
Changes in Structural Neural Networks in the Recovery Process of Motor Paralysis after Stroke

Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Rehabilitation Therapy
2.3. LF-rTMS: Equipment and Protocol
2.4. Clinical Assessment of Motor Function
2.5. MRI Acquisition
2.6. Assessment of 3D T1WI
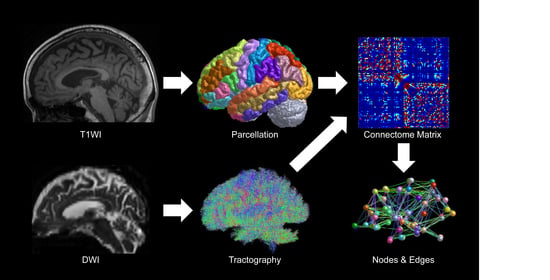
2.7. Development of Structural Neural Networks and Graph Theoretical Analysis
2.8. Meaning of the Network Measures [25,26,36,37,38]
- Degree centrality is defined as the number of connections to the node of interest.
- Betweenness centrality is defined as the proportion of the nodes of interest existing on the connecting path between nodes other than those of interest. The larger the value is, the more the node functions as a hub in the network.
- Nodal clustering coefficient is defined as the proportion of connections between nodes that are connected to the node of the interest. The larger the value is, the more functionally separate the network is.
- Nodal efficiency is defined as the inverse of the average length of the shortest paths between the nodes of interest and every other node. The larger the value is, the more functionally integrated the network is.
2.9. Statistical Analysis
3. Results
3.1. Changes in Upper Limb Motor Function
3.2. Generation of Streamlines and the Structural Connectivity Matrix
3.3. Changes in Network Measures
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Di Pino, G.; Pellegrino, G.; Assenza, G.; Capone, F.; Ferreri, F.; Formica, D.; Ranieri, F.; Tombini, M.; Ziemann, U.; Rothwell, J.C.; et al. Modulation of brain plasticity in stroke: A novel model for neurorehabilitation. Nat. Rev. Neurol. 2014, 10, 597–608. [Google Scholar] [CrossRef] [PubMed]
- Wolf, S.L.; Lecraw, D.E.; Barton, L.A.; Jann, B.B. Forced use of hemiplegic upper extremities to reverse the effect of learned nonuse among chronic stroke and head-injured patients. Exp. Neurol. 1989, 104, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Taub, E.; Miller, N.E.; Novack, T.A.; Cook, E.W., 3rd; Fleming, W.C.; Nepomuceno, C.S.; Connell, J.S.; Crago, J.E. Technique to improve chronic motor deficit after stroke. Arch. Phys. Med. Rehabil. 1993, 74, 347–354. [Google Scholar]
- O’Brien, A.T.; Bertolucci, F.; Torrealba-Acosta, G.; Huerta, R.; Fregni, F.; Thibaut, A. Non-invasive brain stimulation for fine motor improvement after stroke: A meta-analysis. Eur. J. Neurol. 2018, 25, 1017–1026. [Google Scholar] [CrossRef] [PubMed]
- Xiang, H.; Sun, J.; Tang, X.; Zeng, K.; Wu, X. The effect and optimal parameters of repetitive transcranial magnetic stimulation on motor recovery in stroke patients: A systematic review and meta-analysis of randomized controlled trials. Clin. Rehabil. 2019, 33, 847–864. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Xing, G.; Fan, Y.; Guo, Z.; Chen, H.; Mu, Q. Short- and Long-term Effects of Repetitive Transcranial Magnetic Stimulation on Upper Limb Motor Function after Stroke: A Systematic Review and Meta-Analysis. Clin. Rehabil. 2017, 31, 1137–1153. [Google Scholar] [CrossRef] [PubMed]
- Wall, A.; Borg, J.; Palmcrantz, S. Clinical application of the Hybrid Assistive Limb (HAL) for gait training-a systematic review. Front. Syst. Neurosci. 2015, 9, 48. [Google Scholar] [CrossRef]
- Takahashi, K.; Domen, K.; Sakamoto, T.; Toshima, M.; Otaka, Y.; Seto, M.; Irie, K.; Haga, B.; Takebayashi, T.; Hachisuka, K. Efficacy of Upper Extremity Robotic Therapy in Subacute Poststroke Hemiplegia: An Exploratory Randomized Trial. Stroke 2016, 47, 1385–1388. [Google Scholar] [CrossRef]
- Kakuda, W.; Abo, M.; Kobayashi, K.; Momosaki, R.; Yokoi, A.; Fukuda, A.; Ishikawa, A.; Ito, H.; Tominaga, A. Low-frequency repetitive transcranial magnetic stimulation and intensive occupational therapy for poststroke patients with upper limb hemiparesis: Preliminary study of a 15-day protocol. Int. J. Rehabil. Res. 2010, 33, 339–345. [Google Scholar] [CrossRef]
- Chen, R.; Classen, J.; Gerloff, C.; Celnik, P.; Wassermann, E.M.; Hallett, M.; Cohen, L.G. Depression of motor cortex excitability by low-frequency transcranial magnetic stimulation. Neurology. 1997, 48, 1398–1403. [Google Scholar] [CrossRef]
- Takeuchi, N.; Chuma, T.; Matsuo, Y.; Watanabe, I.; Ikoma, K. Repetitive transcranial magnetic stimulation of contralesional primary motor cortex improves hand function after stroke. Stroke 2005, 36, 2681–2686. [Google Scholar] [CrossRef]
- Kakuda, W.; Abo, M.; Kobayashi, K.; Takagishi, T.; Momosaki, R.; Yokoi, A.; Fukuda, A.; Ito, H.; Tominaga, A. Baseline severity of upper limb hemiparesis influences the outcome of low-frequency rTMS combined with intensive occupational therapy in patients who have had a stroke. PM&R 2011, 3, 516–522. [Google Scholar]
- Kakuda, W.; Abo, M.; Shimizu, M.; Sasanuma, J.; Okamoto, T.; Yokoi, A.; Taguchi, K.; Mitani, S.; Harashima, H.; Urushidani, N.; et al. NEURO Investigators. A multi-center study on low-frequency rTMS combined with intensive occupational therapy for upper limb hemiparesis in post-stroke patients. J. Neuroeng. Rehabil. 2012, 9, 4. [Google Scholar] [CrossRef]
- Abo, M.; Kakuda, W.; Momosaki, R.; Harashima, H.; Kojima, M.; Watanabe, S.; Sato, T.; Yokoi, A.; Umemori, T.; Sasanuma, J. Randomized, multicenter, comparative study of NEURO versus CIMT in poststroke patients with upper limb hemiparesis: The NEURO-VERIFY Study. Int. J. Stroke 2014, 9, 607–612. [Google Scholar] [CrossRef]
- Kakuda, W.; Abo, M.; Sasanuma, J.; Shimizu, M.; Okamoto, T.; Kimura, C.; Kakita, K.; Hara, H. Combination Protocol of Low-Frequency rTMS and Intensive Occupational Therapy for Post-stroke Upper Limb Hemiparesis: A 6-year Experience of More Than 1700 Japanese Patients. Transl. Stroke Res. 2016, 7, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Nudo, R.J.; Wise, B.M.; SiFuentes, F.; Milliken, G.W. Neural substrates for the effects of rehabilitative training on motor recovery after ischemic infarct. Science 1996, 272, 1791–1794. [Google Scholar] [CrossRef] [PubMed]
- Marumoto, K.; Koyama, T.; Hosomi, M.; Takebayashi, T.; Hanada, K.; Ikeda, S.; Kodama, N.; Domen, K. Diffusion tensor imaging predicts the outcome of constraint-induced movement therapy in chronic infarction patients with hemiplegia: A pilot study. Restor. Neurol. Neurosci. 2013, 31, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Nair, V.A.; Young, B.M.; Walton, L.M.; Nigogosyan, Z.; Remsik, A.; Tyler, M.E.; Farrar-Edwards, D.; Caldera, K.E.; Sattin, J.A.; et al. DTI measures track and predict motor function outcomes in stroke rehabilitation utilizing BCI technology. Front. Hum. Neurosci. 2015, 9, 195. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.T.; Lin, K.C.; Liu, H.L.; Chen, Y.L.; Wu, C.Y. Changes in structural integrity are correlated with motor and functional recovery after post-stroke rehabilitation. Restor. Neurol. Neurosci. 2015, 33, 835–844. [Google Scholar] [CrossRef] [PubMed]
- Ueda, R.; Yamada, N.; Kakuda, W.; Abo, M.; Senoo, A. White matter structure and clinical characteristics of stroke patients: A diffusion tensor MRI study. Brain Res. 2016, 1635, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Yamada, N.; Ueda, R.; Kakuda, W.; Momosaki, R.; Kondo, T.; Hada, T.; Sasaki, N.; Hara, T.; Senoo, A.; Abo, M. Diffusion Tensor Imaging Evaluation of Neural Network Development in Patients Undergoing Therapeutic Repetitive Transcranial Magnetic Stimulation following Stroke. Neural Plast. 2018, 2018, 39010160. [Google Scholar] [CrossRef]
- Ueda, R.; Yamada, N.; Abo, M.; Senoo, A. Relationship between motor function improvements and white matter structure after low-frequency repetitive transcranial magnetic stimulation plus intensive occupational therapy in chronic subcortical stroke patients. Neuroreport 2019, 30, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Pinter, D.; Gattringer, T.; Fandler-Höfler, S.; Kneihsl, M.; Eppinger, S.; Deutschmann, H.; Pichler, A.; Poltrum, B.; Reishofer, G.; Ropele, S.; et al. Early Progressive Changes in White Matter Integrity Are Associated with Stroke Recovery. Transl. Stroke Res. 2020, 11, 1264–1272. [Google Scholar] [CrossRef] [PubMed]
- Wanni Arachchige, P.R.; Karunarathna, S.; Meidian, A.C.; Ueda, R.; Uchida, W.; Abo, M.; Senoo, A. Structural connectivity changes in the motor execution network after stroke rehabilitation. Restor. Neurol. Neurosci. 2021, 39, 237–245. [Google Scholar] [CrossRef] [PubMed]
- Bullmore, E.; Sporns, O. Complex brain networks: Graph theoretical analysis of structural and functional systems. Nat. Rev. Neurosci. 2009, 10, 186–198. [Google Scholar] [CrossRef] [PubMed]
- Rubinov, M.; Sporns, O. Complex network measures of brain connectivity: Uses and interpretations. Neuroimage 2010, 52, 1059–1069. [Google Scholar] [CrossRef]
- Shi, L.; Wang, D.; Chu, W.C.; Liu, S.; Xiong, Y.; Wang, Y.; Wang, Y.; Wong, L.K.; Mok, V.C. Abnormal organization of white matter network in patients with no dementia after ischemic stroke. PLoS ONE 2013, 8, e81388. [Google Scholar] [CrossRef]
- Schlemm, E.; Schulz, R.; Bönstrup, M.; Krawinkel, L.; Fiehler, J.; Gerloff, C.; Thomalla, G.; Cheng, B. Structural brain networks and functional motor outcome after stroke-a prospective cohort study. Brain Commun. 2020, 2, fcaa001. [Google Scholar] [CrossRef] [PubMed]
- Brunnstrom, S. Motor testing procedures in hemiplegia: Based on sequential recovery stages. Phys. Ther. 1966, 46, 357–375. [Google Scholar] [CrossRef]
- Wassermann, E.M. Risk and safety of repetitive transcranial magnetic stimulation: Report and suggested guidelines from the International Workshop on the Safety of Repetitive Transcranial Magnetic Stimulation, June 5–7, 1996. Electroencephalogr. Clin. Neurophysiol. 1998, 108, 1–16. [Google Scholar] [CrossRef]
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar] [CrossRef]
- Gladstone, D.J.; Danells, C.J.; Black, S.E. The fugl-meyer assessment of motor recovery after stroke: A critical review of its measurement properties. Neurorehabil. Neural Repair 2002, 16, 232–240. [Google Scholar] [CrossRef]
- Lyle, R.C. A performance test for assessment of upper limb function in physical rehabilitation treatment and research. Int. J. Rehabil. Res. 1981, 4, 483–492. [Google Scholar] [CrossRef]
- Desikan, R.S.; Ségonne, F.; Fischl, B.; Quinn, B.T.; Dickerson, B.C.; Blacker, D.; Buckner, R.L.; Dale, A.M.; Maguire, R.P.; Hyman, B.T.; et al. An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. Neuroimage 2006, 31, 968–980. [Google Scholar] [CrossRef]
- Wang, J.; Wang, X.; Xia, M.; Liao, X.; Evans, A.; He, Y. GRETNA: A graph theoretical network analysis toolbox for imaging connectomics. Front. Hum. Neurosci. 2015, 9, 386. [Google Scholar] [PubMed]
- Onoda, K. Basis of graph theory on brain imaging study. Jpn. J. Physiol. Psychol. Psychophysiol. 2015, 33, 231–238. [Google Scholar] [CrossRef][Green Version]
- Wright, L.M.; De Marco, M.; Venneri, A. A Graph Theory Approach to Clarifying Aging and Disease Related Changes in Cognitive Networks. Front. Aging Neurosci. 2021, 13, 676618. [Google Scholar] [CrossRef] [PubMed]
- Scharwächter, L.; Schmitt, F.J.; Pallast, N.; Fink, G.R.; Aswendt, M. Network analysis of neuroimaging in mice. Neuroimage 2022, 253, 119110. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Yu, C.; Chen, H.; Qin, W.; He, Y.; Fan, F.; Zhang, Y.; Wang, M.; Li, K.; Zang, Y.; et al. Dynamic functional reorganization of the motor execution network after stroke. Brain 2010, 133, 1224–1238. [Google Scholar] [CrossRef] [PubMed]
- Jiang, T.; He, Y.; Zang, Y.; Weng, X. Modulation of functional connectivity during the resting state and the motor task. Hum. Brain Mapp. 2004, 22, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Mazrooyisebdani, M.; Nair, V.A.; Loh, P.L.; Remsik, A.B.; Young, B.M.; Moreno, B.S.; Dodd, K.C.; Kang, T.J.; William, J.C.; Prabhakaran, V. Evaluation of Changes in the Motor Network Following BCI Therapy Based on Graph Theory Analysis. Front. Neurosci. 2018, 12, 861. [Google Scholar] [CrossRef] [PubMed]
- Bush, G.; Luu, P.; Posner, M.I. Cognitive and emotional influences in anterior cingulate cortex. Trends Cogn. Sci. 2000, 4, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Allman, J.M.; Hakeem, A.; Erwin, J.M.; Nimchinsky, E.; Hof, P. The anterior cingulate cortex. The evolution of an interface between emotion and cognition. Ann. N. Y. Acad. Sci. 2001, 935, 107–117. [Google Scholar] [CrossRef]
- Maeshima, S.; Osawa, A. Structure and network of inside and orbital side on cerebrum. Jpn. J. Neuropsychol. 2017, 33, 222–228. [Google Scholar]
- Rehme, A.K.; Eickhoff, S.B.; Wang, L.E.; Fink, G.R.; Grefkes, C. Dynamic causal modeling of cortical activity from the acute to the chronic stage after stroke. Neuroimage 2011, 55, 1147–1158. [Google Scholar] [CrossRef]
- Takekawa, T.; Kakuda, W.; Uchiyama, M.; Ikegaya, M.; Abo, M. Brain perfusion and upper limb motor function: A pilot study on the correlation between evolution of asymmetry in cerebral blood flow and improvement in Fugl-Meyer Assessment score after rTMS in chronic post-stroke patients. J. Neuroradiol. 2014, 41, 177–183. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Left Hemiplegia n = 9 | Right Hemiplegia n = 5 | |
|---|---|---|
| Age at intervention, Mean ± SD (years) | 59.3 ± 12.0 | 61.2 ± 14.0 |
| Gender, n (%) | ||
| Female | 4 (44) | 2 (40) |
| Male | 5 (56) | 3 (60) |
| Duration after stroke, Mean ± SD (days) | 1064.6 ± 956.4 | 1434.4 ± 1865.0 |
| Subtype of stroke, n (%) | ||
| Cerebral hemorrhage | 5 (56) | 5 (100) |
| Cerebral infarction | 4 (44) | 0 (0) |
| Brunnstrom stage, n (%) | ||
| Upper limb | ||
| III | 0 (0) | 3 (60) |
| IV | 3 (33) | 1 (20) |
| V | 6 (67) | 1 (20) |
| Hand and fingers | ||
| III | 3 (33) | 4 (80) |
| IV | 3 (33) | 0 (0) |
| V | 3 (33) | 1 (20) |
| Left Hemiplegia n = 9 | Right Hemiplegia n = 5 | All Patients n = 14 | |
|---|---|---|---|
| FMA-UE scores | |||
| Before rehabilitation | 44.8 ± 14.1 | 24.0 ± 17.4 | 37.4 ± 17.9 |
| After rehabilitation | 49.2 ± 11.2 | 28.2 ± 17.9 | 41.7 ± 16.8 |
| (p-value) | (p = 0.0141) | (p = 0.0579) | (p = 0.0016) |
| ARAT scores | |||
| Before rehabilitation | 26.6 ± 17.1 | 9.0 ± 11.8 | 20.3 ± 17.3 |
| After rehabilitation | 29.6 ± 18.0 | 11.0 ± 12.7 | 22.9 ± 18.3 |
| (p-value) | (p = 0.0220) | (p = 0.3710) | (p = 0.0088) |
| Left Hemiplegia | Right Hemiplegia | |
|---|---|---|
| Degree centrality Nodal efficiency | Ih banks of superior temporal sulcus * Ih isthmus of cingulate gyrus * Ih paracentral lobule * Ih postcentral gyrus * | (No significant change) |
| Betweenness centrality | Ch caudal anterior cingulate cortex * Ih banks of superior temporal sulcus * Ih isthmus of cingulate gyrus * Ih postcentral gyrus * | (No significant change) |
| Nodal clustering coefficient | Ch caudal anterior cingulate cortex * Ih isthmus of cingulate gyrus * Ih postcentral gyrus ** | (No significant change) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kimura, I.; Senoo, A.; Abo, M. Changes in Structural Neural Networks in the Recovery Process of Motor Paralysis after Stroke. Brain Sci. 2024, 14, 197. https://doi.org/10.3390/brainsci14030197
Kimura I, Senoo A, Abo M. Changes in Structural Neural Networks in the Recovery Process of Motor Paralysis after Stroke. Brain Sciences. 2024; 14(3):197. https://doi.org/10.3390/brainsci14030197
Chicago/Turabian StyleKimura, Ikuo, Atsushi Senoo, and Masahiro Abo. 2024. "Changes in Structural Neural Networks in the Recovery Process of Motor Paralysis after Stroke" Brain Sciences 14, no. 3: 197. https://doi.org/10.3390/brainsci14030197
APA StyleKimura, I., Senoo, A., & Abo, M. (2024). Changes in Structural Neural Networks in the Recovery Process of Motor Paralysis after Stroke. Brain Sciences, 14(3), 197. https://doi.org/10.3390/brainsci14030197