Exploring the Social Determinants of Health and Health Disparities in Traumatic Brain Injury: A Scoping Review


Abstract
1. Introduction
1.1. Social Determinants of Health
1.2. Health Disparities and TBI
1.3. Purpose of the Study
2. Materials and Methods
2.1. Review Approach
2.2. Identify Research Questions
2.3. Identify Relevant Studies
2.4. Inclusion and Exclusion Criteria
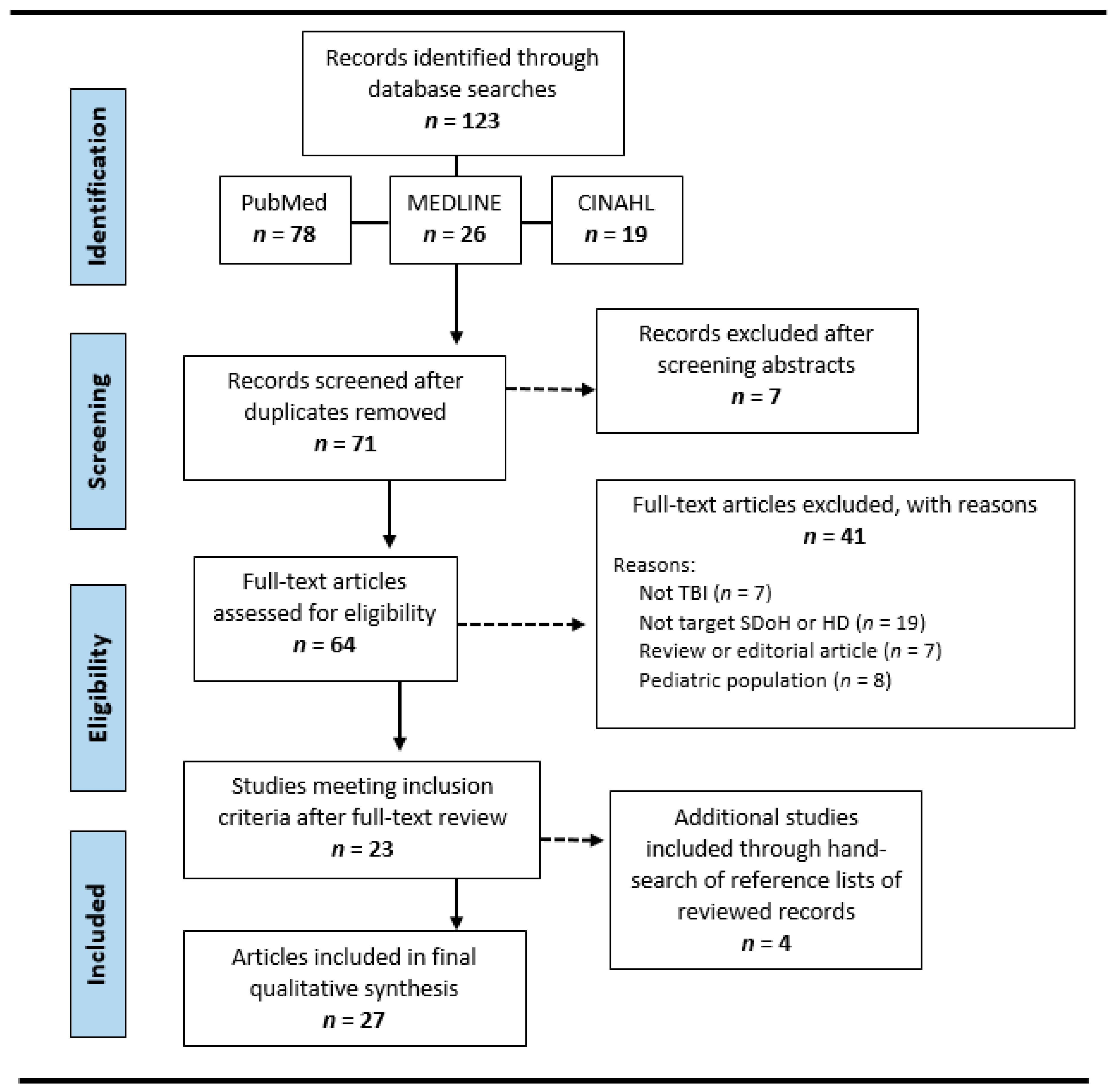
2.5. Study Selection Process
2.6. Data Extraction and Synthesis
3. Results
3.1. Description of Included Studies
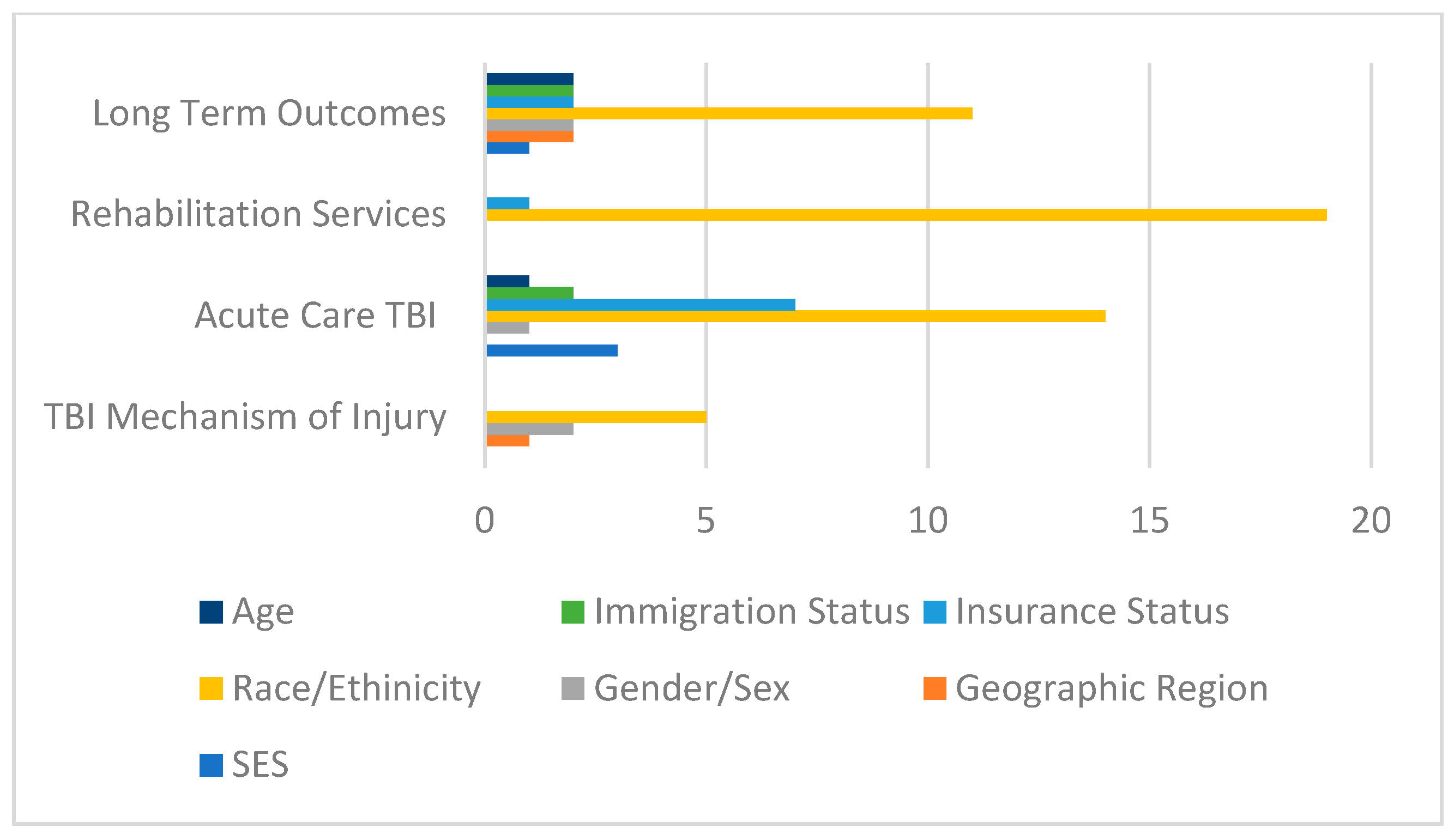
3.2. Social Determinants of Health Associated with TBI
3.3. Noted Health Disparities
4. Discussion
4.1. Which Social Determinants of Health Are Most Associated with TBI in Adults?
4.2. What Are the Most Common Health Disparities Associated with TBI in Adults?
4.3. Study Strengths and Limitations
4.4. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. TBI Mechanism of Injury
- Racial/ethnic minorities with an increased exposure to adverse childhood experiences have an increased risk of TBI [34].
- Race does not inform concussion nondisclosure in collegiate athletes [66].
- Racial/ethnic minorities more likely to sustain a TBI due to motor-pedestrian collisions [34].
- People living in remote areas have an increased risk of neurotrauma following an accident [62].
Appendix A.2. Acute TBI Care
- Racial/ethnic minorities are more likely to leave the emergency department before seeing a physician [34].
- Racial/ethnic minorities are more likely to receive testing for serum alcohol levels [85].
- Racial/ethnic minorities are more likely to experience complications during inpatient hospitalization [74].
- Racial/ethnic minorities were less likely to die in the hospital [85].
- People of color experience more severe injuries [56].
- Asians typically had the lowest injury severity at admission [82].
- Racial differences exist between White patients and patients of color on self-rated injury severity scales that are discordant with severity as measured by more objective markers [56].
- SES disparity is associated with inpatient mortality risk [85].
- SES disparity exists related to length of inpatient hospitalization [85].
- People from lower SES areas had an increased chance of being hospitalized for intracranial injury [88].
- Publicly insured patients have higher odds of undergoing surgical management for traumatic SDH compared to self-pay patients [63].
- A higher percentage of self-pay TBI patients die in the hospital [63].
- Medicare patients are less likely to undergo craniectomy [63].
- There is no association between in-hospital mortality rate and immigrant documentation status [68].
- Undocumented immigrants had a longer average hospital length of stay [68].
- Older patients are less likely to undergo craniectomy [75].
- Females are less likely to undergo craniectomy [75].
- Women receive different inpatient care depending on age and severity of TBI [60].
Appendix A.3. TBI Rehabilitation Services
- Racial/ethnic minorities are more likely to receive fewer rehabilitation minutes [34].
- Racial/ethnic minorities have a higher likelihood of early discharge from rehabilitation [34].
- Hispanic patients with comparable injury severity and insurance status receive different discharge dispositions post-TBI, even in regions in which Hispanics are the demographic majority [55].
- White patients are admitted to acute rehabilitation significantly faster than people of color [56].
- Hispanic ethnicity was associated with a greater odd of discharge to home [71].
- People of color had lower admission and discharge FIM scores [71].
- Asian patients at Trauma Level 1 hospitals were more likely to be discharged to acute rehabilitation if they had private versus public insurance [57].
Appendix A.4. Long-Term TBI Outcomes
- Whites more likely to receive palliative care encounters than Black and Hispanic patients [67].
- Whites more likely to refuse PEG placement after a palliative care consult [67].
- After controlling for covariates, Blacks had a greater rate of depression than Whites, and similar rate as Hispanics [81].
- Blacks had lower life satisfaction rates over time compared to Whites [81].
- Racial/ethnic minorities more likely to report higher levels of caregiver burden after TBI [81].
- Blacks were more likely to report more challenges coping with depression [81].
- Racial/ethnic minorities more likely to experience long-term adverse outcomes [34].
- Black patients with private insurance and Black patients with public insurance had poorer outcomes than privately insured White patients [75].
- Hispanics with TBI showed greater participation than non-Hispanic Whites in the area of being out and about in the community 1-year post-injury [64].
- Asians failed to make similar improvements as noted in Hispanics and Whites between rehabilitation discharge and 1 year post-TBI follow-up [82].
- Race was not a significant predictor of outcome or mortality [71].
- Sex was not a significant predictor of outcome or mortality [61].
- There are gender differences related to self-reported post-concussion syndrome symptoms, which are likely based in anxiety sensitivity [53].
- Older patients are more likely to have poorer outcomes [81].
- Age was not a significant predictor of outcome or mortality [61].
- SES was not a significant predictor of outcome or mortality [61].
- Nativity, moderated by the residential proportion of foreign language speakers, predicted productive activity 1-year post TBI [59].
- Indigenous populations of Canada faced inadequate resources, social problems, and challenges within the health care system [62].
- Lack of health insurance was significantly associated with decreased use of post-hospital healthcare services [36].
- Medicare and Medicaid patients of all race categories had poorer outcomes than privately insured White patients [81].
- People with TBI living in more rural areas traveled significantly further to access post-discharge health services and had decreased amounts of follow-up healthcare appointments [58].
- Countries with a high incidence of TBI has disproportionately higher research publications compared to countries with lower TBI populations [65].
References
- Dewan, M.C.; Rattani, A.; Gupta, S.; Baticulon, R.E.; Hung, Y.C.; Punchak, M.; Agrawal, A.; Adeleye, A.O.; Shrime, M.G.; Rubiano, A.M.; et al. Estimating the global incidence of traumatic brain injury. J. Neurosurg. 2019, 130, 1080–1097. [Google Scholar] [CrossRef] [PubMed]
- Capizzi, A.; Woo, J.; Verduzco-Gutierrez, M. Traumatic brain injury. Med. Clin. N. Am. 2020, 104, 213–238. [Google Scholar] [CrossRef]
- Maas, A.I.R.; Menon, D.K.; Adelson, P.D.; Andelic, N.; Bell, M.J.; Belli, A.; Bragge, P.; Brazinova, A.; Büki, A.; Chesnut, R.M.; et al. InTBIR participants and investigators. Traumatic brain injury: Integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 2017, 16, 987–1048. [Google Scholar] [CrossRef]
- Ng, S.Y.; Lee, A.Y. Traumatic brain injuries: Pathophysiology and potential therapeutic targets. Front. Cell. Neurosci. 2019, 13, 528. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. 21 March 2022. Available online: https://www.cdc.gov/traumaticbraininjury/data/index.html (accessed on 21 March 2023).
- Rosenfeld, J.V.; Maas, A.I.; Bragge, P.; Morganti-Kossmann, M.C.; Manley, G.T.; Gruen, R.L. Early management of severe traumatic brain injury. Lancet 2012, 380, 1088–1098. [Google Scholar] [CrossRef]
- Braveman, P.; Egerter, S.; Williams, D.R. The social determinants of health: Coming of age. Annu. Rev. Public Health 2011, 32, 381–398. [Google Scholar] [CrossRef]
- Osmick, M.J.; Wilson, M. Social Determinants of health—Relevant history, a call to action, an organization’s transformational story, and what can employers do? Am. J. Health Promot. 2020, 34, 219–224. [Google Scholar] [CrossRef]
- Braveman, P. What are Health Disparities and health equity? We need to be clear. Public Health Rep. 2014, 129, 5–8. [Google Scholar] [CrossRef]
- Braveman, P.; Gottlieb, L. The social determinants of health: It’s time to consider the causes of the causes. Public Health Rep. 2014, 129, 19–31. [Google Scholar] [CrossRef]
- Chan, V.; Marcus, L.; Burlie, D.; Mann, R.E.; Toccalino, D.; Cusimano, M.D.; Ilie, G.; Colantonio, A. Social determinants of health associated with psychological distress stratified by lifetime traumatic brain injury status and sex: Cross-sectional evidence from a population sample of adults in Ontario, Canada. PLoS ONE 2022, 17, e0273072. [Google Scholar] [CrossRef]
- Islam, M.M. Social determinants of health and related inequalities: Confusion and implications. Front. Public Health 2019, 7, 11. [Google Scholar] [CrossRef] [PubMed]
- Osypuk, T.L.; Joshi, P.; Geronimo, K.; Acevedo-Garcia, D. Do social and economic policies influence health? A review. Curr. Epidemiol. Rep. 2014, 1, 149–164. [Google Scholar] [CrossRef]
- Banks, A.R.; Bell, B.A.; Ngendahimana, D.; Embaye, M.; Freedman, D.A.; Chisolm, D.J. Identification of factors related to food insecurity and the implications for social determinants of health screenings. BMC Public Health 2021, 21, 1410. [Google Scholar] [CrossRef]
- Towne, S.D.; Liu, X.; Li, R.; Smith, M.L.; Maddock, J.E.; Tan, A.; Hayek, S.; Zelber-Sagi, S.; Jiang, X.; Ruan, H.; et al. Social and structural determinants of health inequities: Socioeconomic, transportation-related, and provincial-level indicators of cost-related Forgone Hospital Care in China. Int. J. Environ. Res. Public Health 2021, 18, 6113. [Google Scholar] [CrossRef]
- Marmot, M.; Friel, S.; Bell, R.; Houweling, T.A.J.; Taylor, S. Closing the gap in a generation: Health equity through action on the social determinants of health. Lancet 2008, 372, 1661–1669. [Google Scholar] [CrossRef] [PubMed]
- Weida, E.B.; Phojanakong, P.; Patel, F.; Chilton, M. Financial health as a measurable social determinant of health. PLoS ONE 2020, 15, e0233359. [Google Scholar] [CrossRef]
- Andermann, A.; CLEAR Collaboration. Taking action on the social determinants of health in clinical practice: A framework for health professionals. Can. Med. Assoc. J. 2016, 188, E474–E483. [Google Scholar] [CrossRef]
- Protheroe, J.; Nutbeam, D.; Rowlands, G. Health literacy: A necessity for increasing participation in health care. Br. J. Gen. Pract. 2009, 59, 721–723. [Google Scholar] [CrossRef]
- Healthy People 2030. Available online: https://health.gov/healthypeople (accessed on 23 March 2023).
- Gulati, R.K.; Hur, K. Association between limited English proficiency and healthcare access and utilization in California. J. Immigr. Minor. Health 2021, 24, 95–101. [Google Scholar] [CrossRef]
- Al Shamsi, H.; Almutairi, A.G.; Al Mashrafi, S.; Al Kalbani, T. Implications of language barriers for healthcare: A systematic review. Oman. Med. J. 2020, 35, e122. [Google Scholar] [CrossRef] [PubMed]
- Schillinger, D. The intersections between social determinants of health, health literacy, and health disparities. Stud. Health Technol. Inform. 2020, 269, 22–41. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. 3 February 2023. Available online: https://www.cdc.gov/traumaticbraininjury/health-disparities-tbi.html (accessed on 21 March 2023).
- Adler, N.E.; Glymour, M.M.; Fielding, J. Addressing social determinants of health and health inequalities. JAMA 2016, 316, 1641. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. 24 November 2020. Available online: https://www.cdc.gov/healthyyouth/disparities/index.htm (accessed on 21 March 2023).
- NIH (National Institutes of Health). Health Disparities. 2018. Available online: http://www.nhlbi.nih.gov/health/educational/healthdisp (accessed on 21 March 2023).
- Primary Care Collaborative. (n.d.). Available online: https://www.pcpcc.org/topic-page/health-disparities (accessed on 23 March 2023).
- Lee, H.; Kim, D.; Lee, S.A.; Fawcett, J. The concepts of health inequality, disparities and equity in the era of population health. Appl. Nurs. Res. 2020, 56, 151367. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, J.N.; Geller, A.; Negussie, Y.; Baciu, A. Communities in Action: Pathways to Health Equity; National Academies Press (US): Washington, DC, USA, 2017. [Google Scholar]
- Havranek, E.P.; Mujahid, M.S.; Barr, D.A.; Blair, I.V.; Cohen, M.S.; Cruz-Flores, S.; Davey-Smith, G.; Dennison-Himmelfarb, C.R.; Lauer, M.S.; Lockwood, D.W.; et al. Social determinants of risk and outcomes for cardiovascular disease. Circ. J. 2015, 132, 873–898. [Google Scholar] [CrossRef]
- Pinheiro, L.C.; Reshetnyak, E.; Akinyemiju, T.; Phillips, E.; Safford, M.M. Social determinants of health and cancer mortality in the reasons for geographic and racial differences in stroke (REGARDS) cohort study. Cancer 2022, 128, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Reshetnyak, E.; Ntamatungiro, M.; Pinheiro, L.C.; Howard, V.J.; Carson, A.P.; Martin, K.D.; Safford, M.M. Impact of multiple social determinants of health on incident stroke. Stroke 2020, 51, 2445–2453. [Google Scholar] [CrossRef]
- Saadi, A.; Bannon, S.; Watson, E.; Vranceanu, A.M. Racial and ethnic disparities associated with traumatic brain injury across the continuum of care: A narrative review and directions for future research. J. Racial. Ethn. Health Disparities 2021, 9, 786–799. [Google Scholar] [CrossRef]
- Barthelemy, E.R.; Affana, C.K.; Asfaw, Z.K.; Dams-O′Connor, K.; Rahman, J.; Jones, S.; Ullman, J.; Margetis, K.; Hickman, Z.L.; Dangayach, N.S.; et al. Racial and socioeconomic disparities in neurotrauma: Research priorities in the New York metropolitan area through a global neurosurgery paradigm. World Neurosurg. 2022, 165, 51–57. [Google Scholar] [CrossRef]
- Gao, S.; Kumar, R.G.; Wisniewski, S.R.; Fabio, A. Disparities in health care utilization of adults with traumatic brain injuries are related to insurance, race, and ethnicity: A systematic review. J. Head Trauma Rehabil. 2018, 33, E40–E50. [Google Scholar] [CrossRef]
- Mukhtarzada, M.G.; Monteith, T.S. Equity and disparities in diagnosis, management, and research of post-traumatic headache. Curr. Pain Headache Rep. 2022, 26, 555–566. [Google Scholar] [CrossRef]
- Burnett, D.M.; Kolakowsky-Hayner, S.A.; Slater, D.; Stringer, A.; Bushnik, T.; Zafonte, R.; Cifu, D.X. Ethnographic analysis of traumatic brain injury patients in the national model systems database. Arch. Phys. Med. Rehabil. 2003, 84, 263–267. [Google Scholar] [CrossRef] [PubMed]
- Alban, R.F.; Berry, C.; Ley, E.; Mirocha, J.; Margulies, D.R.; Tillou, A.; Salim, A. Does health care insurance affect outcomes after traumatic brain injury? analysis of the National Trauma Databank. Am. Surg. 2010, 76, 1108–1111. [Google Scholar] [CrossRef] [PubMed]
- Gardizi, E.; Hanks, R.A.; Millis, S.R.; Figueroa, M.J. Comorbidity and insurance as predictors of disability after traumatic brain injury. Arch. Phys. Med. Rehabil. 2014, 95, 2396–2401. [Google Scholar] [CrossRef] [PubMed]
- Dall, T.M.; Storm, M.V.; Chakrabarti, R.; Drogan, O.; Keran, C.M.; Donofrio, P.D.; Henderson, V.W.; Kaminski, H.J.; Stevens, J.C.; Vidic, T.R. Supply and demand analysis of the current and future US neurology workforce. Neurology 2013, 81, 470–478. [Google Scholar] [CrossRef] [PubMed]
- Mauser, E.D.; Rosen, N.L. So many migraines, so few subspecialists: Analysis of the geographic location of United Council for Neurologic subspecialties (UCNS) certified headache subspecialists compared to United States headache demographics. J. Headache Pain 2014, 54, 1347–1357. [Google Scholar] [CrossRef]
- Johnson, L.W.; Hall, K.D. A scoping review of cognitive assessment in adults with acute traumatic brain injury. Am. J. Speech Lang. Pathol. 2021, 31, 739–756. [Google Scholar] [CrossRef]
- Byom, L.; O′Neil-Pirozzi, T.M.; Lemoncello, R.; MacDonald, S.; Meulenbroek, P.; Ness, B. Social communication following adult traumatic brain injury: A scoping review of theoretical models. Am. J. Speech Lang. Pathol. 2020, 2, 1735–1748. [Google Scholar]
- Iverson, G.L.; Karr, J.E.; Gardner, A.J.; Silverberg, N.D.; Terry, D.P. Results of scoping review do not support mild traumatic brain injury being associated with a high incidence of chronic cognitive impairment: Commentary on McInnes et al. 2017. PLoS ONE 2019, 14, e0218997. [Google Scholar] [CrossRef]
- Patterson, F.; Fleming, J.; Doig, E. Group-based delivery of interventions in traumatic brain injury rehabilitation: A scoping review. Disabil. Rehabil. 2016, 38, 1961–1986. [Google Scholar] [CrossRef]
- Arksey, H.; O′Malley, L. Scoping Studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. Theory Pract. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Colquhoun, H.L.; Levac, D.; O′Brien, K.K.; Straus, S.; Tricco, A.C.; Perrier, L.; Kastner, M.; Moher, D. Scoping reviews: Time for clarity in definition, methods, and reporting. J. Clin. Epidemiol. 2014, 67, 1291–1294. [Google Scholar] [CrossRef] [PubMed]
- Levac, D.; Colquhoun, H.; O′Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O′Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Nowell, L.; Alix Hayden, K.; Berenson, C.; Kenny, N.; Chick, N.; Emery, C. Professional learning and development of postdoctoral scholars: A scoping review protocol. Syst. Rev. 2018, 7, 224. [Google Scholar] [CrossRef]
- Shoreland, J.; Douglas, J.; O′Halloran, R. Cognitive-communication difficulties following traumatic brain injury sustained in older adulthood: A scoping review. Int. J. Lang. Commun. Disord. 2020, 55, 821–835. [Google Scholar] [CrossRef] [PubMed]
- Albanese, B.J.; Boffa, J.W.; Macatee, R.J.; Schmidt, N.B. Anxiety sensitivity mediates gender differences in post-concussive symptoms in a clinical sample. Psychiatry Res. 2017, 252, 242–246. [Google Scholar] [CrossRef]
- Anto-Ocrah, M.; Aboagye, R.G.; Hasman, L.; Ghanem, A.; Owusu-Agyei, S.; Buranosky, R. The elephant in the room: Intimate partner violence, women, and traumatic brain injury in sub-Saharan Africa. Front. Neurol. 2022, 13, 197967. [Google Scholar] [CrossRef]
- Budnick, H.C.; Tyroch, A.H.; Milan, S.A. Ethnic disparities in traumatic brain injury care referral in a hispanic-majority population. J. Surg. Res. 2017, 215, 231–238. [Google Scholar] [CrossRef]
- Fuentes, A.; Schoen, C.; Kulzer, R.R.; Long, C.; Bushnik, T.; Rath, J.F. Impact of racial-ethnic minority status and systemic vulnerabilities on time to acute TBI rehabilitation admission in an urban public hospital setting. Rehabil. Psychol. 2019, 64, 229–236. [Google Scholar] [CrossRef]
- Gorman, E.; Frangos, S.; DiMaggio, C.; Bukur, M.; Klein, M.; Pachter, H.L.; Berry, C. Is trauma center designation associated with disparities in discharge to rehabilitation centers among elderly patients with traumatic brain injury? Am. J. Surg. 2020, 219, 587–591. [Google Scholar] [CrossRef]
- Keeves, J.; Gabbe, B.; Arnup, S.; Ekegren, C.; Beck, B. Serious injury in metropolitan and regional victoria: Exploring travel to treatment and utilisation of post-discharge health services by injury type. Int. J. Environ. Res. Public Health 2022, 19, 14063. [Google Scholar] [CrossRef] [PubMed]
- Lequerica, A.H.; Botticello, A.; O’Neill, J.; Lengenfelder, J.; Krch, D.; Chiaravalloti, N.D.; Sander, A.M.; Bushnik, T.; Ketchum, J.M.; Hammond, F.M.; et al. Relationship between hispanic nativity, residential environment, and productive activity among individuals with traumatic brain injury: A TBI model systems study. J. Head Trauma Rehabil. 2019, 34, E46–E54. [Google Scholar] [CrossRef] [PubMed]
- Mikolić, A.; van Klaveren, D.; Groeniger, J.O.; Wiegers, E.J.A.; Lingsma, H.F.; Zeldovich, M.; von Steinbüchel, N.; Maas, A.I.R.; Roeters van Lennep, J.E.; Polinder, S.; et al. Differences between men and women in treatment and outcome after traumatic brain injury. J. Neurotrauma 2021, 38, 235–251. [Google Scholar] [CrossRef]
- Rolle, M.L.; McLellan, R.M.; Nanda, P.; Patel, A.B.; Sacks, C.A.; Masiakos, P.T.; Stapleton, C.J. Racial and social determinants of civilian gunshot wounds to the head. Neurohospitalist 2022, 12, 444–452. [Google Scholar] [CrossRef] [PubMed]
- Salaheen, Z.; Moghaddamjou, A.; Fehlings, M. Neurotrauma in indigenous populations of Canada—challenges and opportunities at a global level: A scoping review. World Neurosurg. 2022, 167, 213–221.e2. [Google Scholar] [CrossRef]
- Sullivan, J.E.; Panjwani, S.; Cahan, M.A. Influence of insurance status on subdural hematoma management: A national trauma data bank analysis. J. Surg. Res. 2022, 270, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Stevens, L.F.; Ketchum, J.M.; Sander, A.M.; Callender, L.; Dillahunt-Aspillaga, C.; Dreer, L.E.; Finn, J.A.; Gary, K.W.; Graham, K.M.; Juengst, S.B.; et al. Race/ethnicity and community participation among veterans and service members with Traumatic Brain Injury: A VA traumatic brain injury model systems study. J. Head Trauma Rehabil. 2021, 36, 408–417. [Google Scholar] [CrossRef]
- Tropeano, M.P.; Spaggiari, R.; Ileyassoff, H.; Park, K.B.; Kolias, A.G.; Hutchinson, P.J.; Servadei, F. A comparison of publication to TBI burden ratio of low- and middle-income countries versus high-income countries: How can we improve worldwide care of TBI? Neurosurg. Focus 2019, 47, E5. [Google Scholar] [CrossRef]
- Wallace, J.; Covassin, T.; Moran, R.; Deitrick, J.M. Factors contributing to disparities in baseline neurocognitive performance and concussion symptom scores between black and white collegiate athletes. J. Racial Ethn. Health Disparities 2018, 5, 894–900. [Google Scholar] [CrossRef]
- Williamson, T.L.; Adil, S.M.; Shalita, C.; Charalambous, L.T.; Mitchell, T.; Yang, Z.; Parente, B.A.; Lee, H.; Ubel, P.A.; Lemmon, M.E.; et al. Palliative care consultations in patients with severe traumatic brain injury: Who receives palliative care consultations and what does that mean for utilization? Neurocrit. Care 2022, 36, 781–790. [Google Scholar] [CrossRef]
- Wyrick, J.M.; Kalosza, B.A.; Coritsidis, G.N.; Tse, R.; Agriantonis, G. Trauma care in a multiethnic population: Effects of being undocumented. J. Surg. Res. 2017, 214, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Cheng, T.L.; Johnson, S.B.; Goodman, E. Breaking the intergenerational cycle of disadvantage: The three generation approach. Pediatrics 2016, 137, e20152467. [Google Scholar] [CrossRef] [PubMed]
- Smeeding, T.M. Multiple barriers to economic opportunity for the “truly” disadvantaged and vulnerable. Russell Sage Found. J. Soc. Sci. RSF 2016, 2, 98–122. [Google Scholar] [CrossRef]
- Warren, K.L.; García, J.J. Centering race/ethnicity: Differences in traumatic brain injury inpatient rehabilitation outcomes. PM&R 2022, 14, 1430–1438. [Google Scholar]
- Churchwell, K.; Elkind, M.S.V.; Benjamin, R.M.; Carson, A.P.; Chang, E.K.; Lawrence, W.; Mills, A.; Odom, T.M.; Rodriguez, C.J.; Rodriguez, F.; et al. Call to action: Structural racism as a fundamental driver of health disparities: A presidential advisory from the American Heart Association. Circ. J. 2020, 142, e454–e468. [Google Scholar] [CrossRef]
- Gee, G.C.; Ford, C.L. Structural racism and health inequities: Old issues, new directions. Du. Bois. Rev. 2011, 8, 115–132. [Google Scholar] [CrossRef]
- McQuistion, K.; Zens, T.; Jung, H.; Beems, M.; Leverson, G.; Liepert, A.; Scarborough, J.; Agarwal, S. Insurance status and race affect treatment and outcome of traumatic brain injury. J. Surg. Res. 2016, 205, 261–271. [Google Scholar] [CrossRef]
- Reilly, A.S.; Khawaja, A.M.; Ali, A.B.; Madsen, T.; Molino-Bacic, J.; Heffernan, D.S.; Zonfrillo, M.R.; Vaitkevicius, H.; Gormley, W.B.; Izzy, S.; et al. Disparities in decompressive cranial surgery utilization in severe traumatic brain injury patients without a primary extra-axial hematoma: A U.S. nationwide study. World Neurosurg. 2023, 169, e16–e28. [Google Scholar] [CrossRef]
- Richie, E.A.; Nugent, J.G.; Raslan, A.M. Racial and ethnic inequities in mortality during hospitalization for traumatic brain injury: A call to action. Front. Surg. 2021, 8, 690971. [Google Scholar] [CrossRef]
- Owens, A.; Holroyd, B.R.; McLane, P. Patient race, ethnicity, and care in the emergency department: A scoping review. CJEM 2020, 22, 245–253. [Google Scholar] [CrossRef]
- Berwick, D.M.; Bowman, K.; Matney, C. Traumatic Brain Injury: A Roadmap for Accelerating Progress; National Academies Press: Washington, DC, USA, 2022. [Google Scholar]
- Asemota, A.O.; George, B.P.; Cumpsty-Fowler, C.J.; Haider, A.H.; Schneider, E.B. Race and insurance disparities in discharge to rehabilitation for patients with traumatic brain injury. J. Neurotrauma 2013, 30, 2057–2065. [Google Scholar] [CrossRef] [PubMed]
- Shafi, S.; de la Marquez Plata, C.; Diaz-Arrastia, R.; Shipman, K.; Carlile, M.; Frankel, H.; Parks, J.; Gentilello, L.M. Racial disparities in long-term functional outcome after traumatic brain injury. J. Loss. Trauma 2007, 63, 1263–1270. [Google Scholar] [CrossRef] [PubMed]
- Odonkor, C.A.; Esparza, R.; Flores, L.E.; Verduzco-Gutierrez, M.; Escalon, M.X.; Solinsky, R.; Silver, J.K. Disparities in health care for black patients in physical medicine and rehabilitation in the united states: A narrative review. PM&R 2021, 13, 180–203. [Google Scholar]
- Kuerban, A.; Dams-O′Connor, K. Effect of race and nativity on functional outcomes following traumatic brain injury among asian, hispanic, and non-hispanic white survivors in the united states: A NIDILRR TBI model systems study. J. Head Trauma Rehabil. 2022, 37, E310–E318. [Google Scholar] [CrossRef]
- Englum, B.R.; Hui, X.; Zogg, C.K.; Chaudhary, M.A.; Villegas, C.; Bolorunduro, O.B.; Stevens, K.A.; Haut, E.R.; Cornwell, E.E.; Efron, D.T.; et al. Association between insurance status and hospital length of stay following trauma. Am. Surg. 2016, 82, 281–288. [Google Scholar] [CrossRef]
- Missios, S.; Bekelis, K. The association of insurance status and race with the procedural volume of traumatic brain injury patients. Injury 2016, 47, 154–159. [Google Scholar] [CrossRef]
- Haines, K.L.; Nguyen, B.P.; Vatsaas, C.; Alger, A.; Brooks, K.; Agarwal, S.K. Socioeconomic status affects outcomes after severity-stratified traumatic brain injury. J. Surg. Res. 2019, 235, 131–140. [Google Scholar] [CrossRef]
- Bruns, J., Jr.; Hauser, W.A. The epidemiology of traumatic brain injury: A review. Epilepsia 2003, 44, 2–10. [Google Scholar] [CrossRef]
- Kraus, J.F.; Fife, D.; Ramstein, K.; Conroy, C.; Cox, P. The relationship of family income to the incidence, external causes, and outcomes of serious brain injury, San Diego County, California. Am. J. Public Health 1986, 76, 1345–1347. [Google Scholar] [CrossRef]
- Park, H.A.; Vaca, F.E.; Jung-Choi, K.; Park, H.; Park, J.O. Area-level socioeconomic inequalities in intracranial injury-related hospitalization in Korea: A retrospective analysis of data from Korea national hospital discharge survey 2008–2015. J. Korean Med. Sci. 2023, 38, e38. [Google Scholar] [CrossRef]
- Daugherty, J.; Sarmiento, K.; Waltzman, D.; Xu, L. Traumatic brain injury–related hospitalizations and deaths in urban and rural counties—2017. Ann. Emerg. Med. 2022, 79, 288–296.e1. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.C.; Chiu, W.T.; Yeh, C.C.; Chang, H.C.; Chen, T.L. Risk and outcomes for traumatic brain injury in patients with mental disorders. J. Neurol. Neurosurg. Psychiatry 2012, 83, 1186–1192. [Google Scholar] [CrossRef] [PubMed]
- Nordström, A.; Edin, B.B.; Lindström, S.; Nordström, P. Cognitive function and other risk factors for mild traumatic brain injury in young men: Nationwide cohort study. BMJ 2013, 346, f723. [Google Scholar] [CrossRef] [PubMed]
- Gugushvili, A.; Bulczak, G.; Zelinska, O.; Koltai, J. Socioeconomic position, social mobility, and health selection effects on allostatic load in the United States. PLoS ONE 2021, 16, e0254414. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Domain | Key Words in the Title or Abstract | MeSH Terms |
|---|---|---|
| Brain Injury | brain OR injury OR “brain injury” OR “brain injuries” OR “traumatic brain injury” | brain injury OR traumatic brain injury OR TBI |
| Social Determinants of Health | “social determinants of health” OR “determinants of health” OR “health determinants” | social determinants of health OR SDOH OR health determinants OR healthcare determinants |
| Health Disparity | “health disparity” OR “health disparities” OR “health equity” OR ‘health inequity’ | health dispar OR health equity |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Johnson, L.W.; Diaz, I. Exploring the Social Determinants of Health and Health Disparities in Traumatic Brain Injury: A Scoping Review. Brain Sci. 2023, 13, 707. https://doi.org/10.3390/brainsci13050707
Johnson LW, Diaz I. Exploring the Social Determinants of Health and Health Disparities in Traumatic Brain Injury: A Scoping Review. Brain Sciences. 2023; 13(5):707. https://doi.org/10.3390/brainsci13050707
Chicago/Turabian StyleJohnson, Leslie W., and Isabella Diaz. 2023. "Exploring the Social Determinants of Health and Health Disparities in Traumatic Brain Injury: A Scoping Review" Brain Sciences 13, no. 5: 707. https://doi.org/10.3390/brainsci13050707
APA StyleJohnson, L. W., & Diaz, I. (2023). Exploring the Social Determinants of Health and Health Disparities in Traumatic Brain Injury: A Scoping Review. Brain Sciences, 13(5), 707. https://doi.org/10.3390/brainsci13050707