
Transcranial Direct Current Stimulation for Orthopedic Pain: A Systematic Review with Meta-Analysis
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Literature Search
2.3. Study Selection
2.4. Assessment of Methodological Quality
2.5. Statistical Analysis
2.6. Certainty of Evidence
3. Results
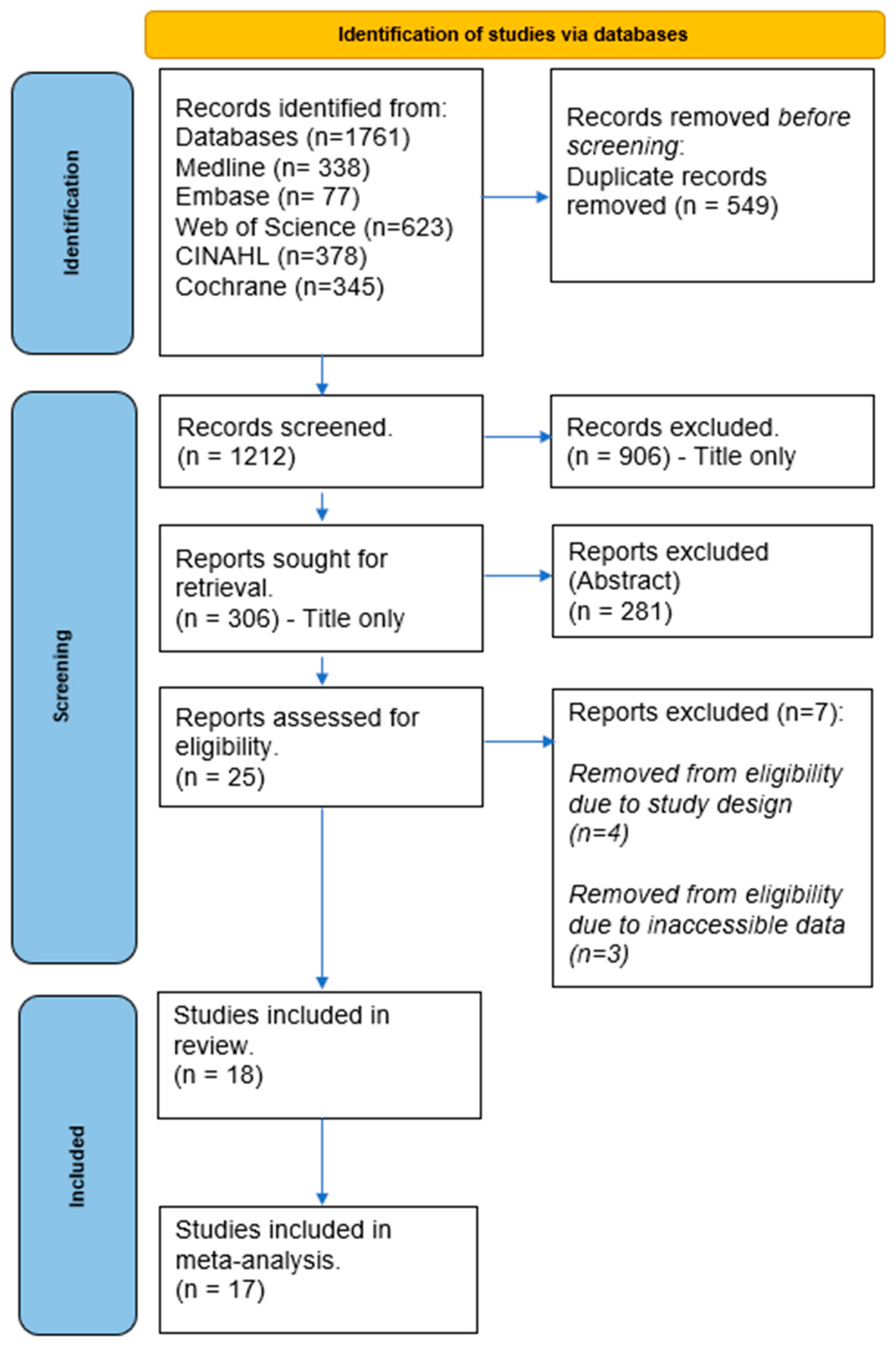
3.1. Search Findings
3.2. Study Characteristics
3.3. Intervention
3.3.1. Knee Pain
3.3.2. Lower Back Pain
3.3.3. Shoulder Pain
3.3.4. Orofacial Pain
3.3.5. Sham and Blinding
3.4. Quality Assessment
3.5. Meta-Analysis
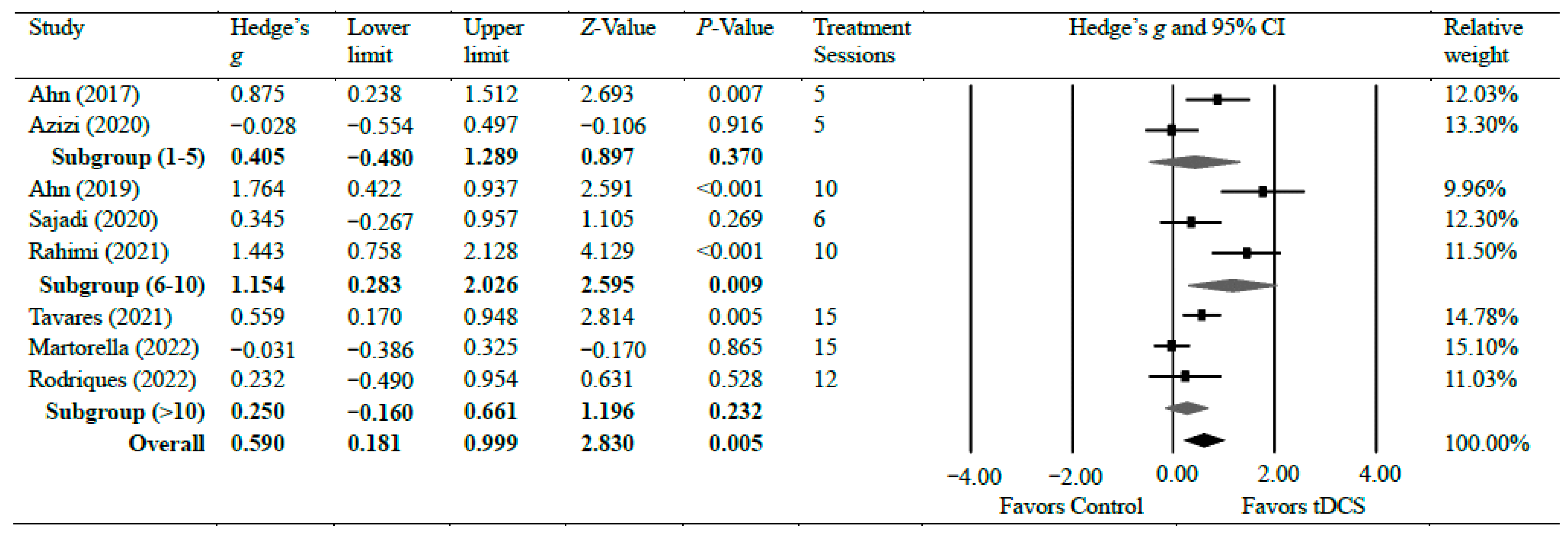
3.5.1. Knee Pain
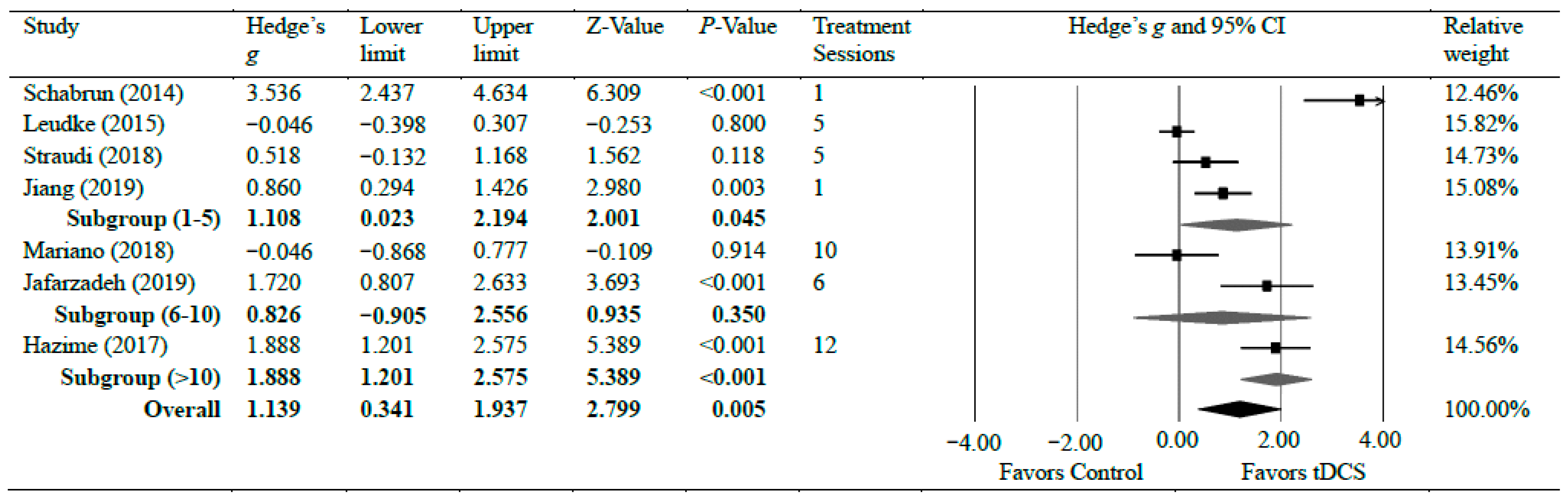
3.5.2. Lower Back Pain
3.5.3. Shoulder Pain
3.5.4. Orofacial Pain
4. Discussion
4.1. Knee Pain
4.2. Lower Back Pain
4.3. Shoulder Pain
4.4. Other Chronic Orthopedic Joint Pain
4.5. Clinical Implication
4.6. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cohen, S.P.; Vase, L.; Hooten, W.M. Chronic pain: An update on burden, best practices, and new advances. Lancet 2021, 397, 2082–2097. [Google Scholar] [CrossRef] [PubMed]
- Hylands-White, N.; Duarte, R.V.; Raphael, J.H. An overview of treatment approaches for chronic pain management. Rheumatol. Int. 2017, 37, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, R.H.; O’Connor, A.B.; Backonja, M.; Farrar, J.T.; Finnerup, N.B.; Jensen, T.S.; Kalso, E.A.; Loeser, J.D.; Miaskowski, C.; Nurmikko, T.J.; et al. Pharmacologic management of neuropathic pain: Evidence-based recommendations. Pain 2007, 132, 237–251. [Google Scholar] [CrossRef] [PubMed]
- Steingrímsdóttir, Ó.A.; Landmark, T.; Macfarlane, G.J.; Nielsen, C.S. Defining chronic pain in epidemiological studies: A systematic review and meta-analysis. Pain 2017, 158, 2092–2107. [Google Scholar] [CrossRef] [PubMed]
- Fregni, F.; Nitsche, M.A.; Loo, C.K.; Brunoni, A.R.; Marangolo, P.; Leite, J.; Carvalho, S.; Bolognini, N.; Caumo, W.; Paik, N.J.; et al. Regulatory Considerations for the Clinical and Research Use of Transcranial Direct Current Stimulation (tDCS): Review and recommendations from an expert panel. Clin. Res. Regul. Aff. 2015, 32, 22–35. [Google Scholar] [CrossRef] [PubMed]
- Coffman, B.A.; Clark, V.P.; Parasuraman, R. Battery powered thought: Enhancement of attention, learning, and memory in healthy adults using transcranial direct current stimulation. Neuroimage 2014, 85 Pt 3, 895–908. [Google Scholar] [CrossRef] [PubMed]
- Parasuraman, R.; McKinley, R.A. Using noninvasive brain stimulation to accelerate learning and enhance human performance. Hum. Factors 2014, 56, 816–824. [Google Scholar] [CrossRef] [PubMed]
- van Griensven, H.; Schmid, A.; Trendafilova, T.; Low, M. Central Sensitization in Musculoskeletal Pain: Lost in Translation? J. Orthop. Sports Phys. Ther. 2020, 50, 592–596. [Google Scholar] [CrossRef]
- Latremoliere, A.; Woolf, C.J. Central sensitization: A generator of pain hypersensitivity by central neural plasticity. J. Pain 2009, 10, 895–926. [Google Scholar] [CrossRef]
- Kold, S.; Graven-Nielsen, T. Modulation Of Experimental Prolonged Pain and Sensitization Using High-Definition Transcranial Direct Current Stimulation: A Double-Blind, Sham-Controlled Study. J. Pain 2022, 23, 1220–1233. [Google Scholar] [CrossRef]
- Shirahige, L.; Melo, L.; Nogueira, F.; Rocha, S.; Monte-Silva, K. Efficacy of Noninvasive Brain Stimulation on Pain Control in Migraine Patients: A Systematic Review and Meta-Analysis. Headache 2016, 56, 1565–1596. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.E.; Yu, B.; Zhang, W.; Chen, W.H.; Qi, Q.; Miao, Y. Effiectiveness and safety of transcranial direct current stimulation in fibromyalgia: A systematic review and meta-analysis. J. Rehabil. Med. 2017, 49, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Hazime, F.A.; Baptista, A.F.; Freitas, D.G.; Monteiro, R.L.; Maretto, R.L.; Hasue, R.H.; João, S.M.A. Treating low back pain with combined cerebral and peripheral electrical stimulation: A randomized, double-blind, factorial clinical trial. Eur. J. Pain 2017, 21, 1132–1143. [Google Scholar] [CrossRef] [PubMed]
- Luedtke, K.; Rushton, A.; Wright, C.; Jürgens, T.; Polzer, A.; Mueller, G.; May, A. Effectiveness of transcranial direct current stimulation preceding cognitive behavioural management for chronic low back pain: Sham controlled double blinded randomised controlled trial. BMJ (Clin. Res. Ed.) 2015, 350, h1640. [Google Scholar] [CrossRef] [PubMed]
- Schabrun, S.M.; Jones, E.; Elgueta Cancino, E.L.; Hodges, P.W. Targeting chronic recurrent low back pain from the top-down and the bottom-up: A combined transcranial direct current stimulation and peripheral electrical stimulation intervention. Brain Stimul. 2014, 7, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Tsao, H.; Galea, M.P.; Hodges, P.W. Reorganization of the motor cortex is associated with postural control deficits in recurrent low back pain. Brain 2008, 131, 2161–2171. [Google Scholar] [CrossRef]
- Clark, B.C.; Issac, L.C.; Lane, J.L.; Damron, L.A.; Hoffman, R.L. Neuromuscular plasticity during and following 3 wk of human forearm cast immobilization. J. Appl. Physiol. 2008, 105, 868–878. [Google Scholar] [CrossRef]
- Ngernyam, N.; Jensen, M.P.; Arayawichanon, P.; Auvichayapat, N.; Tiamkao, S.; Janjarasjitt, S.; Punjaruk, W.; Amatachaya, A.; Aree-uea, B.; Auvichayapat, P. The effects of transcranial direct current stimulation in patients with neuropathic pain from spinal cord injury. Clin. Neurophysiol. 2015, 126, 382–390. [Google Scholar] [CrossRef]
- Rahimi, F.; Nejati, V.; Nassadj, G.; Ziaei, B.; Mohammadi, H.K. The effect of transcranial direct stimulation as an add-on treatment to conventional physical therapy on pain intensity and functional ability in individuals with knee osteoarthritis: A randomized controlled trial. Neurophysiol. Clin. 2021, 51, 507–516. [Google Scholar] [CrossRef]
- Alwardat, M.; Pisani, A.; Etoom, M.; Carpenedo, R.; Chine, E.; Dauri, M.; Leonardis, F.; Natoli, S. Is transcranial direct current stimulation (tDCS) effective for chronic low back pain? A systematic review and meta-analysis. J. Neural Transm. 2020, 127, 1257–1270. [Google Scholar] [CrossRef]
- Cai, G.S.; Xia, Z.; Charvet, L.; Xiao, F.F.; Datta, A.; Androulakis, X.M. A Systematic Review and Meta-Analysis on the Efficacy of Repeated Transcranial Direct Current Stimulation for Migraine. J. Pain Res. 2021, 14, 1171–1183. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, D.M.; Wittkopf, P.G.; Arendsen, L.J.; Jones, A.K.P. Is Transcranial Direct Current Stimulation (tDCS) Effective for the Treatment of Pain in Fibromyalgia? A Systematic Review and Meta-Analysis. J. Pain 2020, 21, 1085–1100. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Rev. Esp. Cardiol. (Engl. Ed.) 2021, 74, 790–799. [Google Scholar] [CrossRef] [PubMed]
- Wewege, M.A.; Jones, M.D.; Williams, S.A.; Kamper, S.J.; McAuley, J.H. Rescaling pain intensity measures for meta-analyses of analgesic medicines for low back pain appears justified: An empirical examination from randomised trials. BMC Med. Res. Methodol. 2022, 22, 285. [Google Scholar] [CrossRef] [PubMed]
- Cashin, A.G.; McAuley, J.H. Clinimetrics: Physiotherapy Evidence Database (PEDro) Scale. J. Physiother. 2020, 66, 59. [Google Scholar] [CrossRef]
- Elkins, M.R.; Moseley, A.M.; Sherrington, C.; Herbert, R.D.; Maher, C.G. Growth in the Physiotherapy Evidence Database (PEDro) and use of the PEDro scale. Br. J. Sports Med. 2013, 47, 188–189. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Paige, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; Cochrane: London, UK, 2020. [Google Scholar]
- Pollock, A.; Farmer, S.E.; Brady, M.C.; Langhorne, P.; Mead, G.E.; Mehrholz, J.; van Wijck, F.; Wiffen, P.J. An algorithm was developed to assign GRADE levels of evidence to comparisons within systematic reviews. J. Clin. Epidemiol. 2016, 70, 106–110. [Google Scholar] [CrossRef]
- Ahn, H.; Woods, A.J.; Kunik, M.E.; Bhattacharjee, A.; Chen, Z.G.; Choi, E.; Fillingim, R.B. Efficacy of transcranial direct current stimulation over primary motor cortex (anode) and contralateral supraorbital area (cathode) on clinical pain severity and mobility performance in persons with knee osteoarthritis: An experimenter- and participant-blinded, randomized, sham-controlled pilot clinical study. Brain Stimul. 2017, 10, 902–909. [Google Scholar] [CrossRef]
- Ahn, H.; Zhong, C.X.; Miao, H.Y.; Chaoul, A.; Park, L.; Yen, I.H.; Vila, M.A.; Sorkpor, S.; Abdi, S. Efficacy of combining home-based transcranial direct current stimulation with mindfulness-based meditation for pain in older adults with knee osteoarthritis: A randomized controlled pilot study. J. Clin. Neurosci. 2019, 70, 140–145. [Google Scholar] [CrossRef]
- Azizi, S.; Rezasoltani, Z.; Najafi, S.; Mohebi, B.; Tabatabaee, S.M.; Dadarkhah, A. Transcranial direct current stimulation for knee osteoarthritis: A single-blind randomized sham-controlled trial. Neurophysiol. Clin. 2021, 51, 329–338. [Google Scholar] [CrossRef]
- Choi, Y.H.; Jung, S.J.; Lee, C.H.; Lee, S.U. Additional effects of transcranial direct-current stimulation and trigger-point injection for treatment of myofascial pain syndrome: A pilot study with randomized, single-blinded trial. J. Altern. Complement. Med. 2014, 20, 698–704. [Google Scholar] [CrossRef] [PubMed]
- Jafarzadeh, A.; Ehsani, F.; Yosephi, M.H.; Zoghi, M.; Jaberzadeh, S. Concurrent postural training and M1 anodal transcranial direct current stimulation improve postural impairment in patients with chronic low back pain. J. Clin. Neurosci. 2019, 68, 224–234. [Google Scholar] [CrossRef] [PubMed]
- Jiang, N.; Wei, J.; Li, G.; Wei, B.; Zhu, F.F.; Hu, Y. Effect of dry-electrode-based transcranial direct current stimulation on chronic low back pain and low back muscle activities: A double-blind sham-controlled study. Restor. Neurol. Neurosci. 2020, 38, 41–54. [Google Scholar] [CrossRef] [PubMed]
- Mariano, T.Y.; Burgess, F.W.; Bowker, M.; Kirschner, J.; Van’t Wout-Frank, M.; Jones, R.N.; Halladay, C.W.; Stein, M.; Greenberg, B.D. Transcranial Direct Current Stimulation for Affective Symptoms and Functioning in Chronic Low Back Pain: A Pilot Double-Blinded, Randomized, Placebo-Controlled Trial. Pain. Med. 2019, 20, 1166–1177. [Google Scholar] [CrossRef] [PubMed]
- Martorella, G.; Mathis, K.; Miao, H.; Wang, D.; Park, L.; Ahn, H. Self-administered transcranial direct current stimulation for pain in older adults with knee osteoarthritis: A randomized controlled study. Brain Stimul. 2022, 15, 902–909. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, L.B.; Lopes, T.S.; Soares, C.; Maluf, R.; Goes, B.T.; Sá, K.N.; Baptista, A.F. Transcranial direct current stimulation and exercises for treatment of chronic temporomandibular disorders: A blind randomised-controlled trial. J. Oral Rehabil. 2015, 42, 723–732. [Google Scholar] [CrossRef]
- Rodrigues, G.M.; Paixão, A.; Arruda, T.; de Oliveira, B.R.R.; Maranhão Neto, G.A.; Marques Neto, S.R.; Lattari, E.; Machado, S. Anodal Transcranial Direct Current Stimulation Increases Muscular Strength and Reduces Pain Perception in Women With Patellofemoral Pain. J. Strength Cond. Res. 2022, 36, 371–378. [Google Scholar] [CrossRef]
- Sajadi, S.; Karimi, M.; Forogh, B.; Raissi, G.R.; Zarnegar, F.; Ahadi, T. Randomized clinical trial comparing of transcranial direct current stimulation (tDCS) and transcutaneous electrical nerve stimulation (TENS) in knee osteoarthritis. Neurophysiol. Clin. 2020, 50, 367–374. [Google Scholar] [CrossRef]
- Sakrajai, P.; Janyacharoen, T.; Jensen, M.P.; Sawanyawisuth, K.; Auvichayapat, N.; Tunkamnerdthai, O.; Keeratitanont, K.; Auvichayapat, P. Pain reduction in myofascial pain syndrome by anodal transcranial direct current stimulation combined with standard treatment: A randomized controlled study. Clin. J. Pain 2014, 30, 1076–1083. [Google Scholar] [CrossRef]
- Straudi, S.; Buja, S.; Baroni, A.; Pavarelli, C.; Pranovi, G.; Fregni, F.; Basaglia, N. The effects of transcranial direct current stimulation (tDCS) combined with group exercise treatment in subjects with chronic low back pain: A pilot randomized control trial. Clin. Rehabil. 2018, 32, 1348–1356. [Google Scholar] [CrossRef] [PubMed]
- Tavares, D.R.B.; Okazaki, J.E.F.; Santana, M.V.A.; Pinto, A.; Tutiya, K.K.; Gazoni, F.M.; Pinto, C.B.; Santos, F.C.; Fregni, F.; Trevisani, V.F.M. Motor cortex transcranial direct current stimulation effects on knee osteoarthritis pain in elderly subjects with dysfunctional descending pain inhibitory system: A randomized controlled trial. Brain Stimul. 2021, 14, 477–487. [Google Scholar] [CrossRef] [PubMed]
- Wen, Y.R.; Shi, J.; Hu, Z.Y.; Lin, Y.Y.; Lin, Y.T.; Jiang, X.; Wang, R.; Wang, X.Q.; Wang, Y.L. Is transcranial direct current stimulation beneficial for treating pain, depression, and anxiety symptoms in patients with chronic pain? A systematic review and meta-analysis. Front. Mol. Neurosci. 2022, 15, 1056966. [Google Scholar] [CrossRef] [PubMed]
- Burston, J.J.; Sagar, D.R.; Shao, P.; Bai, M.; King, E.; Brailsford, L.; Turner, J.M.; Hathway, G.J.; Bennett, A.J.; Walsh, D.A.; et al. Cannabinoid CB2 receptors regulate central sensitization and pain responses associated with osteoarthritis of the knee joint. PLoS ONE 2013, 8, e80440. [Google Scholar] [CrossRef] [PubMed]
- Maarrawi, J.; Peyron, R.; Mertens, P.; Costes, N.; Magnin, M.; Sindou, M.; Laurent, B.; Garcia-Larrea, L. Motor cortex stimulation for pain control induces changes in the endogenous opioid system. Neurology 2007, 69, 827–834. [Google Scholar] [CrossRef] [PubMed]
- Pinto, C.B.; Teixeira Costa, B.; Duarte, D.; Fregni, F. Transcranial Direct Current Stimulation as a Therapeutic Tool for Chronic Pain. J. ECT 2018, 34, e36–e50. [Google Scholar] [CrossRef]
- Desai, M.J.; Saini, V.; Saini, S. Myofascial pain syndrome: A treatment review. Pain Ther. 2013, 2, 21–36. [Google Scholar] [CrossRef]
- Boggio, P.S.; Zaghi, S.; Lopes, M.; Fregni, F. Modulatory effects of anodal transcranial direct current stimulation on perception and pain thresholds in healthy volunteers. Eur. J. Neurol. 2008, 15, 1124–1130. [Google Scholar] [CrossRef]
- Sanzarello, I.; Merlini, L.; Rosa, M.A.; Perrone, M.; Frugiuele, J.; Borghi, R.; Faldini, C. Central sensitization in chronic low back pain: A narrative review. J. Back Musculoskelet. Rehabil. 2016, 29, 625–633. [Google Scholar] [CrossRef]
- Lefaucheur, J.P.; Antal, A.; Ayache, S.S.; Benninger, D.H.; Brunelin, J.; Cogiamanian, F.; Cotelli, M.; De Ridder, D.; Ferrucci, R.; Langguth, B.; et al. Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS). Clin. Neurophysiol. 2017, 128, 56–92. [Google Scholar] [CrossRef]
- Keeser, D.; Meindl, T.; Bor, J.; Palm, U.; Pogarell, O.; Mulert, C.; Brunelin, J.; Möller, H.J.; Reiser, M.; Padberg, F. Prefrontal transcranial direct current stimulation changes connectivity of resting-state networks during fMRI. J. Neurosci. 2011, 31, 15284–15293. [Google Scholar] [CrossRef] [PubMed]
- Meeker, T.J.; Keaser, M.L.; Khan, S.A.; Gullapalli, R.P.; Seminowicz, D.A.; Greenspan, J.D. Non-invasive Motor Cortex Neuromodulation Reduces Secondary Hyperalgesia and Enhances Activation of the Descending Pain Modulatory Network. Front. Neurosci. 2019, 13, 467. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pain Area | Author (Year) | Total (tx/c) a | Age (Mean) | Pain Condition | tDCS Mode | tDCS Placement | Control | Intensity (mA) | Duration (min) | Total Sessions (S) Frequency (F) Length of Tx (L) | Other Interventions | Pain Outcome | Finding e |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Knee | Ahn (2017) [30] | 40 (20/20) | 60.0 | Knee OA | Anodal | M1 (Contra) c | Sham | 2 | 20 | S:5; F:Daily; L:1 wk | None | NRS | Improved |
| Ahn (2019) [31] | 30 (15/15) | 59.5 | Knee OA | Anodal | M1 (Contra) c | Sham | 2 | 20 | S:10; F:Daily; L:2 wk | MBM | NRS | Improved | |
| Azizi (2021) [32] | 54 (27/27) | 58.9 | Knee OA | Anodal | M1 (Contra) c | Sham | 2 | 20 | S:5; F:Daily; L:1 wk | None | VAS | Improved | |
| Sajadi (2020) [40] | 40 (20/20) | 58.1 | Knee OA | Anodal | M1 (Contra) c | PES | 2 | 20 | S:6; F:3 x/wk; L:2 wk | EX | VAS | NC | |
| Rahimi (2021) [19] | 80 (20/20) | 58.8 | Knee OA | Anodal | M1, S1, DLPFC (Contra) c | Sham | 1 | 20 | S:10; F:Daily; L:2 wk | EX | VAS | Improved | |
| Tavares (2021) [43] | 104 (51/53) | 73.9 | Knee OA | Anodal | M1 (Contra) c | Sham | 2 | 20 | S:15; F:Daily; L:3 wk | None | VAS | Improved | |
| Martorella (2022) [37] | 120 (60/60) | 66.0 | Knee OA | Anodal | M1 (Contra) c | Sham | 2 | 20 | S:15; F:Daily; L:3 wk | None | NRS | Improved | |
| Rodrigues (2022) [39] | 28 (14/14) | 22.9 | PFPS | Anodal | M1 (B/L) c | Sham | 2 | 20 | S:12; F:2–3/wk; L:6 wk | EX | VAS | Improved | |
| Lower back | Schabrun (2014) [15] | 16 (16) b | 30.0 | CLBP | Anodal | M1 (Contra) c | Sham | 2 | 30 | S:1 | PES | VAS | NC |
| Leudke (2015) [14] | 135 (67/68) | 44.5 | CLBP | Anodal | M1 (Left) c | Sham | 2 | 20 | S:5; F:Daily; L:1 wk | CBT | VAS | NC | |
| Hazime (2017) [13] | 92 (23/23) b | 52.6 | CLBP | Anodal | M1 (Contra) c | Sham | 2 | 20 | S:12; F:3x/wk; L:4 wk | PES | VAS | NC | |
| Mariano (2019) [36] | 21 (10/11) | 63.2 | CLBP | Anodal | dACC (Left) d | Sham | 2 | 20 | S:10; F:Daily; L:2 wk | None | VAS | NC | |
| Straudi (2018) [42] | 35 (18/17) | 55.1 | CLBP | Anodal | M1 (Contra or B/L) c | Sham | 2 | 20 | S:5; F:Daily; L:1 wk | EX | VAS | Improved | |
| Jafarzadeh (2019) [34] | 36 (12/12) b | 31.6 | CLBP | Anodal | M1 (Left) c | Sham | 2 | 20 | S:6; F:3x/wk; L:2 wk | Postural training | VAS | Improved | |
| Jiang (2020) [35] | 51 (26/25) | 42.0 | CLBP | Anodal | M1 (Dom) c | Sham | 2 | 20 | S:1 | None | NRS | Improved | |
| Shoulder | Choi (2014) [33] | 14 (8/6) | 59.6 | MPS | Anodal | M1, DLPFC (Contra) c | Sham | 2 | 20 | S:5; F:Daily; L:1 wk | None | VAS | Improved |
| Sakrajai (2014) [41] | 31 (16/15) | 47.9 | MPS | Anodal | M1 (Contra) c | Sham | 2 | 20 | S:5; F:Daily; L:1 wk | None | VAS | Improved | |
| Head | Oliviera (2015) [38] | 32 (16/16) | 24.7 | TMJD | Anodal | M1 (Contra) c | Sham | 2 | 20 | S:5; F:Daily; L:1 wk | EX | VAS | NC |
| Pain Area | Author (Year) | Score | Random Allocation | Concealed Allocation | Group Similar at Baseline | Subject Blinding | Therapist Blinding | Assessor Blinding | <15% of Dropouts | Intention-to-Treat Analysis | Between-Group Comparison | Point Estimates and Variability |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Knee | Ahn (2017) [30] | 9 | O | O | O | O | O | O | - | O | O | O |
| Ahn (2019) [31] | 8 | O | O | O | O | O | - | - | O | O | O | |
| Sajadi (2020) [40] | 10 | O | O | O | O | O | O | O | O | O | O | |
| Azizi (2021) [32] | 8 | O | O | O | O | O | - | - | O | O | O | |
| Rahimi (2021) [19] | 9 | O | O | O | O | O | O | - | O | O | O | |
| Tavares (2021) [43] | 10 | O | O | O | O | O | O | O | O | O | O | |
| Martorella (2022) [37] | 10 | O | O | O | O | O | O | O | O | O | O | |
| Rodrigues (2022) [39] | 8 | O | O | O | O | O | - | - | O | O | O | |
| Average | 9 | 100% | 100% | 100% | 100% | 100% | 63% | 38% | 100% | 100% | 100% | |
| Lower back | Schabrun (2014) [15] | 10 | O | O | O | O | O | - | - | O | O | O |
| Leudke (2015) [14] | 9 | O | O | O | O | O | - | O | O | O | O | |
| Hazime (2017) [13] | 10 | O | O | O | O | O | O | O | O | O | O | |
| Mariano (2019) [36] | 8 | O | O | O | O | O | O | O | O | O | O | |
| Straudi (2018) [42] | 10 | O | O | O | O | O | O | O | O | O | O | |
| Jafarzadeh (2019) [34] | 10 | O | O | O | O | O | O | O | O | O | O | |
| Jiang (2020) [35] | 10 | O | O | O | O | O | - | O | O | O | O | |
| Average | 9.6 | 100% | 100% | 100% | 100% | 100% | 63% | 87% | 100% | 100% | 100% | |
| Shoulder | Choi (2009) [33] | 10 | O | O | O | O | O | O | O | O | O | O |
| Sakrajai (2014) [41] | 10 | O | O | O | O | O | O | O | O | O | O | |
| Average | 10 | 100% | 100% | 100% | 100% | 100% | 100% | 100% | 100% | 100% | 100% | |
| Head | Oliviera (2015) [38] | 10 | O | O | O | O | O | O | O | O | O | O |
| Total Avg | 10 | 100% | 100% | 100% | 100% | 100% | 72.2% | 66.7% | 100% | 100% | 100% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adams, W.; Idnani, S.; Kim, J. Transcranial Direct Current Stimulation for Orthopedic Pain: A Systematic Review with Meta-Analysis. Brain Sci. 2024, 14, 66. https://doi.org/10.3390/brainsci14010066
Adams W, Idnani S, Kim J. Transcranial Direct Current Stimulation for Orthopedic Pain: A Systematic Review with Meta-Analysis. Brain Sciences. 2024; 14(1):66. https://doi.org/10.3390/brainsci14010066
Chicago/Turabian StyleAdams, William, Sherina Idnani, and Joosung Kim. 2024. "Transcranial Direct Current Stimulation for Orthopedic Pain: A Systematic Review with Meta-Analysis" Brain Sciences 14, no. 1: 66. https://doi.org/10.3390/brainsci14010066
APA StyleAdams, W., Idnani, S., & Kim, J. (2024). Transcranial Direct Current Stimulation for Orthopedic Pain: A Systematic Review with Meta-Analysis. Brain Sciences, 14(1), 66. https://doi.org/10.3390/brainsci14010066