

Aberrant Resting-State Functional Connectivity in MDD and the Antidepressant Treatment Effect—A 6-Month Follow-Up Study
Abstract
1. Introduction
2. Methods
2.1. Participants and Clinical Characteristics
2.2. Study Design
2.3. MRI Data Acquisition, Preprocessing and Network Construction
2.4. Network-Based Statistics Analysis
2.5. Overlap of Functional Connectivity Sub-Network
2.6. Statistic Analysis
2.7. Visualization of the Network Anatomy
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Characteristics of rsFC in Patients with Acute MDD
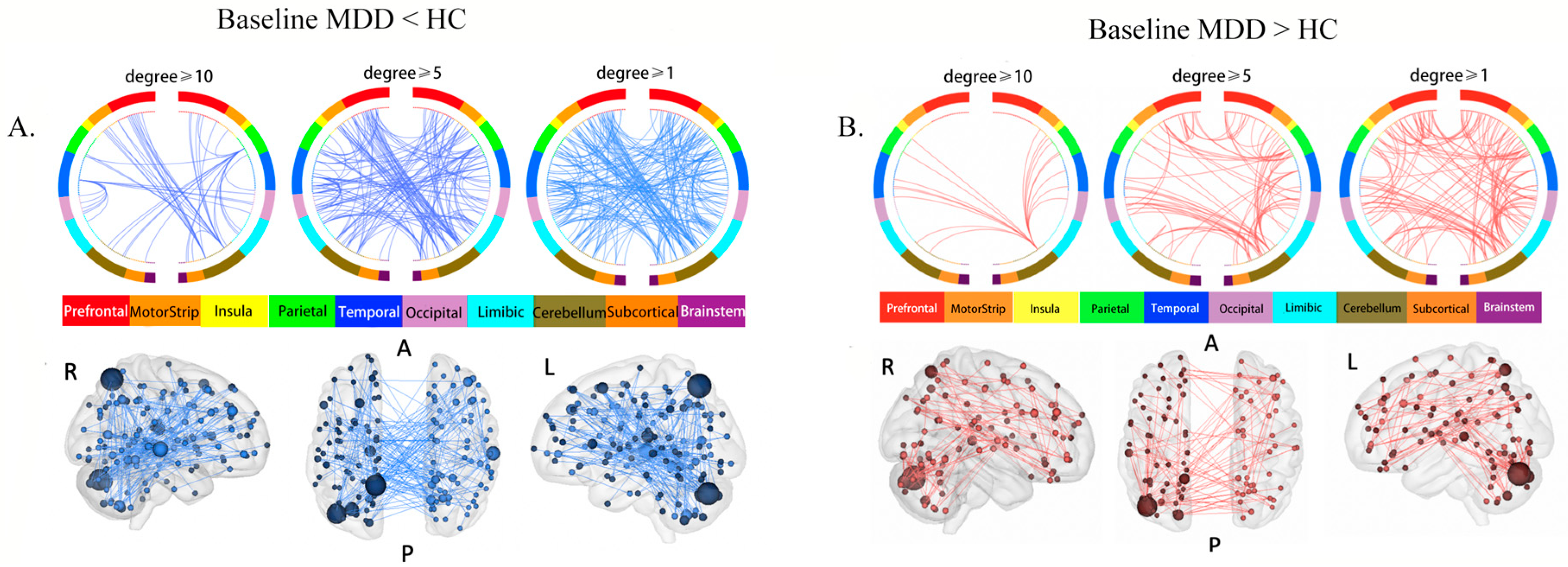
3.2.1. Comparison of rsFC between Baseline MDD and HCs
3.2.2. Changes in Aberrant rsFC after 6-Month Treatment
3.2.3. State-Dependence of the Aberrant rsFC
3.3. Changes in rsFC before and after Treatment in Patients with MDD
3.4. The Overlap between Networks
3.5. Comparisons of rsFC at Baseline and Pre- and Post-Treatment Changes in rsFC between Remitters and Non-Remitters
4. Discussion
4.1. Aberrant rsFC in Baseline MDD
4.2. States-Independence and -Dependence of the Aberrant rsFC
4.3. Changes of rsFC before and after the Treatment in Patients with MDD
4.4. The Overlap between the Networks
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5™, 5th ed.; American Psychiatric Publishing, Inc.: Arlington, VA, USA, 2013; pp. 150–151. [Google Scholar]
- Ferrari, A.J.; Charlson, F.J.; Norman, R.E.; Patten, S.B.; Freedman, G.; Murray, C.J.; Vos, T.; Whiteford, H.A. Burden of depressive disorders by country, sex, age, and year: Findings from the global burden of disease study 2010. PLoS Med. 2013, 10, e1001547. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Wang, Y.; Wang, H.; Liu, Z.; Yu, X.; Yan, J.; Yu, Y.; Kou, C.; Xu, X.; Lu, J.; et al. Prevalence of mental disorders in China: A cross-sectional epidemiological study. Lancet Psychiatry 2019, 6, 211–224. [Google Scholar] [CrossRef] [PubMed]
- Monroe, S.M.; Harkness, K.L. Major Depression and Its Recurrences: Life Course Matters. Annu. Rev. Clin. Psychol. 2022, 18, 329–357. [Google Scholar] [CrossRef] [PubMed]
- Baldessarini, R.J. Chemotherapy in Psychiatry, 3rd ed.; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Davidson, J.R. Major depressive disorder treatment guidelines in America and Europe. J. Clin. Psychiatry 2010, 71 (Suppl. E1), e04. [Google Scholar] [CrossRef]
- Rush, A.J.; Trivedi, M.H.; Wisniewski, S.R.; Nierenberg, A.A.; Stewart, J.W.; Warden, D.; Niederehe, G.; Thase, M.E.; Lavori, P.W.; Lebowitz, B.D.; et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: A STAR * D report. Am. J. Psychiatry 2006, 163, 1905–1917. [Google Scholar] [CrossRef]
- Dunlop, B.W. Prediction of treatment outcomes in major depressive disorder. Expert Rev. Clin. Pharmacol. 2015, 8, 669–672. [Google Scholar] [CrossRef]
- Zisook, S.; Lesser, I.; Stewart, J.W.; Wisniewski, S.R.; Balasubramani, G.K.; Fava, M.; Gilmer, W.S.; Dresselhaus, T.R.; Thase, M.E.; Nierenberg, A.A.; et al. Effect of age at onset on the course of major depressive disorder. Am. J. Psychiatry 2007, 164, 1539–1546. [Google Scholar] [CrossRef]
- Leuchter, A.F.; Cook, I.A.; Marangell, L.B.; Gilmer, W.S.; Burgoyne, K.S.; Howland, R.H.; Trivedi, M.H.; Zisook, S.; Jain, R.; McCracken, J.T.; et al. Comparative effectiveness of biomarkers and clinical indicators for predicting outcomes of SSRI treatment in Major Depressive Disorder: Results of the BRITE-MD study. Psychiatry Res. 2009, 169, 124–131. [Google Scholar] [CrossRef]
- Gottesman, I.I.; Gould, T.D. The Endophenotype Concept in Psychiatry: Etymology and Strategic Intentions. Am. J. Psychiatry 2003, 160, 636–645. [Google Scholar] [CrossRef]
- Drysdale, A.T.; Grosenick, L.; Downar, J.; Dunlop, K.; Mansouri, F.; Meng, Y.; Fetcho, R.N.; Zebley, B.; Oathes, D.J.; Etkin, A.; et al. Resting-state connectivity biomarkers define neurophysiological subtypes of depression. Nat. Med. 2017, 23, 28–38. [Google Scholar] [CrossRef]
- Tavor, I.; Parker Jones, O.; Mars, R.B.; Smith, S.M.; Behrens, T.E.; Jbabdi, S. Task-free MRI predicts individual differences in brain activity during task performance. Science 2016, 352, 216–220. [Google Scholar] [CrossRef]
- Panksepp, J. Affective neuroscience of the emotional BrainMind: Evolutionary perspectives and implications for understanding depression. Dialogues Clin. Neurosci. 2010, 12, 533–545. [Google Scholar] [CrossRef]
- Mulders, P.C.; van Eijndhoven, P.F.; Schene, A.H.; Beckmann, C.F.; Tendolkar, I. Resting-state functional connectivity in major depressive disorder: A review. Neurosci. Biobehav. Rev. 2015, 56, 330–344. [Google Scholar] [CrossRef]
- Berwian, I.M.; Wenzel, J.G.; Kuehn, L.; Schnuerer, I.; Kasper, L.; Veer, I.M.; Seifritz, E.; Stephan, K.E.; Walter, H.; Huys, Q.J.M. The relationship between resting-state functional connectivity, antidepressant discontinuation and depression relapse. Sci. Rep. 2020, 10, 22346. [Google Scholar] [CrossRef]
- Dichter, G.S.; Gibbs, D.; Smoski, M.J. A systematic review of relations between resting-state functional-MRI and treatment response in major depressive disorder. J. Affect. Disord. 2015, 172, 8–17. [Google Scholar] [CrossRef]
- McCabe, C.; Mishor, Z. Antidepressant medications reduce subcortical-cortical resting-state functional connectivity in healthy volunteers. Neuroimage 2011, 57, 1317–1323. [Google Scholar] [CrossRef]
- Liu, B.; Sun, J.; Qin, X.; Wang, M.; Lu, X.; Dong, Q.; Zhang, L.; Liu, J.; Ju, Y.; Wan, P.; et al. State-Dependent and Trait-Like Characteristics of Dysfunctional Attitudes in Patients With Major Depressive Disorder. Front. Psychiatry 2020, 11, 645. [Google Scholar] [CrossRef]
- Repple, J.; Mauritz, M.; Meinert, S.; de Lange, S.C.; Grotegerd, D.; Opel, N.; Redlich, R.; Hahn, T.; Förster, K.; Leehr, E.J.; et al. Severity of current depression and remission status are associated with structural connectome alterations in major depressive disorder. Mol. Psychiatry 2020, 25, 1550–1558. [Google Scholar] [CrossRef]
- Fales, C.L.; Barch, D.M.; Rundle, M.M.; Mintun, M.A.; Mathews, J.; Snyder, A.Z.; Sheline, Y.I. Antidepressant treatment normalizes hypoactivity in dorsolateral prefrontal cortex during emotional interference processing in major depression. J. Affect. Disord. 2009, 112, 206–211. [Google Scholar] [CrossRef]
- Mayberg, H.S.; Brannan, S.K.; Tekell, J.L.; Silva, J.A.; Mahurin, R.K.; McGinnis, S.; Jerabek, P.A. Regional metabolic effects of fluoxetine in major depression: Serial changes and relationship to clinical response. Biol. Psychiatry 2000, 48, 830–843. [Google Scholar] [CrossRef]
- Andreescu, C.; Tudorascu, D.L.; Butters, M.A.; Tamburo, E.; Patel, M.; Price, J.; Karp, J.F.; Reynolds, C.F., 3rd; Aizenstein, H. Resting state functional connectivity and treatment response in late-life depression. Psychiatry Res. 2013, 214, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, P.B.; Laird, A.R.; Maller, J.; Daskalakis, Z.J. A meta-analytic study of changes in brain activation in depression. Hum. Brain Mapp. 2008, 29, 683–695. [Google Scholar] [CrossRef] [PubMed]
- Delaveau, P.; Jabourian, M.; Lemogne, C.; Guionnet, S.; Bergouignan, L.; Fossati, P. Brain effects of antidepressants in major depression: A meta-analysis of emotional processing studies. J. Affect. Disord. 2011, 130, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Depping, M.S.; Schmitgen, M.M.; Kubera, K.M.; Wolf, R.C. Cerebellar Contributions to Major Depression. Front. Psychiatry 2018, 9, 634. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Su, Y.A.; Wu, Y.K.; Castellanos, F.X.; Li, K.; Li, J.T.; Si, T.M.; Yan, C.G. Eight-week antidepressant treatment reduces functional connectivity in first-episode drug-naïve patients with major depressive disorder. Hum. Brain Mapp. 2021, 42, 2593–2605. [Google Scholar] [CrossRef]
- Rütgen, M.; Pletti, C.; Tik, M.; Kraus, C.; Pfabigan, D.M.; Sladky, R.; Klöbl, M.; Woletz, M.; Vanicek, T.; Windischberger, C.; et al. Antidepressant treatment, not depression, leads to reductions in behavioral and neural responses to pain empathy. Transl. Psychiatry 2019, 9, 164. [Google Scholar] [CrossRef]
- Qin, J.; Shen, H.; Zeng, L.L.; Jiang, W.; Liu, L.; Hu, D. Predicting clinical responses in major depression using intrinsic functional connectivity. Neuroreport 2015, 26, 675–680. [Google Scholar] [CrossRef]
- Korgaonkar, M.S.; Goldstein-Piekarski, A.N.; Fornito, A.; Williams, L.M. Intrinsic connectomes are a predictive biomarker of remission in major depressive disorder. Mol. Psychiatry 2020, 25, 1537–1549. [Google Scholar] [CrossRef]
- Cheng, Y.; Xu, J.; Arnone, D.; Nie, B.; Yu, H.; Jiang, H.; Bai, Y.; Luo, C.; Campbell, R.A.; Shan, B.; et al. Resting-state brain alteration after a single dose of SSRI administration predicts 8-week remission of patients with major depressive disorder. Psychol. Med. 2017, 47, 438–450. [Google Scholar] [CrossRef]
- Meyer, B.M.; Rabl, U.; Huemer, J.; Bartova, L.; Kalcher, K.; Provenzano, J.; Brandner, C.; Sezen, P.; Kasper, S.; Schatzberg, A.F.; et al. Prefrontal networks dynamically related to recovery from major depressive disorder: A longitudinal pharmacological fMRI study. Transl. Psychiatry 2019, 9, 64. [Google Scholar] [CrossRef]
- Wang, L.; Li, K.; Zhang, Q.; Zeng, Y.; Dai, W.; Su, Y.; Wang, G.; Tan, Y.; Jin, Z.; Yu, X.; et al. Short-term effects of escitalopram on regional brain function in first-episode drug-naive patients with major depressive disorder assessed by resting-state functional magnetic resonance imaging. Psychol. Med. 2014, 44, 1417–1426. [Google Scholar] [CrossRef]
- Wang, L.; Li, X.; Li, K.; Su, Y.; Zeng, Y.; Zhang, Q.; Wang, G.; Jin, Z.; Kong, Q.; Si, T. Mapping the effect of escitalopram treatment on amplitude of low-frequency fluctuations in patients with depression: A resting-state fMRI study. Metab. Brain Dis. 2017, 32, 147–154. [Google Scholar] [CrossRef]
- Zalesky, A.; Fornito, A.; Bullmore, E.T. Network-based statistic: Identifying differences in brain networks. Neuroimage 2010, 53, 1197–1207. [Google Scholar] [CrossRef]
- Ju, Y.; Wang, M.; Liu, J.; Liu, B.; Yan, D.; Lu, X.; Sun, J.; Dong, Q.; Zhang, L.; Guo, H.; et al. Modulation of resting-state functional connectivity in default mode network is associated with the long-term treatment outcome in major depressive disorder. Psychol. Med. 2022, 52, 1–13. [Google Scholar] [CrossRef]
- Ju, Y.; Horien, C.; Chen, W.; Guo, W.; Lu, X.; Sun, J.; Dong, Q.; Liu, B.; Liu, J.; Yan, D.; et al. Connectome-based models can predict early symptom improvement in major depressive disorder. J. Affect. Disord. 2020, 273, 442–452. [Google Scholar] [CrossRef]
- Finn, E.S.; Shen, X.; Scheinost, D.; Rosenberg, M.D.; Huang, J.; Chun, M.M.; Papademetris, X.; Constable, R.T. Functional connectome fingerprinting: Identifying individuals using patterns of brain connectivity. Nat. Neurosci. 2015, 18, 1664–1671. [Google Scholar] [CrossRef]
- Ahuja, R.; Magnanti, T.; Orlin, J. Network Flows: Theory, Algorithms and Applications. Interfaces 1994, 24, 133–135. [Google Scholar]
- Cheng, W.; Rolls, E.T.; Qiu, J.; Liu, W.; Tang, Y.; Huang, C.C.; Wang, X.; Zhang, J.; Lin, W.; Zheng, L.; et al. Medial reward and lateral non-reward orbitofrontal cortex circuits change in opposite directions in depression. Brain 2016, 139, 3296–3309. [Google Scholar] [CrossRef]
- Wegener, I.; Geiser, F.; Alfter, S.; Mierke, J.; Imbierowicz, K.; Kleiman, A.; Koch, A.S.; Conrad, R. Changes of explicitly and implicitly measured self-esteem in the treatment of major depression: Evidence for implicit self-esteem compensation. Compr. Psychiatry 2015, 58, 57–67. [Google Scholar] [CrossRef]
- Köhler, C.A.; Carvalho, A.F.; Alves, G.S.; McIntyre, R.S.; Hyphantis, T.N.; Cammarota, M. Autobiographical Memory Disturbances in Depression: A Novel Therapeutic Target? Neural. Plast. 2015, 2015, 759139. [Google Scholar] [CrossRef]
- Wang, M.; Ju, Y.; Lu, X.; Sun, J.; Dong, Q.; Liu, J.; Zhang, L.; Zhang, Y.; Zhang, S.; Wang, Z.; et al. Longitudinal changes of amplitude of low-frequency fluctuations in MDD patients: A 6-month follow-up resting-state functional magnetic resonance imaging study. J. Affect. Disord. 2020, 276, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Buckner, R.L.; Krienen, F.M.; Castellanos, A.; Diaz, J.C.; Yeo, B.T. The organization of the human cerebellum estimated by intrinsic functional connectivity. J. Neurophysiol. 2011, 106, 2322–2345. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Liu, F.; Xue, Z.; Gao, K.; Liu, Z.; Xiao, C.; Chen, H.; Zhao, J. Abnormal resting-state cerebellar-cerebral functional connectivity in treatment-resistant depression and treatment sensitive depression. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2013, 44, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Alalade, E.; Denny, K.; Potter, G.; Steffens, D.; Wang, L. Altered cerebellar-cerebral functional connectivity in geriatric depression. PLoS ONE 2011, 6, e20035. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Zeng, L.L.; Li, Y.; Ma, Q.; Li, B.; Shen, H.; Hu, D. Altered cerebellar functional connectivity with intrinsic connectivity networks in adults with major depressive disorder. PLoS ONE 2012, 7, e39516. [Google Scholar] [CrossRef]
- Narumoto, J.; Okada, T.; Sadato, N.; Fukui, K.; Yonekura, Y. Attention to emotion modulates fMRI activity in human right superior temporal sulcus. Cogn. Brain Res. 2001, 12, 225–231. [Google Scholar] [CrossRef]
- Disner, S.G.; Beevers, C.G.; Haigh, E.A.; Beck, A.T. Neural mechanisms of the cognitive model of depression. Nat. Rev. Neurosci. 2011, 12, 467–477. [Google Scholar] [CrossRef]
- Wang, L.; Yu, L.; Wu, F.; Wu, H.; Wang, J. Altered whole brain functional connectivity pattern homogeneity in medication-free major depressive disorder. J. Affect. Disord. 2019, 253, 18–25. [Google Scholar] [CrossRef]
- Pizzagalli, D.A.; Holmes, A.J.; Dillon, D.G.; Goetz, E.L.; Birk, J.L.; Bogdan, R.; Dougherty, D.D.; Iosifescu, D.V.; Rauch, S.L.; Fava, M. Reduced caudate and nucleus accumbens response to rewards in unmedicated individuals with major depressive disorder. Am. J. Psychiatry 2009, 166, 702–710. [Google Scholar] [CrossRef]
- Murrough, J.W.; Collins, K.A.; Fields, J.; DeWilde, K.E.; Phillips, M.L.; Mathew, S.J.; Wong, E.; Tang, C.Y.; Charney, D.S.; Iosifescu, D.V. Regulation of neural responses to emotion perception by ketamine in individuals with treatment-resistant major depressive disorder. Transl. Psychiatry 2015, 5, e509. [Google Scholar] [CrossRef]
- Abdallah, C.G.; Averill, L.A.; Collins, K.A.; Geha, P.; Schwartz, J.; Averill, C.; DeWilde, K.E.; Wong, E.; Anticevic, A.; Tang, C.Y.; et al. Ketamine Treatment and Global Brain Connectivity in Major Depression. Neuropsychopharmacology 2017, 42, 1210–1219. [Google Scholar] [CrossRef]
- Stalnaker, T.A.; Cooch, N.K.; Schoenbaum, G. What the orbitofrontal cortex does not do. Nat. Neurosci. 2015, 18, 620–627. [Google Scholar] [CrossRef]
- de Pasquale, F.; Della Penna, S.; Snyder, A.Z.; Marzetti, L.; Pizzella, V.; Romani, G.L.; Corbetta, M. A cortical core for dynamic integration of functional networks in the resting human brain. Neuron 2012, 74, 753–764. [Google Scholar] [CrossRef]
- Wada, S.; Honma, M.; Masaoka, Y.; Yoshida, M.; Koiwa, N.; Sugiyama, H.; Iizuka, N.; Kubota, S.; Kokudai, Y.; Yoshikawa, A.; et al. Volume of the right supramarginal gyrus is associated with a maintenance of emotion recognition ability. PLoS ONE 2021, 16, e0254623. [Google Scholar] [CrossRef]
- Buhle, J.T.; Silvers, J.A.; Wager, T.D.; Lopez, R.; Onyemekwu, C.; Kober, H.; Weber, J.; Ochsner, K.N. Cognitive Reappraisal of Emotion: A Meta-Analysis of Human Neuroimaging Studies. Cereb. Cortex 2013, 24, 2981–2990. [Google Scholar] [CrossRef]
- Murray, E.A.; Wise, S.P.; Drevets, W.C. Localization of dysfunction in major depressive disorder: Prefrontal cortex and amygdala. Biol. Psychiatry 2011, 69, e43–e54. [Google Scholar] [CrossRef]
- Zhuo, C.; Zhou, C.; Lin, X.; Tian, H.; Wang, L.; Chen, C.; Ji, F.; Xu, Y.; Jian, D. Common and distinct global functional connectivity density alterations in drug-naïve patients with first-episode major depressive disorder with and without auditory verbal hallucination. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2020, 96, 109738. [Google Scholar] [CrossRef]
- Vercammen, A.; Knegtering, H.; Bruggeman, R.; Aleman, A. Subjective loudness and reality of auditory verbal hallucinations and activation of the inner speech processing network. Schizophr. Bull. 2011, 37, 1009–1016. [Google Scholar] [CrossRef]
- Qiu, L.; Ye, J.; Ji, F.; Li, G.; Li, G.; Ma, X.; Li, R.; Tian, H.; Wang, L.; Chen, G.; et al. Common and distinct global functional connectivity density alterations in patients with bipolar disorder with and without auditory verbal hallucination during major depressive episodes. Brain Imaging Behav. 2020, 14, 2724–2730. [Google Scholar] [CrossRef]
- Grimm, S.; Ernst, J.; Boesiger, P.; Schuepbach, D.; Boeker, H.; Northoff, G. Reduced negative BOLD responses in the default-mode network and increased self-focus in depression. World J. Biol. Psychiatry 2011, 12, 627–637. [Google Scholar] [CrossRef]
- Li, B.; Liu, L.; Friston, K.J.; Shen, H.; Wang, L.; Zeng, L.L.; Hu, D. A treatment-resistant default mode subnetwork in major depression. Biol. Psychiatry 2013, 74, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Yao, J.; Jiang, X.; Zhang, L.; Xu, L.; Feng, R.; Cai, L.; Liu, J.; Wang, J.; Chen, W. Sub-hubs of baseline functional brain networks are related to early improvement following two-week pharmacological therapy for major depressive disorder. Hum. Brain Mapp. 2015, 36, 2915–2927. [Google Scholar] [CrossRef] [PubMed]
- Lu, F.; Cui, Q.; Huang, X.; Li, L.; Duan, X.; Chen, H.; Pang, Y.; He, Z.; Sheng, W.; Han, S.; et al. Anomalous intrinsic connectivity within and between visual and auditory networks in major depressive disorder. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2020, 100, 109889. [Google Scholar] [CrossRef] [PubMed]
- Roet, M.; Boonstra, J.; Sahin, E.; Mulders, A.E.P.; Leentjens, A.F.G.; Jahanshahi, A. Deep Brain Stimulation for Treatment-Resistant Depression: Towards a More Personalized Treatment Approach. J. Clin. Med. 2020, 9, 2729. [Google Scholar] [CrossRef]
- Phillips, M.L.; Chase, H.W.; Sheline, Y.I.; Etkin, A.; Almeida, J.R.; Deckersbach, T.; Trivedi, M.H. Identifying predictors, moderators, and mediators of antidepressant response in major depressive disorder: Neuroimaging approaches. Am. J. Psychiatry 2015, 172, 124–138. [Google Scholar] [CrossRef]
- Fonseka, T.M.; MacQueen, G.M.; Kennedy, S.H. Neuroimaging biomarkers as predictors of treatment outcome in Major Depressive Disorder. J. Affect. Disord. 2018, 233, 21–35. [Google Scholar] [CrossRef]
- Guo, C.C.; Kurth, F.; Zhou, J.; Mayer, E.A.; Eickhoff, S.B.; Kramer, J.H.; Seeley, W.W. One-year test-retest reliability of intrinsic connectivity network fMRI in older adults. Neuroimage 2012, 61, 1471–1483. [Google Scholar] [CrossRef]
- Birn, R.M.; Molloy, E.K.; Patriat, R.; Parker, T.; Meier, T.B.; Kirk, G.R.; Nair, V.A.; Meyerand, M.E.; Prabhakaran, V. The effect of scan length on the reliability of resting-state fMRI connectivity estimates. Neuroimage 2013, 83, 550–558. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Baseline MDD (n = 196) | Follow-up MDD (n = 114) | Follow-up Excluded (n = 82) | HCs (n = 143) | Baseline MDD vs. HCs | Follow-up MDD vs. HCs | Follow-up MDD vs. Follow-Up Excluded | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| t/χ2 Value | p Value | t/χ2 Value | p Value | t/χ2/Z Value | p Value | |||||
| Age (years, x ± s) | 35.9 ± 10.1 | 36.4 ± 10.3 | 35.3 ± 10.0 | 35.2 ± 9.6 | 0.697 a | 0.486 | 0.968 a | 0.334 | 0.722 a | 0.471 |
| Gender (%) | 1.849 b | 0.174 | 1.154 b | 0.283 | 0.056 b | 0.831 | ||||
| Male | 120 (61.2%) | 69 (60.5%) | 51 (62%) | 77 (53.9%) | ||||||
| Female | 76 (38.8%) | 45 (39.5%) | 31 (37.8%) | 66 (46.1%) | ||||||
| Education (years, x ± s) | 10.3 ± 3.3 | 10.6 ± 3.4 | 9.7 ± 3.2 | 11.0 ± 3.5 | 1.826 a | 0.069 | 0.949 a | 0.344 | 1.880 a | 0.062 |
| Age of onset (years, x ± s) | 33.1 ± 7.0 | 32.7 ± 10.5 | 32.7 ± 10.5 | - | - | - | - | - | 0.750 a | 0.454 |
| Total illness duration, M (P25, P75) | 18 (3, 65) | 21 (6, 63) | 16 (3, 75) | - | - | - | - | - | 0.727 c | 0.476 |
| Current illness duration, M (P25, P75) | 2 (2, 5) | 2 (1.75, 4) | 3 (2, 6) | - | - | - | - | - | 1.796 c | 0.072 |
| Total number of episodes (x ± s) | 2.1 ± 1.4 | 2 ± 1.6 | 1.9 ± 2.1 | - | - | - | - | - | 1.196 a | 0.233 |
| Status of onset, (%) | - | - | - | - | 2.655 b | 0.103 | ||||
| First onset | 80 (40.8%) | 41 (36.0%) | 39 (47.5%) | - | ||||||
| Recurrent onset | 116 (59.2%) | 73 (64.0%) | 43 (52.4%) | - | ||||||
| HAMD at baseline (x ± s) | 31.5 ± 6.9 | 31.5 ± 6.9 | 30.2 ± 7.2 | 1.4 ± 1.8 | 55.83 a | <0.001 | 45.33 a | <0.001 | 1.217 a | 0.225 |
| HAMA at baseline (x ± s) | 17.9 ± 6.3 | 17.8 ± 6.4 | 18.0 ± 6.0 | 1.3 ± 1.9 | 32.74 a | <0.001 | 25.28 a | <0.001 | 0.250 a | 0.803 |
| Antidepressants (%) | - | - | - | - | 5.441 * | 0.067 | ||||
| Paroxetine | 119 (60.7%) | 78 (68.4%) | 41 (50.0%) | |||||||
| Other SSRIs | 53 (27.0%) | 23 (20.2%) | 30 (36.6%) | |||||||
| SNRIs | 10 (5.1%) | 8 (7.0%) | 2 (2.4%) | |||||||
| Others | 14 (7.1%) | 5 (4.4%) | 9 (11.0%) | |||||||
| Combined medication (%) | ||||||||||
| Mood stabilizer | 5(2.6%) | 4(3.5%) | 1(1.2%) | - | - | - | - | 1.005 a | 1.306 | |
| Antianxiety | 50(25.6) | 29(25.4%) | 21(25.6%) | - | - | - | - | 0.533 a | 0.465 | |
| Antidepressant | 23(11.7%) | 15(13.2%) | 8(9.8%) | - | - | - | - | 0.023 a | 0.881 | |
| Antipsychotic | 15 (7.6%) | 9 (7.9%) | 6 (7.3%) | - | - | - | - | 0.023 a | 0.881 | |
| Sedative-hypnotics | 94 (48.0%) | 58 (50.9%) | 36 (43.9%) | - | - | - | - | 0.930 a | 0.335 | |
| Baseline mean FFD (mm, x ± s) | 0.065 ± 0.042 | 0.061 ± 0.038 | 0.071 ± 0.046 | 0.062 ± 0.037 | 0.647 a | 0.085 | 0.298 a | 0.770 | 1.633 a | 0.029 |
| Follow-up mean FFD (mm, x ± s) | - | - | - | - | - | - | - | - | - | - |
| Remitters (n = 83) | Non-Remitters (n = 31) | HCs (n = 143) | Comparisons among Three Groups | Remitters vs. HCs | Non-Remitters vs. HCs | Remitters vs. Non-Remitters | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| F/χ2 Value | p Value | t/χ2 Value | p Value | t/χ2 Value | p Value | t/χ2/Z Value | p Value | ||||
| Age (years, x ± s) | 36.6 ± 10.5 | 35.7 ± 9.8 | 35.2 ± 9.6 | 0.435 a | 0.648 | 1.054 a | 0.293 | 0.291 a | 0.771 | 0.411 a | 0.682 |
| Gender (%) | 1.661 b | 0.436 | 2.153 b | 0.142 | 0.051 b | 0.821 | 1.416 b | 0.234 | |||
| Female | 53 (63.9%) | 16 (51.6%) | 77 (53.9%) | ||||||||
| Male | 30 (36.1%) | 15 (48.4%) | 66 (46.1%) | ||||||||
| Education (years, x ± s) | 10.8 ± 3.4 | 9.9 ± 3.5 | 11.0 ± 3.5 | 2.527 a | 0.081 | 0.357 a | 0.721 | 1.527 a | 0.129 | 1.247 a | 0.215 |
| Age of onset (years, x ± s) | 33.0 ± 10.8 | 32.1 ± 9.7 | - | - | - | - | - | - | - | 0.392 c | 0.696 |
| Total illness duration M (P25, P75) | 14 (3,70) | 25 (13,61) | - | - | - | - | - | - | - | 1.228 d | 0.219 |
| Current illness duration M (P25, P75) | 2 (1, 4) | 2 (2, 4) | - | - | - | - | - | - | - | 0.340 d | 0.734 |
| Total number of episodes (x ± s) | 2 ± 1.7 | 2 ± 1.3 | - | - | - | - | - | - | - | 0.074 c | 0.941 |
| Status of onset (%) | - | - | - | - | - | - | 1.908 b | 0.167 | |||
| First onset | 33 (39.7%) | 8 (25.8%) | - | ||||||||
| Recurrent onset | 50 (60.3%) | 23 (74.2%) | - | ||||||||
| HAMD at baseline (x ± s) | 31.7 ± 7.1 | 30.9 ± 6.5 | 1.4 ± 1.8 | 267.5 a | <0.001 | 38.27 a | <0.001 | 25.19 a | <0.001 | 0.561 a | 0.576 |
| HAMD at the end of 6 months (x ± s) | 2.4 ± 3 | 14.5 ± 9.0 | - | - | - | - | - | - | - | - | - |
| HAMA at baseline (x ± s) | 17.9 ± 6.6 | 17.6 ± 6.1 | 1.3 ± 1.9 | 220.1 a | <0.001 | 16.61 a | <0.001 | 14.27 a | <0.001 | 0.241 a | 0.81 |
| HAMA at the end of 6 months (x ± s) | 1.6 ± 1.8 | 10.2 ± 5.7 | - | - | - | - | - | - | - | - | - |
| Antidepressants (%) | - | - | - | - | - | 0.444 *b | 0.801 | ||||
| Paroxetine | 59 (71.1%) | 19 (61.3%) | - | ||||||||
| Other SSRIs | 15 (18.1%) | 8 (25.8%) | - | ||||||||
| SNRIs | 6 (7.2%) | 2 (6.5%) | - | ||||||||
| Others | 3 (3.6%) | 2 (6.5%) | - | ||||||||
| Drug combination (%) | |||||||||||
| Mood stabilizer | 3(3.6%) | 1(3.2%) | - | - | - | - | - | - | - | 0.0004 b | 0.983 |
| Antianxiety | 22(26.5%) | 7(22.6%) | - | - | - | - | - | - | - | 0.004 b | 0.951 |
| Antidepressant | 9(10.8%) | 6(19.4) | - | - | - | - | - | - | - | 2.222 b | 0.136 |
| Antipsychotic | 6 (7.1%) | 3 (9.7%) | - | - | - | - | - | - | - | 0.186 b | 0.666 |
| Sedative-hypnotics | 43 (51.8%) | 15 (48.4%) | - | - | - | - | - | - | - | 0.106 b | 0.745 |
| Baseline mean FFD (mm, x ± s) | 0.060 ± 0.039 | 0.065 ± 0.036 | 0.062 ± 0.037 | 0.251 a | 0.779 | 0.534 a | 0.608 | 0.314 a | 0.750 | 0.633 a | 0.529 |
| Follow-up mean FFD (mm, x ± s) | 0.068 ± 0.044 | 0.063 ± 0.036 | - | - | - | - | - | - | - | 0.524 a | 0.135 |
| Brain Region 1 | MNI Coordinate (x, y, z) | Brain Network | Brain Region 2 | MNI Coordinate (x, y, z) | Brain Network | ||||
|---|---|---|---|---|---|---|---|---|---|
| The overlap between the“MDD reduced sub-network” and “follow-up increased sub-network” | |||||||||
| R supramarginal gyrus | 13.9 | 56.9 | −16.6 | Mot | R orbitofrontal gyrus | 49 | −58.1 | 14.4 | DMN |
| L cerebellum | 13.9 | 56.9 | −16.6 | SAL | R dorsolateral prefrontal lobe | 61.8 | −22.9 | −22.4 | FP |
| R secondary visual cortex | 13.9 | 56.9 | −16.6 | VI | L primary sensory area | 7.8 | 34.7 | 17.1 | Mot |
| The overlap between the“MDD increased network” and “follow-up decreased sub-network” | |||||||||
| R orbitofrontal gyrus | 5.1 | 34.9 | −17.4 | DMN | L visual associative cortex | −41.3 | −75.4 | 22.8 | DMN |
| R precuneus | 7.5 | −57.3 | 61.8 | SAL | R dorsal posterior cingulate cortex | 7.8 | −23.1 | 44.9 | Mot |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, K.; Lu, X.; Xiao, C.; Zheng, K.; Sun, J.; Dong, Q.; Wang, M.; Zhang, L.; Liu, B.; Liu, J.; et al. Aberrant Resting-State Functional Connectivity in MDD and the Antidepressant Treatment Effect—A 6-Month Follow-Up Study. Brain Sci. 2023, 13, 705. https://doi.org/10.3390/brainsci13050705
Li K, Lu X, Xiao C, Zheng K, Sun J, Dong Q, Wang M, Zhang L, Liu B, Liu J, et al. Aberrant Resting-State Functional Connectivity in MDD and the Antidepressant Treatment Effect—A 6-Month Follow-Up Study. Brain Sciences. 2023; 13(5):705. https://doi.org/10.3390/brainsci13050705
Chicago/Turabian StyleLi, Kangning, Xiaowen Lu, Chuman Xiao, Kangning Zheng, Jinrong Sun, Qiangli Dong, Mi Wang, Liang Zhang, Bangshan Liu, Jin Liu, and et al. 2023. "Aberrant Resting-State Functional Connectivity in MDD and the Antidepressant Treatment Effect—A 6-Month Follow-Up Study" Brain Sciences 13, no. 5: 705. https://doi.org/10.3390/brainsci13050705
APA StyleLi, K., Lu, X., Xiao, C., Zheng, K., Sun, J., Dong, Q., Wang, M., Zhang, L., Liu, B., Liu, J., Zhang, Y., Guo, H., Zhao, F., Ju, Y., & Li, L. (2023). Aberrant Resting-State Functional Connectivity in MDD and the Antidepressant Treatment Effect—A 6-Month Follow-Up Study. Brain Sciences, 13(5), 705. https://doi.org/10.3390/brainsci13050705