
Machine Learning for Early Diagnosis of ATTRv Amyloidosis in Non-Endemic Areas: A Multicenter Study from Italy

 ,
, 
 ,
,  , , , ,
, , , ,  , and
, and 
Abstract
1. Introduction
2. Methods
2.1. Study Procedures
2.2. Patient’s Population
2.3. Clinical Variables: “Red Flags”
2.4. Machine Learning Analysis
3. Results
4. Discussion
5. Limitations and Future Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Disclosures
References
- Adams, D.; Ando, Y.; Beirão, J.M.; Coelho, T.; Gertz, M.A.; Gillmore, J.D.; Hawkins, P.N.; Lousada, I.; Suhr, O.B.; Merlini, G. Expert consensus recommendations to improve diagnosis of ATTR amyloidosis with polyneuropathy. J. Neurol. 2021, 268, 2109–2122. [Google Scholar] [CrossRef]
- Waddington-Cruz, M.; Schmidt, H.; Botteman, M.F.; Carter, J.A.; Stewart, M.; Hopps, M.; Fallet, S.; Amass, L. Epidemiological and clinical characteristics of symptomatic hereditary transthyretin amyloid polyneuropathy: A global case series. Orphanet J. Rare Dis. 2019, 14, 34. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, H.H.; Waddington-Cruz, M.; Botteman, M.F.; Carter, J.; Chopra, A.S.; Hopps, M.; Stewart, M.; Fallet, S.; Amass, L. Estimating the global prevalence of transthyretin familial amyloid polyneuropathy. Muscle Nerve 2018, 57, 829–837. [Google Scholar] [CrossRef] [PubMed]
- Gertz, M.; Adams, D.; Ando, Y.; Beirão, J.M.; Bokhari, S.; Coelho, T.; Comenzo, R.L.; Damy, T.; Dorbala, S.; Drachman, B.M.; et al. Avoiding misdiagnosis: Expert consensus recommendations for the suspicion and diagnosis of transthyretin amyloidosis for the general practitioner. BMC Fam. Pract. 2020, 21, 198. [Google Scholar] [CrossRef]
- Cortese, A.; Vegezzi, E.; Lozza, A.; Alfonsi, E.; Montini, A.; Moglia, A.; Merlini, G.; Obici, L. Diagnostic challenges in hereditary transthyretin amyloidosis with polyneuropathy: Avoiding misdiagnosis of a treatable hereditary neuropathy. J. Neurol. Neurosurg. Psychiatry 2017, 88, 457–458. [Google Scholar] [CrossRef] [PubMed]
- Russo, M.; Obici, L.; Bartolomei, I.; Cappelli, F.; Luigetti, M.; Fenu, S.; Cavallaro, T.; Chiappini, M.G.; Gemelli, C.; Pradotto, L.G.; et al. ATTRv amyloidosis Italian Registry: Clinical and epidemiological data. Amyloid 2020, 27, 259–265. [Google Scholar] [CrossRef]
- Koike, H.; Hashimoto, R.; Tomita, M.; Kawagashira, Y.; Iijima, M.; Tanaka, F.; Sobue, G. Diagnosis of sporadic transthyretin Val30Met familial amyloid polyneuropathy: A practical analysis. Amyloid 2011, 18, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Sekijima, Y.; Ueda, M.; Koike, H.; Misawa, S.; Ishii, T.; Ando, Y. Diagnosis and management of transthyretin familial amyloid polyneuropathy in Japan: Red-flag symptom clusters and treatment algorithm. Orphanet J. Rare Dis. 2018, 13, 6. [Google Scholar] [CrossRef]
- Russo, M.; Gentile, L.; Toscano, A.; Aguennouz, M.; Vita, G.; Mazzeo, A. Advances in Treatment of ATTRv Amyloidosis: State of the Art and Future Prospects. Brain Sci. 2020, 10, 952. [Google Scholar] [CrossRef]
- Di Stefano, V.; Fava, A.; Gentile, L.; Guaraldi, P.; Leonardi, L.; Poli, L.; Tagliapietra, M.; Vastola, M.; Fanara, S.; Ferrero, B.; et al. Italian Real-Life Experience of Patients with Hereditary Transthyretin Amyloidosis Treated with Patisiran. Pharmacogenom. Pers. Med. 2022, 15, 499–514. [Google Scholar] [CrossRef]
- Di Lisi, D.; Di Stefano, V.; Brighina, F.; Galassi, A.R.; Novo, G. Therapy of ATTR Cardiac Amyloidosis: Current Indications. Curr. Probl. Cardiol. 2023, 48, 101487. [Google Scholar] [CrossRef] [PubMed]
- Nativi-Nicolau, J.N.; Karam, C.; Khella, S.; Maurer, M.S. Screening for ATTR amyloidosis in the clinic: Overlapping disorders, misdiagnosis, and multiorgan awareness. Heart Fail. Rev. 2021, 27, 785–793. [Google Scholar] [CrossRef]
- Brownrigg, J.; Lorenzini, M.; Lumley, M.; Elliott, P. Diagnostic performance of imaging investigations in detecting and differentiating cardiac amyloidosis: A systematic review and meta-analysis. ESC Heart Fail. 2019, 6, 1041–1051. [Google Scholar] [CrossRef]
- Luigetti, M.; Romozzi, M.; Bisogni, G.; Cardellini, D.; Cavallaro, T.; Di Paolantonio, A.; Fabrizi, G.M.; Fenu, S.; Gentile, L.; Grandis, M.; et al. hATTR Pathology: Nerve Biopsy Results from Italian Referral Centers. Brain Sci. 2020, 10, 780. [Google Scholar] [CrossRef]
- Conceição, I.; González-Duarte, A.; Obici, L.; Schmidt, H.H.J.; Simoneau, D.; Ong, M.L.; Amass, L. Red-flag symptom clusters in transthyretin familial amyloid polyneuropathy. J. Peripher. Nerv. Syst. 2016, 21, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Leung, E.T.; Raboin, M.J.; McKelvey, J.; Graham, A.; Lewis, A.; Prongay, K.; Cohen, A.M.; Vinson, A. Modelling disease risk for amyloid A (AA) amyloidosis in non-human primates using machine learning. Amyloid 2019, 26, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Agibetov, A.; Seirer, B.; Dachs, T.-M.; Koschutnik, M.; Dalos, D.; Rettl, R.; Duca, F.; Schrutka, L.; Agis, H.; Kain, R.; et al. Machine Learning Enables Prediction of Cardiac Amyloidosis by Routine Laboratory Parameters: A Proof-of-Concept Study. J. Clin. Med. 2020, 9, 1334. [Google Scholar] [CrossRef]
- Martini, N.; Aimo, A.; Barison, A.; Della Latta, D.; Vergaro, G.; Aquaro, G.D.; Ripoli, A.; Emdin, M.; Chiappino, D. Deep learning to diagnose cardiac amyloidosis from cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2020, 22, 84. [Google Scholar] [CrossRef] [PubMed]
- Lipton, Z.C. The Mythos of Model Interpretability. Queue 2018, 16, 31–57. [Google Scholar] [CrossRef]
- Flaxman, A.D.; Vos, T. Machine learning in population health: Opportunities and threats. PLoS Med. 2018, 15, e1002702. [Google Scholar] [CrossRef]
- Saberi-Karimian, M.; Khorasanchi, Z.; Ghazizadeh, H.; Tayefi, M.; Saffar, S.; Ferns, G.A.; Ghayour-Mobarhan, M. Potential value and impact of data mining and machine learning in clinical diagnostics. Crit. Rev. Clin. Lab. Sci. 2021, 58, 275–296. [Google Scholar] [CrossRef] [PubMed]
- Amann, J.; Blasimme, A.; Vayena, E.; Frey, D.; Madai, V.I. Explainability for artificial intelligence in healthcare: A multidisciplinary perspective. BMC Med. Inform. Decis. Mak. 2020, 20, 310. [Google Scholar] [CrossRef]
- Friedman, J.H. Stochastic gradient boosting. Comput. Stat. Data Anal. 2002, 38, 367–378. [Google Scholar] [CrossRef]
- Hosni, M.; Abnane, I.; Idri, A.; de Gea, J.M.C.; Alemán, J.L.F. Reviewing ensemble classification methods in breast cancer. Comput. Methods Programs Biomed. 2019, 177, 89–112. [Google Scholar] [CrossRef] [PubMed]
- Shwartz-Ziv, R.; Armon, A. Tabular data: Deep learning is not all you need. Inf. Fusion 2021, 81, 84–90. [Google Scholar] [CrossRef]
- Liang, W.; Luo, S.; Zhao, G.; Wu, H. Predicting Hard Rock Pillar Stability Using GBDT, XGBoost, and LightGBM Algorithms. Mathematics 2020, 8, 765. [Google Scholar] [CrossRef]
- Li, H.; Cao, Y.; Li, S.; Zhao, J.; Sun, Y. XGBoost Model and Its Application to Personal Credit Evaluation. IEEE Intell. Syst. 2020, 35, 52–61. [Google Scholar] [CrossRef]
- Kotsiantis, S.B. Decision trees: A recent overview. Artif. Intell. Rev. 2013, 39, 261–283. [Google Scholar] [CrossRef]
- Lundberg, S.M.; Lee, S.I. A Unified Approach to Interpreting Model Predictions. Part of Advances in Neural Information Processing Systems. 2017. Available online: https://papers.nips.cc/paper/2017/hash/8a20a8621978632d76c43dfd28b67767-Abstract.html (accessed on 27 March 2022).
- Lundberg, S.M.; Erion, G.; Chen, H.; DeGrave, A.; Prutkin, J.M.; Nair, B.; Katz, R.; Himmelfarb, J.; Bansal, N.; Lee, S.-I. From local explanations to global understanding with explainable AI for trees. Nat. Mach. Intell. 2020, 2, 56–67. [Google Scholar] [CrossRef]
- Scheda, R.; Diciotti, S. Explanations of Machine Learning Models in Repeated Nested Cross-Validation: An Application in Age Prediction Using Brain Complexity Features. Appl. Sci. 2022, 12, 6681. [Google Scholar] [CrossRef]
- Wang, J.; Gribskov, M. IRESpy: An XGBoost model for prediction of internal ribosome entry sites. BMC Bioinform. 2019, 20, 409. [Google Scholar] [CrossRef] [PubMed]
- Alves, M.A.; de Castro, G.Z.; Oliveira, B.A.S.; Ferreira, L.A.; Ramírez, J.A.; Silva, R.; Guimarães, F.G. Explaining machine learning based diagnosis of COVID-19 from routine blood tests with decision trees and criteria graphs. Comput. Biol. Med. 2021, 132, 104335. [Google Scholar] [CrossRef] [PubMed]
- Grandis, M.; Obici, L.; Luigetti, M.; Briani, C.; Benedicenti, F.; Bisogni, G.; Canepa, M.; Cappelli, F.; Danesino, C.; Fabrizi, G.M.; et al. Recommendations for pre-symptomatic genetic testing for hereditary transthyretin amyloidosis in the era of effective therapy: A multicenter Italian consensus. Orphanet J. Rare Dis. 2020, 15, 348. [Google Scholar] [CrossRef]
- Jovanovic, M.; Schmitz, M. Explainability as a User Requirement for Artificial Intelligence Systems. Computer 2022, 55, 90–94. [Google Scholar] [CrossRef]
- Goodman, B.; Flaxman, S. European Union Regulations on Algorithmic Decision-Making and a “Right to Explanation”. AI Mag. 2017, 38, 50–57. [Google Scholar] [CrossRef]
- Di Stefano, V.; Thomas, E.; Giustino, V.; Iacono, S.; Torrente, A.; Pillitteri, G.; Gagliardo, A.; Lupica, A.; Palma, A.; Battaglia, G.; et al. Motor Conduction Studies and Handgrip in Hereditary TTR Amyloidosis: Simple Tools to Evaluate the Upper Limbs. Front. Neurol. 2022, 13, 835812. [Google Scholar] [CrossRef]
- Severi, D.; Aruta, F.; Iovino, A.; Spina, E.; Nolano, M.; Manganelli, F.; Tozza, S. Can we identify hereditary TTR amyloidosis by the screening of carpal tunnel syndrome patients? Neurol. Sci. 2022, 43, 3435–3438. [Google Scholar] [CrossRef] [PubMed]
- Atroshi, I.; Gummesson, C.; Johnsson, R.; Ornstein, E.; Ranstam, J.; Rosén, I. Prevalence of Carpal Tunnel Syndrome in a General Population. JAMA 1999, 282, 153–158. [Google Scholar] [CrossRef]
- Tozza, S.; Severi, D.; Spina, E.; Iovino, A.; Aruta, F.; Ruggiero, L.; Dubbioso, R.; Iodice, R.; Nolano, M.; Manganelli, F. The neuropathy in hereditary transthyretin amyloidosis: A narrative review. J. Peripher. Nerv. Syst. 2021, 26, 155–159. [Google Scholar] [CrossRef]
- Uncini, A.; Aretusi, G.; Manganelli, F.; Sekiguchi, Y.; Magy, L.; Tozza, S.; Tsuneyama, A.; Lefour, S.; Kuwabara, S.; Santoro, L.; et al. Electrodiagnostic accuracy in polyneuropathies: Supervised learning algorithms as a tool for practitioners. Neurol. Sci. 2020, 41, 3719–3727. [Google Scholar] [CrossRef]
- Wixner, J.; Mundayat, R.; Karayal, O.N.; Anan, I.; Karling, P.; Suhr, O.B.; on behalf of the THAOS investigators. THAOS: Gastrointestinal manifestations of transthyretin amyloidosis—Common complications of a rare disease. Orphanet J. Rare Dis. 2014, 9, 61. [Google Scholar] [CrossRef]
- Tashima, K.; Suhr, O.B.; Ando, Y.; Hölmgren, G.; Yamashita, T.; Obayashi, K.; Terazaki, H.; Uchino, M. Gastrointestinal dysfunction in familial amyloidotic polyneuropathy (ATTR Val30Met)—Comparison of Swedish and Japanese patients. Amyloid 1999, 6, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Di Stefano, V.; Thomas, E.; Alonge, P.; Giustino, V.; Pillitteri, G.; Leale, I.; Torrente, A.; Pignolo, A.; Norata, D.; Iacono, S.; et al. Patisiran Enhances Muscle Mass after Nine Months of Treatment in ATTRv Amyloidosis: A Study with Bioelectrical Impedance Analysis and Handgrip Strength. Biomedicines 2022, 11, 62. [Google Scholar] [CrossRef]
- Russo, M.; Gentile, L.; Toscano, A.; Vita, G.; Mazzeo, A. From a misdiagnosis of anorexia nervosa to a dramatic patisiran-induced improvement in a patient with ATTRE89Q amyloidosis. Amyloid 2020, 27, 279–280. [Google Scholar] [CrossRef]
- Ikeda, S.-I.; Makishita, H.; Oguchi, K.; Yanagisawa, N.; Nagata, T. Gastrointestinal amyloid deposition in familial amyloid polyneuropathy. Neurology 1982, 32, 1364. [Google Scholar] [CrossRef]
- Iida, T.; Yamano, H.; Nakase, H. Systemic amyloidosis with gastrointestinal involvement: Diagnosis from endoscopic and histological views. J. Gastroenterol. Hepatol. 2018, 33, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Maurer, M.S.; Schwartz, J.H.; Gundapaneni, B.; Elliott, P.M.; Merlini, G.; Waddington-Cruz, M.; Kristen, A.V.; Grogan, M.; Witteles, R.; Damy, T.; et al. Tafamidis Treatment for Patients with Transthyretin Amyloid Cardiomyopathy. N. Engl. J. Med. 2018, 379, 1007–1016. [Google Scholar] [CrossRef] [PubMed]
- Koike, H.; Katsuno, M. Transthyretin Amyloidosis: Update on the Clinical Spectrum, Pathogenesis, and Disease-Modifying Therapies. Neurol. Ther. 2020, 9, 317–333. [Google Scholar] [CrossRef] [PubMed]
- Luigetti, M.; Guglielmino, V.; Antonini, G.; Casali, C.; Ceccanti, M.; Chiappini, M.G.; De Giglio, L.; Di Lazzaro, V.; Di Muzio, A.; Goglia, M.; et al. ATTRv in Lazio-Italy: A High-Prevalence Region in a Non-Endemic Country. Genes 2021, 12, 829. [Google Scholar] [CrossRef] [PubMed]
- Oh, T.J.; Kang, S.; Lee, J.-E.; Moon, J.H.; Choi, S.H.; Lim, S.; Jang, H.C. Association between deterioration in muscle strength and peripheral neuropathy in people with diabetes. J. Diabetes Its Complicat. 2019, 33, 598–601. [Google Scholar] [CrossRef]
- Nanayakkara, N.; Curtis, A.J.; Heritier, S.; Gadowski, A.M.; Pavkov, M.E.; Kenealy, T.; Owens, D.R.; Thomas, R.L.; Song, S.; Wong, J.; et al. Impact of age at type 2 diabetes mellitus diagnosis on mortality and vascular complications: Systematic review and meta-analyses. Diabetologia 2021, 64, 275–287. [Google Scholar] [CrossRef] [PubMed]
- Yasemin, Ö.; Seydahmet, A.; Özcan, K. Relationship between diabetic neuropathy and sarcopenia. Prim. Care Diabetes 2019, 13, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Haase, J. Carpal tunnel syndrome—A comprehensive review. Adv. Tech. Stand. Neurosurg. 2007, 32, 175–249. [Google Scholar] [CrossRef]
- Tozza, S.; Severi, D.; Spina, E.; Di Paolantonio, A.; Iovino, A.; Guglielmino, V.; Aruta, F.; Nolano, M.; Sabatelli, M.; Santoro, L.; et al. A compound score to screen patients with hereditary transthyretin amyloidosis. J. Neurol. 2022, 269, 4281–4287. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Clinical Features | Screening-Positive ATTRv Patients (n = 93) | Screening-Negative Patients (n = 96) | p Value |
|---|---|---|---|
| Age (years) | 68 (32–87) | 69 (52–82) | 0.24 |
| Gender (males) | 72 (77%) | 70 (73%) | 0.29 |
| Bilateral carpal tunnel syndrome | 47 (51%) | 51 (53%) | 0.42 |
| Autonomic dysfunction | 47 (51%) | 50 (52%) | 0.47 |
| Ataxia | 45 (48%) | 46 (48%) | 0.53 |
| Unexplained weight loss | 42 (45%) | 30 (31%) | 0.034 * |
| Cardiomyopathy | 39 (42%) | 35 (36%) | 0.26 |
| Gastrointestinal disturbances | 34 (37%) | 40 (42%) | 0.28 |
| Lumbar canal stenosis | 19 (20%) | 28 (26%) | 0.11 |
| Diabetes | 7 (8%) | 24 (25%) | 0.001 * |
| Ocular disorders | 5 (5%) | 27 (28%) | <0.001 * |
| Renal dysfunction | 4 (4%) | 13 (14%) | 0.023 * |
| Autoimmunity | 2 (2%) | 21 (22%) | <0.001 * |
| TTR Mutations | |||
| Phe64Leu | 48 (52%) | - | - |
| Val30Met | 29 (31%) | - | - |
| Glu89Gln | 5 (5%) | - | - |
| Val122Ile | 3 (3%) | - | - |
| Others | 1 (8%) | - | - |
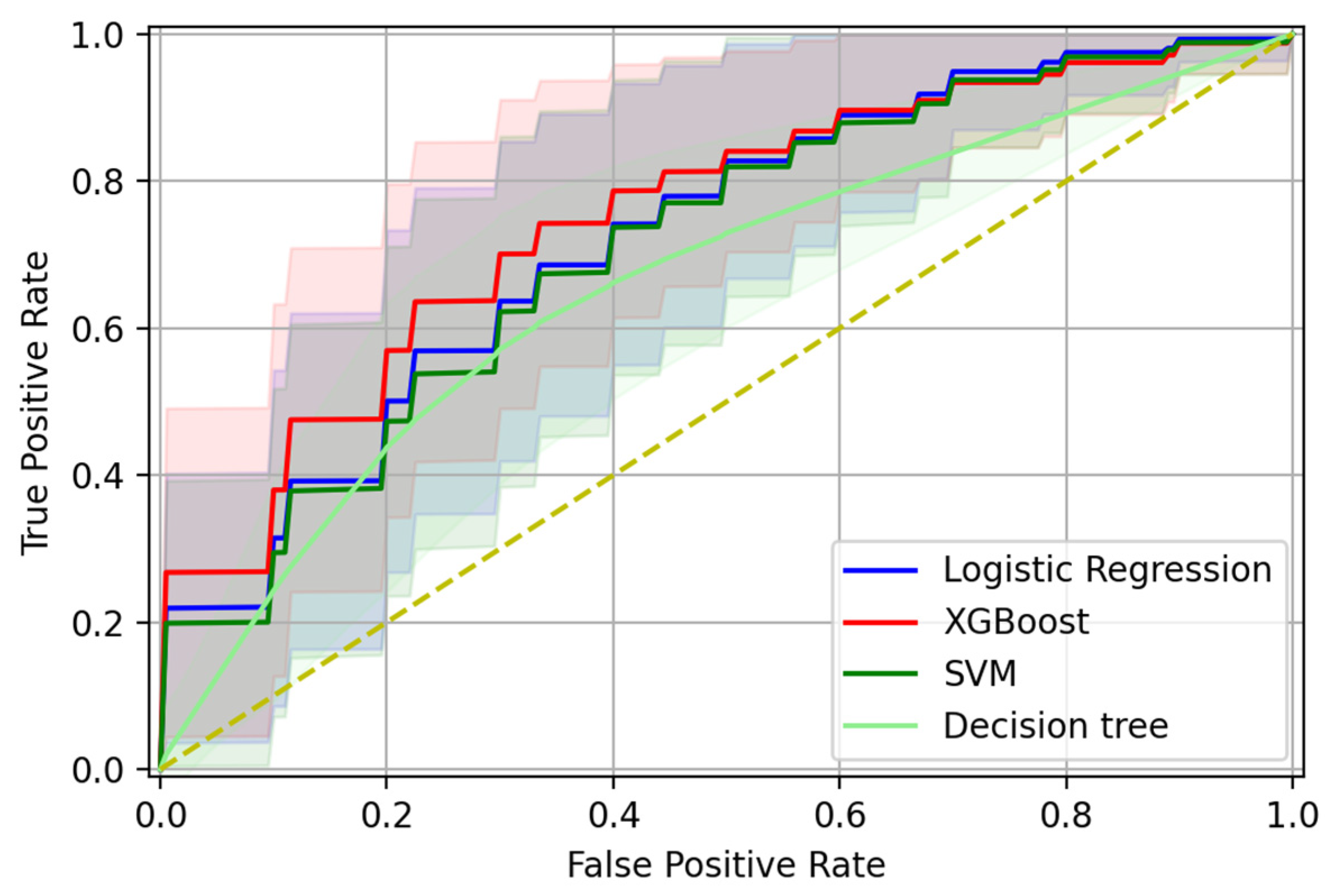
| Accuracy | AUC-ROC | Sensitivity | Specificity | PPV | NPV | |
|---|---|---|---|---|---|---|
| XGBoost | 0.707 ± 0.101 | 0.752 ± 0.107 | 0.712 ± 0.147 | 0.704 ± 0.150 | 0.711 ± 0.119 | 0.726 ± 0.118 |
| LR | 0.660 ± 0.099 | 0.725 ± 0.107 | 0.732 ± 0.135 | 0.592 ± 0.150 | 0.641 ± 0.102 | 0.703 ± 0.129 |
| SVM | 0.662 ± 0.099 | 0.713 ± 0.118 | 0.795 ± 0.165 | 0.534 ± 0.154 | 0.626 ± 0.095 | 0.749 ± 0.160 |
| DT | 0.656 ± 0.100 | 0.661 ± 0.101 | 0.644 ± 0.154 | 0.669 ± 0.143 | 0.660 ± 0.118 | 0.668 ± 0.114 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Stefano, V.; Prinzi, F.; Luigetti, M.; Russo, M.; Tozza, S.; Alonge, P.; Romano, A.; Sciarrone, M.A.; Vitali, F.; Mazzeo, A.; et al. Machine Learning for Early Diagnosis of ATTRv Amyloidosis in Non-Endemic Areas: A Multicenter Study from Italy. Brain Sci. 2023, 13, 805. https://doi.org/10.3390/brainsci13050805
Di Stefano V, Prinzi F, Luigetti M, Russo M, Tozza S, Alonge P, Romano A, Sciarrone MA, Vitali F, Mazzeo A, et al. Machine Learning for Early Diagnosis of ATTRv Amyloidosis in Non-Endemic Areas: A Multicenter Study from Italy. Brain Sciences. 2023; 13(5):805. https://doi.org/10.3390/brainsci13050805
Chicago/Turabian StyleDi Stefano, Vincenzo, Francesco Prinzi, Marco Luigetti, Massimo Russo, Stefano Tozza, Paolo Alonge, Angela Romano, Maria Ausilia Sciarrone, Francesca Vitali, Anna Mazzeo, and et al. 2023. "Machine Learning for Early Diagnosis of ATTRv Amyloidosis in Non-Endemic Areas: A Multicenter Study from Italy" Brain Sciences 13, no. 5: 805. https://doi.org/10.3390/brainsci13050805
APA StyleDi Stefano, V., Prinzi, F., Luigetti, M., Russo, M., Tozza, S., Alonge, P., Romano, A., Sciarrone, M. A., Vitali, F., Mazzeo, A., Gentile, L., Palumbo, G., Manganelli, F., Vitabile, S., & Brighina, F. (2023). Machine Learning for Early Diagnosis of ATTRv Amyloidosis in Non-Endemic Areas: A Multicenter Study from Italy. Brain Sciences, 13(5), 805. https://doi.org/10.3390/brainsci13050805