

Evaluation of MTT Heterogeneity of Perfusion CT Imaging in the Early Brain Injury Phase: An Insight into aSAH Pathopysiology

 , ,
, ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Inclusion Criteria
2.3. aSAH Management
2.4. Perfusion CT Analysis
2.5. Definition of Outcome Measures
2.6. Statistical Analysis
3. Results
3.1. Patient Cohort
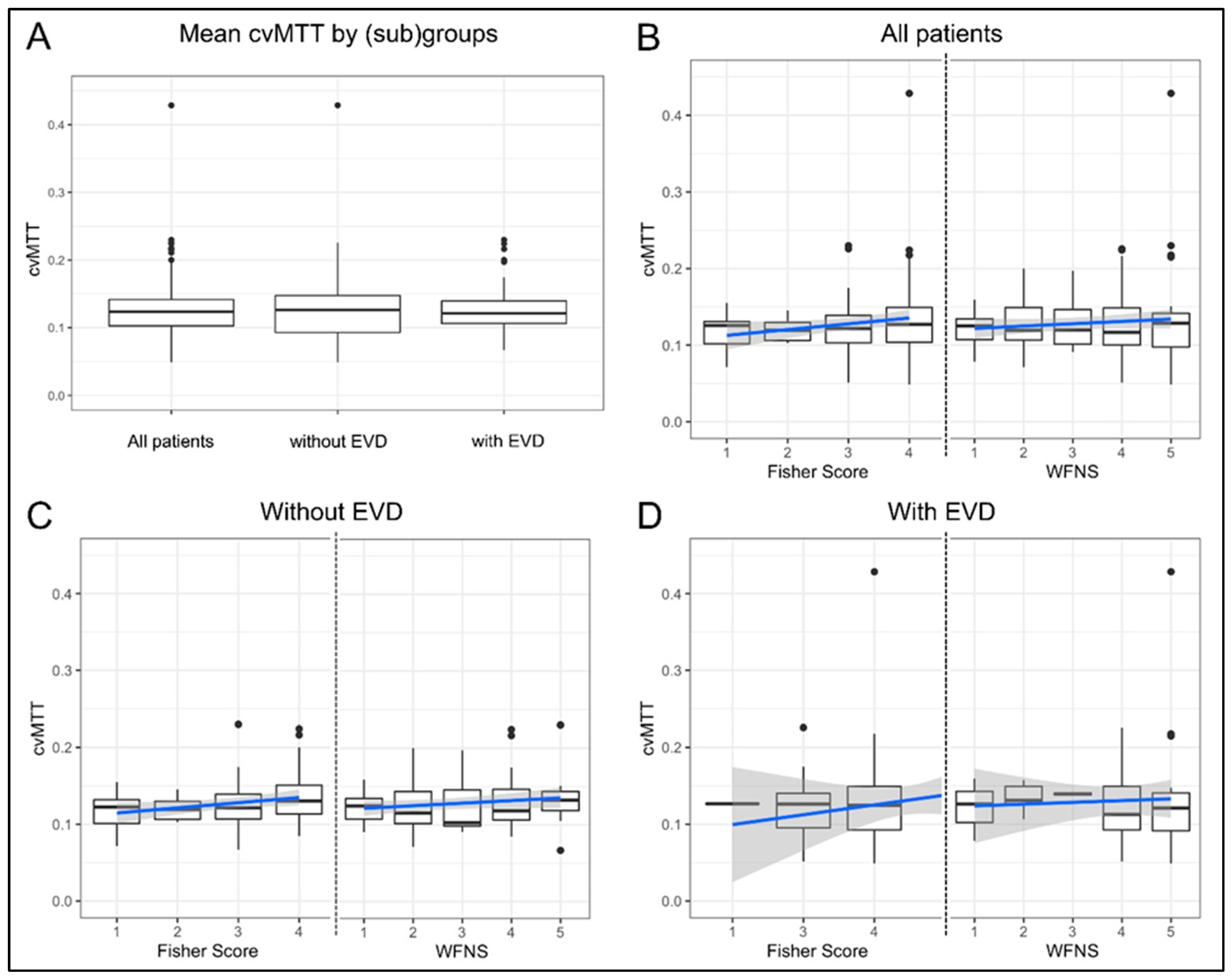
3.2. Early MTT Heterogeneity
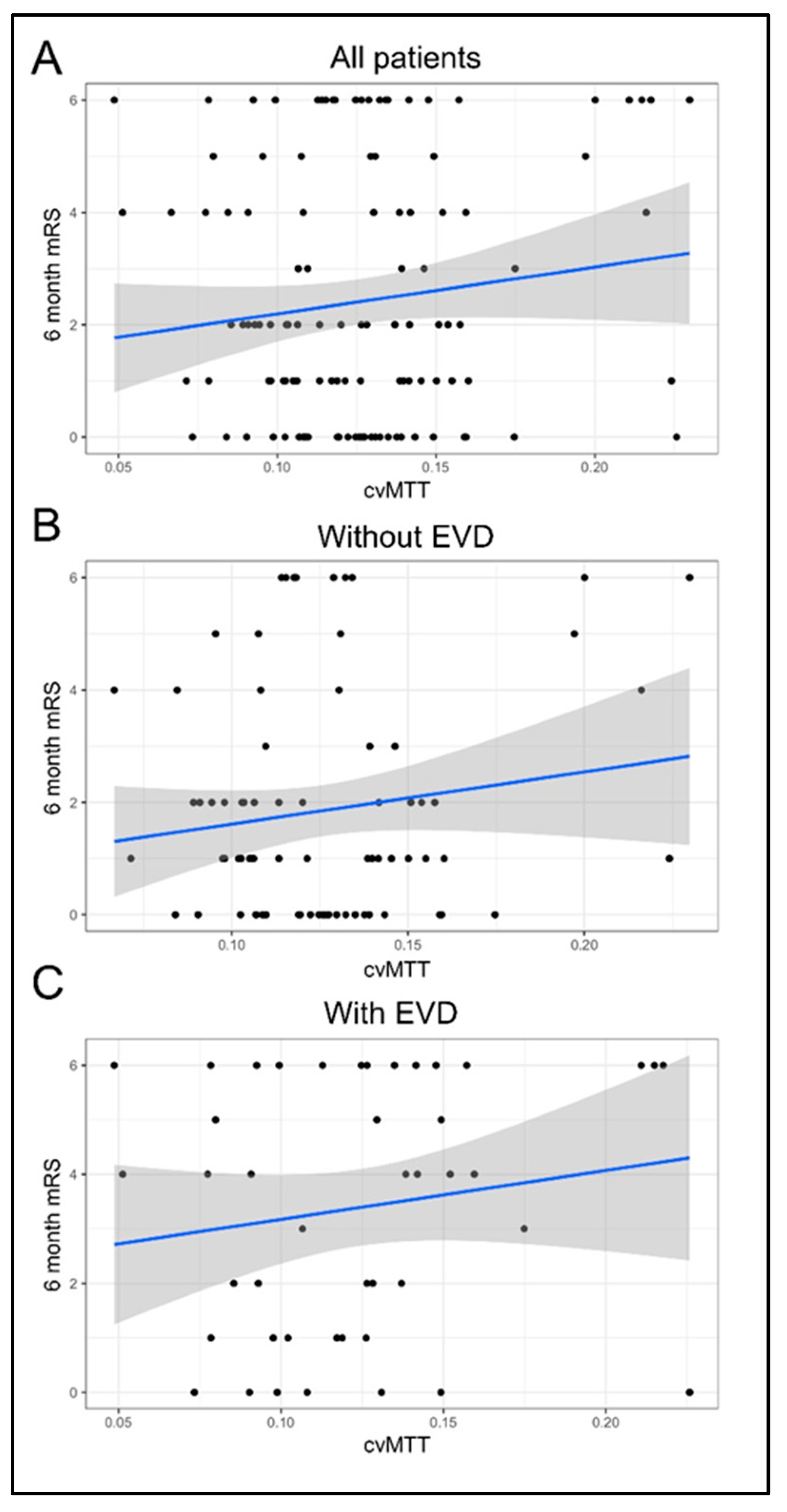
3.3. Early CTP Heterogeneity Does Not Correlate with 6-Month mRS
4. Discussion
- (1)
- The heterogeneity of microvascular perfusion, as defined by cvMTT in early CTP imaging during the EBI phase of aSAH, did not significantly correlate with the dichotomized outcome after 6 months;
- (2)
- There was no significant difference in the mean heterogeneity of microvascular perfusion, as defined by mean cvMTT, between patients with and without EVD at the time of early CTP imaging;
- (3)
- The heterogeneity of microvascular perfusion, as defined by cvMTT at early CTP imaging, did not significantly correlate with the initial WFNS grade or Fisher score.
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Al-Khindi, T.; Macdonald, R.L.; Schweizer, T.A. Cognitive and Functional Outcome After Aneurysmal Subarachnoid Hemorrhage. Stroke 2010, 41, e519–e536. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, R.L. Delayed neurological deterioration after subarachnoid haemorrhage. Nat. Rev. Neurol. 2014, 10, 44–58. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Guillén, N.M.; León-López, R.; Túnez-Fiñana, I.; Cano-Sánchez, A. From vasospasm to early brain injury: New frontiers in subarachnoid haemorrhage research. Neurología 2013, 28, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Lauritzen, M.; Dreier, J.P.; Fabricius, M.; Hartings, J.A.; Graf, R.; Strong, A.J. Clinical Relevance of Cortical Spreading Depression in Neurological Disorders: Migraine, Malignant Stroke, Subarachnoid and Intracranial Hemorrhage, and Traumatic Brain Injury. J. Cereb. Blood Flow Metab. 2010, 31, 17–35. [Google Scholar] [CrossRef]
- Pluta, R.M.; Hansen-Schwartz, J.; Dreier, J.; Vajkoczy, P.; Macdonald, R.L.; Nishizawa, S.; Kasuya, H.; Wellman, G.; Keller, E.; Zauner, A.; et al. Cerebral vasospasm following subarachnoid hemorrhage: Time for a new world of thought. Neurol. Res. 2009, 31, 151–158. [Google Scholar] [CrossRef] [PubMed]
- van Lieshout, J.H.; Dibue-Adjei, M.; Cornelius, J.F.; Slotty, P.J.; Schneider, T.; Restin, T.; Boogaarts, H.D.; Steiger, H.J.; Petridis, A.K.; Kamp, M.A. An introduction to the pathophysiology of aneurysmal subarachnoid hemorrhage. Neurosurg. Rev. 2018, 41, 917–930. [Google Scholar] [CrossRef] [PubMed]
- Etminan, N.; Beseoglu, K.; Heiroth, H.J.; Turowski, B.; Steiger, H.J.; Hanggi, D. Early perfusion computerized tomography imaging as a radiographic surrogate for delayed cerebral ischemia and functional outcome after subarachnoid hemorrhage. Stroke 2013, 44, 1260–1266. [Google Scholar] [CrossRef]
- Kamp, M.A.; Heiroth, H.J.; Beseoglu, K.; Turowski, B.; Steiger, H.J.; Hanggi, D. Early CT perfusion measurement after aneurysmal subarachnoid hemorrhage: A screening method to predict outcome? Acta Neurochir. Suppl. 2012, 114, 329–332. [Google Scholar] [CrossRef]
- Sehba, F.A.; Hou, J.; Pluta, R.M.; Zhang, J.H. The importance of early brain injury after subarachnoid hemorrhage. Prog. Neurobiol. 2012, 97, 14–37. [Google Scholar] [CrossRef]
- Fujii, M.; Yan, J.; Rolland, W.B.; Soejima, Y.; Caner, B.; Zhang, J.H. Early brain injury, an evolving frontier in subarachnoid hemorrhage research. Transl. Stroke Res. 2013, 4, 432–446. [Google Scholar] [CrossRef]
- Grote, E.; Hassler, W. The critical first minutes after subarachnoid hemorrhage. Neurosurgery 1988, 22, 654–661. [Google Scholar] [CrossRef] [PubMed]
- Forcione, M.; Chiarelli, A.M.; Davies, D.J.; Perpetuini, D.; Sawosz, P.; Merla, A.; Belli, A. Cerebral perfusion and blood–brain barrier assessment in brain trauma using contrast-enhanced near-infrared spectroscopy with indocyanine green: A review. J. Cereb. Blood Flow Metab. 2020, 40, 1586–1598. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Wang, B.; Wolfowitz, R.; Yeh, P.H.; Nathan, D.E.; Graner, J.; Tang, H.; Pan, H.; Harper, J.; Pham, D. Perfusion deficits in patients with mild traumatic brain injury characterized by dynamic susceptibility contrast MRI. NMR Biomed. 2013, 26, 651–663. [Google Scholar] [CrossRef]
- Kamp, M.A.; Sarikaya-Seiwert, S.; Petridis, A.K.; Beez, T.; Cornelius, J.F.; Steiger, H.-J.; Turowski, B.; Slotty, P.J. Intraoperative indocyanine green–based cortical perfusion assessment in patients suffering from severe traumatic brain injury. World Neurosurg. 2017, 101, 431–443. [Google Scholar] [CrossRef] [PubMed]
- Starnoni, D.; Maduri, R.; Hajdu, S.D.; Pierzchala, K.; Giammattei, L.; Rocca, A.; Grosfilley, S.B.; Saliou, G.; Messerer, M.; Daniel, R.T. Early Perfusion Computed Tomography Scan for Prediction of Vasospasm and Delayed Cerebral Ischemia After Aneurysmal Subarachnoid Hemorrhage. World Neurosurg. 2019, 130, e743–e752. [Google Scholar] [CrossRef] [PubMed]
- Binaghi, S.; Colleoni, M.L.; Maeder, P.; Uské, A.; Regli, L.; Dehdashti, A.R.; Schnyder, P.; Meuli, R. CT Angiography and Perfusion CT in Cerebral Vasospasm after Subarachnoid Hemorrhage. Am. J. Neuroradiol. 2007, 28, 750. [Google Scholar]
- Dankbaar, J.W.; de Rooij, N.K.; Rijsdijk, M.; Velthuis, B.K.; Frijns, C.J.M.; Rinkel, G.J.E.; van der Schaaf, I.C. Diagnostic Threshold Values of Cerebral Perfusion Measured With Computed Tomography for Delayed Cerebral Ischemia After Aneurysmal Subarachnoid Hemorrhage. Stroke 2010, 41, 1927–1932. [Google Scholar] [CrossRef]
- Beseoglu, K.; Etminan, N.; Hanggi, D. The value of perfusion computed tomography (PCT) imaging after aneurysmal subarachnoid hemorrhage: A review of the current data. Acta Neurochir. Suppl. 2015, 120, 35–38. [Google Scholar] [CrossRef]
- Caspers, J.; Rubbert, C.; Turowski, B.; Martens, D.; Reichelt, D.C.; May, R.; Aissa, J.; Hanggi, D.; Etminan, N.; Mathys, C. Timing of Mean Transit Time Maximization is Associated with Neurological Outcome After Subarachnoid Hemorrhage. Clin. Neuroradiol. 2017, 27, 15–22. [Google Scholar] [CrossRef]
- Turowski, B.; Haenggi, D.; Wittsack, J.; Beck, A.; Moedder, U. Cerebral perfusion computerized tomography in vasospasm after subarachnoid hemorrhage: Diagnostic value of MTT. Rofo 2007, 179, 847–854. [Google Scholar] [CrossRef]
- Ostergaard, L.; Aamand, R.; Karabegovic, S.; Tietze, A.; Blicher, J.U.; Mikkelsen, I.K.; Iversen, N.K.; Secher, N.; Engedal, T.S.; Anzabi, M.; et al. The role of the microcirculation in delayed cerebral ischemia and chronic degenerative changes after subarachnoid hemorrhage. J. Cereb. Blood Flow Metab. 2013, 33, 1825–1837. [Google Scholar] [CrossRef] [PubMed]
- Jespersen, S.N.; Ostergaard, L. The roles of cerebral blood flow, capillary transit time heterogeneity, and oxygen tension in brain oxygenation and metabolism. J. Cereb. Blood Flow Metab. 2012, 32, 264–277. [Google Scholar] [CrossRef] [PubMed]
- Østergaard, L. Blood flow, capillary transit times, and tissue oxygenation: The centennial of capillary recruitment. J. Appl. Physiol. 2020, 129, 1413–1421. [Google Scholar] [CrossRef] [PubMed]
- Anzabi, M.; Angleys, H.; Aamand, R.; Ardalan, M.; Mouridsen, K.; Rasmussen, P.M.; Sørensen, J.C.H.; Plesnila, N.; Østergaard, L.; Iversen, N.K. Capillary flow disturbances after experimental subarachnoid hemorrhage: A contributor to delayed cerebral ischemia? Microcirculation 2019, 26, e12516. [Google Scholar] [CrossRef]
- Hofmann, B.B.; Fischer, I.; Engel, A.; Jannusch, K.; Donaldson, D.M.; Karadag, C.; van Lieshout, J.H.; Beseoglu, K.; Muhammad, S.; Turowski, B.; et al. MTT Heterogeneity in Perfusion CT Imaging as a Predictor of Outcome after Aneurysmal SAH. AJNR Am. J. Neuroradiol. 2021, 42, 1387–1395. [Google Scholar] [CrossRef]
- Connolly, E.S., Jr.; Rabinstein, A.A.; Carhuapoma, J.R.; Derdeyn, C.P.; Dion, J.; Higashida, R.T.; Hoh, B.L.; Kirkness, C.J.; Naidech, A.M.; Ogilvy, C.S.; et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: A guideline for healthcare professionals from the American Heart Association/american Stroke Association. Stroke 2012, 43, 1711–1737. [Google Scholar] [CrossRef]
- Turowski, B.; Haenggi, D.; Wittsack, H.J.; Beck, A.; Aurich, V. Computerized analysis of brain perfusion parameter images. RoFo 2007, 179, 525–529. [Google Scholar] [CrossRef]
- Wittsack, H.J.; Wohlschlager, A.M.; Ritzl, E.K.; Kleiser, R.; Cohnen, M.; Seitz, R.J.; Modder, U. CT-perfusion imaging of the human brain: Advanced deconvolution analysis using circulant singular value decomposition. Comput. Med. Imaging Graph. 2008, 32, 67–77. [Google Scholar] [CrossRef]
- Teasdale, G.M.; Drake, C.G.; Hunt, W.; Kassell, N.; Sano, K.; Pertuiset, B.; De Villiers, J.C. A universal subarachnoid hemorrhage scale: Report of a committee of the World Federation of Neurosurgical Societies. J. Neurol. Neurosurg. Psychiatry 1988, 51, 1457. [Google Scholar] [CrossRef]
- Rankin, J. Cerebral vascular accidents in patients over the age of 60. II. Prognosis. Scott. Med. J. 1957, 2, 200–215. [Google Scholar] [CrossRef]
- Kamp, M.A.; Dibue, M.; Schneider, T.; Steiger, H.J.; Hanggi, D. Calcium and potassium channels in experimental subarachnoid hemorrhage and transient global ischemia. Stroke Res. Treat. 2012, 2012, 382146. [Google Scholar] [CrossRef] [PubMed]
- Voldby, B.; Enevoldsen, E.M. Intracranial pressure changes following aneurysm rupture: Part 1: Clinical and angiographic correlations. J. Neurosurg. 1982, 56, 186–196. [Google Scholar] [CrossRef] [PubMed]
- Slotty, P.J.; Kamp, M.A.; Steiger, S.H.; Cornelius, J.F.; Macht, S.; Stummer, W.; Turowski, B. Cerebral perfusion changes in chronic subdural hematoma. J. Neurotrauma 2013, 30, 347–351. [Google Scholar] [CrossRef]
- Hofmann, B.B.; Donaldson, D.M.; Fischer, I.; Karadag, C.; Neyazi, M.; Piedade, G.S.; Abusabha, Y.; Muhammad, S.; Rubbert, C.; Hänggi, D.; et al. Blood Pressure Affects the Early CT Perfusion Imaging in Patients with aSAH Reflecting Early Disturbed Autoregulation. Neurocrit. Care 2023. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All Patients | With EVD | Without EVD | |
|---|---|---|---|
| No. (%) | No. (%) | No. (%) | |
| Total | 124 (100) | 45 (100) | 79 (100) |
| Age | |||
| <50 years | 41 (33.1) | 8 (17.8) | 33 (41.8) |
| ≥50 years | 83 (66.9) | 37 (82.2) | 46 (58.2) |
| Sex | |||
| Female | 83 (66.9) | 32 (71.1) | 51 (64.6) |
| Male | 41 (33.1) | 13 (28.9) | 28 (35.4) |
| WFNS grade | |||
| I–III | 61 (49.2) | 10 (22.2) | 51 (64.6) |
| IV–V | 63 (50.8) | 35 (77.8) | 28 (35.4) |
| Fisher grade | |||
| 0–II | 22 (17.7) | 1 (2.2) | 21 (26.6) |
| III–IV | 102 (82.3) | 44 (97.8) | 58 (73.4) |
| Aneurysm location | |||
| ACA | 1 (0.8) | 0 (0.0) | 1 (1.3) |
| Acom | 49 (39.5) | 17 (37.8) | 32 (40.5) |
| BA | 12 (9.7) | 8 (17.8) | 4 (5.1) |
| ICA | 5 (4.0) | 3 (6.7) | 2 (2.5) |
| MCA | 21 (16.9) | 6 (13.3) | 15 (19.0) |
| PcaA | 4 (3.2) | 1 (2.2) | 3 (3.8) |
| PCOM | 14 (11.3) | 2 (4.4) | 12 (15.2) |
| PICA | 10 (8.1) | 7 (15.6) | 3 (3.8) |
| SCA | 2 (1.6) | 0 (0.0) | 2 (2.5) |
| VA | 4 (3.2) | 1 (2.2) | 3 (3.8) |
| Other | 2 (1.6) | 0 (0.0) | 2 (2.5) |
| Therapy | |||
| Endovascular | 59 (47.6) | 24 (53.3) | 35 (44.3) |
| Surgical | 59 (47.6) | 19 (42.3) | 40 (50.6) |
| Combined/no treatment | 6 (4.8) | 2 (4.4) | 4 (5.1) |
| mRS 6 months | |||
| 0–2 | 76 (61.3) | 18 (40.0) | 58 (73.4) |
| 3–5 | 24 (19.4) | 12 (26.7) | 12 (15.2) |
| 6 | 24 (19.4) | 15 (33.3) | 9 (11.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hofmann, B.B.; Fischer, I.; Donaldson, D.M.; Abusabha, Y.; Karadag, C.; Muhammad, S.; Beseoglu, K.; Hänggi, D.; Turowski, B.; Rubbert, C.; et al. Evaluation of MTT Heterogeneity of Perfusion CT Imaging in the Early Brain Injury Phase: An Insight into aSAH Pathopysiology. Brain Sci. 2023, 13, 824. https://doi.org/10.3390/brainsci13050824
Hofmann BB, Fischer I, Donaldson DM, Abusabha Y, Karadag C, Muhammad S, Beseoglu K, Hänggi D, Turowski B, Rubbert C, et al. Evaluation of MTT Heterogeneity of Perfusion CT Imaging in the Early Brain Injury Phase: An Insight into aSAH Pathopysiology. Brain Sciences. 2023; 13(5):824. https://doi.org/10.3390/brainsci13050824
Chicago/Turabian StyleHofmann, Björn B., Igor Fischer, Daniel M. Donaldson, Yousef Abusabha, Cihat Karadag, Sajjad Muhammad, Kerim Beseoglu, Daniel Hänggi, Bernd Turowski, Christian Rubbert, and et al. 2023. "Evaluation of MTT Heterogeneity of Perfusion CT Imaging in the Early Brain Injury Phase: An Insight into aSAH Pathopysiology" Brain Sciences 13, no. 5: 824. https://doi.org/10.3390/brainsci13050824
APA StyleHofmann, B. B., Fischer, I., Donaldson, D. M., Abusabha, Y., Karadag, C., Muhammad, S., Beseoglu, K., Hänggi, D., Turowski, B., Rubbert, C., Cornelius, J. F., & Kamp, M. A. (2023). Evaluation of MTT Heterogeneity of Perfusion CT Imaging in the Early Brain Injury Phase: An Insight into aSAH Pathopysiology. Brain Sciences, 13(5), 824. https://doi.org/10.3390/brainsci13050824