27 Suppl. A, S25–S37. [Google Scholar] [CrossRef]
- Davidson, L.; Tondora, J. Person-centred care planning as foundational to clinical practice. World Psychiatry 2022, 21, 1–2. [Google Scholar] [CrossRef]
- Kasper, S.; Jones, M.; Duchesne, I.; RODOS Investigator Group. Risperidone olanzapine drug outcomes studies in schizophrenia (RODOS): Health economic results of an international naturalistic study. Int. Clin. Psychopharmacol. 2001, 16, 189–196. [Google Scholar] [CrossRef]
- D’Souza, D.C. Cannabis, cannabinoids and psychosis: A balanced view. World Psychiatry 2023, 22, 231–232. [Google Scholar] [CrossRef]
- Wilson, J.E.; Nian, H.; Heckers, S. The schizoaffective disorder diagnosis: A conundrum in the clinical setting. Eur. Arch. Psychiatry Clin. Neurosci. 2014, 264, 29–34. [Google Scholar] [CrossRef]
- Abrams, D.J.; Rojas, D.C.; Arciniegas, D.B. Is schizoaffective disorder a distinct categorical diagnosis? A critical review of the literature. Neuropsychiatr. Dis. Treat. 2008, 4, 1089–1109. [Google Scholar] [CrossRef]
- Demyttenaere, K.; Anthonis, E.; Acsai, K.; Correll, C.U. Depressive Symptoms and PANSS Symptom Dimensions in Patients With Predominant Negative Symptom Schizophrenia: A Network Analysis. Front. Psychiatry 2022, 13, 795866. [Google Scholar] [CrossRef]
- Bartels, S.J.; Drake, R.E. Depressive symptoms in schizophrenia: Comprehensive differential diagnosis. Compr. Psychiatry 1988, 29, 467–483. [Google Scholar] [CrossRef]
- Gozdzik-Zelazny, A.; Borecki, L.; Pokorski, M. Depressive symptoms in schizophrenic patients. Eur. J. Med. Res. 2011, 16, 549–552. [Google Scholar] [CrossRef]
- Grover, S.; Sahoo, S.; Dua, D.; Chakrabarti, S.; Avasthi, A. Scales for assessment of depression in schizophrenia: Factor analysis of Calgary depression rating scale and Hamilton depression rating scale. Psychiatry Res. 2017, 252, 333–339. [Google Scholar] [CrossRef]
- Cheniaux, E.; Landeira-Fernandez, J.; Lessa Telles, L.; Lessa, J.L.; Dias, A.; Duncan, T.; Versiani, M. Does schizoaffective disorder really exist? A systematic review of the studies that compared schizoaffective disorder with schizophrenia or mood disorders. J. Affect. Disord. 2008, 106, 209–217. [Google Scholar] [CrossRef]
- Monsonet, M.; Kwapil, T.R.; Barrantes-Vidal, N. Exploring the Psychometric Properties and the Factor Structure of the Calgary Depression Scale for Schizophrenia Across the Schizotypy Continuum. Assessment 2022, 29, 686–699. [Google Scholar] [CrossRef]
- Oliveri, L.N.; Awerbuch, A.W.; Jarskog, L.F.; Penn, D.L.; Pinkham, A.; Harvey, P.D. Depression predicts self assessment of social function in both patients with schizophrenia and healthy people. Psychiatry Res. 2020, 284, 112681. [Google Scholar] [CrossRef]
- Pagel, T.; Franklin, J.; Baethge, C. Schizoaffective disorder diagnosed according to different diagnostic criteria--systematic literature search and meta-analysis of key clinical characteristics and heterogeneity. J. Affect. Disord. 2014, 156, 111–1118. [Google Scholar] [CrossRef] [PubMed]
- Peralta, V.; Cuesta, M.J. Exploring the borders of the schizoaffective spectrum: A categorical and dimensional approach. J. Affect. Disord. 2008, 108, 71–86. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rekhi, G.; Ng, W.Y.; Lee, J. Clinical utility of the Calgary Depression Scale for Schizophrenia in individuals at ultra-high risk of psychosis. Schizophr. Res. 2018, 193, 423–427. [Google Scholar] [CrossRef]
- Schennach, R.; Obermeier, M.; Seemüller, F.; Jäger, M.; Schmauss, M.; Laux, G.; Pfeiffer, H.; Naber, D.; Schmidt, L.G.; Gaebel, W.; et al. Evaluating depressive symptoms in schizophrenia: A psychometric comparison of the Calgary Depression Scale for Schizophrenia and the Hamilton Depression Rating Scale. Psychopathology 2012, 45, 276–285. [Google Scholar] [CrossRef]
- Galderisi, S. Promoting schizophrenia research in Europe: The contribution of the European Group for Research in Schizophrenia. World Psychiatry 2023, 22, 486–487. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author, Year, Country, and Study Design | Sample Size | Assessment Tool(s) | Main Findings | Study’s Limitations |
|---|---|---|---|---|
| Miura et al., 2022, Japan Double-blind study and 12-week extension study [34]. | 289 adult patients with schizophrenia. | Positive and Negative Syndrome Scale (PANSS) subscale scores Clinical Global Impression–Severity Scale (CGI-S) The Calgary Depression Scale for Schizophrenia (CDSS) | Patients reported a mean endpoint (week 12) change from the open-label baseline for lurasidone modal 80 mg/d vs. modal 40 mg/d of −0.5 vs. −0.4 at the CGI-S scale and −0.7 vs. −0.1 at the CDSS score. Patients receiving lurasidone modal 80 mg/d reported greater reductions on the PANSS positive subscale (−3.0 vs. −2.3), PANSS negative subscale (−1.9 vs. −1.7), and global scores (−5.1 vs. −3.8) compared to modal 40 mg/d. | Lack of random allocation to different dosages during the extension phase No patients were treated with a fixed dosage of lurasidone 80 mg/d due to the study design Short follow-up period No statistical test for identifying differences between groups |
| Iyo et al., 2021, Japan A 6-week, double-blind, placebo-controlled study was enrolled in a 12-week open-label extension study with flexible dosing of lurasidone at 40 or 80 mg/day [41]. | 289 patients were enrolled in the open-label extension study. | Positive and Negative Syndrome Scale (PANSS) total score Clinical Global Impression–Severity Scale (CGI-S) The Calgary Depression Scale for Schizophrenia (CDSS) European Quality of Life 5 Dimensions 3 Level Version (EQ-5D-3L) EuroQol visual analog scale (EQ-VAS) | Treatment with lurasidone compared to placebo has resulted in a broad range of benefits, including improvements in depressive and cognitive symptoms. Patients reported a significant reduction in clinical sympotmatology, scoring −29.4 (17.6) at the PANSS total score in the double blind and −8.8 (13.3) in the open-label study. The CDSS score was stable. An improvement in quality of life evaluated at EQ-5D-3L was found at week 12. Patients reported an overall mean (SD) increase of 0.097 (0.190) (double-blind study) and 0.028 (0.141) (open-label study). An improvement in quality of life evaluated at the EQ VAS was found, scoring 16.8 (24.1) and 5.3 (18.8) at the double-blind and open-label baselines, respectively. | Short follow-up period Lack of a comparator No statistical test for identifying differences between groups |
| Patel et al., 2020, USA Post hoc analyses [35]. | Patients with schizophrenia were randomized to lurasidone (n = 399) and risperidone (n = 190), of whom 129 and 84 continued into OLE, respectively. | Positive and Negative Syndrome Scale (PANSS) Clinical Global Impression–Severity Scale (CGI-S) Montgomery–Asberg Depression Rating Scale (MADRS) | Patients treated with lurasidone (mean change −0.8, 95% CI: −1.6, 0.0) and risperidone (mean change −2.3, 95% CI: −3.2, −1.3) both reported a reduction in the MADRS total score from baseline to month 12. A statistically significant difference was found between patients treated with lurasidone and with risperidone only at month 12 (p = 0.013). | Exclusion criteria: patients with a previous poor or inadequate response/intolerability to risperidone or with an acute exacerbation of schizophrenia Open-label design Lack of a control group |
| Mattingly et al., 2020, USA Post hoc analyses [36]. | Of the 236 patients who completed the initial 12-month double-blind study, 223 (94.5%) continued into the open-label extension study. | Positive and Negative Syndrome Scale (PANSS) Clinical Global Impression (CGI) Montgomery–Åsberg Depression Rating Scale (MADRS) | After completion of 12 months of double-blind treatment with lurasidone or risperidone, mean change scores were −1.7 and −2.6, respectively. | Open-label design Lack of randomization Lack of active control group Small sample size in the risperidone switch group Exclusion criteria: patients with an acute exacerbation No statistical test for identifying differences between groups |
| Feng et al., 2020, China Randomized, flexible-dose, double-blind, double-dummy, 6-week non-inferiority study comparing the efficacy and the safety of lurasidone to risperidone [33]. | 444 patients were screened to obtain an intent-to-treat sample of 384 patients, of whom 54 discontinued treatment prior to 6 weeks. | Positive and Negative Syndrome Scale (PANSS) Positive and Negative Syndrome Scale (PANSS)—positive symptoms subscale Positive and Negative Syndrome Scale (PANSS)—negative symptoms subscale Clinical Global Impression–Severity of Illness (CGI-S) Clinical Global Impression–Improvement scale (CGI-I) The Calgary Depression Scale for Schizophrenia (CDSS) Barnes Akathisia Scale (BAS) Abnormal Involuntary Movement Scale (AIMS) Simpson Angus Scale (SAS) | Patients treated with risperidone compared to lurasidone reported a significant increase in glucose (+1.1 mg/dL vs. −0.3 mg/dL; p < 0.05), serum prolactin (+60.4 ng/mL vs. +3.5 ng/mL; p < 0.001), and body mass index (+0.45 kg/m2 vs. +0.20 kg/m2; p < 0.05). No significant differences were found at BARNES, AIMS, and SAS between patients treated with lurasidone and those treated with risperidone (+0.2 vs. +0.2, p = 0.369; +0.0 vs. +0.0, p = 0.922; +0.5 vs. +0.8, p = 0.098 at week 6). | Exclusion criteria: patients with physical and psychiatric comorbidities Short follow-up (i.e., 6 weeks) |
| Harvey et al., 2017, USA Post hoc analysis based on data from a previously randomized, double-blind, six-week placebo- and active controlled acute study, followed by a one-year [37]. | 488 patients with schizophrenia, were randomly assigned to lurasidone 80 mg/d, lurasidone 160 mg/d, quetiapine XR 600 mg/die, or placebo. | Item G12: “impaired insight and judgment” of the Positive and Negative Syndrome Scale (PANSS) Montgomery–Åsberg Depression Rating Scale (MADRS) Quality of Well-Being Scale Self-Administered (QWB-SA) scale | Patients treated with lurasidone reported a significant improvement in “insight and judgment” from acute phase baseline to week 6 (effect size = 0.61 for 160 mg/d vs. placebo, p < 0.001; effect size = 0.58 for 80 mg/d vs. placebo, p < 0.001), as well as those treated with quetiapine XR 600 mg/d (effect size = 0.67 vs. placebo, p < 0.001) compared to patients treated with placebo. | Using the single PANSS-item G12 for measuring insight and judgment |
| Correll et al., 2016, USA Open-label study [42]. | A total of 496 patients were randomized in the core acute study. Patients who completed a 6-week, double-blind (DB), placebo-controlled trial continued in a 22-month, open-label (OL) study during which they received once-daily, flexible doses of lurasidone, 40–120 mg. | Positive and Negative Syndrome Scale (PANSS) Clinical Global Impression– Severity Scale (CGI-S) Montgomery–Åsberg Depression Rating Scale (MADRS) | Patients reported a mean change from DB baseline of −43.6 and −28.4 at the PANSS total score at month 24. A significant reduction in MADRS score was found (10.6 ± 6.7 vs. 11.4 ± 6.09). Treatment with lurasidone was associated with a mean change in weight of +0.4 kg at month 12 and +0.8 kg at month 24. Median change to month 12 and month 24, respectively, was −1.0 and −9.0 mg/dL for total cholesterol; 0.0 and −1.0 mg/dL for LDL; +1.0 and −11.0 mg/dL for triglycerides; and 0.0 and −0.1/% for HbA1c. | Lack of randomization Lack of an active comparator Lack of a double-bind design High attrition rate |
| Nasrallah et al., 2015, USA Patient-level data were pooled from four similarly designed, double-blind, placebo-controlled, 6-week registration studies of lurasidone (40–160 mg/d) [43]. | Adult patients with an acute exacerbation of schizophrenia. N = 1330 patients with acute schizophrenia (N = 898 lurasidone, N = 432 placebo). | Montgomery–Åsberg Depression Rating Scale (MADRS) | At week 6, patients treated with both doses of lurasidone reported a significant reduction of depressive symptoms evaluated at MADRS (8.4) compared to those treated with placebo (10.2) (p < 0.001). | Differences in study design, study duration, severity of depressive symptoms at baseline, and outcome measures used in the pooled analysis |
| Citrome et al., 2014, USA Open-label, 6-month study [40]. | Of the 198 patients who completed the core 6-week study, 149 (75.3%) entered the extension study. Clinically stable, but symptomatic, outpatients with schizophrenia or schizoaffective disorder were switched to lurasidone. | Positive and Negative Syndrome Scale (PANSS) Clinical Global Impression Severity of Illness (CGI-S) scores Calgary Depression Scale for Schizophrenia (CDSS) scores | Patients reported a significant reduction in PANSS total score (−8.2 ± 12.6), in CGI-S score (−0.39 ± 0.85), and in CDSS score (−1.2 ± 4.3). | Short follow-up period (i.e., 6 months) Open-label design Lack of a parallel control group |
| McEvoy et al., 2013, USA Open-label, 6-month study [44]. | 244 patients with schizophrenia, randomly allocated to lurasidone 40/40, lurasidone 40/80, and lurasidone 80/80. | Positive and Negative Syndrome Scale (PANSS) Clinical Global Impression– Severity Scale (CGI-S) Calgary Depression Scale for Schizophrenia (CDSS) scores | Significant reductions in depressive symptoms were similar across all randomized groups (p = 0.861). | Short follow-up period (i.e., 6 months) |
| Loebel et al., 2013, USA Prospective, parallel-group study [45]. | Patients with schizophrenia randomly assigned to receive 6 weeks of double-blind treatment with once-daily evening doses of lurasidone (80 mg, 160 mg), QXR (600 mg), or placebo, recently hospitalized for an acute exacerbation of psychotic symptoms. | Positive and Negative Syndrome Scale (PANSS) total and subscale scores Clinical Global Impression Severity of Illness (CGI-S) scores Montgomery–Åsberg Depression Rating Scale (MADRS) Negative Symptom Assessment Scale, subject-rated Medication Satisfaction Questionnaire | Patients treated with both doses of lurasidone and QXR-600 mg reported a significantly greater improvement in depressive symptoms compared with the placebo group at week 6, as assessed with the MADRS. Patients treated with lurasidone 80 mg (−22.2 [1.8]) and 160 mg (−26.5 [1.8]) reported a significant improvement compared with the placebo group (−10.3 [1.8]) (p < 0.001). Patients receiving QXR-600 mg reported a greater reduction in PANSS total score compared to placebo (−27.8 [1.8], p < 0.001). Variation in the PANSS total score was similar for patients treated with lurasidone 160 mg compared to those treated with QXR-600 mg (−26.5 vs. −27.8; p = 1.00). | The use of a fixed-dose design facilitated the assessment of dose–response effects Exclusion criteria: patients with physical comorbidity and using other medications |
| Author, Year, and Country | Sample Size | Assessment Tool | Main Findings | Study’s Limitations |
|---|---|---|---|---|
| Oguchi et al., 2023, Japan [38]. | One young male patient with schizophrenia, aged 20 years old. | No specified, qualitative interview | The patient developed post-psychotic depression, including despair, overwhelming loss, humiliation, and suicidal ideation, during treatment with paliperidone. He was switched to lurasidone 40 mg monotherapy. | Case report |
| Ricci et al., 2023, Italy [46]. | One young male patient with schizophrenia, aged 19 years old. | Positive and Negative Syndrome Scale (PANSS) Clinical Global Impression–Severity Scale (CGI-S) Montgomery–Asberg Rating Scale (MADRS) | 19-year-old male patient with first-episode psychosis (FEP) and predominant depressive symptoms. Remarkable clinical and functional improvement was observed 3 months after the beginning of lurasidone treatment. The patient’s depressive symptoms disappear with a dramatic reduction of psychotic ones, with good tolerance of the drug and without adverse effects. Lurasidone seems to be a promising treatment option for FEP with predominant depressive symptoms. | Case report |
| Olivola et al., 2023, Italy [47]. | Four patients treated with clozapine who were diagnosed with treatment-resistant schizophrenia. | Positive and Negative Syndrome Scale (PANSS) Udvalg for Kliniske Undersøgelser Side Effect Rating Scale (UKU-SERS) | All patients achieved a significant reduction of both positive and negative symptoms, with no significant adverse effects to be reported. | Case series |
| Ricci et al., 2022, Italy [39]. | Four patients experienced their first cannabis-induced psychotic episode. | Unspecified | Lurasidone also appears to be effective in other symptom domains related to schizophrenia, such as depressive symptoms. | Case series |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiorillo, A.; Sampogna, G.; Albert, U.; Bondi, E.; De Giorgi, S.; Fagiolini, A.; Pompili, M.; Serafini, G.; Volpe, U.; Vita, A. The Role of Lurasidone in Managing Depressive Symptoms in People with Schizophrenia: A Review. Brain Sci. 2024, 14, 225. https://doi.org/10.3390/brainsci14030225
Fiorillo A, Sampogna G, Albert U, Bondi E, De Giorgi S, Fagiolini A, Pompili M, Serafini G, Volpe U, Vita A. The Role of Lurasidone in Managing Depressive Symptoms in People with Schizophrenia: A Review. Brain Sciences. 2024; 14(3):225. https://doi.org/10.3390/brainsci14030225
Chicago/Turabian StyleFiorillo, Andrea, Gaia Sampogna, Umberto Albert, Emi Bondi, Serafino De Giorgi, Andrea Fagiolini, Maurizio Pompili, Gianluca Serafini, Umberto Volpe, and Antonio Vita. 2024. "The Role of Lurasidone in Managing Depressive Symptoms in People with Schizophrenia: A Review" Brain Sciences 14, no. 3: 225. https://doi.org/10.3390/brainsci14030225
APA StyleFiorillo, A., Sampogna, G., Albert, U., Bondi, E., De Giorgi, S., Fagiolini, A., Pompili, M., Serafini, G., Volpe, U., & Vita, A. (2024). The Role of Lurasidone in Managing Depressive Symptoms in People with Schizophrenia: A Review. Brain Sciences, 14(3), 225. https://doi.org/10.3390/brainsci14030225