
Artificial Intelligence Frameworks to Detect and Investigate the Pathophysiology of Spaceflight Associated Neuro-Ocular Syndrome (SANS)

 , , and
, , and
Abstract
1. Introduction
2. Spaceflight-Associated Neuro-Ocular Syndrome (SANS)
Proposed Pathophysiology of SANS
3. Medical Diagnostic Challenges during Spaceflight
3.1. Delayed Communication and Imaging Transmission
3.2. Limited Individuals Undergoing Spaceflight
4. Imaging Onboard the International Space Station
- 1.
- Fundus photography: Fundus photography is a non-invasive imaging modality that captures detailed images of the retina, optic nerve, and blood vessels. This technique can be used to detect and monitor a variety of ocular abnormalities, including diabetic retinopathy, glaucoma, macular degeneration, and retinal detachment [52].
- 2.
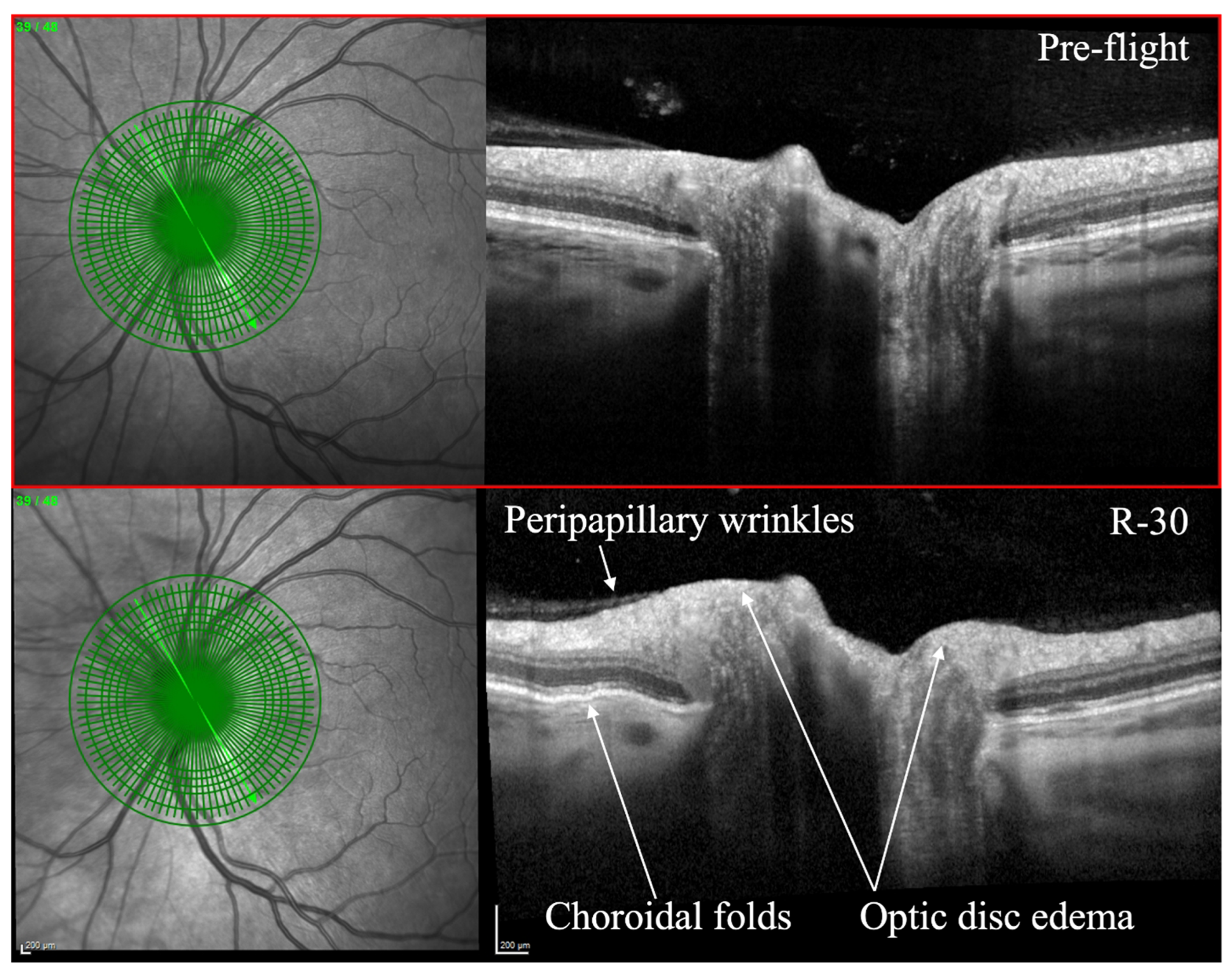
- Optical coherence tomography (OCT): OCT is an imaging technique that utilizes light waves to produce a detailed, cross-sectional image of the retina. This technique can provide detailed information on the thickness of the retinal layers, which can be useful for diagnosing and monitoring conditions such as macular edema, macular holes, and vitreomacular traction [53,54]. OCT can also be used to monitor changes in the retinal nerve fiber layer thickness, which is important for diagnosing and monitoring glaucoma [55]. OCT has been utilized to evaluate SANS during and after spaceflight (Figure 1) [7]. As of 2018, OCT angiography (OCTA) and MultiColor Imaging became available onboard on the ISS [1]. These recent advances will allow for additional insights into changes within the retina and retinal vasculature during spaceflight.
- 3.
- Orbital ultrasound: Orbital ultrasound is a non-invasive imaging technique that employs sound waves to produce images of the structures in and around the eye. This technique can be used to visualize the optic nerve and surrounding tissues, which can be useful for diagnosing and monitoring conditions such as optic nerve swelling (papilledema), retinal detachment, and retrobulbar hematoma [56].
5. Introduction to Artificial Intelligence-Based Diagnosis in Ophthalmic Imaging
6. Convolutional Neural Networks, Supervised Learning, and Unsupervised Learning for SANS
6.1. Convolutional Neural Networks
6.2. Similarities and Differences between Supervised and Unsupervised Learning
6.3. Supervised Learning for SANS
6.4. Unsupervised Learning for SANS
7. Generative Adversarial Networks
7.1. GANS for Denoising Retinal Imaging and Data Generation
7.2. GAN Non-Invasive Angiogram Synthesis for SANS
8. Transfer Learning
- -
- Addressing Data Scarcity: Space missions often have limited resources, including medical data. Transfer learning helps AI systems overcome the problem of sparse data by using prior knowledge from large, publicly accessible datasets such as ImageNet.
- -
- Effective Model Training: The amount of computing power and training time are reduced when pre-trained models are fine-tuned using a limited dataset of retinal pictures acquired in space. In resource-constrained areas such as space, this effectiveness is important. Furthermore, transfer learning combined with pre-trained models allows AI systems to identify ocular anomalies in astronauts with high accuracy, assisting in the early detection and treatment of SANS-related problems.
9. Limitations of the Application of Artificial Intelligence to SANS
10. Future Direction and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lee, A.G.; Mader, T.H.; Gibson, C.R.; Tarver, W.; Rabiei, P.; Riascos, R.F.; Galdamez, L.A.; Brunstetter, T. Spaceflight associated neuro-ocular syndrome (SANS) and the neuro-ophthalmologic effects of microgravity: A review and an update. npj Microgravity 2020, 6, 7. [Google Scholar] [CrossRef]
- Patel, Z.S.; Brunstetter, T.J.; Tarver, W.J.; Whitmire, A.M.; Zwart, S.R.; Smith, S.M.; Huff, J.L. Red risks for a journey to the red planet: The highest priority human health risks for a mission to Mars. npj Microgravity 2020, 6, 33. [Google Scholar] [CrossRef]
- Xu, Y.; Liu, X.; Cao, X.; Huang, C.; Liu, E.; Qian, S.; Liu, X.; Wu, Y.; Dong, F.; Qiu, C.-W.; et al. Artificial intelligence: A powerful paradigm for scientific research. Innovation 2021, 2, 100179. [Google Scholar] [CrossRef]
- Hardy, M.; Harvey, H. Artificial intelligence in diagnostic imaging: Impact on the radiography profession. Br. J. Radiol. 2020, 93, 20190840. [Google Scholar] [CrossRef]
- Mader, T.H.; Gibson, C.R.; Pass, A.F.; Kramer, L.A.; Lee, A.G.; Fogarty, J.; Tarver, W.J.; Dervay, J.P.; Hamilton, D.R.; Sargsyan, A.; et al. Optic Disc Edema, Globe Flattening, Choroidal Folds, and Hyperopic Shifts Observed in Astronauts after Long-duration Space Flight. Ophthalmology 2011, 118, 2058–2069. [Google Scholar] [CrossRef]
- Waisberg, E.; Ong, J.; Masalkhi, M.; Lee, A.G. Optic neuropathy in spaceflight-associated neuro-ocular syndrome (SANS). Ir. J. Med Sci. (1971-) 2023, 1–3. [Google Scholar] [CrossRef]
- Ong, J.; Tarver, W.; Brunstetter, T.; Mader, T.H.; Gibson, C.R.; Mason, S.S.; Lee, A. Spaceflight associated neuro-ocular syndrome: Proposed pathogenesis, terrestrial analogues, and emerging countermeasures. Br. J. Ophthalmol. 2023, 107, 895–900. [Google Scholar] [CrossRef]
- Waisberg, E.; Ong, J.; Lee, A.G. Factors Associated with Optic Disc Edema Development during Spaceflight. JAMA Ophthalmol. 2023, 141, 409. [Google Scholar] [CrossRef]
- Zhang, L.-F.; Hargens, A.R. Spaceflight-Induced Intracranial Hypertension and Visual Impairment: Pathophysiology and Countermeasures. Physiol. Rev. 2018, 98, 59–87. [Google Scholar] [CrossRef]
- Nelson, E.S.; Mulugeta, L.; Myers, J.G. Microgravity-Induced Fluid Shift and Ophthalmic Changes. Life 2014, 4, 621–665. [Google Scholar] [CrossRef]
- Klarica, M.; Radoš, M.; Erceg, G.; Petošić, A.; Jurjević, I.; Orešković, D. The Influence of Body Position on Cerebrospinal Fluid Pressure Gradient and Movement in Cats with Normal and Impaired Craniospinal Communication. PLoS ONE 2014, 9, e95229. [Google Scholar] [CrossRef] [PubMed]
- Marshall-Goebel, K.; Laurie, S.S.; Alferova, I.V.; Arbeille, P.; Auñón-Chancellor, S.M.; Ebert, D.J.; Lee, S.M.C.; Macias, B.R.; Martin, D.S.; Pattarini, J.M.; et al. Assessment of Jugular Venous Blood Flow Stasis and Thrombosis during Spaceflight. JAMA Netw. Open 2019, 2, e1915011. [Google Scholar] [CrossRef]
- Orešković, D.; Bulat, M. Hydrostatic Force in Regulation of CSF Volume; Springer: Berlin, Heidelberg, 1993. [Google Scholar] [CrossRef]
- Waisberg, E.; Ong, J.; Masalkhi, M.; Lee, A.G.; Berdahl, J. Anatomical considerations for reducing ocular emergencies during spaceflight. Ir. J. Med. Sci. (1971-) 2023, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Ong, J.; Mader, T.H.; Gibson, C.R.; Mason, S.S.; Lee, A.G. Spaceflight associated neuro-ocular syndrome (SANS): An update on potential microgravity-based pathophysiology and mitigation development. Eye 2023, 1–7. [Google Scholar] [CrossRef]
- Buckey, J.C.; Lan, M.; Phillips, S.D.; Archambault-Leger, V.; Fellows, A.M. A theory for why the spaceflight-associated neuro-ocular syndrome develops. J. Appl. Physiol. 2022, 132, 1201–1203. [Google Scholar] [CrossRef] [PubMed]
- Kirsch, K.A.; Röcker, L.; Gauer, O.H.; Krause, R.; Leach, C.; Wicke, H.J.; Landry, R. Venous Pressure in Man during Weightlessness. Science 1984, 225, 218–219. [Google Scholar] [CrossRef]
- Norsk, P. Adaptation of the cardiovascular system to weightlessness: Surprises, paradoxes and implications for deep space missions. Acta Physiol. 2020, 228, e13434. [Google Scholar] [CrossRef]
- Buckey, J.C.; Phillips, S.D.; Anderson, A.P.; Chepko, A.B.; Archambault-Leger, V.; Gui, J.; Fellows, A.M. Microgravity-induced ocular changes are related to body weight. Am. J. Physiol. Integr. Comp. Physiol. 2018, 315, R496–R499. [Google Scholar] [CrossRef]
- Buckey, J.C.; Phillips, S.D.; Anderson, A.P.; Chepko, A.B.; Archambault-Leger, V.; Masterova, K.S.; Fellows, A.M.; Cowan, D.R. The im-portance of tissue weight and tissue compressive forces in human spaceflight. In Proceedings of the 68th International Astronautical Congress, Adelaide, Australia, 25–29 September 2017; International Astronautical Federation: Adelaide, Australia. [Google Scholar]
- Strangman, G.E.; Zhang, Q.; Marshall-Goebel, K.; Mulder, E.; Stevens, B.; Clark, J.B.; Bershad, E.M. Increased cerebral blood volume pulsatility during head-down tilt with elevated carbon dioxide: The SPACECOT Study. J. Appl. Physiol. 2017, 123, 62–70. [Google Scholar] [CrossRef]
- Roberts, D.R.; Albrecht, M.H.; Collins, H.R.; Asemani, D.; Chatterjee, A.R.; Spampinato, M.V.; Zhu, X.; Chimowitz, M.I.; Antonucci, M.U. Effects of Spaceflight on Astronaut Brain Structure as Indicated on MRI. N. Engl. J. Med. 2017, 377, 1746–1753. [Google Scholar] [CrossRef]
- Shinojima, A.; Kakeya, I.; Tada, S. Association of Space Flight with Problems of the Brain and Eyes. JAMA Ophthalmol. 2018, 136, 1075–1076. [Google Scholar] [CrossRef] [PubMed]
- Jessen, N.A.; Munk, A.S.F.; Lundgaard, I.; Nedergaard, M. The Glymphatic System—A Beginner’s Guide. Neurochem Res. 2015, 40, 2583–2599. [Google Scholar] [CrossRef]
- Wostyn, P.; Mader, T.H.; Nedergaard, M.; Gibson, C.R. Does Long-Duration Exposure to Microgravity Lead to Dysregulation of the Brain and Ocular Glymphatic Systems? Eye Brain 2022, 14, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Mathieu, E.; Gupta, N.; Ahari, A.; Zhou, X.; Hanna, J.; Yücel, Y.H. Evidence for Cerebrospinal Fluid Entry Into the Optic Nerve via a Glymphatic Pathway. Investig. Opthalmology Vis. Sci. 2017, 58, 4784–4791. [Google Scholar] [CrossRef]
- Wang, X.; Lou, N.; Eberhardt, A.; Yang, Y.; Kusk, P.; Xu, Q.; Förstera, B.; Peng, S.; Shi, M.; Ladrón-De-Guevara, A.; et al. An ocular glymphatic clearance system removes β-amyloid from the rodent eye. Sci. Transl. Med. 2020, 12, eaaw3210. [Google Scholar] [CrossRef] [PubMed]
- Wostyn, P.; De Deyn, P.P. The “Ocular Glymphatic System”: An Important Missing Piece in the Puzzle of Optic Disc Edema in Astronauts? Investig. Ophthalmol. Vis. Sci. 2018, 59, 20190–22091. [Google Scholar] [CrossRef]
- Zwart, S.R.; Gregory, J.F.; Zeisel, S.H.; Gibson, C.R.; Mader, T.H.; Kinchen, J.M.; Ueland, P.M.; Ploutz-Snyder, R.; Heer, M.A.; Smith, S.M. Genotype, B-vitamin status, and androgens affect spaceflight-induced ophthalmic changes. FASEB J. 2016, 30, 141–148. [Google Scholar] [CrossRef]
- Zwart, S.R.; Laurie, S.S.; Chen, J.J.; Macias, B.R.; Lee, S.M.C.; Stenger, M.; Grantham, B.; Carey, K.; Young, M.; Smith, S.M. Association of Genetics and B Vitamin Status with the Magnitude of Optic Disc Edema during 30-Day Strict Head-Down Tilt Bed Rest. JAMA Ophthalmol. 2019, 137, 1195–1200. [Google Scholar] [CrossRef]
- Zwart, S.; Gibson, C.; Mäder, T.; Ericson, K.; Ploutz-Snyder, R.; Smith, S. Vision Changes after Spaceflight Are Related to Alterations in Folate–and Vitamin B-12–Dependent One-Carbon Metabolism. SciVee 2012, 142, 427–431. [Google Scholar] [CrossRef]
- Ong, J.; Lee, A.G.; Moss, H.E. Head-Down Tilt Bed Rest Studies as a Terrestrial Analog for Spaceflight Associated Neuro-Ocular Syndrome. Front. Neurol. 2021, 12, 648958. [Google Scholar] [CrossRef]
- Martin Paez, Y.; LI, M.; Subramanian, P.S. Spaceflight Associated Neuro-Ocular Syndrome (SANS): A Systematic Review and Future Directions. Eye Brain 2020, 12, 105–117. [Google Scholar] [CrossRef]
- Zhang, L.F.; Hargens, A.R. Intraocular/Intracranial pressure mismatch hypothesis for visual impairment syndrome in space. Aviat. Space Environ. Med. 2014, 85, 78–80. [Google Scholar] [CrossRef] [PubMed]
- Ong, J.; Lee, A.G. An introduction to space medicine and the physiological effects of spaceflight on the human body. In Spaceflight Associated Neuro-Ocular Syndrome; Elsevier: Amsterdam, The Netherlands, 2022; pp. 1–7. [Google Scholar] [CrossRef]
- Waisberg, E.; Ong, J.; Paladugu, P.; Kamran, S.A.; Zaman, N.; Lee, A.G.; Tavakkoli, A. Challenges of Artificial Intelligence in Space Medicine. Space: Sci. Technol. 2022, 2022, 9852872. [Google Scholar] [CrossRef]
- Ong, J.; Tavakkoli, A.; Zaman, N.; Kamran, S.A.; Waisberg, E.; Gautam, N.; Lee, A.G. Terrestrial health applications of visual assessment technology and machine learning in spaceflight associated neuro-ocular syndrome. npj Microgravity 2022, 8, 37. [Google Scholar] [CrossRef] [PubMed]
- O’byrne, C.; Abbas, A.; Korot, E.; Keane, P.A. Automated deep learning in ophthalmology: AI that can build AI. Curr. Opin. Ophthalmol. 2021, 32, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Padhy, S.K.; Takkar, B.; Chawla, R. Artificial intelligence in diabetic retinopathy: A natural step to the future. Indian J. Ophthalmol. 2019, 67, 1004–1009. [Google Scholar] [CrossRef]
- Ong, J.; Tavakkoli, A.; Strangman, G.; Zaman, N.; Kamran, S.A.; Zhang, Q.; Ivkovic, V.; Lee, A.G. Neuro-ophthalmic imaging and visual assessment technology for spaceflight associated neuro-ocular syndrome (SANS). Surv. Ophthalmol. 2022, 67, 1443–1466. [Google Scholar] [CrossRef]
- Baruah, V.L. Development of Artificial Intelligence Methods for Optical Coherence Tomography Based Medical Diagnostic Ap-plications. 2020. Available online: https://hdl.handle.net/2152/85347 (accessed on 5 May 2023).
- Mosier, K.L.; Fischer, U.M. Meeting the Challenge of Transmission Delay: Communication Protocols for Space Operations. Hum. Factors J. Hum. Factors Ergon. Soc. 2021. [Google Scholar] [CrossRef]
- Hosny, A.; Parmar, C.; Quackenbush, J.; Schwartz, L.H.; Aerts, H.J.W.L. Artificial intelligence in radiology. Nat. Rev. Cancer 2018, 18, 500–510. [Google Scholar] [CrossRef]
- Arbeille, P.; Chaput, D.; Zuj, K.; Depriester, A.; Maillet, A.; Belbis, O.; Benarroche, P.; Barde, S. Remote Echography between a Ground Control Center and the International Space Station Using a Tele-operated Echograph with Motorized Probe. Ultrasound Med. Biol. 2018, 44, 2406–2412. [Google Scholar] [CrossRef]
- Arbeille, P.; Guillon, L.; Zuj, K.; Besnard, S.; Clot, C. A 3D volume capture for ultrasound assessment of various organs and vessels by novice operators. Acta Astronaut. 2022, 201, 75–82. [Google Scholar] [CrossRef]
- Law, J.; Macbeth, P.B. Ultrasound: From Earth to Space. McGill J. Med. 2011, 13, 59. [Google Scholar] [CrossRef] [PubMed]
- Spaceflight Associated Neuro-Ocular Syndrome (SANS) and the Neuro-Ophthalmologic Effects of Microgravity: A Review and an Update|npj Microgravity. Available online: https://www.nature.com/articles/s41526-020-0097-9 (accessed on 5 May 2023).
- Chakrabortty, S.K.; Khodor, Y.L.; Kitchen, R.R.; Miller, D.L.; Babcock, K.M.; Manning, K.S.; Lang, S.P.; Tadigotla, V.; Yu, W.; Bershad, E.; et al. Exosome based analysis for Space Associated Neuro-Ocular Syndrome and health risks in space ex-ploration. npj Microgravity 2022, 8, 40. [Google Scholar] [CrossRef] [PubMed]
- Waisberg, E.; Ong, J.; Masalkhi, M.; Lee, A.G.; Berdahl, J. Wearable, dropless reduction in intraocular pressure as an emerging therapy for glaucoma. Eye 2023, 1–2. [Google Scholar] [CrossRef]
- Ong, J.; Zaman, N.; Waisberg, E.; Kamran, S.A.; Lee, A.G.; Tavakkoli, A. Head-mounted digital metamorphopsia suppression as a countermeasure for macular-related visual distortions for prolonged spaceflight missions and terrestrial health. Wearable Technol. 2022, 3, e26. [Google Scholar] [CrossRef]
- Waisberg, E.; Ong, J.; Zaman, N.; Kamran, S.A.; Lee, A.G.; Tavakkoli, A. Head-Mounted Dynamic Visual Acuity for G-Transition Effects during Interplanetary Spaceflight: Technology Development and Results from an Early Validation Study. Aerosp. Med. Hum. Perform. 2022, 93, 800–805. [Google Scholar] [CrossRef]
- Bennett, T.J.; Barry, C.J. Ophthalmic imaging today: An ophthalmic photographer’s viewpoint—A review. Clin. Exp. Ophthalmol. 2009, 37, 2–13. [Google Scholar] [CrossRef]
- Huang, D.; Swanson, E.A.; Lin, C.P.; Schuman, J.S.; Stinson, W.G.; Chang, W.; Hee, M.R.; Flotte, T.; Gregory, K.; Puliafito, C.A.; et al. Optical Coherence Tomography. Science 1991, 254, 1178–1181. [Google Scholar] [CrossRef]
- Lee, J.; Rosen, R. Optical Coherence Tomography Angiography in Diabetes. Curr. Diabetes Rep. 2016, 16, 123. [Google Scholar] [CrossRef]
- Mwanza, J.-C.; Chang, R.T.; Budenz, D.L.; Durbin, M.K.; Gendy, M.G.; Shi, W.; Feuer, W.J. Reproducibility of Peripapillary Retinal Nerve Fiber Layer Thickness and Optic Nerve Head Parameters Measured with Cirrus HD-OCT in Glaucomatous Eyes. Investig. Opthalmology Vis. Sci. 2010, 51, 5724–5730. [Google Scholar] [CrossRef]
- Dudea, S.M. Ultrasonography of the eye and orbit. Med. Ultrason. 2011, 13, 171–174. [Google Scholar] [PubMed]
- Fischer, U.; Mosier, K.; Orasanu, J. The Impact of Transmission Delays on Mission Control-Space Crew Communication. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2013, 57, 1372–1376. [Google Scholar] [CrossRef]
- Oche, P.A.; Ewa, G.A.; Ibekwe, N. Applications and Challenges of Artificial Intelligence in Space Missions; IEEE: Piscataway, NJ, USA, 2021; p. 1. [Google Scholar] [CrossRef]
- Liu, J.; Malekzadeh, M.; Mirian, N.; Song, T.A.; Liu, C.; Dutta, J. Artificial Intelligence-Based Image Enhancement in PET Imaging: Noise Reduction and Resolution Enhancement. PET Clin. 2021, 16, 553–576. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Lo, A.C.Y. Diabetic Retinopathy: Pathophysiology and Treatments. Int. J. Mol. Sci. 2018, 19, 1816. [Google Scholar] [CrossRef]
- Commissioner, O. Of the FDA Permits Marketing of Artificial Intelligence-Based Device to Detect Certain Diabetes-Related Eye Problems. FDA. 2020. Available online: https://www.fda.gov/news-events/press-announcements/fda-permits-marketing-artificial-intelligence-based-device-detect-certain-diabetes-related-eye (accessed on 5 May 2023).
- Cunningham, P.; Cord, M.; Delany, S.J. Supervised Learning. In Machine Learning Techniques for Multimedia: Case Studies on Organization and Retrievali; Cord, M., Cunningham, P., Eds.; Springer: Berlin/Heidelberg, Germany, 2008; pp. 21–49. [Google Scholar] [CrossRef]
- Barlow, H.B. Unsupervised Learning. Neural Comput. 1989, 1, 295–311. [Google Scholar] [CrossRef]
- Karthika, S.; Durgadevi, M. Generative Adversarial Network (GAN): A general review on different variants of GAN and applications. In Proceedings of the 2021 6th International Conference on Communication and Electronics Systems (ICCES), Coimbatre, India, 8–10 July 2021; pp. 1–8. [Google Scholar] [CrossRef]
- Jakhar, D.; Kaur, I. Artificial intelligence, machine learning and deep learning: Definitions and differences. Clin. Exp. Dermatol. 2019, 45, 131–132. [Google Scholar] [CrossRef]
- Namatēvs, I. Deep Convolutional Neural Networks: Structure, Feature Extraction and Training. Inf. Technol. Manag. Sci. 2017, 20, 40–47. [Google Scholar] [CrossRef]
- Gu, J.; Wang, Z.; Kuen, J.; Ma, L.; Shahroudy, A.; Shuai, B.; Liu, T.; Wang, X.; Wang, G.; Cai, J.; et al. Recent advances in convolutional neural networks. Pattern Recognit. 2018, 77, 354–377. [Google Scholar] [CrossRef]
- O’Shea, K.; Nash, R. An Introduction to Convolutional Neural Networks. arXiv 2015, arXiv:1511.08458. [Google Scholar] [CrossRef]
- Albawi, S.; Mohammed, T.A.; Al-Zawi, S. Understanding of a convolutional neural network. In Proceedings of the 2017 International Conference on Engineering and Technology (ICET), Antalya, Turkey, 21–23 August 2017; pp. 1–6. [Google Scholar] [CrossRef]
- Oliveira, A.; Pereira, S.; Silva, C.A. Retinal vessel segmentation based on Fully Convolutional Neural Networks. Expert Syst. Appl. 2018, 112, 229–242. [Google Scholar] [CrossRef]
- Chen, X.; Wang, X.; Zhang, K.; Fung, K.-M.; Thai, T.C.; Moore, K.; Mannel, R.S.; Liu, H.; Zheng, B.; Qiu, Y. Recent advances and clinical applications of deep learning in medical image analysis. Med. Image Anal. 2022, 79, 102444. [Google Scholar] [CrossRef] [PubMed]
- An Overview of Deep Learning in Medical Imaging Focusing on MRI–-ScienceDirect. Available online: https://www.sciencedirect.com/science/article/pii/S0939388918301181 (accessed on 5 May 2023).
- Robertson, S.; Azizpour, H.; Smith, K.; Hartman, J. Digital image analysis in breast pathology—From image processing techniques to artificial intelligence. Transl. Res. 2017, 194, 19–35. [Google Scholar] [CrossRef] [PubMed]
- Noort, F.v.D.; Manzini, C.; Hofsteenge, M.; Sirmacek, B.; van der Vaart, C.H.; Slump, C.H. Unsupervised convolutional autoencoders for 4D transperineal ultrasound classification. J. Med. Imaging 2023, 10, 014004. [Google Scholar] [CrossRef]
- Huang, P.; Yan, H.; Song, Z.; Xu, Y.; Hu, Z.; Dai, J. Combining autoencoder with clustering analysis for anomaly detection in radiotherapy plans. Quant. Imaging Med. Surg. 2023, 13, 2328–2338. [Google Scholar] [CrossRef]
- Kareem, O.S.; Al-Sulaifanie, A.K.; Hasan, D.A.; Ahmed, D.M. Segmenting and Classifiying the Brain Tumor from MRI Medical Images Based on Machine Learning Algorithms: A Review. Asian J. Res. Comput. Sci. 2021, 10, 50–61. [Google Scholar] [CrossRef]
- Libbrecht, M.W.; Noble, W.S. Machine learning applications in genetics and genomics. Nat. Rev. Genet. 2015, 16, 321–332. [Google Scholar] [CrossRef]
- Ngiam, K.Y.; Khor, I.W. Big data and machine learning algorithms for health-care delivery. Lancet Oncol. 2019, 20, e262–e273. [Google Scholar] [CrossRef]
- Yu, Y.; Zuo, S.; Jiang, H.; Ren, W.; Zhao, T.; Zhang, C. Fine-Tuning Pre-trained Language Model with Weak Supervision: A Contrastive-Regularized Self-Training Ap-proach. arXiv 2021, arXiv:2010.07835. [Google Scholar] [CrossRef]
- Zhou, L.; Pan, S.; Wang, J.; Vasilakos, A.V. Machine learning on big data: Opportunities and challenges. Neurocomputing 2017, 237, 350–361. [Google Scholar] [CrossRef]
- Amini, Z.; Miri, M.; Rabbani, H.; Kafieh, R. A Comprehensive Study of Retinal Vessel Classification Methods in Fundus Images. J. Med. Signals Sens. 2017, 7, 59–70. [Google Scholar] [CrossRef]
- Gegundez-Arias, M.E.; Marin-Santos, D.; Perez-Borrero, I.; Vasallo-Vazquez, M.J. A new deep learning method for blood vessel segmentation in retinal images based on convolutional kernels and modified U-Net model. Comput. Methods Programs Biomed. 2021, 205, 106081. [Google Scholar] [CrossRef] [PubMed]
- Boudegga, H.; Elloumi, Y.; Akil, M.; Bedoui, M.H.; Kachouri, R.; Ben Abdallah, A. Fast and efficient retinal blood vessel segmentation method based on deep learning network. Comput. Med. Imaging Graph. 2021, 90, 101902. [Google Scholar] [CrossRef] [PubMed]
- Tan, T.; Wang, Z.; Du, H.; Xu, J.; Qiu, B. Lightweight pyramid network with spatial attention mechanism for accurate retinal vessel segmentation. Int. J. Comput. Assist. Radiol. Surg. 2021, 16, 673–682. [Google Scholar] [CrossRef] [PubMed]
- Escalante-B, A.N.; Wiskott, L. How to Solve Classification and Regression Problems on High-Dimensional Data with a Su-pervised Extension of Slow Feature Analysis. J. Mach. Learn. Res. 2013, 14, 3683–3719. [Google Scholar]
- Kollem, S.; Reddy, K.R.L.; Rao, D.S. A Review of Image Denoising and Segmentation Methods Based on Medical Images. Int. J. Mach. Learn. Comput. 2019, 9, 288–295. [Google Scholar] [CrossRef]
- Abbas, Q.; Fondon, I.; Sarmiento, A.; Jiménez, S.; Alemany, P. Automatic recognition of severity level for diagnosis of diabetic retinopathy using deep visual features. Med. Biol. Eng. Comput. 2017, 55, 1959–1974. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Zhao, D.; Gao, W. Learning-based image restoration for compressed images. Signal Process. Image Commun. 2012, 27, 54–65. [Google Scholar] [CrossRef]
- Jeong, J.J.; Tariq, A.; Adejumo, T.; Trivedi, H.; Gichoya, J.W.; Banerjee, I. Systematic Review of Generative Adversarial Networks (GANs) for Medical Image Classification and Seg-mentation. J. Digit Imaging 2022, 35, 137–152. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.; DiPaola, D.; Breazeal, C. What are GANs?: Introducing Generative Adversarial Networks to Middle School Students. In Proceedings of the AAAI Conference on Artificial Intelligence, virtually, 2–9 February 2021; Volume 35, pp. 15472–15479. [Google Scholar] [CrossRef]
- Wen, Q.; Sun, L.; Yang, F.; Song, X.; Gao, J.; Wang, X.; Xu, H. Time Series Data Augmentation for Deep Learning: A Survey. In Proceedings of the Thirtieth International Joint Conference on Artificial Intelligence, Montreal, Canada, 19–27 August 2021; pp. 4653–4660. [Google Scholar] [CrossRef]
- Rombach, R.; Blattmann, A.; Lorenz, D.; Esser, P.; Ommer, B. High-Resolution Image Synthesis with Latent Diffusion Models. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, New Orleans, LA, USA, 18–24 June 2022; pp. 10674–10685. [Google Scholar] [CrossRef]
- Wang, T.-C.; Liu, M.-Y.; Zhu, J.-Y.; Tao, A.; Kautz, J.; Catanzaro, B. High-Resolution Image Synthesis and Semantic Manipulation with Conditional GANs. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 8798–8807. [Google Scholar]
- Gu, J.; Shen, Y.; Zhou, B. Image Processing Using Multi-Code GAN Prior. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Seattle, WA, USA, 14–19 June 2020; pp. 3009–3018. [Google Scholar] [CrossRef]
- Huang, Y.; Zheng, F.; Wang, D.; Jiang, J.; Wang, X.; Shao, L. Super-resolution and inpainting with degraded and upgraded generative adversarial networks. In Proceedings of the Twenty-Ninth International Joint Conference on Artificial Intelligence, Yokohama, Japan, 7–15 January 2021; pp. 645–651. [Google Scholar]
- Gatys, L.A.; Ecker, A.S.; Bethge, M. Image Style Transfer Using Convolutional Neural Networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2414–2423. [Google Scholar]
- Mahapatra, D.; Bozorgtabar, B.; Garnavi, R. Image super-resolution using progressive generative adversarial networks for medical image analysis. Comput. Med. Imaging Graph. 2018, 71, 30–39. [Google Scholar] [CrossRef]
- Andreini, P.; Ciano, G.; Bonechi, S.; Graziani, C.; Lachi, V.; Mecocci, A.; Sodi, A.; Scarselli, F.; Bianchini, M. A Two-Stage GAN for High-Resolution Retinal Image Generation and Segmentation. Electronics 2021, 11, 60. [Google Scholar] [CrossRef]
- Zhao, H.; Li, H.; Maurer-Stroh, S.; Cheng, L. Synthesizing retinal and neuronal images with generative adversarial nets. Med. Image Anal. 2018, 49, 14–26. [Google Scholar] [CrossRef]
- Xu, F.; Liu, S.; Xiang, Y.; Hong, J.; Wang, J.; Shao, Z.; Zhang, R.; Zhao, W.; Yu, X.; Li, Z.; et al. Prediction of the Short-Term Therapeutic Effect of Anti-VEGF Therapy for Diabetic Macular Edema Using a Gen-erative Adversarial Network with OCT Images. J. Clin. Med. 2022, 11, 2878. [Google Scholar] [CrossRef]
- Ong, J.; Waisberg, E.; Kamran, S.A.; Paladugu, P.; Zaman, N.; Sarker, P.; Tavakkoli, A.; Lee, A.G. Deep learning synthetic angiograms for individuals unable to undergo contrast-guided laser treatment in aggressive retinopathy of prematurity. Eye 2023, 1–2. [Google Scholar] [CrossRef]
- Kamran, S.A.; Hossain, K.F.; Tavakkoli, A.; Ong, J.; Zuckerbrod, S.L. Contributed Session I: A generative adversarial deep neural network to translate between ocular imaging modalities while maintaining anatomical fidelity. J. Vis. 2022, 22, 3. [Google Scholar] [CrossRef]
- E de Carlo, T.; Romano, A.; Waheed, N.K.; Duker, J.S. A review of optical coherence tomography angiography (OCTA). Int. J. Retin. Vitr. 2015, 1, 5. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, F.; Qi, Z.; Duan, K.; Xi, D.; Zhu, Y.; Zhu, H.; Xiong, H.; He, Q. A Comprehensive Survey on Transfer Learning. Proc. IEEE 2021, 109, 43–76. [Google Scholar] [CrossRef]
- Hussain, M.; Bird, J.J.; Faria, D.R. A Study on CNN Transfer Learning for Image Classification. In Advances in Computational Intelligence Systems, Proceedings of the UK Workshop on Computational Intelligence, Nottingham, UK, 5–7 September 2018; Springer: Berlin/Heidelberg, Germany, 2018; Volume 840, pp. 191–202. [Google Scholar] [CrossRef]
- Akhand, M.A.H.; Roy, S.; Siddique, N.; Kamal, A.S.; Shimamura, T. Facial Emotion Recognition Using Transfer Learning in the Deep CNN. Electronics 2021, 10, 1036. [Google Scholar] [CrossRef]
- Zabalza, J.; Ren, J.; Zheng, J.; Zhao, H.; Qing, C.; Yang, Z.; Du, P.; Marshall, S. Novel segmented stacked autoencoder for effective dimensionality reduction and feature extraction in hy-perspectral imaging. Neurocomputing 2016, 185, 1–10. [Google Scholar] [CrossRef]
- Shin, H.-C.; Roth, H.R.; Gao, M.; Lu, L.; Xu, Z.; Nogues, I.; Yao, J.; Mollura, D.; Summers, R.M. Deep Convolutional Neural Networks for Computer-Aided Detection: CNN Architectures, Dataset Characteristics and Transfer Learning. IEEE Trans. Med. Imaging 2016, 35, 1285–1298. [Google Scholar] [CrossRef] [PubMed]
- Waisberg, E.; Ong, J.; Paladugu, P.; Kamran, S.A.; Zaman, N.; Lee, A.G.; Tavakkoli, A. Dynamic visual acuity as a biometric for astronaut performance and safety. Life Sci. Space Res. 2023, 37, 3–6. [Google Scholar] [CrossRef]
- Waisberg, E.; Ong, J.; Paladugu, P.; Zaman, N.; Kamran, S.A.; Lee, A.G.; Tavakkoli, A. Optimizing Screening for Preventable Blindness with Head-Mounted Visual Assessment Technology. J. Vis. Impair. Blind. 2022, 116, 579–581. [Google Scholar] [CrossRef]
- Ong, J.; Zaman, N.; Kamran, S.A.; Waisberg, E.; Tavakkoli, A.; Lee, A.G.; Webster, M. Contributed Session I: A Multi-Modal Visual Assessment System For Monitoring Spaceflight Associated Neuro-Ocular Syndrome (SANS) during Long Duration Spaceflight. J. Vis. 2022, 22, 6. [Google Scholar] [CrossRef]
- Sarker, P.; Ong, J.; Zaman, N.; Kamran, S.A.; Waisberg, E.; Paladugu, P.; Lee, A.G.; Tavakkoli, A. Extended reality quantification of pupil reactivity as a non-invasive assessment for the pathogenesis of spaceflight associated neuro-ocular syndrome: A technology validation study for astronaut health. Life Sci. Space Res. 2023, 38, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Sarker, P.; Zaman, N.; Ong, J.; Paladugu, P.; Aldred, M.; Waisberg, E.; Lee, A.G.; Tavakkoli, A. Test—Retest Reliability of Virtual Reality Devices in Quantifying for Relative Afferent Pupillary Defect. Transl. Vis. Sci. Technol. 2023, 12, 2. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Hypothesis | Summary | Reference |
|---|---|---|
| Cephalad fluid shift and elevated intracranial pressure | Drops in hydrostatic pressure cause widespread disruption of cranial fluids. These shifts can cause venous congestion and block cerebrospinal outflow, resulting in excess pressure on the optic nerve sheath (ONS). Congestion in the cranial vascular system and CSF spaces causes ICP to increase. The elevation in overall pressure is transferred to the ocular system via the ONS, which may cause SANS findings. | Mader et al., 2011 [5] Marshall-Goebel et al., 2019 [12] Orešcović & Bulat, 1993 [13] Martin Paez et al., 2020 [33] Zhang et al., 2018 [9] Zhang et al., 2014 [34] Lee et al., 2020 [1] |
| Brain upward shift | Microgravity can cause the brain to shift upwards, retracting the optic nerve and compressing CSF spaces. Reduced CSF space volume results in congestion and a subsequent increase in CSF pressure. | Roberts et al., 2017 [22] Shinojima et al., 2018 [23] |
| Ocular glymphatic dysfunction | The ocular glymphatic system is an offshoot of the general glymphatic system, a series of perivascular spaces (PVS) that transport CSF. Altered venous and arterial flows modify these PVS; such changes both increase CSF inflow and impair its outflow and drainage, causing CSF buildup near and along the ONS. | Jessen et al., 2015 [24] Mathieu et al., 2017 [26] Wang et al., 2020 [27] Wostyn et al., 2018 [28] Wostyn et al., 2022 [25] |
| Genetics | Several polymorphisms within 1-carbon metabolites have been correlated with increased presentation of SANS symptoms, suggesting that genetic mechanisms could predispose astronauts to developing the syndrome. | Zwart et al., 2012 [31] Zwart et al., 2016 [29] Zwart et al., 2019 [30] |
| Vitamin B levels | Higher levels of vitamin B have been correlated with lower incidence and magnitude of SANS symptom development. | Zwart et al., 2016 [29] Zwart et al., 2019 [30] |
| Reduction of tissue compressive forces | Reduction of tissue compressive forces in microgravity may lead to a reduction in transmural pressure at the posterior aspect of the eye. Persistent transmural reduction may lead to ocular remodeling and SANS. | Buckey et al., 2022 [16] Buckey et al., 2018 [19] Norsk et al., 2020 [18] |
| Cerebral blood volume pulsatility | Cerebral blood volume pulsatility may be increased during spaceflight. This persistent increase in pulsatility during long-duration spaceflight may affect nearby ocular structures to cause remodeling. | Strangman et al., 2017 [21] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ong, J.; Waisberg, E.; Masalkhi, M.; Kamran, S.A.; Lowry, K.; Sarker, P.; Zaman, N.; Paladugu, P.; Tavakkoli, A.; Lee, A.G. Artificial Intelligence Frameworks to Detect and Investigate the Pathophysiology of Spaceflight Associated Neuro-Ocular Syndrome (SANS). Brain Sci. 2023, 13, 1148. https://doi.org/10.3390/brainsci13081148
Ong J, Waisberg E, Masalkhi M, Kamran SA, Lowry K, Sarker P, Zaman N, Paladugu P, Tavakkoli A, Lee AG. Artificial Intelligence Frameworks to Detect and Investigate the Pathophysiology of Spaceflight Associated Neuro-Ocular Syndrome (SANS). Brain Sciences. 2023; 13(8):1148. https://doi.org/10.3390/brainsci13081148
Chicago/Turabian StyleOng, Joshua, Ethan Waisberg, Mouayad Masalkhi, Sharif Amit Kamran, Kemper Lowry, Prithul Sarker, Nasif Zaman, Phani Paladugu, Alireza Tavakkoli, and Andrew G. Lee. 2023. "Artificial Intelligence Frameworks to Detect and Investigate the Pathophysiology of Spaceflight Associated Neuro-Ocular Syndrome (SANS)" Brain Sciences 13, no. 8: 1148. https://doi.org/10.3390/brainsci13081148
APA StyleOng, J., Waisberg, E., Masalkhi, M., Kamran, S. A., Lowry, K., Sarker, P., Zaman, N., Paladugu, P., Tavakkoli, A., & Lee, A. G. (2023). Artificial Intelligence Frameworks to Detect and Investigate the Pathophysiology of Spaceflight Associated Neuro-Ocular Syndrome (SANS). Brain Sciences, 13(8), 1148. https://doi.org/10.3390/brainsci13081148