
Visual Function and Neuropsychological Profiling of Idiopathic Infantile Nystagmus
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Methods
- -
- The Wechsler preschool and primary scale of intelligence, third edition (WPPSI-III) [33], Wechsler preschool and primary scale of intelligence, fourth edition (WPPSI-IV) [34], Wechsler intelligence scale for children, fourth edition (WISC-IV) [35], and Wechsler adult intelligence scale, fourth edition (WAIS-IV) [36]: For the WISC-IV and WAIS-IV, we considered the following scores: (i) the verbal comprehension index (VCI); (ii) the perceptual reasoning index (PRI); (iii) the working memory index (WMI); (iv) the processing speed index (PSI); and (v) the intelligence quotient (IQ). For the WPPSI-III, we collected the following scores: (i) the verbal comprehension index (VCI); (ii) the performance index (PI); (iii) the processing speed index (PSI); and (iv) the total intelligence quotient (TIQ). For the WPPSI-IV, we collected the following scores: (i) the verbal comprehension index (VCI); (ii) the visual–spatial index (VSI) (iii); the fluid reasoning index (FRI) (iv) the working memory index (WMI); (v) the processing speed index (PSI); and (vi) the full-scale IQ (FSIQ).
- -
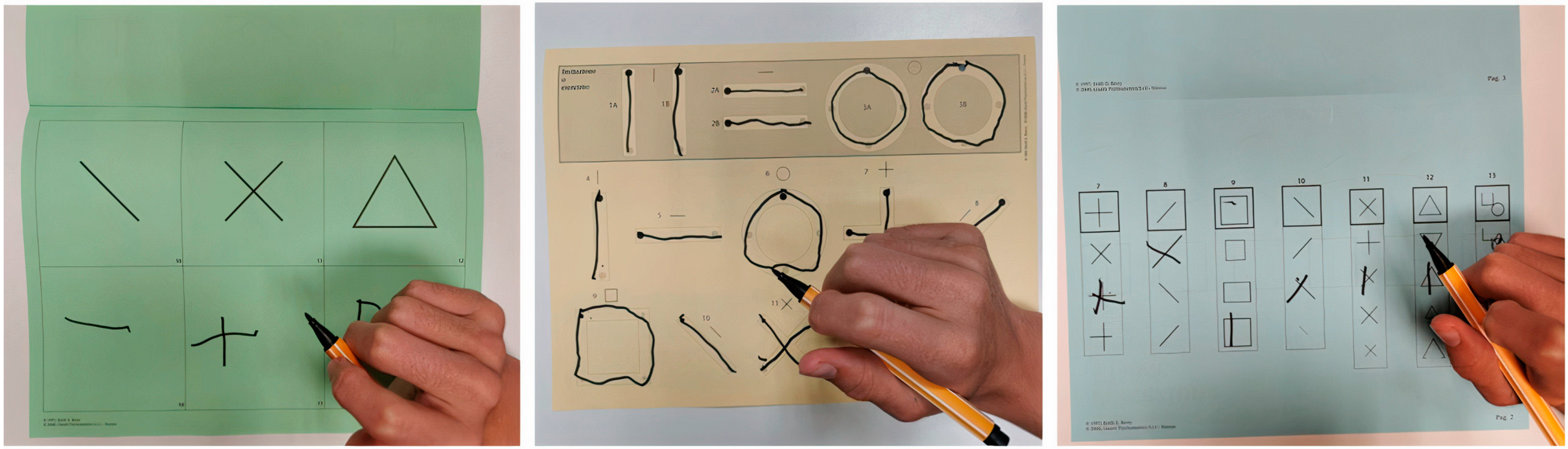
- The Beery developmental test of visual–motor integration (Beery-VMI) [37], composed of the subtests visual perception (VMI-V) and motor coordination (VMI-M): The results were collected in terms of the standard scores and categorized according to the percentiles as normal (>16°P), frail (5°–16°P), or deficient (<5°P). The VMI task evaluates the integration of visual perception and motor skills as the examinee imitates and copies a developmentally sequential series of geometric forms using a pencil and paper. The VMI-V task evaluates an individual’s visual abilities without the integration of fine motor skills. The VMI-M task evaluates fine motor skills when not specifically integrated with visual perceptual abilities [38] (see Figure 2).
- -
- The developmental test for visual perception (DTVP) [37]: The general visual perceptual (DTVP-GVP), non-motor visual perceptual (DTVP-NMVP), and visual–motor integration (DTVP-VMI) quotients were collected and categorized according to the percentiles as normal (>16°P), frail (5°–16°P), or deficient (<5°P). The DTVP-2 consists of eight subscales, four of which assess motor-free visual perceptual skills (also referred to as motor-reduced) and four of which assess visual–motor integration.
2.3. Data Analysis and Statistics
3. Results
3.1. Visual Functions and Cognitive Profiles

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Visual Function | Parameter | Number of Subjects | % |
|---|---|---|---|
| Nys waveform | Jerk | 44 | 73.3 |
| Pendular | 6 | 10.0 | |
| Mixed | 10 | 16.7 | |
| Nys direction | Horizontal | 55 | 91.7 |
| Vertical | 2 | 3.3 | |
| Mixed (horizontal and vertical) | 3 | 5.0 | |
| Visual acuity (for far distance) | Not performed for age (grating acuity) | 14 | 23.3 |
| Normal | 10 | 16.7 | |
| Mild low vision (0.5–0.7 logMAR) | 6 | 10 | |
| Moderate low vision (0.7–1 logMAR) | 3 | 5 | |
| Severe low vision (>1 logMAR) | 27 | 45 | |
| Visual acuity (for near distance) | Not performed for age (grating acuity) | 14 | 23.3 |
| Normal | 37 | 61.6 | |
| Mild low vision (0.5–0.7 logMAR) | 7 | 11.5 | |
| Moderate low vision (0.7–1 logMAR) | 2 | 3.2 | |
| Grating acuity | Not necessary for age | 46 | 76.7 |
| Normal | 1 | 1.7 | |
| Reduced (standard distance for age) | 2 | 3.33 | |
| Reduced (only testable for lower distances compared to standard age) | 11 | 18.3 | |
| Head tilt | Absent | 8 | 13.3 |
| Inconstant/variable | 7 | 11.7 | |
| Mild head tilt | 16 | 26.7 | |
| Severe head tilt | 29 | 48.3 | |
| Visual axis alignment | Normal | 47 | 78.3 |
| Mild misalignment with alternating fixation | 12 | 20 | |
| Paralytic misalignment | 1 | 1.7 | |
| Fixation | Stable, durable, binocular; no difference between near and distant | 18 | 30.0 |
| Durable, but not binocular and/or alternating and/or durable, but slightly different from near and distant | 18 | 30.0 | |
| Instable/slightly discontinuous and/or different from near and distant, but sufficiently durable | 22 | 36.7 | |
| Fluctuating/eccentric | 2 | 3.3 | |
| Saccades | Fluid; complete; normal latency, conjugacy, and precision; no evident hypo- or hypermetria | 7 | 11.7 |
| Fluid, incomplete, and/or asymmetric and/or not binocular | 8 | 13.3 | |
| Slight alteration (hypo- or hypermetria, fluidity, latency) | 21 | 35.0 | |
| Moderate alteration (hypo- or hypermetria, fluidity, latency) | 20 | 33.3 | |
| Severe alteration (hypo- or hypermetria, fluidity, latency) | 1 | 1.7 | |
| Sporadic/difficult to elicit (conditioned by attention) | 1 | 1.7 | |
| Not testable due to lack of cooperation or too severe of a clinical picture | 2 | 3.3 | |
| Smooth pursuit | Durable, complete, and binocular | 4 | 6.7 |
| Durable, but incomplete/asymmetric/non binocular | 5 | 8.3 | |
| Slightly discontinuous in all or great parts of directions | 28 | 46.7 | |
| Discontinuous/jerky/augmented latency | 21 | 35.0 | |
| Inconstant/eccentric/fragmented | 2 | 3.3 | |
| Stereopsis | Not testable for age (<6mo) | 2 | 3.3 |
| Present | 15 | 25 | |
| Partial | 9 | 15 | |
| Absent | 14 | 23.3 | |
| Not testable due to lack of cooperation or too severe of a clinical picture | 7 | 11.7 | |
| Missing data | 13 | 21.7 |
3.2. Visual–Cognitive Profiles
3.3. Learning Abilities
4. Discussion
4.1. Visual Function Profiling
4.2. Cognitive and Visual–Cognitive Profiling
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gottlob, I.; Proudlock, F.A. Aetiology of infantile nystagmus. Curr. Opin. Neurol. 2014, 27, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Ehrt, O. Infantile and acquired nystagmus in childhood. Eur. J. Paediatr. Neurol. 2012, 16, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Casteels, I.; Harris, C.M.; Shawkat, F.; Taylor, D. Nystagmus in infancy. Br. J. Ophthalmol. 1992, 76, 434–437. [Google Scholar] [CrossRef] [PubMed]
- Papageorgiou, E.; McLean, R.J.; Gottlob, I. Nystagmus in Childhood. Pediatr. Neonatol. 2014, 55, 341–351. [Google Scholar] [CrossRef]
- Abadi, R.V.; Bjerre, A. Motor and sensory characteristics of infantile nystagmus. Br. J. Ophthalmol. 2002, 86, 1152–1160. [Google Scholar] [CrossRef]
- Ghannam, A.S.B.; Yassine, S. Pediatric Nystagmus. Int. Ophthalmol. Clin. 2018, 58, 23–65. [Google Scholar] [CrossRef]
- Sarvananthan, N.; Surendran, M.; Roberts, E.O.; Jain, S.; Thomas, S.; Shah, N.; Proudlock, F.A.; Thompson, J.R.; McLean, R.J.; Degg, C.; et al. The Prevalence of Nystagmus: The Leicestershire Nystagmus Survey. Investig. Opthalmol. Vis. Sci. 2009, 50, 5201–5206. [Google Scholar] [CrossRef]
- Suppiej, A.; Ceccato, C.; Lonardi, V.; Reffo, M.E. Infantile nystagmus without overt eye abnormality: Early features and neuro-ophthalmological diagnosis. Dev. Med. Child Neurol. 2022, 64, 1532–1538. [Google Scholar] [CrossRef]
- Nash, D.L.; Diehl, N.N.; Mohney, B.G. Incidence and Types of Pediatric Nystagmus. Arch. Ophthalmol. 2017, 182, 31–34. [Google Scholar] [CrossRef]
- Thomas, M.G. FRMD7 -Related Infantile Nystagmus Summary; GeneReviews®: Seattle, WA, USA, 2009; pp. 1–17. [Google Scholar]
- Aychoua, N.; Schiff, E.; Malka, S.; Tailor, V.K.; Chan, H.W.; Oluonye, N.; Theodorou, M.; Moosajee, M. Prospective study of pediatric patients presenting with idiopathic infantile nystagmus—Management and molecular diagnostics. Front. Genet. 2022, 13, 977806. [Google Scholar] [CrossRef]
- Kashou, N.H.; Zampini, A.R. Oculomotor Neurocircuitry, a Structural Connectivity Study of Infantile Nystagmus Syndrome. PLoS ONE 2015, 10, e0125380. [Google Scholar] [CrossRef]
- Thomas, M.G.; Crosier, M.; Lindsay, S.; Kumar, A.; Araki, M.; Leroy, B.P.; McLean, R.J.; Sheth, V.; Maconachie, G.; Thomas, S.; et al. Abnormal retinal development associated with FRMD7 mutations. Hum. Mol. Genet. 2014, 23, 4086–4093. [Google Scholar] [CrossRef] [PubMed]
- Toufeeq, S.; Gottlob, I.; Tu, Z.; Proudlock, F.A.; Pilat, A. Abnormal Retinal Vessel Architecture in Albinism and Idiopathic Infantile Nystagmus. Investig. Opthalmol. Vis. Sci. 2022, 63, 33. [Google Scholar] [CrossRef]
- Brodsky, M.C.; Dell’osso, L.F. A Unifying Neurologic Mechanism for Infantile Nystagmus. JAMA Ophthalmol. 2014, 132, 761–768. [Google Scholar] [CrossRef] [PubMed]
- Stahl, J.S.; Plant, G.T.; Leigh, R.J. Medical treatment of nystagmus and its visual consequences. J. R. Soc. Med. 2002, 95, 235–237. [Google Scholar] [CrossRef] [PubMed]
- Dale, N.; Sakkalou, E.; O’Reilly, M.; Springall, C.; De Haan, M.; Salt, A. Functional vision and cognition in infants with congenital disorders of the peripheral visual system. Dev. Med. Child Neurol. 2017, 59, 725–731. [Google Scholar] [CrossRef]
- Bathelt, J.; Dale, N.J.; de Haan, M.; A Clark, C. Brain structure in children with congenital visual disorders and visual impairment. Dev. Med. Child Neurol. 2020, 62, 125–131. [Google Scholar] [CrossRef]
- Jacobs, J.B.; Dell’osso, L.F. Congenital nystagmus: Hypotheses for its genesis and complex waveforms within a behavioral ocular motor system model. J. Vis. 2004, 4, 7–25. [Google Scholar] [CrossRef]
- Wang, Z.; Dell’osso, L. Factors influencing pursuit ability in infantile nystagmus syndrome: Target timing and foveation capability. Vis. Res. 2009, 49, 182–189. [Google Scholar] [CrossRef]
- Fu, V.L.N.; Bilonick, R.A.; Felius, J.; Hertle, R.W.; Birch, E.E. Visual Acuity Development of Children with Infantile Nystagmus Syndrome. Investig. Opthalmol. Vis. Sci. 2011, 52, 1404–1411. [Google Scholar] [CrossRef]
- Dai, B.; Cham, K.M.; Abel, L.A. Perception of Coherent Motion in Infantile Nystagmus Syndrome. Investig. Opthalmol. Vis. Sci. 2022, 63, 31. [Google Scholar] [CrossRef] [PubMed]
- Ukwade, M.T.; Bedell, H.E. Spatial-bisection acuity in infantile nystagmus. Vis. Res. 2012, 64, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Dai, B.; Cham, K.M.; Abel, L.A. Velocity Discrimination in Infantile Nystagmus Syndrome. Investig. Opthalmol. Vis. Sci. 2021, 62, 35. [Google Scholar] [CrossRef] [PubMed]
- Nandy, A.S.; Tjan, B.S. Saccade-confounded image statistics explain visual crowding. Nat. Neurosci. 2012, 15, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Tailor, V.K.; Theodorou, M.; Dahlmann-Noor, A.H.; Dekker, T.M.; Greenwood, J.A. Eye movements elevate crowding in idiopathic infantile nystagmus syndrome. J. Vis. 2021, 21, 9. [Google Scholar] [CrossRef]
- Barot, N.; McLean, R.J.; Gottlob, I.; Proudlock, F.A. Reading Performance in Infantile Nystagmus. Ophthalmology 2013, 120, 1232–1238. [Google Scholar] [CrossRef]
- Robson, A.G.; Frishman, L.J.; Grigg, J.; Hamilton, R.; Jeffrey, B.G.; Kondo, M.; Li, S.; McCulloch, D.L. ISCEV Standard for full-field clinical electroretinography (2022 update). Doc. Ophthalmol. 2022, 144, 165–177. [Google Scholar] [CrossRef]
- Hamilton, R.; Bach, M.; Heinrich, S.P.; Hoffmann, M.B.; Odom, J.V.; McCulloch, D.L.; Thompson, D.A. ISCEV extended protocol for VEP methods of estimation of visual acuity. Doc. Ophthalmol. 2021, 142, 17–24. [Google Scholar] [CrossRef]
- Brecelj, J.; Stirn-Kranjc, B. Visual electrophysiological screening in diagnosing infants with congenital nystagmus. Clin. Neurophysiol. 2004, 115, 461–470. [Google Scholar] [CrossRef]
- Signorini, S.; Luparia, A.; Cappagli, G.; Perotto, E.; Antonini, M.; Morelli, F.; Aprile, G.; Ballante, E.; Figini, S.; Borgatti, R.; et al. Visual Function Score: A New Clinical Tool to Assess Visual Function and Detect Visual Disorders in Children. Front. Pediatr. 2022, 10, 868974. [Google Scholar] [CrossRef]
- Morelli, F.; Toni, F.; Saligari, E.; D’Abrusco, F.; Serpieri, V.; Ballante, E.; Ruberto, G.; Borgatti, R.; Valente, E.M.; Signorini, S.; et al. Visual function in children with Joubert syndrome. Dev. Med. Child Neurol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Wechsler, D. Wechsler Preschool and Primay Scale of Intelligence—Third Edition (WPPSI-III) Technical and Interpretive Manual; The Psychological Corp.: San Antonio, TX, USA, 2002. [Google Scholar]
- Watkins, M.W.; Beaujean, A.A. Bifactor structure of the Wechsler Preschool and Primary Scale of Intelligence—Fourth Edition. Sch. Psychol. Q. 2014, 29, 52–63. [Google Scholar] [CrossRef] [PubMed]
- Grizzle, R. Wechsler Intelligence Scale for Children, Fourth Edition. Encycl. Child Behav. Dev. 2011, 1553–1555. [Google Scholar] [CrossRef]
- Ryan, J.J.; Schnakenberg-Ott, S.D. Scoring reliability on the Wechsler Adult Intelligence Scale-Third Edition (WAIS-III). Assessment 2003, 10, 151–159. [Google Scholar] [CrossRef]
- Brown, T. Validity and Reliability of the Developmental Test of Visual Perception—Third Edition (DTVP-3). Occup. Ther. Heal. Care 2016, 30, 272–287. [Google Scholar] [CrossRef] [PubMed]
- McCrimmon, A.W.; Altomare, A.A.; Matchullis, R.L.; Jitlina, K. Test Review: The Beery Developmental Test of Visual-Motor Integration. J. Psychoeduc. Assess. 2012, 30, 588–592. [Google Scholar] [CrossRef]
- Sartori, G.; Job, R.; Tressoldi, P.E. Batteria Per La Valutazione Della Dislessia e Della Disortografia Evolutiva; Giunti Psychometrics: Firenze FI, Italy, 1995. [Google Scholar]
- Cornoldi, C.; Carretti, B. Prove MT-3 Clinica La Valutazione Delle Abilità Di Lettura e Comprensione per La Scuola Primaria e Secondaria Di I Grado; Giunti Editore: Milano, MI, Italy, 2016. [Google Scholar]
- R Development Core Team. R: A Language and Environment for Statistical Computing, Dalgaard, Peter (Producer). 2010.
- Buchner, A.; Erdfelder, F.; Lang, A.G. G* Power Manual. Retrieved Novemb. 2014, 15, 2016. [Google Scholar]
- Sakki, H.; Bowman, R.; Sargent, J.; Kukadia, R.; Dale, N. Visual function subtyping in children with early-onset cerebral visual impairment. Dev. Med. Child Neurol. 2021, 63, 303–312. [Google Scholar] [CrossRef]
- Mayes, S.D.; Calhoun, S.L. Learning, Attention, Writing, and Processing Speed in Typical Children and Children with ADHD, Autism, Anxiety, Depression, and Oppositional-Defiant Disorder. Child Neuropsychol. 2007, 13, 469–493. [Google Scholar] [CrossRef]
- Volker, M.A.; Lopata, C.; Vujnovic, R.K.; Smerbeck, A.M.; Toomey, J.A.; Rodgers, J.D.; Schiavo, A.; Thomeer, M.L. Comparison of the Bender Gestalt-II and VMI-V in Samples of Typical Children and Children with High-Functioning Autism Spectrum Disorders. J. Psychoeduc. Assess. 2010, 28, 187–200. [Google Scholar] [CrossRef]
- Hyvärinen, L.; Näsänen, R.; Laurinen, P. New visual acuity test for pre-school children. Acta Ophthalmol. 2009, 58, 507–511. [Google Scholar] [CrossRef]
- Teller, D.Y.; McDonald, M.A.; Preston, K.; Sebris, S.L.; Dobson, V. Assessment of visual acuity in infants and children; the acuity card procedure. Dev. Med. Child Neurol. 2008, 28, 779–789. [Google Scholar] [CrossRef] [PubMed]
- Thomas, M.G.; Gottlob, I.; McLean, R.J.; Maconachie, G.; Kumar, A.; Proudlock, F.A. Reading Strategies in Infantile Nystagmus Syndrome. Investig. Opthalmol. Vis. Sci. 2011, 52, 8156–8165. [Google Scholar] [CrossRef] [PubMed]
- Colenbrander, A. Assessment of functional vision and its rehabilitation. Acta Ophthalmol. 2010, 88, 163–173. [Google Scholar] [CrossRef]
- Kurent, A.; Stirn-Kranjc, B.; Brecelj, J. Electroretinographic Characteristics in Children with Infantile Nystagmus Syndrome and Early-Onset Retinal Dystrophies. Eur. J. Ophthalmol. 2015, 25, 33–42. [Google Scholar] [CrossRef]
- Saunders, K.J.; Brown, G.; McCulloch, D.L. Pattern-onset visual evoked potentials: More useful than reversal for patients with nystagmus. Doc. Ophthalmol. 1997, 94, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Pieh, C.; Gottlob, I. Infantile nystagmus. Monatsschr. Kinderheilkd. 2010, 158, 653–660. [Google Scholar] [CrossRef]
- Kushner, B.J. Ocular Causes of Abnormal Head Postures. Ophthalmology 1979, 86, 2115–2125. [Google Scholar] [CrossRef]
- Pel, J.J.M.; Kooiker, M.J.G.; van der Does, J.M.E.; Boot, F.H.; de Faber, J.T.; van der Steen-Kant, S.P.; van der Steen, J. Orienting Responses to Various Visual Stimuli in Children With Visual Processing Impairments or Infantile Nystagmus Syndrome. J. Child Neurol. 2014, 29, 1632–1637. [Google Scholar] [CrossRef]
- Hindmarsh, G.P.; A Black, A.; White, S.L.; Hopkins, S.; Wood, J.M. Eye movement patterns and reading ability in children. Ophthalmic Physiol. Opt. 2021, 41, 1134–1143. [Google Scholar] [CrossRef]
- Morelli, F.; Aprile, G.; Martolini, C.; Ballante, E.; Olivier, L.; Ercolino, E.; Perotto, E.; Signorini, S. Visual Function and Neuropsychological Profile in Children with Cerebral Visual Impairment. Children 2022, 9, 921. [Google Scholar] [CrossRef] [PubMed]
- Gottlob, I. Nystagmus. Curr. Opin. Ophthalmol. 2000, 11, 330–335. [Google Scholar] [CrossRef] [PubMed]
- Crawford, J.R.; Anderson, V.; Rankin, P.M.; MacDonald, J. An index-based short-form of the WISC-IV with accompanying analysis of the reliability and abnormality of differences. Br. J. Clin. Psychol. 2010, 49, 235–258. [Google Scholar] [CrossRef] [PubMed]
- Bauer, A.N.B.J.L.; Gershon, P.J.D.S.S.; Jerry, R.C.M.D.S.; Philip, T.D.W.S.Z. David Heaton Robert K. VIII. NIH Toolbox Cognition Battery (CB): Composite scores of crystallized, fluid, and overall cognition. Monogr. Soc. Res. Child Dev. 2013, 78, 119. [Google Scholar]
- Kaufman, A.S.; Flanagan, D.P.; Alfonso, V.C.; Mascolo, J.T. Test review: Wechsler intelligence scale for children, (WISC-IV). J. Psychoeduc. Assess. 2006, 24, 278–295. [Google Scholar] [CrossRef]
- Huurneman, B.; Boonstra, F.N.; Cox, R.F.; Cillessen, A.H.; van Rens, G. A systematic review on ‘Foveal Crowding’ in visually impaired children and perceptual learning as a method to reduce Crowding. BMC Ophthalmol. 2012, 12, 27. [Google Scholar] [CrossRef]
- Oliveras-Rentas, R.E.; Kenworthy, L.; Roberson, R.B.; Martin, A.; Wallace, G.L. WISC-IV Profile in High-Functioning Autism Spectrum Disorders: Impaired Processing Speed is Associated with Increased Autism Communication Symptoms and Decreased Adaptive Communication Abilities. J. Autism Dev. Disord. 2012, 42, 655–664. [Google Scholar] [CrossRef]
- Shmukler, A.; Latanov, A.V.; Karyakina, M.; Anisimov, V.N.; Churikova, M.A.; Sukhachevsky, I.S.; Spektor, V.A. Eye Movements and Cognitive Functioning in Patients With Schizophrenia Spectrum Disorders: Network Analysis. Front. Psychiatry 2021, 12, 736228. [Google Scholar] [CrossRef]
- Walg, M.; Hapfelmeier, G.; El-Wahsch, D.; Prior, H. The faster internal clock in ADHD is related to lower processing speed: WISC-IV profile analyses and time estimation tasks facilitate the distinction between real ADHD and pseudo-ADHD. Eur. Child Adolesc. Psychiatry 2017, 26, 1177–1186. [Google Scholar] [CrossRef]
- Poletti, M. WISC-IV intellectual profiles in Italian children with specific learning disorder and related impairments in reading, written expression, and mathematics. J. Learn. Disabil. 2016, 49, 320–335. [Google Scholar] [CrossRef]
- Calhoun, S.L.; Mayes, S.D. Processing speed in children with clinical disorders. Psychol. Sch. 2005, 42, 333–343. [Google Scholar] [CrossRef]
- Atkinson, J.; Braddick, O. Visual development. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2020; Volume 173, pp. 121–142. [Google Scholar]
- Longcamp, M.; Velay, J.-L.; Berninger, V.W.; Richards, T. Neuroanatomy of Handwriting and Related Reading and Writing Skills in Adults and Children with and without Learning Disabilities: French-American Connections. Pratiques 2016, 171–172. [Google Scholar] [CrossRef]
- Mayes, S.D.; Calhoun, S.L.; Bixler, E.O.; Zimmerman, D.N. IQ and neuropsychological predictors of academic achievement. Learn. Individ. Differ. 2009, 19, 238–241. [Google Scholar] [CrossRef]
- Fazzi, E.; Signorini, S.G.; Bova, S.M.; La Piana, R.; Ondei, P.; Bertone, C.; Misefari, W.; Bianchi, P.E. Spectrum of Visual Disorders in Children With Cerebral Visual Impairment. J. Child Neurol. 2007, 22, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Green, R.R.; Bigler, E.D.; Froehlich, A.; Prigge, M.B.D.; Travers, B.G.; Cariello, A.N.; Anderson, J.S.; Zielinski, B.A.; Alexander, A.; Lange, N.; et al. Beery VMI performance in autism spectrum disorder. Child Neuropsychol. 2016, 22, 795–817. [Google Scholar] [CrossRef]
- Sutton, G.P.; Barchard, K.A.; Bello, D.T.; Thaler, N.S.; Ringdahl, E.; Mayfield, J.; Allen, D.N. Beery-Buktenica Developmental Test of Visual-Motor Integration performance in children with traumatic brain injury and attention-deficit/hyperactivity disorder. Psychol. Assess. 2011, 23, 805–809. [Google Scholar] [CrossRef] [PubMed]
- Clausi, S.; De Luca, M.; Chiricozzi, F.R.; Tedesco, A.M.; Casali, C.; Molinari, M.; Leggio, M.G. Oculomotor deficits affect neuropsychological performance in oculomotor apraxia type 2. Cortex 2013, 49, 691–701. [Google Scholar] [CrossRef]
- Ibrahimi, A.P.; Mendiola-Santibañez, D.; Gkaros, J.D. Analysis of the potential impact of strabismus with and without amblyopia on visual-perceptual and visual-motor skills evaluated using TVPS-3 and VMI-6 tests. J. Optom. 2021, 14, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Battajon, N.; Bechini, C.; De Osti, F.; Galletti, A.; Frigo, A.C.; Lago, P. Neurodevelopmental outcomes of very low birth weight preterms in preschool childhood: A prospective cohort study. Ital. J. Pediatr. 2023, 49, 56. [Google Scholar] [CrossRef] [PubMed]
- Daibert-Nido, M.; Pyatova, Y.; Markowitz, M.; Taheri-Shirazi, M.; Markowitz, S.N. Post audio-visual biofeedback training visual functions and quality of life in paediatric idiopathic infantile nystagmus: A pilot study. Eur. J. Ophthalmol. 2021, 31, 3324–3331. [Google Scholar] [CrossRef]




| Parameter | n | % | |
|---|---|---|---|
| Sex | F | 17 | 28.3 |
| M | 43 | 71.7 | |
| Age | Mean: 7.0 Y | Median: 6.9 Y | Range: 0.2–17.9 Y |
| WISC-IV (N = 18) | Index | N Performed/Interpretable | Mean | Median | Range | Standard Deviation |
| W_VCI | 18 | 109.7 | 108 | 88–140 | 14.4 | |
| W_PRI | 18 | 109.3 | 108.5 | 85–139 | 15.1 | |
| W_WMI | 17 | 103.4 | 97 | 82–127 | 16.9 | |
| W_PSI | 18 | 94.1 | 98.5 | 62–115 | 14.9 | |
| W_IQ | 15 | 104.7 | 102 | 76–141 | 15.8 |
| Visual–Cognitive Test | Subtest | Mean | Median | Range | SD | Category | Count (%) |
|---|---|---|---|---|---|---|---|
| Beery-VMI (n = 27) | VMI-V | 107.9 | 104 | 84–152 | 13.2 | deficit (<5°p) | 0 |
| frailty (5°–16°p) | 2 | ||||||
| normal (>16°p) | 25 | ||||||
| VMI-M | 93.9 | 97 | 63–115 | 15.9 | deficit (<5°p) | 1 | |
| frailty (5°–16°p) | 6 | ||||||
| normal (>16°p) | 20 | ||||||
| VMI-SS | 96.1 | 95 | 73–131 | 13.2 | deficit (<5°p) | 1 | |
| frailty (5°–16°p) | 3 | ||||||
| normal (>16°p) | 23 | ||||||
| DTVP (n = 27) | GVP | 102.0 | 103 | 82–134 | 12.1 | deficit (<5°p) | 0 |
| frailty (5°–16°p) | 3 | ||||||
| normal (>16°p) | 24 | ||||||
| MRVP | 104.6 | 105 | 78–143 | 15.8 | deficit (<5°p) | 0 | |
| frailty (5°–16°p) | 1 | ||||||
| normal (>16°p) | 26 | ||||||
| VMI | 98.7 | 100 | 35–72 | 12.1 | deficit (<5°p) | 3 | |
| frailty (5°–16°p) | 2 | ||||||
| normal (>16°p) | 22 |
| Learning Ability Test | Normal (%) | Deficit (%) |
|---|---|---|
| Reading speed (n = 20) | 15 (75) | 5 (25) |
| Reading accuracy (n = 20) | 18 (90) | 2 (10) |
| Text comprehension (n = 19) | 15 (79) | 4 (21) |
| Writing (n = 16) | 14 (88) | 2 (12) |
| Math (n = 20) | 14 (70) | 6 (30) |
| Total (n = 20) | 7 (35) | 13 (65) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morelli, F.; Catalano, G.; Scognamillo, I.; Balzarotti, N.; Luparia, A.; Olivier, L.; Bertone, C.; Gori, M.; Signorini, S. Visual Function and Neuropsychological Profiling of Idiopathic Infantile Nystagmus. Brain Sci. 2023, 13, 1348. https://doi.org/10.3390/brainsci13091348
Morelli F, Catalano G, Scognamillo I, Balzarotti N, Luparia A, Olivier L, Bertone C, Gori M, Signorini S. Visual Function and Neuropsychological Profiling of Idiopathic Infantile Nystagmus. Brain Sciences. 2023; 13(9):1348. https://doi.org/10.3390/brainsci13091348
Chicago/Turabian StyleMorelli, Federica, Guido Catalano, Ilaria Scognamillo, Nicolò Balzarotti, Antonella Luparia, Lucrezia Olivier, Chiara Bertone, Monica Gori, and Sabrina Signorini. 2023. "Visual Function and Neuropsychological Profiling of Idiopathic Infantile Nystagmus" Brain Sciences 13, no. 9: 1348. https://doi.org/10.3390/brainsci13091348
APA StyleMorelli, F., Catalano, G., Scognamillo, I., Balzarotti, N., Luparia, A., Olivier, L., Bertone, C., Gori, M., & Signorini, S. (2023). Visual Function and Neuropsychological Profiling of Idiopathic Infantile Nystagmus. Brain Sciences, 13(9), 1348. https://doi.org/10.3390/brainsci13091348