
Acute Effect of Single-Session Cerebellar Anodal Transcranial Direct Current Stimulation on Static and Dynamic Balance in Healthy Volunteers
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
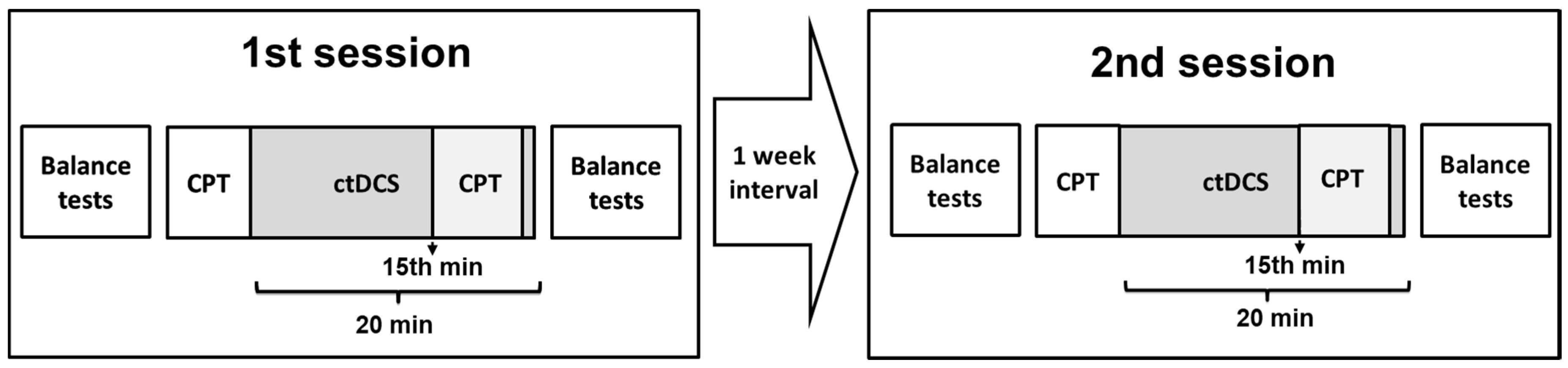
2.2. Experimental Design
2.3. Cerebellar tDCS
2.4. Continuous Performance Test (CPT)
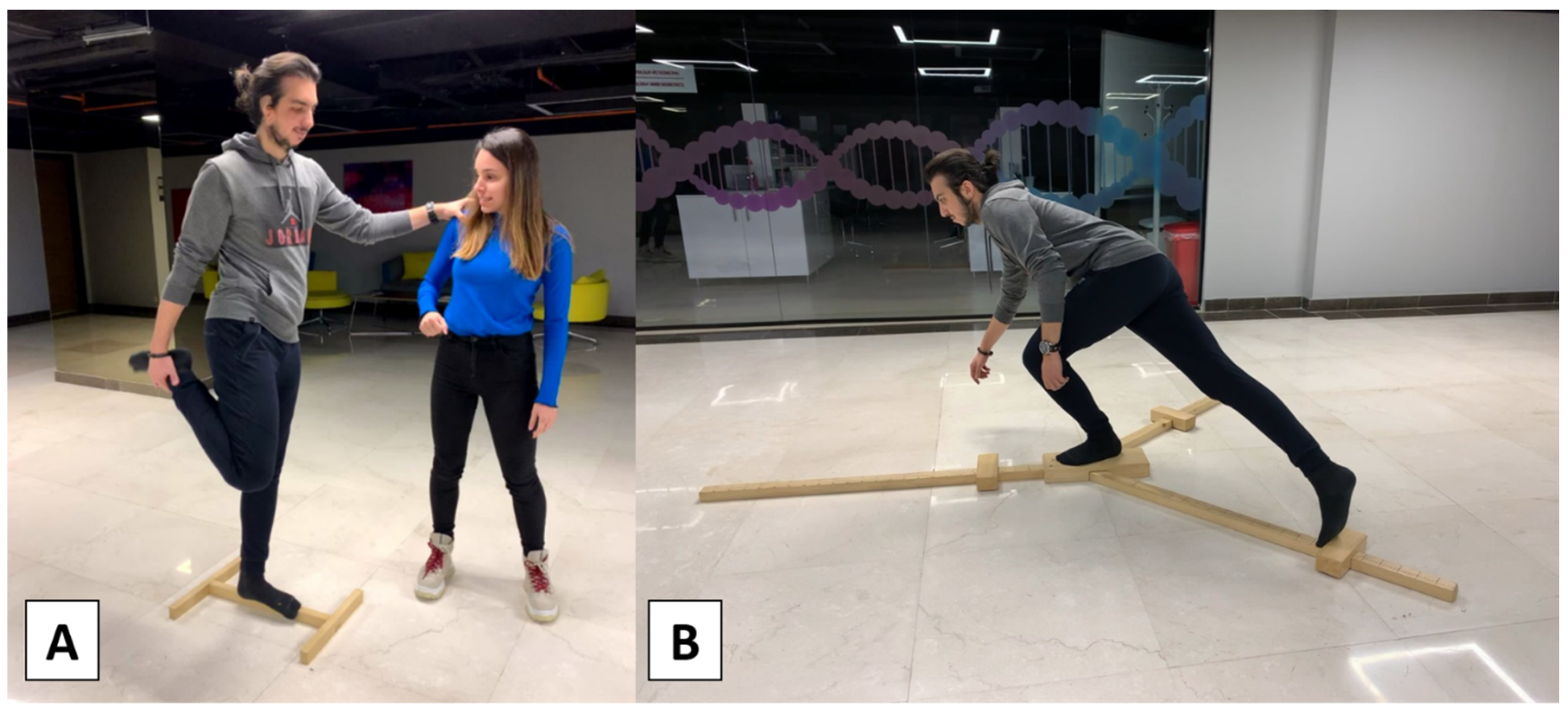
2.5. Balance Tests
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Conradsson, D.; Löfgren, N.; Nero, H.; Hagströmer, M.; Ståhle, A.; Lökk, J.; Franzén, E. The effects of highly challenging balance training in elderly with Parkinson’s disease: A randomized controlled trial. Neurorehabilit. Neural Repair 2015, 29, 827–836. [Google Scholar] [CrossRef] [PubMed]
- Lesinski, M.; Hortobágyi, T.; Muehlbauer, T.; Gollhofer, A.; Granacher, U. Effects of balance training on balance performance in healthy older adults: A systematic review and meta-analysis. Sports Med. 2015, 45, 1721–1738. [Google Scholar] [CrossRef] [PubMed]
- Alizadehsaravi, L.; Bruijn, S.M.; Muijres, W.; Koster, R.; van Dieën, J.H. Improvement in gait stability in older adults after ten sessions of standing balance training. PLoS ONE 2022, 17, e0242115. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.; Huang, D.B.; Li, X.M.; Guo, J.H.; Guo, M.M.; Yu, S.; Huang, S.; Lin, Z.H. Effects of balance training on dynamic postural stability in patients with chronic ankle instability: Systematic review and meta-analysis of randomized controlled trials. J. Sports Med. Phys. 2022, 62, 1707–1715. [Google Scholar] [CrossRef] [PubMed]
- Yosephi, M.H.; Ehsani, F.; Zoghi, M.; Jaberzadeh, S. Multi-session anodal tDCS enhances the effects of postural training on balance and postural stability in older adults with high fall risk: Primary motor cortex versus cerebellar stimulation. Brain Stimul. 2018, 11, 1239–1250. [Google Scholar] [CrossRef]
- Ahn, J.H.; Lee, D.; Kim, M.; Cho, J.W.; Chang, W.H.; Youn, J. M1 and cerebellar tDCS for MSA-C: A double-Blind, randomized, sham-controlled, crossover study. Cerebellum 2023, 22, 386–393. [Google Scholar] [CrossRef]
- Guo, Z.; Bao, D.; Manor, B.; Zhou, J. The effects of transcranial direct current stimulation (TDCS) on balance control in older adults: A systematic review and meta-analysis. Front. Aging Neurosci. 2020, 12, 275. [Google Scholar] [CrossRef]
- Wang, S.M.; Chan, Y.W.; Tsui, Y.O.; Chu, F.Y. Effects of anodal cerebellar transcranial direct current stimulation on movements in patients with cerebellar ataxias: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 10690. [Google Scholar] [CrossRef]
- Pohjola, H.; Tolmunen, T.; Kotilainen, T.; Lehto, S.M. Using transcranial direct current stimulation to enhance performance in balance tasks. Clin. Neurophysiol. 2017, 128, 501–502. [Google Scholar] [CrossRef]
- Zandvliet, S.B.; Meskers, C.; Kwakkel, G.; van Wegen, E. Short-term effects of cerebellar TDCS on standing balance performance in patients with chronic stroke and healthy age-matched elderly. Cerebellum 2018, 17, 575–589. [Google Scholar] [CrossRef]
- Barretto, T.L.; Bandeira, I.D.; Jagersbacher, J.G.; Barretto, B.L.; de Oliveira E Torres, Â.; Peña, N.; Miranda, J.; Lucena, R. Transcranial direct current stimulation in the treatment of cerebellar ataxia: A two-phase, double-blind, auto-matched, pilot study. Clin. Neurol. Neurosurg. 2019, 182, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Jafarzadeh, A.; Ehsani, F.; Yosephi, M.H.; Zoghi, M.; Jaberzadeh, S. Concurrent postural training and M1 anodal transcranial direct current stimulation improve postural impairment in patients with chronic low back pain. J. Clin. Neurosci. 2019, 68, 224–234. [Google Scholar] [CrossRef]
- Dong, K.; Meng, S.; Guo, Z.; Zhang, R.; Xu, P.; Yuan, E.; Lian, T. The effects of transcranial direct current stimulation on balance and gait in stroke patients: A systematic review and meta-analysis. Front. Neurol. 2021, 12, 650925. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.A.; Kim, M.K. The effect of transcranial direct current stimulation combined with visual cueing training on motor function, balance, and gait ability of patients with Parkinson’s disease. Medicina 2021, 57, 1146. [Google Scholar] [CrossRef] [PubMed]
- Beretta, V.S.; Santos, P.; Orcioli-Silva, D.; Zampier, V.C.; Vitório, R.; Gobbi, L. Transcranial direct current stimulation for balance rehabilitation in neurological disorders: A systematic review and meta-analysis. Ageing Res. Rev. 2022, 81, 101736. [Google Scholar] [CrossRef]
- Marotta, N.; de Sire, A.; Marinaro, C.; Moggio, L.; Inzitari, M.T.; Russo, I.; Tasselli, A.; Paolucci, T.; Valentino, P.; Ammendolia, A. Efficacy of transcranial direct current stimulation (TDCS) on balance and gait in multiple sclerosis patients: A machine learning approach. J. Clin. Med. 2022, 11, 3505. [Google Scholar] [CrossRef]
- Morya, E.; Monte-Silva, K.; Bikson, M.; Esmaeilpour, Z.; Biazoli, C.E., Jr.; Fonseca, A.; Bocci, T.; Farzan, F.; Chatterjee, R.; Hausdorff, J.M.; et al. Beyond the target area: An integrative view of tDCS-induced motor cortex modulation in patients and athletes. J. Neuroeng. Rehabil. 2019, 16, 141. [Google Scholar] [CrossRef]
- Ehsani, F.; Bakhtiary, A.H.; Jaberzadeh, S.; Talimkhani, A.; Hajihasani, A. Differential effects of primary motor cortex and cerebellar transcranial direct current stimulation on motor learning in healthy individuals: A randomized double-blind sham-controlled study. Neurosci. Res. 2016, 112, 10–19. [Google Scholar] [CrossRef]
- Foerster, Á.; Melo, L.; Mello, M.; Castro, R.; Shirahige, L.; Rocha, S.; Monte-Silva, K. Cerebellar transcranial direct current stimulation (ctDCS) impairs balance control in healthy individuals. Cerebellum 2017, 16, 872–875. [Google Scholar] [CrossRef]
- Steiner, K.M.; Enders, A.; Thier, W.; Batsikadze, G.; Ludolph, N.; Ilg, W.; Timmann, D. Cerebellar tDCS does not improve learning in a complex whole body dynamic balance task in young healthy subjects. PLoS ONE 2016, 11, e0163598. [Google Scholar] [CrossRef]
- Emadi Andani, M.; Villa-Sánchez, B.; Raneri, F.; Dametto, S.; Tinazzi, M.; Fiorio, M. Cathodal cerebellar TDCS combined with visual feedback improves balance control. Cerebellum 2020, 19, 812–823. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Xiao, S.; Yu, C.; Zhou, J.; Fu, W. Effects of transcranial direct current stimulation combined with physical training on the excitability of the motor cortex, physical performance, and motor learning: A systematic review. Front. Neurosci. 2021, 15, 648354. [Google Scholar] [CrossRef] [PubMed]
- Inukai, Y.; Saito, K.; Sasaki, R.; Kotan, S.; Nakagawa, M.; Onishi, H. Influence of transcranial direct current stimulation to the cerebellum on standing posture control. Front. Hum. Neurosci. 2016, 10, 325. [Google Scholar] [CrossRef]
- Poortvliet, P.; Hsieh, B.; Cresswell, A.; Au, J.; Meinzer, M. Cerebellar transcranial direct current stimulation improves adaptive postural control. Clin. Neurophysiol. 2018, 129, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Rauscher, M.; Yavari, F.; Batsikadze, G.; Ludolph, N.; Ilg, W.; Nitsche, M.A.; Timmann, D.; Steiner, K.M. Lack of cerebellar tDCS effects on learning of a complex whole body dynamic balance task in middle-aged (50–65 years) adults. Neurol. Res. Pract. 2020, 2, 38. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.E.; Doumas, M. Anodal transcranial direct current stimulation shows minimal, measure-specific effects on dynamic postural control in young and older adults: A double blind, sham-controlled study. PLoS ONE 2017, 12, e0170331. [Google Scholar] [CrossRef]
- Brachman, A.; Kamieniarz, A.; Michalska, J.; Pawłowski, M.; Słomka, K.J.; Juras, G. Balance training programs in athletes—A systematic review. J. Hum. Kinet. 2017, 58, 45–64. [Google Scholar] [CrossRef]
- Hou, J.; Nitsche, M.A.; Yi, L.; Kong, Z.; Qi, F. Effects of transcranial direct current stimulation over the primary motor cortex in improving postural stability in healthy young adults. Biology 2022, 11, 1370. [Google Scholar] [CrossRef]
- Rosvold, H.E.; Mirsky, A.F.; Sarason, I.; Bransome, E.D., Jr.; Beck, L.H. A continuous performance test of brain damage. J. Consult. Psychol. 1956, 20, 343–350. [Google Scholar] [CrossRef]
- Riccio, C.A.; Reynolds, C.R.; Lowe, P.A. Clinical Applications of Continuous Performance Tests: Measuring Attention and Impulsive Responding in Children and Adults; John Wiley & Sons Inc.: Hoboken, NJ, USA, 2001. [Google Scholar]
- Ulusoy, M.; Sahin, N.H.; Erkmen, H. Turkish version of the Beck Anxiety Inventory: Psychometric properties. J. Cogn. Psychother. 1998, 12, 163–172. [Google Scholar]
- Hisli, N. Beck Depresyon Envanterinin Üniversite Ögrencileri için geçerligi, güvenilirligi. Psikol. Derg. 1989, 7, 3–13. [Google Scholar]
- Ipek, F.; Doğan, M.; Yildiz Kabak, V.; Atasavun Uysal, S.; Düger, T. Cross-cultural adaptation, validity and reliability of Turkish version of the Waterloo Handedness and Footedness Questionnaire-Revised. Laterality 2021, 26, 624–644. [Google Scholar] [CrossRef] [PubMed]
- Parazzini, M.; Rossi, E.; Ferrucci, R.; Liorni, I.; Priori, A.; Ravazzani, P. Modelling the electric field and the current density generated by cerebellar transcranial DC stimulation in humans. Clin. Neurophysiol. 2014, 125, 577–584. [Google Scholar] [CrossRef]
- Tsigilis, N.; Douda, H.; Tokmakidis, S.P. Test–retest reliability of the Eurofit test battery administered to university students. Percept. Mot. Skills 2016, 95, 1295–1300. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, S.W.; Teyhen, D.S.; Lorenson, C.L.; Warren, R.L.; Koreerat, C.M.; Straseske, C.A.; Childs, J.D. Y-balance test: A reliability study involving multiple raters. Mil. Med. 2013, 178, 1264–1270. [Google Scholar] [CrossRef] [PubMed]
- Schwiertz, G.; Beurskens, R.; Muehlbauer, T. Discriminative validity of the lower and upper quarter Y balance test performance: A comparison between healthy trained and untrained youth. BMC Sports Sci. Med. Rehabil. 2020, 12, 73. [Google Scholar] [CrossRef] [PubMed]
- Rosano, C.; Aizenstein, H.J.; Studenski, S.; Newman, A.B. A regions-of-interest volumetric analysis of mobility limitations in community-dwelling older adults. J. Gerontol. A Biol. 2007, 62, 1048–1055. [Google Scholar] [CrossRef]
- Birch, R.C.; Hocking, D.R.; Cornish, K.M.; Menant, J.C.; Georgiou-Karistianis, N.; Godler, D.E.; Wen, W.; Hackett, A.; Rogers, C.; Trollor, J.N. Preliminary evidence of an effect of cerebellar volume on postural sway in FMR1 premutation males. Genes Brain Behav. 2015, 14, 251–259. [Google Scholar] [CrossRef]
- Kannan, L.; Bhatt, T.; Zhang, A.; Ajilore, O. Association of balance control mechanisms with brain structural integrity in older adults with mild cognitive impairment. Neurosci. Lett. 2022, 783, 136699. [Google Scholar] [CrossRef]
- Jalali, R.; Miall, R.C.; Galea, J.M. No consistent effect of cerebellar transcranial direct current stimulation on visuomotor adaptation. J. Neurophysiol. 2017, 118, 655–665. [Google Scholar] [CrossRef]
- de Albuquerque, L.L.; Pantovic, M.; Clingo, M.G.; Fischer, K.M.; Jalene, S.; Landers, M.R.; Mari, Z.; Poston, B. Long-term application of cerebellar transcranial direct current stimulation does not improve motor learning in Parkinson’s disease. Cerebellum 2022, 21, 333–349. [Google Scholar] [CrossRef] [PubMed]
- Lima de Albuquerque, L.; Pantovic, M.; Clingo, M.; Fischer, K.; Jalene, S.; Landers, M.; Mari, Z.; Poston, B. An acute application of cerebellar transcranial direct current stimulation does not improve motor performance in Parkinson’s disease. Brain Sci. 2020, 10, 735. [Google Scholar] [CrossRef] [PubMed]
- Steiner, K.M.; Thier, W.; Batsikadze, G.; Ludolph, N.; Ilg, W.; Timmann, D. Lack of effects of a single session of cerebellar transcranial direct current stimulation (tDCS) in a dynamic balance task. J. Neurol. 2020, 267, 1206–1208. [Google Scholar] [CrossRef] [PubMed]
- Baharlouei, H.; Saba, M.A.; Shaterzadeh Yazdi, M.J.; Jaberzadeh, S. The effect of transcranial direct current stimulation on balance in healthy young and older adults: A systematic review of the literature. Neurophysiol. Clin. 2020, 50, 119–131. [Google Scholar] [CrossRef] [PubMed]
- Parsaee, S.; Shohani, M.; Jalilian, M. The effect of cerebellar TDCS on static and dynamic balance of inactive elderly men. Gerontol. Geriatr. Med. 2023, 9, 23337214231159760. [Google Scholar] [CrossRef]
- Ferrucci, R.; Marceglia, S.; Vergari, M.; Cogiamanian, F.; Mrakic-Sposta, S.; Mameli, F.; Zago, S.; Barbieri, S.; Priori, A. Cerebellar transcranial direct current stimulation impairs the practice-dependent proficiency increase in working memory. J. Cogn. Neurosci. 2008, 20, 1687–1697. [Google Scholar] [CrossRef]
- Jongkees, B.J.; Immink, M.A.; Boer, O.D.; Yavari, F.; Nitsche, M.A.; Colzato, L.S. The effect of cerebellar tDCS on sequential motor response selection. Cerebellum 2019, 18, 738–749. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Anodal tDCS | |||||||
| Tests | Y-Balance scores | Flamingo scores | CPT results | ||||
| Foot | D | ND | D | ND | Omission | Commission | RT (ms) |
| Pre | 81.12 ± 5.33 | 81.35 ± 5.37 | 13.33 ± 3.94 | 14.44 ± 5.83 | 0.61 ± 0.91 | 1.22 ± 1.21 | 317.94 ± 55.76 |
| Post | 82.72 ± 6.35 | 82.37 ± 6.72 | 11.38 ± 4.40 | 12.55 ± 4.28 | 0.27 ± 0.57 | 0.83 ± 0.92 | 332.88 ± 50.40 |
| Sham tDCS | |||||||
| Tests | Y-Balance scores | Flamingo scores | CPT results | ||||
| Foot | D | ND | D | ND | Omission | Commission | RT (ms) |
| Pre | 81.63 ± 5.34 | 82.84 ± 5.17 | 13.33 ± 5.26 | 13.33 ± 5.22 | 0.27 ± 0.46 | 1.16 ± 1.38 | 316.72 ± 48.60 |
| Post | 82.05 ± 5.97 | 83.30 ± 6.32 | 10.88 ± 4.30 | 11.16 ± 5.46 | 0.22 ± 0.42 | 0.88 ± 0.83 | 321.83 ± 50.17 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Erdoğan, E.T.; Kır, C.; Beycan, E.; Karakaya, E.; Altınçınar, S.; Bayramoğlu, T.; Eskikurt, G.; Karamürsel, S. Acute Effect of Single-Session Cerebellar Anodal Transcranial Direct Current Stimulation on Static and Dynamic Balance in Healthy Volunteers. Brain Sci. 2023, 13, 1107. https://doi.org/10.3390/brainsci13071107
Erdoğan ET, Kır C, Beycan E, Karakaya E, Altınçınar S, Bayramoğlu T, Eskikurt G, Karamürsel S. Acute Effect of Single-Session Cerebellar Anodal Transcranial Direct Current Stimulation on Static and Dynamic Balance in Healthy Volunteers. Brain Sciences. 2023; 13(7):1107. https://doi.org/10.3390/brainsci13071107
Chicago/Turabian StyleErdoğan, Ezgi Tuna, Can Kır, Esin Beycan, Esin Karakaya, Sanem Altınçınar, Türkü Bayramoğlu, Gökçer Eskikurt, and Sacit Karamürsel. 2023. "Acute Effect of Single-Session Cerebellar Anodal Transcranial Direct Current Stimulation on Static and Dynamic Balance in Healthy Volunteers" Brain Sciences 13, no. 7: 1107. https://doi.org/10.3390/brainsci13071107
APA StyleErdoğan, E. T., Kır, C., Beycan, E., Karakaya, E., Altınçınar, S., Bayramoğlu, T., Eskikurt, G., & Karamürsel, S. (2023). Acute Effect of Single-Session Cerebellar Anodal Transcranial Direct Current Stimulation on Static and Dynamic Balance in Healthy Volunteers. Brain Sciences, 13(7), 1107. https://doi.org/10.3390/brainsci13071107