

A Pilot Study of Short-Course Oral Vitamin A and Aerosolised Diffuser Olfactory Training for the Treatment of Smell Loss in Long COVID

 , ,
, ,  ,
, 
 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
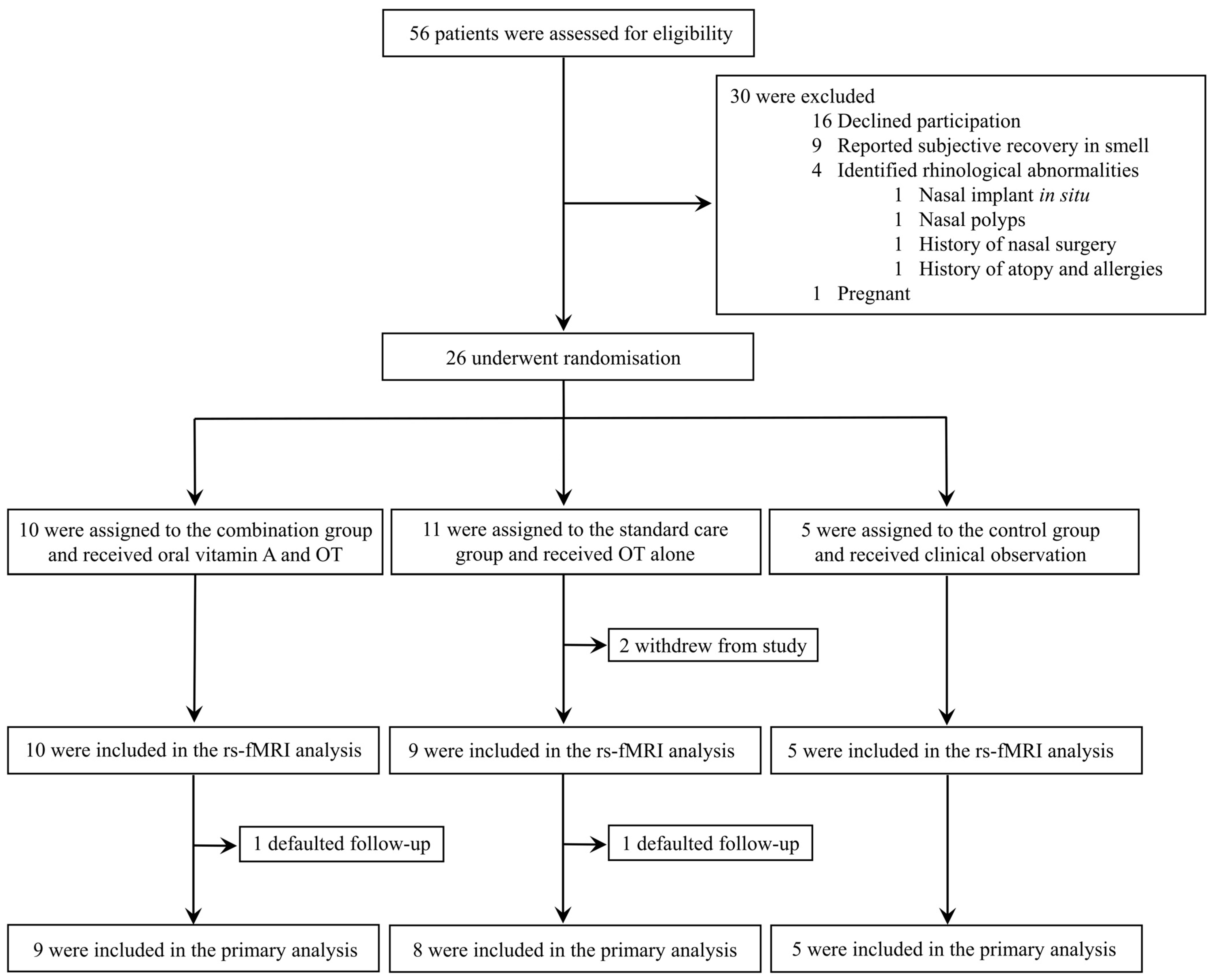
2.1. Study Design
2.2. Participants
2.3. Randomisation and Blinding
3. Procedures
3.1. Therapeutic Interventions
3.2. Baseline Assessments
3.3. Otolaryngological and Functional Olfactory Assessments
3.4. Magnetic Resonance Imaging Assessments
3.4.1. Structural Sequence Acquisition
3.4.2. Volumetric Measurements of the Olfactory Bulbs and Tracts
3.5. Magnetic Resonance Spectroscopy
3.6. Resting-State Functional MRI Data Acquisition and Seed–Based Analyses within the Olfactory Cortical Network
3.7. Interval Assessments and Follow–Up Evaluations
4. Outcomes
5. Statistical Analysis
6. Trial Registration
7. Data Availability
8. Results
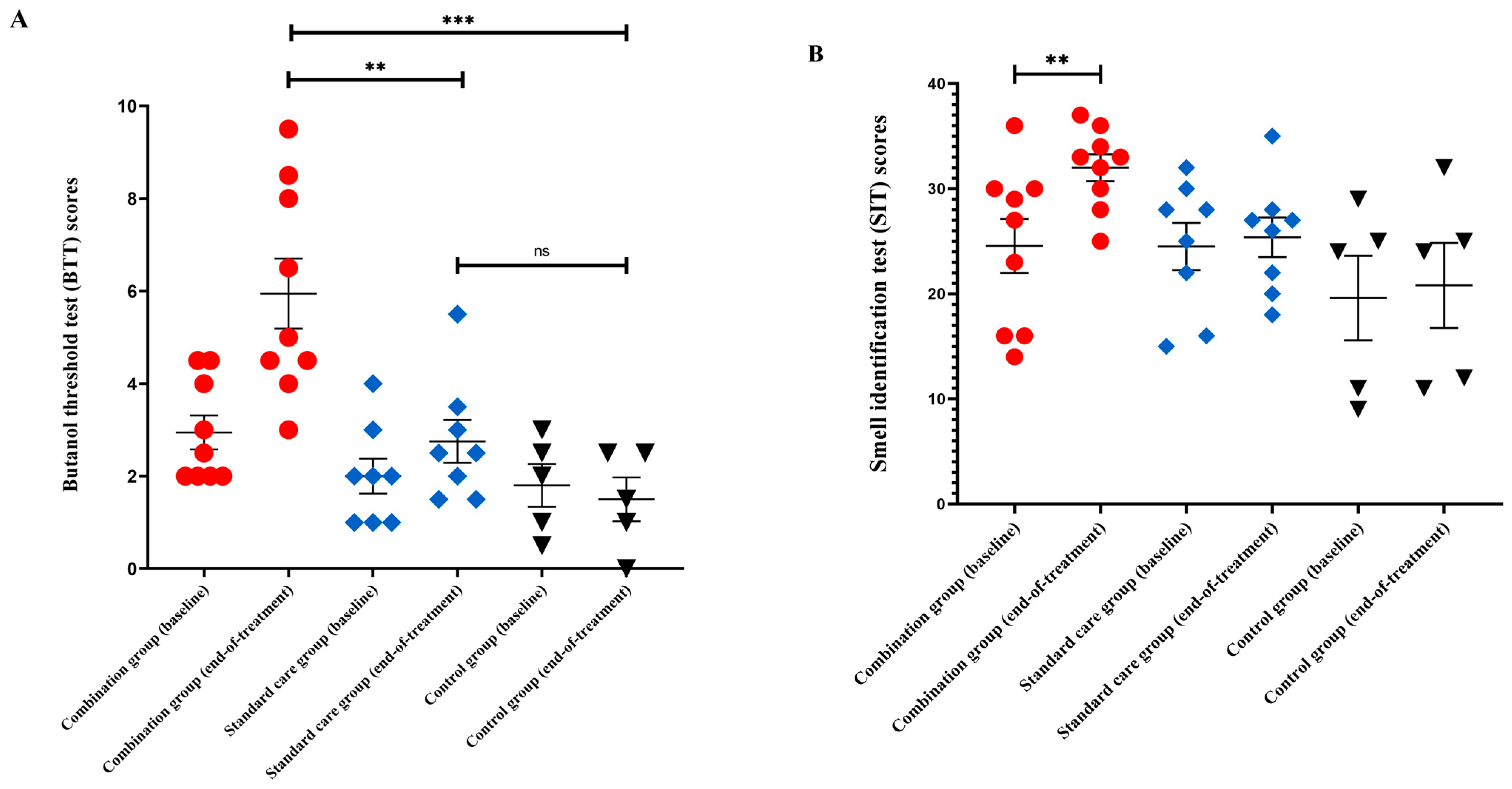
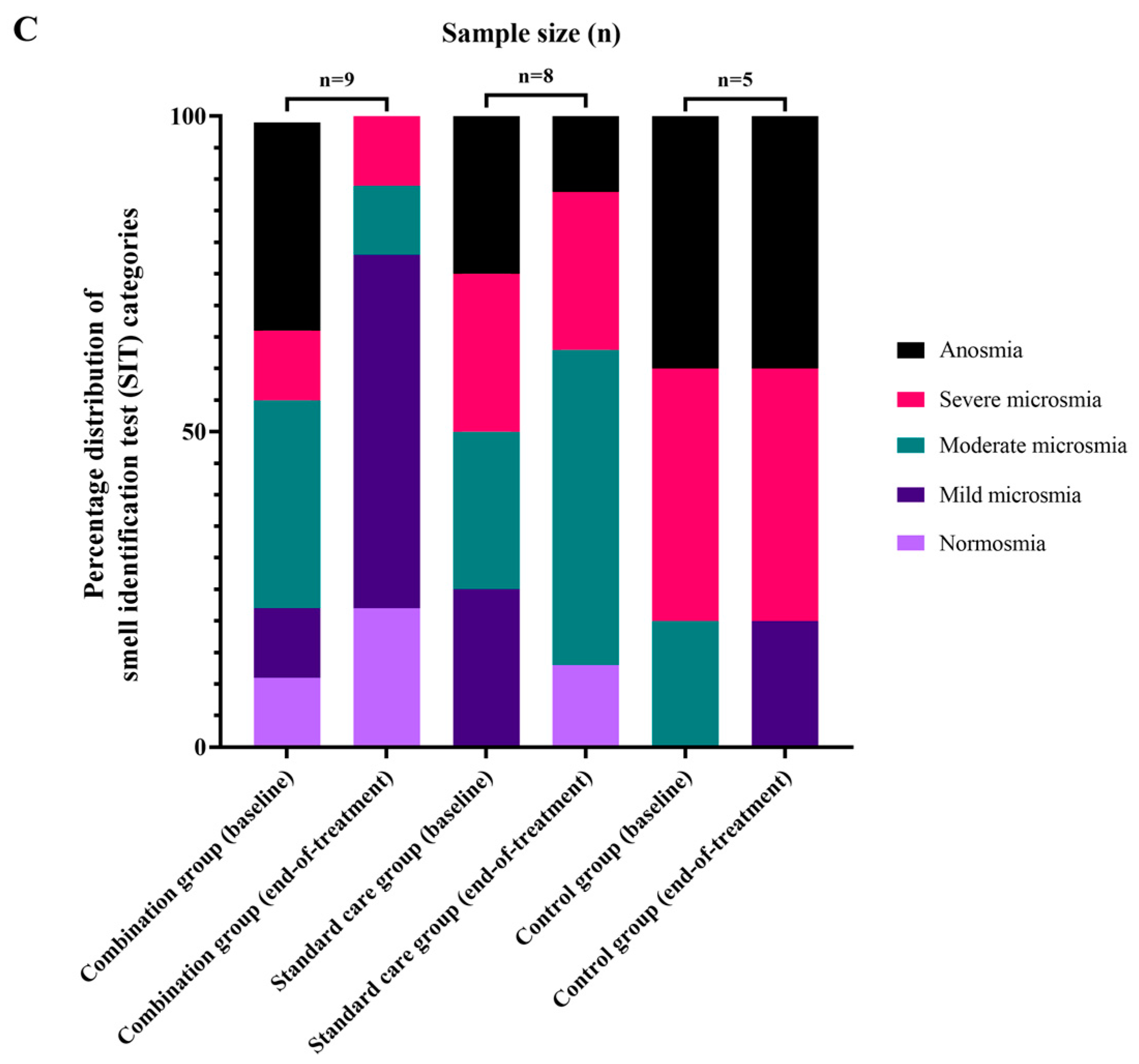
8.1. Clinical and Olfactory Function Status
8.2. Neuroradiological Outcomes
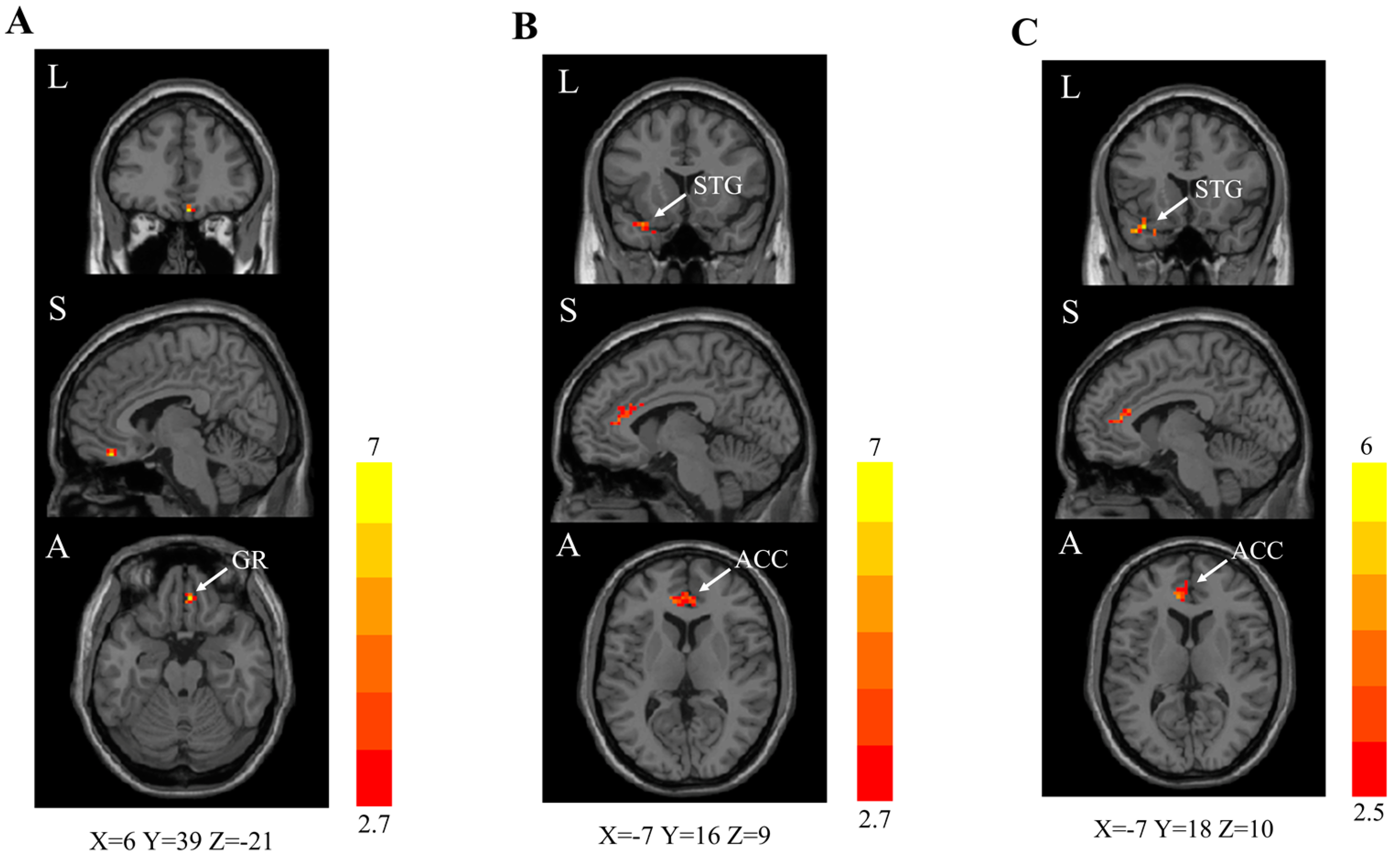
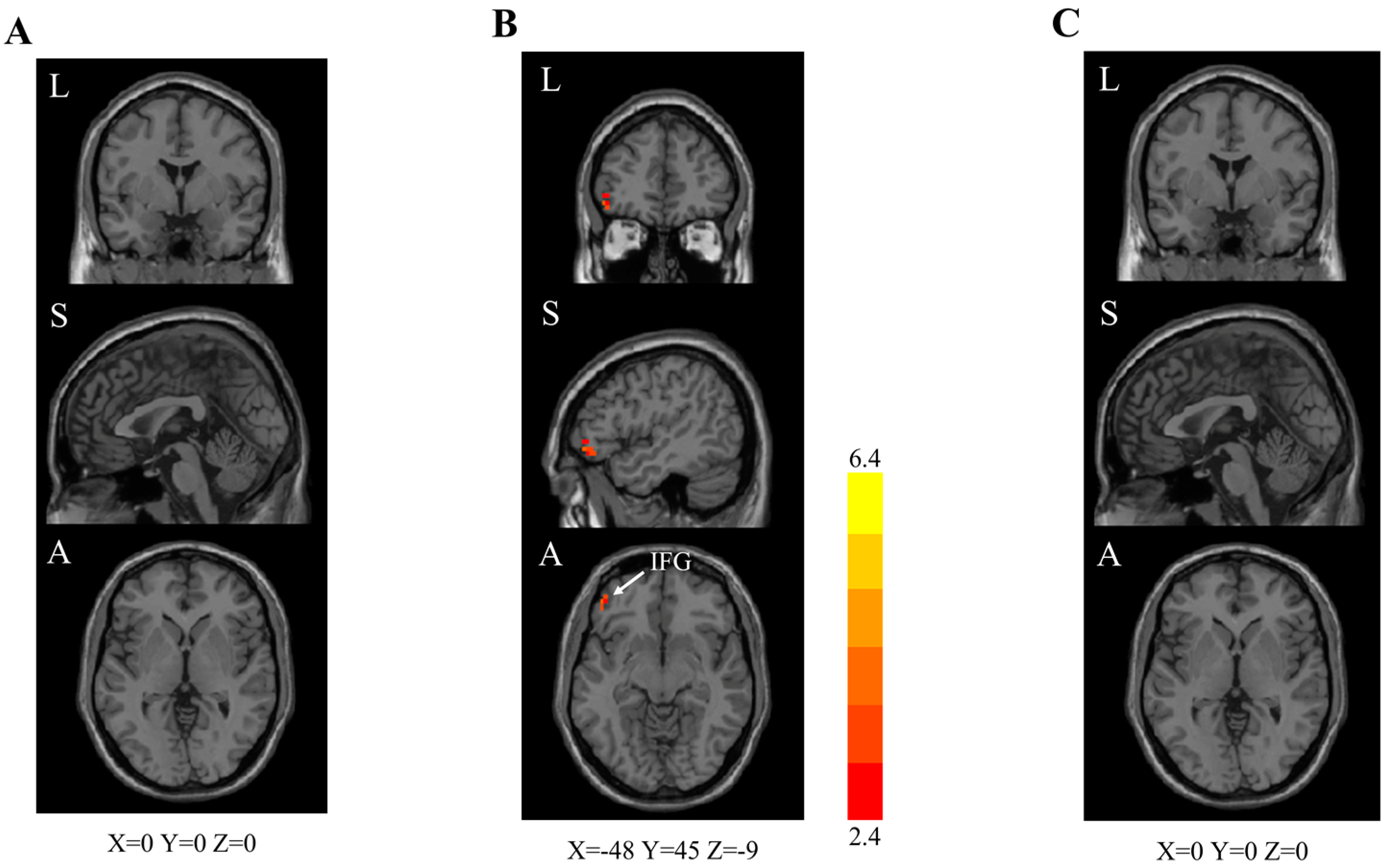
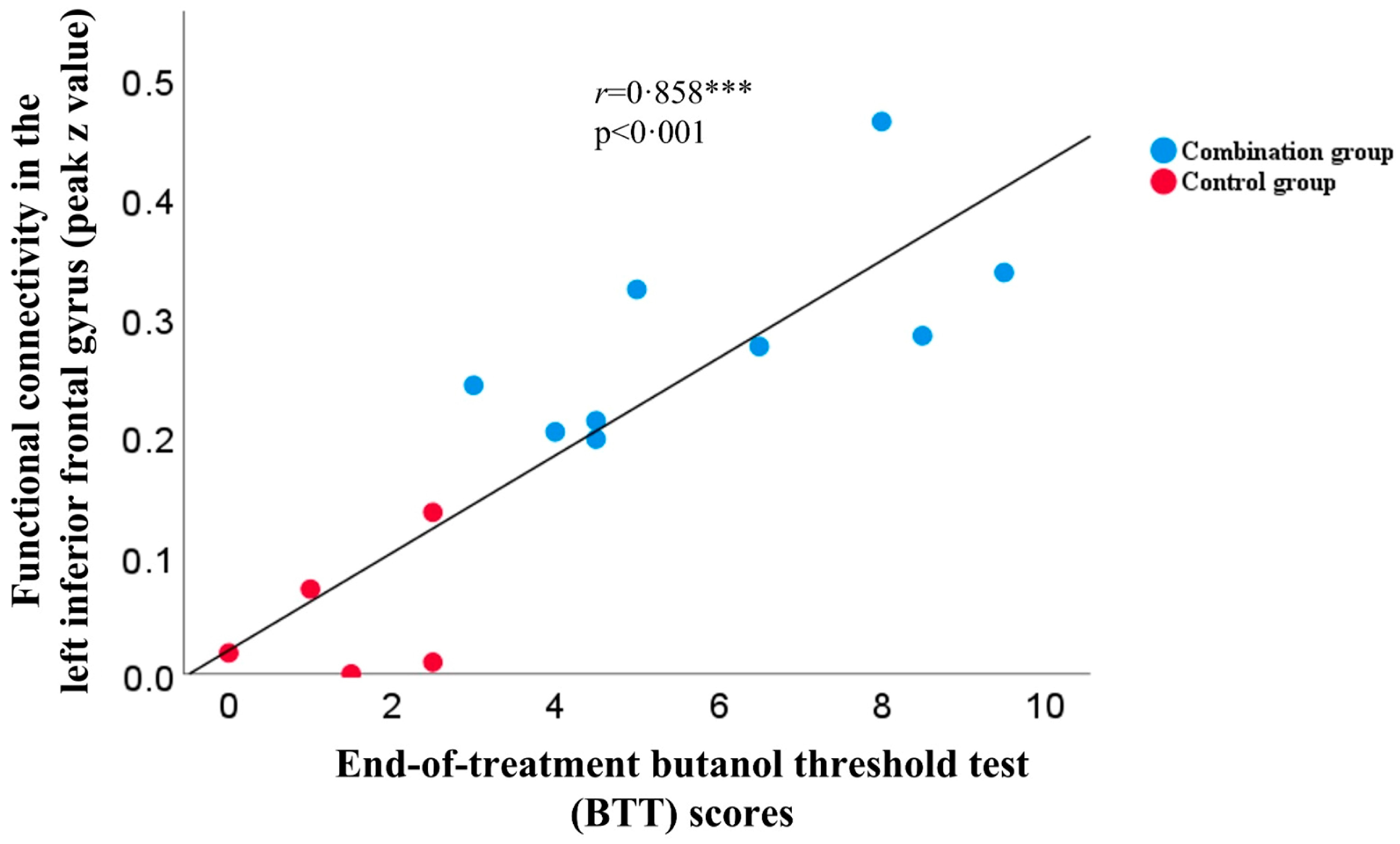
8.2.1. Seed–Based rs–fMRI Analyses in the Olfactory Functional Network
8.2.2. MR Spectroscopy Analyses at the Gyrus Rectus and Superior Frontal Cortex
8.2.3. Volumetric Analysis of the Olfactory Bulbs and Tracts
9. Safety and Tolerability
10. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Chan, J.F.-W.; Yuan, S.; Kok, K.-H.; To, K.K.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.; Poon, R.W.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [PubMed]
- To, K.K.; Sridhar, S.; Chiu, K.H.; Hung, D.L.; Li, X.; Hung, I.F.; Tam, A.R.; Chung, T.W.-H.; Chan, J.F.; Zhang, A.J.; et al. Lessons learned 1 year after SARS-CoV-2 emergence leading to COVID-19 pandemic. Emerg. Microbes Infect. 2021, 10, 507–535. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19; NICE Guideline; National Institute for Health and Care Excellence: London, UK, 2020; p. 35. [Google Scholar]
- Chung, T.W.-H.; Sridhar, S.; Zhang, A.J.; Chan, K.H.; Li, H.L.; Wong, F.K.; Ng, M.Y.; Tsang, R.K.; Lee, A.C.; Fan, Z.; et al. Olfactory Dysfunction in Coronavirus Disease 2019 Patients: Observational Cohort Study and Systematic Review. Open. Forum Infect. Dis. 2020, 7, ofaa199. [Google Scholar] [CrossRef] [PubMed]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and predictors of long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef]
- Ercoli, T.; Masala, C.; Pinna, I.; Orofino, G.; Solla, P.; Rocchi, L.; Defazio, G. Qualitative smell/taste disorders as sequelae of acute COVID-19. Neurol. Sci. 2021, 42, 4921–4926. [Google Scholar] [CrossRef]
- Peterson, J.; Lin, B.; Barrios-Camacho, C.M.; Herrick, D.B.; Holbrook, E.H.; Jang, W.; Coleman, J.H.; Schwob, J.E. Activating a Reserve Neural Stem Cell Population In Vitro Enables Engraftment and Multipotency after Transplantation. Stem Cell. Rep. 2019, 12, 680–695. [Google Scholar] [CrossRef]
- Paschaki, M.; Cammas, L.; Muta, Y.; Matsuoka, Y.; Mak, S.S.; Rataj-Baniowska, M.; Fraulob, V.; Dollé, P.; Ladher, R.K. Retinoic acid regulates olfactory progenitor cell fate and differentiation. Neural Dev. 2013, 8, 13. [Google Scholar] [CrossRef]
- Chung, T.W.-H.; Zhang, H.; Wong, F.K.-C.; Sridhar, S.; Chan, K.H.; Cheng, V.C.-C.; Yuen, K.Y.; Hung, I.F.-N.; Mak, H.K.-F. Neurosensory Rehabilitation and Olfactory Network Recovery in Covid-19-related Olfactory Dysfunction. Brain Sci. 2021, 11, 686. [Google Scholar] [CrossRef]
- Hummel, T.; Whitcroft, K.L.; Rueter, G.; Haehner, A. Intranasal vitamin A is beneficial in post-infectious olfactory loss. Eur. Arch. Otorhinolaryngol. 2017, 274, 2819–2825. [Google Scholar] [CrossRef]
- Kartal, D.; Yaşar, M.; Kartal, L.; Özcan, I.; Borlu, M. Effects of isotretinoin on the olfactory function in patients with acne. Bras. Derm. 2017, 92, 191–195. [Google Scholar] [CrossRef]
- Reden, J.; Lill, K.; Zahnert, T.; Haehner, A.; Hummel, T. Olfactory function in patients with postinfectious and posttraumatic smell disorders before and after treatment with vitamin A: A double-blind, placebo-controlled, randomized clinical trial. Laryngoscope 2012, 122, 1906–1909. [Google Scholar] [CrossRef]
- Duncan, R.B.; Briggs, M. Treatment of Uncomplicated Anosmia by Vitamin A. Arch. Otolaryngol. 1962, 75, 116–124. [Google Scholar] [CrossRef]
- Hopkins, C.; Alanin, M.; Philpott, C.; Harries, P.; Whitcroft, K.; Qureishi, A.; Anari, S.; Ramakrishnan, Y.; Sama, A.; Davies, E.; et al. Management of new onset loss of sense of smell during the COVID-19 pandemic—BRS Consensus Guidelines. Clin. Otolaryngol. 2021, 46, 16–22. [Google Scholar] [CrossRef]
- Addison, A.B.; Wong, B.; Ahmed, T.; Macchi, A.; Konstantinidis, I.; Huart, C.; Frasnelli, J.; Fjaeldstad, A.W.; Ramakrishnan, V.R.; Rombaux, P.; et al. Clinical Olfactory Working Group consensus statement on the treatment of postinfectious olfactory dysfunction. J. Allergy Clin. Immunol. 2021, 147, 1704–1719. [Google Scholar] [CrossRef]
- Vaira, L.A.; Hopkins, C.; Petrocelli, M.; Lechien, J.R.; Cutrupi, S.; Salzano, G.; Chiesa-Estomba, C.M.; Saussez, S.; De Riu, G. Efficacy of corticosteroid therapy in the treatment of long- lasting olfactory disorders in COVID-19 patients. Rhinology 2021, 59, 21–25. [Google Scholar] [CrossRef]
- Abdelalim, A.A.; Mohamady, A.A.; Elsayed, R.A.; Elawady, M.A.; Ghallab, A.F. Corticosteroid nasal spray for recovery of smell sensation in COVID-19 patients: A randomized controlled trial. Am. J. Otolaryngol. 2021, 42, 102884. [Google Scholar] [CrossRef]
- Kasiri, H.; Rouhani, N.; Salehifar, E.; Ghazaeian, M.; Fallah, S. Mometasone furoate nasal spray in the treatment of patients with COVID-19 olfactory dysfunction: A randomized, double blind clinical trial. Int. Immunopharmacol. 2021, 98, 107871. [Google Scholar] [CrossRef]
- Rashid, R.A.; Zgair, A.; Al-Ani, R.M. Effect of nasal corticosteroid in the treatment of anosmia due to COVID-19: A randomised double-blind placebo-controlled study. Am. J. Otolaryngol. 2021, 42, 103033. [Google Scholar] [CrossRef]
- Yildiz, E.; Koca Yildiz, S.; Kuzu, S.; Günebakan, Ç.; Bucak, A.; Kahveci, O.K. Comparison of the Healing Effect of Nasal Saline Irrigation with Triamcinolone Acetonide Versus Nasal Saline Irrigation alone in COVID-19 Related Olfactory Dysfunction: A Randomized Controlled Study. Indian J. Otolaryngol. Head Neck Surg. 2021, 74, 3022–3027. [Google Scholar] [CrossRef] [PubMed]
- Cain, W.S.; Gent, J.F.; Goodspeed, R.B.; Leonard, G. Evaluation of olfactory dysfunction in the Connecticut Chemosensory Clinical Research Center. Laryngoscope 1988, 98, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Doty, R.L.; Shaman, P.; Dann, M. Development of the University of Pennsylvania Smell Identification Test: A standardized microencapsulated test of olfactory function. Physiol. Behav. 1984, 32, 489–502. [Google Scholar] [CrossRef] [PubMed]
- Yousem, D.M.; Geckle, R.J.; Bilker, W.B.; McKeown, D.A.; Doty, R.L. Posttraumatic olfactory dysfunction: MR and clinical evaluation. AJNR Am. J. Neuroradiol. 1996, 17, 1171–1179. [Google Scholar] [PubMed]
- Oz, G.; Alger, J.R.; Barker, P.B.; Bartha, R.; Bizzi, A.; Boesch, C.; Bolan, P.J.; Brindle, K.M.; Cudalbu, C.; Dinçer, A.; et al. Clinical proton MR spectroscopy in central nervous system disorders. Radiology 2014, 270, 658–679. [Google Scholar] [CrossRef]
- Moffett, J.R.; Ross, B.; Arun, P.; Madhavarao, C.N.; Namboodiri, A.M. N-Acetylaspartate in the CNS: From neurodiagnostics to neurobiology. Prog. Neurobiol. 2007, 81, 89–131. [Google Scholar] [CrossRef]
- Ashburner, J. A fast diffeomorphic image registration algorithm. Neuroimage 2007, 38, 95–113. [Google Scholar] [CrossRef]
- Tzourio-Mazoyer, N.; Landeau, B.; Papathanassiou, D.; Crivello, F.; Etard, O.; Delcroix, N.; Mazoyer, B.; Joliot, M. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage 2002, 15, 273–289. [Google Scholar] [CrossRef]
- Fjaeldstad, A.; Fernandes, H.M.; Van Hartevelt, T.J.; Gleesborg, C.; Møller, A.; Ovesen, T.; Kringelbach, M.L. Brain fingerprints of olfaction: A novel structural method for assessing olfactory cortical networks in health and disease. Sci. Rep. 2017, 7, 42534. [Google Scholar] [CrossRef]
- Chu, H.; Chan, J.F.; Yuen, T.T.; Shuai, H.; Yuan, S.; Wang, Y.; Hu, B.; Yip, C.C.; Tsang, J.O.; Huang, X.; et al. Comparative tropism, replication kinetics, and cell damage profiling of SARS-CoV-2 and SARS-CoV with implications for clinical manifestations, transmissibility, and laboratory studies of COVID-19: An observational study. Lancet Microbe 2020, 1, e14–e23. [Google Scholar] [CrossRef]
- Zhang, B.Z.; Chu, H.; Han, S.; Shuai, H.; Deng, J.; Hu, Y.F.; Gong, H.R.; Lee, A.C.; Zou, Z.; Yau, T.; et al. SARS-CoV-2 infects human neural progenitor cells and brain organoids. Cell. Res. 2020, 30, 928–931. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.J.; Lee, A.C.; Chu, H.; Chan, J.F.; Fan, Z.; Li, C.; Liu, F.; Chen, Y.; Yuan, S.; Poon, V.K.; et al. Severe Acute Respiratory Syndrome Coronavirus 2 Infects and Damages the Mature and Immature Olfactory Sensory Neurons of Hamsters. Clin. Infect. Dis. 2021, 73, e503–e512. [Google Scholar] [CrossRef] [PubMed]
- Kirschenbaum, D.; Imbach, L.L.; Ulrich, S.; Rushing, E.J.; Keller, E.; Reimann, R.R.; Frauenknecht, K.B.M.; Lichtblau, M.; Witt, M.; Hummel, T.; et al. Inflammatory olfactory neuropathy in two patients with COVID-19. Lancet 2020, 396, 166. [Google Scholar] [CrossRef] [PubMed]
- Matschke, J.; Lütgehetmann, M.; Hagel, C.; Sperhake, J.P.; Schröder, A.S.; Edler, C.; Mushumba, H.; Fitzek, A.; Allweiss, L.; Dandri, M.; et al. Neuropathology of patients with COVID-19 in Germany: A post-mortem case series. Lancet Neurol. 2020, 19, 919–929. [Google Scholar] [CrossRef]
- Meinhardt, J.; Radke, J.; Dittmayer, C.; Franz, J.; Thomas, C.; Mothes, R.; Laue, M.; Schneider, J.; Brünink, S.; Greuel, S.; et al. Olfactory transmucosal SARS-CoV-2 invasion as a port of central nervous system entry in individuals with COVID-19. Nat. Neurosci. 2021, 24, 168–175. [Google Scholar] [CrossRef]
- Schurink, B.; Roos, E.; Radonic, T.; Barbe, E.; Bouman, C.S.C.; de Boer, H.H.; de Bree, G.J.; Bulle, E.B.; Aronica, E.M.; Florquin, S.; et al. Viral presence and immunopathology in patients with lethal COVID-19: A prospective autopsy cohort study. Lancet Microbe 2020, 1, e290–e299. [Google Scholar] [CrossRef]
- Bryche, B.; St Albin, A.; Murri, S.; Lacôte, S.; Pulido, C.; Ar Gouilh, M.; Lesellier, S.; Servat, A.; Wasniewski, M.; Picard-Meyer, E.; et al. Massive transient damage of the olfactory epithelium associated with infection of sustentacular cells by SARS-CoV-2 in golden Syrian hamsters. Brain Behav. Immun. 2020, 89, 579–586. [Google Scholar] [CrossRef]
- Zheng, J.; Wong, L.R.; Li, K.; Verma, A.K.; Ortiz, M.E.; Wohlford-Lenane, C.; Leidinger, M.R.; Knudson, C.M.; Meyerholz, D.K.; McCray, P.B., Jr.; et al. COVID-19 treatments and pathogenesis including anosmia in K18-hACE2 mice. Nature 2021, 589, 603–607. [Google Scholar] [CrossRef]
- Everett, H.E.; Lean, F.Z.X.; Byrne, A.M.P.; van Diemen, P.M.; Rhodes, S.; James, J.; Mollett, B.; Coward, V.J.; Skinner, P.; Warren, C.J.; et al. Intranasal Infection of Ferrets with SARS-CoV-2 as a Model for Asymptomatic Human Infection. Viruses 2021, 13, 113. [Google Scholar] [CrossRef]
- Jiao, L.; Yang, Y.; Yu, W.; Zhao, Y.; Long, H.; Gao, J.; Ding, K.; Ma, C.; Li, J.; Zhao, S.; et al. The olfactory route is a potential way for SARS-CoV-2 to invade the central nervous system of rhesus monkeys. Signal. Transduct. Target. Ther. 2021, 6, 169. [Google Scholar] [CrossRef]
- Brann, D.H.; Tsukahara, T.; Weinreb, C.; Lipovsek, M.; Van den Berge, K.; Gong, B.; Chance, R.; Macaulay, I.C.; Chou, H.J.; Fletcher, R.B.; et al. Non-neuronal expression of SARS-CoV-2 entry genes in the olfactory system suggests mechanisms underlying COVID-19-associated anosmia. Sci. Adv. 2020, 6, eabc5801. [Google Scholar] [CrossRef]
- Leung, C.T.; Coulombe, P.A.; Reed, R.R. Contribution of olfactory neural stem cells to tissue maintenance and regeneration. Nat. Neurosci. 2007, 10, 720–726. [Google Scholar] [CrossRef]
- Herrick, D.B.; Lin, B.; Peterson, J.; Schnittke, N.; Schwob, J.E. Notch1 maintains dormancy of olfactory horizontal basal cells, a reserve neural stem cell. Proc. Natl. Acad. Sci. USA 2017, 114, E5589–E5598. [Google Scholar] [CrossRef]
- Margulies, D.S.; Kelly, A.M.; Uddin, L.Q.; Biswal, B.B.; Castellanos, F.X.; Milham, M.P. Mapping the functional connectivity of anterior cingulate cortex. Neuroimage 2007, 37, 579–588. [Google Scholar] [CrossRef]
- Zahn, R.; Moll, J.; Krueger, F.; Huey, E.D.; Garrido, G.; Grafman, J. Social concepts are represented in the superior anterior temporal cortex. Proc. Natl. Acad. Sci. USA 2007, 104, 6430–6435. [Google Scholar] [CrossRef]
- Karnath, H.O. New insights into the functions of the superior temporal cortex. Nat. Rev. Neurosci. 2001, 2, 568–576. [Google Scholar] [CrossRef]
- Tyler, L.K.; Marslen-Wilson, W.D.; Randall, B.; Wright, P.; Devereux, B.J.; Zhuang, J.; Papoutsi, M.; Stamatakis, E.A. Left inferior frontal cortex and syntax: Function, structure and behaviour in patients with left hemisphere damage. Brain 2011, 134 Pt 2, 415–431. [Google Scholar] [CrossRef]
- Royet, J.P.; Koenig, O.; Gregoire, M.C.; Cinotti, L.; Lavenne, F.; Le Bars, D.; Costes, N.; Vigouroux, M.; Farget, V.; Sicard, G.; et al. Functional anatomy of perceptual and semantic processing for odors. J. Cogn. Neurosci. 1999, 11, 94–109. [Google Scholar] [CrossRef]
- Savic, I.; Berglund, H. Passive perception of odors and semantic circuits. Hum. Brain Mapp. 2004, 21, 271–278. [Google Scholar] [CrossRef]
- Zhang, H.; Chung, T.W.-H.; Wong, F.K.-C.; Hung, I.F.-N.; Mak, H.K.-F. Changes in the Intranetwork and Internetwork Connectivity of the Default Mode Network and Olfactory Network in Patients with COVID-19 and Olfactory Dysfunction. Brain Sci. 2022, 12, 511. [Google Scholar] [CrossRef]
- Menni, C.; Valdes, A.M.; Polidori, L.; Antonelli, M.; Penamakuri, S.; Nogal, A.; Louca, P.; May, A.; Figueiredo, J.C.; Hu, C.; et al. Symptom prevalence, duration, and risk of hospital admission in individuals infected with SARS-CoV-2 during periods of omicron and delta variant dominance: A prospective observational study from the ZOE COVID Study. Lancet 2022, 399, 1618–1624. [Google Scholar] [CrossRef] [PubMed]
- Vihta, K.D.; Pouwels, K.B.; Peto, T.E.; Pritchard, E.; House, T.; Studley, R.; Rourke, E.; Cook, D.; Diamond, I.; Crook, D.; et al. Omicron-associated changes in SARS-CoV-2 symptoms in the United Kingdom. Clin. Infect. Dis. 2022, 76, e133–e141. [Google Scholar] [PubMed]
- World Health Organization. Coronavirus Disease 2019 (COVID-19) Weekly Operational Update on COVID-19 9 September 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/weekly-updates/wou-9-september-2020-cleared.pdf?sfvrsn=d39784f7_2 (accessed on 14 September 2020).
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Damm, M.; Pikart, L.K.; Reimann, H.; Burkert, S.; Göktas, Ö.; Haxel, B.; Frey, S.; Charalampakis, I.; Beule, A.; Renner, B.; et al. Olfactory training is helpful in postinfectious olfactory loss: A randomized, controlled, multicenter study. Laryngoscope 2013, 124, 826–831. [Google Scholar] [CrossRef]
- Langdon, C.; Lehrer, E.; Berenguer, J.; Laxe, S.; Alobid, I.; Quintó, L.; Mariño-Sánchez, F.; Bernabeu, M.; Marin, C.; Mullol, J. Olfactory Training in Post-Traumatic Smell Impairment: Mild Improvement in Threshold Performances: Results from a Randomized Controlled Trial. J. Neurotrauma 2018, 35, 2641–2652. [Google Scholar] [CrossRef]
- Kollndorfer, K.; Fischmeister, F.; Kowalczyk, K.; Hoche, E.; Mueller, C.; Trattnig, S.; Schöpf, V. Olfactory training induces changes in regional functional connectivity in patients with long-term smell loss. NeuroImage Clin. 2015, 9, 401–410. [Google Scholar] [CrossRef]
- Al Aïn, S.; Poupon, D.; Hétu, S.; Mercier, N.; Steffener, J.; Frasnelli, J. Smell training improves olfactory function and alters brain structure. Neuroimage 2019, 189, 45–54. [Google Scholar] [CrossRef]
- Shearer, K.D.; Stoney, P.N.; Morgan, P.J.; McCaffery, P.J. A vitamin for the brain. Trends Neurosci. 2012, 35, 733–741. [Google Scholar] [CrossRef]
- World Health Organization. Measles. Available online: https://www.who.int/news-room/fact-sheets/detail/measles (accessed on 22 July 2020).
- Huiming, Y.; Chaomin, W.; Meng, M. Vitamin A for treating measles in children. Cochrane Database Syst Rev. 2005, 2005, CD001479. [Google Scholar]
- Hussey, G.D.; Klein, M. A Randomized, Controlled Trial of Vitamin A in Children with Severe Measles. N. Engl. J. Med. 1990, 323, 160–164. [Google Scholar] [CrossRef]
- Psaltis, A.; Li, G.; Vaezeafshar, R.; Cho, K.; Hwang, P.H. Modification of the lund-kennedy endoscopic scoring system improves its reliability and correlation with patient-reported outcome measures. Laryngoscope 2014, 124, 2216–2223. [Google Scholar] [CrossRef]
- Guidance for Industry: Converting Units of Measure for Folate, Niacin, and Vitamins A, D, and E on the Nutrition and Supplement Facts Labels. Docket Number: FDA-2016-D-4484. Center for Food Safety and Applied Nutrition. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/guidance-industry-converting-units-measure-folate-niacin-and-vitamins-d-and-e-nutrition-and (accessed on 22 July 2020).
- Vitamin A Fact Sheet for Health Professionals. Available online: https://ods.od.nih.gov/factsheets/Vitamin%20A-HealthProfessional/#en5 (accessed on 15 June 2020).
- Reichert, J.L.; Schöpf, V. Olfactory Loss and Regain: Lessons for Neuroplasticity. Neurosci. 2017, 24, 22–35. [Google Scholar] [CrossRef]
- Kollndorfer, K.; Kowalczyk, K.; Hoche, E.; Mueller, C.A.; Pollak, M.; Trattnig, S.; Schöpf, V. Recovery of Olfactory Function Induces Neuroplasticity Effects in Patients with Smell Loss. Neural Plast. 2014, 2014, 140419. [Google Scholar] [CrossRef]
- Karunanayaka, P.R.; Wilson, D.A.; Tobia, M.J.; Martinez, B.E.; Meadowcroft, M.D.; Eslinger, P.J.; Yang, Q.X. Default mode network deactivation during odor-visual association. Hum. Brain Mapp. 2016, 38, 1125–1139. [Google Scholar] [CrossRef]
- Lu, J.; Yang, Q.X.; Zhang, H.; Eslinger, P.J.; Zhang, X.; Wu, S.; Zhang, B.; Zhu, B.; Prasanna, R. Karunanayaka. Disruptions of the olfactory and default mode networks in Alzheimer’s disease. Brain Behav. 2019, 9, e01296. [Google Scholar] [CrossRef]
- Zhang, H.; Hao, Y.; Manor, B.; Novak, P.; Milberg, W.; Zhang, J.; Fang, J.; Novak, V. Intranasal insulin enhanced resting-state functional connectivity of hippocampal regions in type 2 diabetes. Diabetes 2015, 64, 1025–1034. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intervention Groups | |||
|---|---|---|---|
| Characteristics | Combination (n = 9) | Standard Care (n = 8) | Control (n = 5) |
| Median age (IQR)–year | 36 (26.0–43.0) | 49 (37.3–56.3) | 58 (50.0–61.0) |
| Female sex–no. (%) | 5 (56) | 6 (75) | 3 (60) |
| Tobacco smoker–no. (%) | 3 (33) | 0 (0) | 0 (0) |
| Coexisting conditions–no. (%) | |||
| Good past health | 8 (89) | 4 (50) | 2 (40) |
| Diabetes mellitus | 0 (0) | 0 (0) | 1 (20) |
| Hypertension | 0 (0) | 1 (13) | 2 (40) |
| Hyperlipidaemia | 1 (11) | 0 (0) | 1 (20) |
| Atherosclerotic diseases | 0 (0) | 2 (25) | 1 (20) |
| Rheumatological conditions | 1 † (11) | 0 (0) | 0 (0) |
| Malignancies | 0 (0) | 0 (0) | 2 ‡ (40) |
| History of haematological or solid organ transplantation | 0 (0) | 0 (0) | 0 (0) |
| SARS-CoV-2 diagnosis | |||
| Positive RT–PCR–no. (%) | 9 (100) | 8 (100) | 5 (100) |
| CT values (IQR) | 22.1 (18.1–29.0) | 20.1 (15.1–21.7) | 17.2 (15.7–22.8) |
| COVID–19 disease severity | |||
| Mild disease–no. (%) | 9 (100) | 8 (100) | 5 (100) |
| COVID–19-related OD, onset and duration (IQR)–days | |||
| Onset of OD from first COVID–19 symptom | 0.0 (0.0–7.0) | 4.0 (1.8–16.0) | 3.0 (0.0–3.0) |
| Median duration of COVID–19-related OD | 159 (130.0–163.0) | 164.5 (118.3–180.3) | 138.0 (135.0–225.0) |
| COVID–19-related OD, symptomatology–no. (%) | |||
| OD onset | |||
| Sudden | 6 (67) | 6 (75) | 1 (20) |
| Gradual | 3 (33) | 2 (25) | 4 (80) |
| OD characteristics | |||
| Anosmia | 4 (44) | 5 (63) | 2 (40) |
| Hyposmia | 4 (44) | 2 (25) | 3 (60) |
| Parosmia | 1 (11) | 3 (38) | 0 (0) |
| Hyperosmia | 0 (0) | 0 (0) | 0 (0) |
| Phantosmia ※ | 2 (22%) | 1 (13) | 0 (0) |
| Olfactory assessments–mean (SD) | |||
| Modified LK score | 0.7 (1.0) | 0.0 (0.0) | 0.0 (0.0) |
| BTT | 2.9 (1.1) | 2.0 (1.1) | 1.8 (1.0) |
| SIT | 24.6 (7.7) | 24.5 (6.3) | 19.6 (9.0) |
| SIT category–no. (%) | |||
| Normosmia | 1 (11) | 0 (0) | 0 (0) |
| Mild microsmia | 1 (11) | 2 (25) | 0 (0) |
| Moderate microsmia | 3 (33) | 2 (25) | 1 (20) |
| Severe microsmia | 1 (11) | 2 (25) | 2 (40) |
| Anosmia | 3 (33) | 2 (25) | 2 (40) |
| Olfactory Cortical Network Regions | Cluster Size | Peak z Value |
|---|---|---|
| Combination group vs. standard care group | ||
| Right gyrus rectus | 21 | 6.4 |
| Combination group vs. control group | ||
| Left anterior cingulate cortex | 38 | 5.0 |
| Right anterior cingulate cortex | 7 | 4.2 |
| Left superior temporal gyrus | 28 | 5.2 |
| Standard care group vs. control group | ||
| Left anterior cingulate cortex | 24 | 4.8 |
| Left superior temporal gyrus | 20 | 6.0 |
| Interim Assessment (Week 2) | End-of-Treatment Assessment (Week 4) | ||||
|---|---|---|---|---|---|
| OCN Regions | Cluster Size | Peak z Value | OCN Regions | Cluster Size | Peak z Value |
| Combination group vs. control group | |||||
| Right medial frontal gyrus | 23 | 5.6 | Left inferior frontal gyrus | 21 | 4.2 |
| Standard care group vs. control group | |||||
| Right superior temporal gyrus | 22 | 6.1 | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, T.W.-H.; Zhang, H.; Wong, F.K.-C.; Sridhar, S.; Lee, T.M.-C.; Leung, G.K.-K.; Chan, K.-H.; Lau, K.-K.; Tam, A.R.; Ho, D.T.-Y.; et al. A Pilot Study of Short-Course Oral Vitamin A and Aerosolised Diffuser Olfactory Training for the Treatment of Smell Loss in Long COVID. Brain Sci. 2023, 13, 1014. https://doi.org/10.3390/brainsci13071014
Chung TW-H, Zhang H, Wong FK-C, Sridhar S, Lee TM-C, Leung GK-K, Chan K-H, Lau K-K, Tam AR, Ho DT-Y, et al. A Pilot Study of Short-Course Oral Vitamin A and Aerosolised Diffuser Olfactory Training for the Treatment of Smell Loss in Long COVID. Brain Sciences. 2023; 13(7):1014. https://doi.org/10.3390/brainsci13071014
Chicago/Turabian StyleChung, Tom Wai-Hin, Hui Zhang, Fergus Kai-Chuen Wong, Siddharth Sridhar, Tatia Mei-Chun Lee, Gilberto Ka-Kit Leung, Koon-Ho Chan, Kui-Kai Lau, Anthony Raymond Tam, Deborah Tip-Yin Ho, and et al. 2023. "A Pilot Study of Short-Course Oral Vitamin A and Aerosolised Diffuser Olfactory Training for the Treatment of Smell Loss in Long COVID" Brain Sciences 13, no. 7: 1014. https://doi.org/10.3390/brainsci13071014
APA StyleChung, T. W.-H., Zhang, H., Wong, F. K.-C., Sridhar, S., Lee, T. M.-C., Leung, G. K.-K., Chan, K.-H., Lau, K.-K., Tam, A. R., Ho, D. T.-Y., Cheng, V. C.-C., Yuen, K.-Y., Hung, I. F.-N., & Mak, H. K.-F. (2023). A Pilot Study of Short-Course Oral Vitamin A and Aerosolised Diffuser Olfactory Training for the Treatment of Smell Loss in Long COVID. Brain Sciences, 13(7), 1014. https://doi.org/10.3390/brainsci13071014