
Maximal Safe Resection in Glioblastoma Surgery: A Systematic Review of Advanced Intraoperative Image-Guided Techniques

 ,
, 
Abstract
1. Introduction
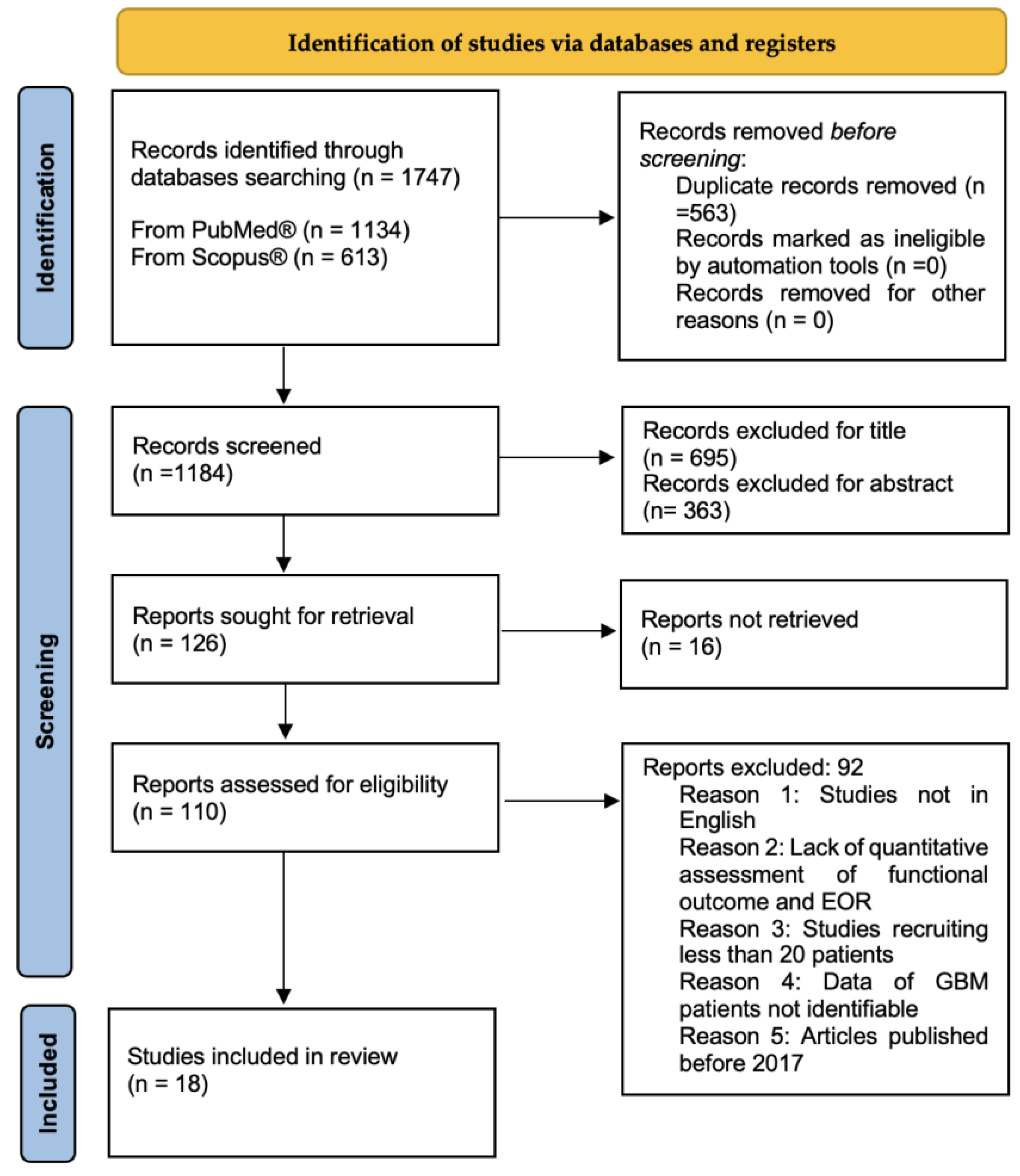
2. Materials and Methods
2.1. Search of the Literature
2.2. Study Selection and Risk of Bias Assessment
2.3. Eligibility Criteria
- Full articles in English;
- Clinical studies;
- Studies including patients affected by GBM and/or HGG (studies focusing on HGG were considered only if characteristics of GBM patients were identifiable);
- Age > 18 years old;
- Studies assessing functional outcomes (expressed using standardized scales, i.e., KPS or NANO score);
- Studies assessing EOR.
- Meta-analysis, reviews, case reports, editorials, technical notes;
- Lack of quantitative assessment of functional outcome and extent of resection;
- Recruited less than 20 patients;
- Article published before 2017.
2.4. Data Extraction
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias Assessment
3.4. Study Synthesis
4. Discussion
4.1. Fluorescence Techniques
4.1.1. Aminolaevulinic Acid
4.1.2. Sodium Fluorescein
4.2. Neuronavigation and Tractography
4.3. Intraoperative Ultrasound
4.4. Intraoperative MRI
4.5. Future Directions–Digital Biopsy
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Salcman, M. Glioblastoma Multiforme. Am. J. Med. Sci. 1980, 279, 84–94. [Google Scholar] [CrossRef] [PubMed]
- Zigiotto, L.; Annicchiarico, L.; Corsini, F.; Vitali, L.; Falchi, R.; Dalpiaz, C.; Rozzanigo, U.; Barbareschi, M.; Avesani, P.; Papagno, C.; et al. Effects of Supra-Total Resection in Neurocognitive and Oncological Outcome of High-Grade Gliomas Comparing Asleep and Awake Surgery. J. Neuro-Oncol. 2020, 148, 97–108. [Google Scholar] [CrossRef] [PubMed]
- Torregrossa, F.; Aguennouz, M.; la Torre, D.; Sfacteria, A.; Grasso, G. Role of Erythropoietin in Cerebral Glioma: An Innovative Target in Neuro-Oncology. World Neurosurg. 2019, 131, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Grasso, G.; Midiri, M.; Catalano, C.; Gagliardo, C. Transcranial Magnetic Resonance-Guided Focused Ultrasound Surgery for Brain Tumor Ablation: Are We Ready for This Challenging Treatment? World Neurosurg. 2018, 119, 438–440. [Google Scholar] [CrossRef] [PubMed]
- Grasso, G.; Torregrossa, F. When Neuroprotection Becomes a Potential Ally of High-Grade Glioma. World Neurosurg. 2019, 125, 529–530. [Google Scholar] [CrossRef]
- Kotrotsou, A.; Elakkad, A.; Sun, J.; Thomas, G.A.; Yang, D.; Abrol, S.; Wei, W.; Weinberg, J.S.; Bakhtiari, A.S.; Kircher, M.F.; et al. Multi-Center Study Finds Postoperative Residual Non-Enhancing Component of Glioblastoma as a New Determinant of Patient Outcome. J. Neuro-Oncol. 2018, 139, 125–133. [Google Scholar] [CrossRef]
- Brown, T.J.; Brennan, M.C.; Li, M.; Church, E.W.; Brandmeir, N.J.; Rakszawski, K.L.; Patel, A.S.; Rizk, E.B.; Suki, D.; Sawaya, R.; et al. Association of the Extent of Resection with Survival in Glioblastoma a Systematic Review and Meta-Analysis. JAMA Oncol. 2016, 2, 1460–1469. [Google Scholar] [CrossRef]
- Lacroix, M.; Abi-Said, D.; Fourney, D.R.; Gokaslan, Z.L.; Shi, W.; DeMonte, F.; Lang, F.F.; McCutcheon, I.E.; Hassenbusch, S.J.; Holland, E.; et al. A Multivariate Analysis of 416 Patients with Glioblastoma Multiforme: Prognosis, Extent of Resection, and Survival. J. Neurosurg. 2001, 95, 190–198. [Google Scholar] [CrossRef]
- Grasso, G. Extent of Resection and Survival in Glioblastoma Multiforme. JAMA Oncol. 2016, 2, 1508–1509. [Google Scholar] [CrossRef]
- Tomlinson, S.B.; Hendricks, B.K.; Torregrossa, F.; Grasso, G.; Cohen-Gadol, A.A. Innovations in the Art of Microneurosurgery for Reaching Deep-Seated Cerebral Lesions. World Neurosurg. 2019, 131, 321–327. [Google Scholar] [CrossRef]
- Li, Y.M.; Suki, D.; Hess, K.; Sawaya, R. The Influence of Maximum Safe Resection of Glioblastoma on Survival in 1229 Patients: Can We Do Better than Gross-Total Resection? J. Neurosurg. 2016, 124, 977–988. [Google Scholar] [CrossRef] [PubMed]
- Grasso, G.; Torregrossa, F.; Leone, L. Maximizing the Extent of Resection in High-Grade Glioma. World Neurosurg. 2019, 123, 256–258. [Google Scholar] [CrossRef]
- Di Ieva, A.; Magnussen, J.S.; McIntosh, J.; Mulcahy, M.J.; Pardey, M.; Choi, C. Magnetic Resonance Spectroscopic Assessment of Isocitrate Dehydrogenase Status in Gliomas: The New Frontiers of Spectrobiopsy in Neurodiagnostics. World Neurosurg. 2020, 133, e421–e427. [Google Scholar] [CrossRef]
- Duffau, H.; Mandonnet, E. The “Onco-Functional Balance” in Surgery for Diffuse Low-Grade Glioma: Integrating the Extent of Resection with Quality of Life. Acta Neurochir. 2013, 155, 951–957. [Google Scholar] [CrossRef] [PubMed]
- Rossi, M.; Nibali, M.C.; Torregrossa, F.; Bello, L.; Grasso, G. Innovation in Neurosurgery: The Concept of Cognitive Mapping. World Neurosurg. 2019, 131, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Abhinav, K.; Yeh, F.-C.; Mansouri, A.; Zadeh, G.; Fernandez-Miranda, J.C. High-Definition Fiber Tractography for the Evaluation of Perilesional White Matter Tracts in High-Grade Glioma Surgery. Neuro. Oncol. 2015, 17, 1199–1209. [Google Scholar] [CrossRef] [PubMed]
- Dadario, N.B.; Brahimaj, B.; Yeung, J.; Sughrue, M.E. Reducing the Cognitive Footprint of Brain Tumor Surgery. Front. Neurol. 2021, 12, 711646. [Google Scholar] [CrossRef]
- Samuel, N.; Vetkas, A.; Pancholi, A.; Sarica, C.; Loh, A.; Germann, J.; Harmsen, I.E.; Tasserie, J.; Milano, V.; Yamamoto, K.; et al. A Network-Based Approach to Glioma Surgery: Insights from Functional Neurosurgery. Cancers 2021, 13, 6127. [Google Scholar] [CrossRef] [PubMed]
- Grasso, G. Innovation in Neurosurgery: Integration Between Cutting-Edge Devices and “Old-Fashioned” Surgical Technique. World Neurosurg. 2019, 131, 311–312. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Whiting, P.; Savović, J.; Higgins, J.P.T.; Caldwell, D.M.; Reeves, B.C.; Shea, B.; Davies, P.; Kleijnen, J.; Churchill, R. ROBIS: A New Tool to Assess Risk of Bias in Systematic Reviews Was Developed. J. Clin. Epidemiol. 2016, 69, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Sollmann, N.; Kelm, A.; Ille, S.; Schröder, A.; Zimmer, C.; Ringel, F.; Meyer, B.; Krieg, S.M. Setup presentation and clinical outcome analysis of treating highly language-eloquent gliomas via preoperative navigated transcranial magnetic stimulation and tractography. Neurosurg Focus. 2018, 44, E2. [Google Scholar] [CrossRef]
- Neira, J.A.; Ung, T.H.; Sims, J.S.; Malone, H.R.; Chow, D.S.; Samanamud, J.L.; Zanazzi, G.J.; Guo, X.; Bowden, S.G.; Zhao, B.; et al. Aggressive Resection at the Infiltrative Margins of Glioblastoma Facilitated by Intraoperative Fluorescein Guidance. J. Neurosurg. 2017, 127, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Marongiu, A.; D’Andrea, G.; Raco, A. 1.5-T Field Intraoperative Magnetic Resonance Imaging Improves Extent of Resection and Survival in Glioblastoma Removal. World Neurosurg. 2017, 98, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Moiraghi, A.; Prada, F.; Delaidelli, A.; Guatta, R.; May, A.; Bartoli, A.; Saini, M.; Perin, A.; Wälchli, T.; Momjian, S.; et al. Navigated Intraoperative 2-Dimensional Ultrasound in High-Grade Glioma Surgery: Impact on Extent of Resection and Patient Outcome. Oper. Neurosurg. 2020, 18, 363–373. [Google Scholar] [CrossRef]
- Barbagallo, G.M.V.; Altieri, R.; Garozzo, M.; Maione, M.; Di Gregorio, S.; Visocchi, M.; Peschillo, S.; Dolce, P.; Certo, F. High Grade Glioma Treatment in Elderly People: Is It Different Than in Younger Patients? Analysis of Surgical Management Guided by an Intraoperative Multimodal Approach and Its Impact on Clinical Outcome. Front Oncol. 2021, 24, 631255. [Google Scholar] [CrossRef]
- Incekara, F.; Smits, M.; Dirven, L.; Bos, E.M.; Balvers, R.K.; Haitsma, I.K.; Schouten, J.W.; Vincent, A.J.P.E. Intraoperative B-Mode Ultrasound Guided Surgery and the Extent of Glioblastoma Resection: A Randomized Controlled Trial. Front. Oncol. 2021, 11, 649797. [Google Scholar] [CrossRef]
- Vincenzo Barbagallo, G.M.; Certo, F.; di Gregorio, S.; Maione, M.; Garozzo, M.; Peschillo, S.; Altieri, R. Recurrent High-Grade Glioma Surgery: A Multimodal Intraoperative Protocol to Safely Increase Extent of Tumor Resection and Analysis of Its Impact on Patient Outcome. Neurosurg. Focus 2021, 50, E20. [Google Scholar] [CrossRef]
- Bassaganyas-Vancells, C.; Roldán, P.; González, J.J.; Ferrés, A.; García, S.; Culebras, D.; Hoyos, J.; Reyes, L.; Torales, J.; Enseñat, J. Combined Use of 5-Aminolevulinic Acid and Intraoperative Low-Field Magnetic Resonance Imaging in High-Grade Glioma Surgery. World Neurosurg. 2019, 130, e206–e212. [Google Scholar] [CrossRef]
- Nickel, K.; Renovanz, M.; König, J.; Stöckelmaier, L.; Hickmann, A.K.; Nadji-Ohl, M.; Engelke, J.; Weimann, E.; Freudenstein, D.; Ganslandt, O.; et al. The Patients’ View: Impact of the Extent of Resection, Intraoperative Imaging, and Awake Surgery on Health-Related Quality of Life in High-Grade Glioma Patients—Results of a Multicenter Cross-Sectional Study. Neurosurg. Rev. 2018, 41, 207–219. [Google Scholar] [CrossRef]
- Luzzi, S.; Lucifero, A.G.; Martinelli, A.; del Maestro, M.; Savioli, G.; Simoncelli, A.; Lafe, E.; Preda, L.; Galzio, R. Supratentorial High-Grade Gliomas: Maximal Safe Anatomical Resection Guided by Augmented Reality High-Definition Fiber Tractography and Fluorescein. Neurosurg. Focus 2021, 51, E5. [Google Scholar] [CrossRef]
- Raffa, G.; Scibilia, A.; Conti, A.; Cardali, S.M.; Rizzo, V.; Terranova, C.; Quattropani, M.C.; Marzano, G.; Ricciardo, G.; Vinci, S.L.; et al. Multimodal Surgical Treatment of High-Grade Gliomas in the Motor Area: The Impact of the Combination of Navigated Transcranial Magnetic Stimulation and Fluorescein-Guided Resection. World Neurosurg. 2019, 128, e378–e390. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Li, X.; Zhu, X.; Wu, L.; Ma, S.; Yan, J.; Yan, D. Diffusion Tensor Imaging with Fluorescein Sodium Staining in the Resection of High-Grade Gliomas in Functional Brain Areas. World Neurosurg. 2019, 124, e595–e603. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.; Chen, B.; Yao, X.; Yang, Y. Outcome Comparisons of High-Grade Glioma Resection with or without Fluorescein. Curr. Probl. Cancer 2019, 43, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Francaviglia, N.; Iacopino, D.G.; Costantino, G.; Villa, A.; Impallaria, P.; Meli, F.; Maugeri, R. Fluorescein for Resection of High-Grade Gliomas: A Safety Study Control in a Single Center and Review of the Literature. Surg. Neurol. Int. 2017, 8, 145. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.; Fu, Z.; He, X.; Lu, J.; Deng, X.; Lin, D.; Gu, Y.; Fan, Y.; Lai, M.; Li, J.; et al. T2 Fluid-Attenuated Inversion Recovery Resection for Glioblastoma Involving Eloquent Brain Areas Facilitated Through Awake Craniotomy and Clinical Outcome. World Neurosurg. 2020, 135, e738–e747. [Google Scholar] [CrossRef] [PubMed]
- Picart, T.; Armoiry, X.; Berthiller, J.; Dumot, C.; Pelissou-guyotat, I.; Signorelli, F. Is Fluorescence-Guided Surgery with 5-Ala in Eloquent Areas for Malignant Gliomas a Reasonable and Useful Technique? Neurochirurgie 2017, 63, 189–196. [Google Scholar] [CrossRef]
- Bettag, C.; Hussein, A.; Behme, D.; Maragkou, T.; Rohde, V.; Mielke, D. Endoscopic Fluorescence-Guided Resection Increases Radicality in Glioblastoma Surgery. Oper. Neurosurg. 2020, 18, 41–46. [Google Scholar] [CrossRef]
- Catapano, G.; Sgulò, F.G.; Seneca, V.; Lepore, G.; Columbano, L.; di Nuzzo, G. Fluorescein-Guided Surgery for High-Grade Glioma Resection: An Intraoperative “Contrast-Enhancer”. World Neurosurg. 2017, 104, 239–247. [Google Scholar] [CrossRef]
- Giammalva, G.R.; Brunasso, L.; Costanzo, R.; Paolini, F.; Umana, G.E.; Scalia, G.; Gagliardo, C.; Gerardi, R.M.; Basile, L.; Graziano, F.; et al. Brain Mapping-Aided Supratotal Resection (Sptr) of Brain Tumors: The Role of Brain Connectivity. Front. Oncol. 2021, 11, 645854. [Google Scholar] [CrossRef]
- Jackson, C.; Choi, J.; Khalafallah, A.M.; Price, C.; Bettegowda, C.; Lim, M.; Gallia, G.; Weingart, J.; Brem, H.; Mukherjee, D. A Systematic Review and Meta-Analysis of Supratotal versus Gross Total Resection for Glioblastoma. J. Neurooncol. 2020, 148, 419–431. [Google Scholar] [CrossRef]
- Folaron, M.; Strawbridge, R.; Samkoe, K.S.; Filan, C.; Roberts, D.W.; Davis, S.C. Elucidating the Kinetics of Sodium Fluorescein for Fluorescence-Guided Surgery of Glioma. J. Neurosurg. 2019, 131, 724–734. [Google Scholar] [CrossRef]
- Stummer, W.; Suero Molina, E. Fluorescence Imaging/Agents in Tumor Resection. Neurosurg. Clin. N. Am. 2017, 28, 569–583. [Google Scholar] [CrossRef] [PubMed]
- Hadjipanayis, C.G.; Stummer, W. 5-ALA and FDA Approval for Glioma Surgery. J. Neurooncol. 2019, 141, 479–486. [Google Scholar] [CrossRef] [PubMed]
- della Pepa, G.M.; Ius, T.; la Rocca, G.; Gaudino, S.; Isola, M.; Pignotti, F.; Rapisarda, A.; Mazzucchi, E.; Giordano, C.; Dragonetti, V.; et al. 5-Aminolevulinic Acid and Contrast-Enhanced Ultrasound: The Combination of the Two Techniques to Optimize the Extent of Resection in Glioblastoma Surgery. Neurosurgery 2020, 86, E529–E540. [Google Scholar] [CrossRef] [PubMed]
- Eatz, T.A.; Eichberg, D.G.; Lu, V.M.; Di, L.; Komotar, R.J.; Ivan, M.E. Intraoperative 5-ALA Fluorescence-Guided Resection of High-Grade Glioma Leads to Greater Extent of Resection with Better Outcomes: A Systematic Review. J. Neurooncol. 2022, 156, 233–256. [Google Scholar] [CrossRef] [PubMed]
- Dadario, N.B.; Khatri, D.; Reichman, N.; Nwagwu, C.D.; D’Amico, R.S. 5-Aminolevulinic Acid–Shedding Light on Where to Focus. World Neurosurg. 2021, 150, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Eljamel, S. 5-ALA Fluorescence Image Guided Resection of Glioblastoma Multiforme: A Meta-Analysis of the Literature. Int. J. Mol. Sci. 2015, 16, 10443–10456. [Google Scholar] [CrossRef]
- Ba, N.L. Fluorescence—Guided Surgery for High-Grade Gliomas. J. Surg. Oncol. 2018, 118, 356–361. [Google Scholar] [CrossRef]
- Kiesel, B.; Wadiura, L.I.; Mischkulnig, M.; Makolli, J.; Sperl, V.; Borkovec, M.; Freund, J.; Lang, A.; Millesi, M.; Berghoff, A.S.; et al. Efficacy, Outcome and Safety of Elderly Patients with Glioblastoma in the 5-ALA Era: Single Center Experience of More Than 10 Years. Cancers 2021, 13, 6119. [Google Scholar] [CrossRef]
- Baig Mirza, A.; Christodoulides, I.; Lavrador, J.P.; Giamouriadis, A.; Vastani, A.; Boardman, T.; Ahmed, R.; Norman, I.; Murphy, C.; Devi, S.; et al. Aminolevulinic Acid-Guided Resection Improves the Overall Survival of Patients with Glioblastoma-a Comparative Cohort Study of 343 Patients. Neuro-Oncol. Adv. 2021, 3, vdab047. [Google Scholar] [CrossRef]
- Schupper, A.J.; Yong, R.L.; Hadjipanayis, C.G. The Neurosurgeon’ s Armamentarium for Gliomas: An Update on Intraoperative Technologies to Improve Extent of Resection. J. Clin. Med. 2021, 10, 236. [Google Scholar] [CrossRef]
- Cordova, J.S.; Gurbani, S.S.; Holder, C.A.; Olson, J.J.; Schreibmann, E.; Shi, R.; Guo, Y.; Shu, H.G.; Shim, H.; Hadjipanayis, C.G. Semi-Automated Volumetric and Morphological Assessment of Glioblastoma Resection with Fluorescence-Guided Surgery. Mol. Imaging Biol. 2016, 18, 454–462. [Google Scholar] [CrossRef]
- Bettag, C.; Schregel, K.; Langer, P.; Thomas, C.; Behme, D.; Stadelmann, C.; Rohde, V.; Mielke, D. Endoscope-Assisted Fluorescence-Guided Resection Allowing Supratotal Removal in Glioblastoma Surgery. Neurosurg. Focus 2021, 50, E3. [Google Scholar] [CrossRef] [PubMed]
- Pathways, T.; Manini, I.; Caponnetto, F.; Dalla, E.; Ius, T.; Maria, G.; Pepa, D.; Pegolo, E.; Bartolini, A.; la Rocca, G.; et al. Cancers Heterogeneity Matters: Different Regions of Glioblastoma Are Characterized by Distinctive. Cancers 2020, 12, 2960. [Google Scholar]
- Wachter, D.; Kallenberg, K.; Wrede, A. Fluorescence-Guided Operation in Recurrent Glioblastoma Multiforme Treated with Bevacizumab?—Fluorescence of the Noncontrast Enhancing Tumor Tissue? J. Neurol. Surg. Part A Central Eur. Neurosurg. 2012, 73, 401–406. [Google Scholar]
- Kamp, M.A.; Felsberg, J.; Sadat, H.; Kuzibaev, J.; Steiger, H.J.; Rapp, M.; Reifenberger, G.; Dibué, M.; Sabel, M. 5-ALA-Induced Fluorescence Behavior of Reactive Tissue Changes Following Glioblastoma Treatment with Radiation and Chemotherapy. Acta Neurochir. 2015, 157, 207–214. [Google Scholar] [CrossRef]
- Chohan, M.O.; Berger, M.S. 5-Aminolevulinic Acid Fluorescence Guided Surgery for Recurrent High-Grade Gliomas. J. Neurooncol. 2019, 141, 517–522. [Google Scholar] [CrossRef]
- Kiesel, B.; Mischkulnig, M.; Woehrer, A.; Martinez-Moreno, M.; Millesi, M.; Mallouhi, A.; Czech, T.; Preusser, M.; Hainfellner, J.A.; Wolfsberger, S.; et al. Systematic Histopathological Analysis of Different 5-Aminolevulinic Acid–Induced Fluorescence Levels in Newly Diagnosed Glioblastomas. J. Neurosurg. 2018, 129, 341–353. [Google Scholar] [CrossRef] [PubMed]
- Kamp, M.A.; Krause Molle, Z.; Munoz-Bendix, C.; Rapp, M.; Sabel, M.; Steiger, H.J.; Cornelius, J.F. Various Shades of Red—A Systematic Analysis of Qualitative Estimation of ALA-Derived Fluorescence in Neurosurgery. Neurosurg. Rev. 2018, 41, 3–18. [Google Scholar] [CrossRef] [PubMed]
- Mischkulnig, M.; Kiesel, B.; Borkovec, M.; Wadiura, L.I.; Benner, D.; Hosmann, A.; Hervey-Jumper, S.; Knosp, E.; Roessler, K.; Berger, M.S.; et al. High Interobserver Agreement in the Subjective Classification of 5-Aminolevulinic Acid Fluorescence Levels in Newly Diagnosed Glioblastomas. Lasers Surg. Med. 2020, 52, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Wada, S.; Eguchi, H.; Adachi, J.I.; Mishima, K.; Matsutani, M.; Nishikawa, R.; Nishiyama, M. Cadherin 13 Overexpression as an Important Factor Related to the Absence of Tumor Fluorescence in 5-Aminolevulinic Acid-Guided Resection of Glioma. J. Neurosurg. 2013, 119, 1331–1339. [Google Scholar] [CrossRef]
- Sánchez-Ortega, J.F.; Aguas-Valiente, J.; Sota-Ochoa, P.; Calatayud-Pérez, J.; Sánchez-Ortega, J.F. Glioblastoma with Primitive Neuronal Component: A Case Report and Considerations of Fluorescence-Guided Surgery. Surg. Neurol. Int. 2020, 11, 178. [Google Scholar] [CrossRef] [PubMed]
- Bonnin, D.A.A.; Havrda, M.C.; Lee, M.C.; Evans, L.; Ran, C.; Qian, D.C.; Harrington, L.X.; Valdes, P.A.; Cheng, C.; Amos, C.I.; et al. Characterizing the Heterogeneity in 5-Aminolevulinic Acid-Induced Fluorescence in Glioblastoma. J. Neurosurg. 2020, 132, 1706–1714. [Google Scholar] [CrossRef] [PubMed]
- Omoto, K.; Matsuda, R.; Nakagawa, I.; Motoyama, Y.; Nakase, H. Case Report False—Positive Inflammatory Change Mimicking Glioblastoma Multiforme under 5—Aminolevulinic Acid—Guided Surgery: A Case Report. Surg. Neuron. Int. 2018, 9, 49. [Google Scholar] [CrossRef]
- della Puppa, A.; Munari, M.; Gardiman, M.P.; Volpin, F. Combined Fluorescence Using 5-Aminolevulinic Acid and Fluorescein Sodium at Glioblastoma Border: Intraoperative Findings and Histopathologic Data About 3 Newly Diagnosed Consecutive Cases. World Neurosurg. 2019, 122, e856–e863. [Google Scholar] [CrossRef] [PubMed]
- Yano, H.; Nakayama, N.; Ohe, N.; Miwa, K.; Shinoda, J.; Iwama, T. Pathological Analysis of the Surgical Margins of Resected Glioblastomas Excised Using Photodynamic Visualization with Both 5-Aminolevulinic Acid and Fluorescein Sodium. J. Neurooncol. 2017, 133, 389–397. [Google Scholar] [CrossRef]
- Coburger, J.; Hagel, V.; Wirtz, C.R.; König, R. Surgery for Glioblastoma: Impact of the Combined Use of 5-Aminolevulinic Acid and Intraoperative MRI on Extent of Resection and Survival. PLoS ONE 2015, 10, e0131872. [Google Scholar] [CrossRef]
- Smith, E.J.; Gohil, K.; Thompson, C.M.; Naik, A.; Hassaneen, W. Fluorescein-Guided Resection of High-Grade Gliomas: A Meta-Analysis. World Neurosurg. 2021, 155, 181–188.e7. [Google Scholar] [CrossRef]
- Wang, L.M.; Banu, M.A.; Canoll, P.; Bruce, J.N. Rationale and Clinical Implications of Fluorescein-Guided Supramarginal Resection in Newly Diagnosed High-Grade Glioma. Front. Oncol. 2021, 11, 666734. [Google Scholar] [CrossRef]
- Diaz, R.J.; Dios, R.R.; Hattab, E.M.; Burrell, K.; Rakopoulos, P.; Sabha, N.; Hawkins, C.; Zadeh, G.; Rutka, J.T.; Cohen-gadol, A.A. Study of the Biodistribution of Fluorescein in Glioma-Infiltrated Mouse Brain and Histopathological Correlation of Intraoperative Findings in High-Grade Gliomas Resected under Fluorescein Fluorescence Guidance. J. Neurosurg. 2015, 122, 1360–1369. [Google Scholar] [CrossRef] [PubMed]
- Waqas, M.; Shamim, M.S. Sodium Fluorescein Guided Resection of Malignant Glioma. J. Pak. Med. Assoc. 2018, 68, 968–970. [Google Scholar] [PubMed]
- Schipmann, S.; Schwake, M.; Suero Molina, E.; Stummer, W. Markers for Identifying and Targeting Glioblastoma Cells during Surgery. J. Neurol. Surg. A Cent. Eur. Neurosurg. 2019, 80, 475–487. [Google Scholar] [CrossRef] [PubMed]
- Acerbi, F.; Broggi, M.; Schebesch, K.M.; Höhne, J.; Cavallo, C.; de Laurentis, C.; Eoli, M.; Anghileri, E.; Servida, M.; Boffano, C.; et al. Fluorescein-Guided Surgery for Resection of High-Grade Gliomas: A Multicentric Prospective Phase II Study (FLUOGLIO). Clin. Cancer Res. 2018, 24, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Katsevman, G.A.; Turner, R.C.; Urhie, O.; Voelker, J.L.; Bhatia, S. Utility of Sodium Fluorescein for Achieving Resection Targets in Glioblastoma: Increased Gross- or near-Total Resections and Prolonged Survival. J. Neurosurg. 2019, 132, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Kutlay, M.; Durmaz, O.; Ozer, İ.; Kırık, A.; Yasar, S.; Kural, C.; Temiz, Ç.; Tehli, Ö.; Ezgu, M.C.; Daneyemez, M.; et al. Fluorescein Sodium-Guided Neuroendoscopic Resection of Deep-Seated Malignant Brain Tumors: Preliminary Results of 18 Patients. Oper Neurosurg. 2021, 20, 206–218. [Google Scholar] [CrossRef]
- Fan, C.; Jiang, Y.; Liu, R.; Wu, G.; Wu, G.; Xu, K.; Miao, Z. Safety and Feasibility of Low-Dose Fl Uorescein-Guided Resection of Glioblastoma. Clin. Neurol. Neurosurg. 2018, 175, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Höhne, J.; Schebesch, K.M.; de Laurentis, C.; Akçakaya, M.O.; Pedersen, C.B.; Brawanski, A.; Poulsen, F.R.; Kiris, T.; Cavallo, C.; Broggi, M.; et al. Fluorescein Sodium in the Surgical Treatment of Recurrent Glioblastoma Multiforme. World Neurosurg. 2019, 125, e158–e164. [Google Scholar] [CrossRef]
- Bowden, S.G.; Neira, J.A.; Gill, B.J.A.; Ung, T.H.; Englander, Z.K.; Zanazzi, G.; Chang, P.D.; Samanamud, J.; Grinband, J.; Sheth, S.A.; et al. Sodium Fluorescein Facilitates Guided Sampling of Diagnostic Tumor Tissue in Nonenhancing Gliomas. Neurosurgery 2018, 82, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Schebesch, K.-M.; Höhne, J.; Rosengarth, K.; Noeva, E.; Schmidt, N.O.; Proescholdt, M. Fluorescein-Guided Resection of Newly Diagnosed High-Grade Glioma: Impact on Extent of Resection and Outcome. Brain Spine 2022, 2, 101690. [Google Scholar] [CrossRef]
- Willems, P.W.A.; Taphoorn, M.J.B.; Burger, H.; van der Sprenkel, J.W.B.; Tulleken, C.A.F. Effectiveness of Neuronavigation in Resecting Solitary Intracerebral Contrast-Enhancing Tumors: A Randomized Controlled Trial. J. Neurosurg. 2006, 104, 360–368. [Google Scholar] [CrossRef]
- Orringer, D.A.; Golby, A.; Jolesz, F. Neuronavigation in the Surgical Management of Brain Tumors: Current and Future Trends. Expert Rev. Med. Devices 2012, 9, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Walter, J.; Kuhn, S.A.; Waschke, A.; Kalff, R.; Ewald, C. Operative Treatment of Subcortical Metastatic Tumours in the Central Region. J. Neurooncol. 2011, 103, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Kubben, P.L.; Scholtes, F.; Schijns, O.E.M.G.; ter Laak-Poort, M.P.; Teernstra, O.P.M.; Kessels, A.G.H.; van Overbeeke, J.J.; Martin, D.H.; van Santbrink, H. Intraoperative Magnetic Resonance Imaging versus Standard Neuronavigation for the Neurosurgical Treatment of Glioblastoma: A Randomized Controlled Trial. Surg. Neurol. Int. 2014, 5, 70. [Google Scholar] [CrossRef]
- Castellano, A.; Bello, L.; Michelozzi, C.; Gallucci, M.; Fava, E.; Iadanza, A.; Riva, M.; Casaceli, G.; Falini, A. Role of Diffusion Tensor Magnetic Resonance Tractography in Predicting the Extent of Resection in Glioma Surgery. Neuro Oncol. 2012, 14, 192–202. [Google Scholar] [CrossRef]
- Toescu, S.M.; Hales, P.W.; Tisdall, M.M.; Aquilina, K.; Clark, C.A. Neurosurgical Applications of Tractography in the UK. Br. J. Neurosurg. 2021, 35, 424–429. [Google Scholar] [CrossRef]
- Gulati, S.; Berntsen, E.M.; Solheim, O.; Kvistad, K.A.; Håberg, A.; Selbekk, T.; Torp, S.H.; Unsgaard, G. Surgical Resection of High-Grade Gliomas in Eloquent Regions Guided by Blood Oxygenation Level Dependent Functional Magnetic Resonance Imaging, Diffusion Tensor Tractography, and Intraoperative Navigated 3D Ultrasound. Minim Invasive Neurosurg. 2009, 52, 17–24. [Google Scholar] [CrossRef]
- Vassal, F.; Schneider, F.; Sontheimer, A.; Lemaire, J.J.; Nuti, C. Intraoperative Visualisation of Language Fascicles by Diffusion Tensor Imaging-Based Tractography in Glioma Surgery. Acta Neurochir. 2013, 155, 437–448. [Google Scholar] [CrossRef]
- Wu, J.-S.; Mao, Y.; Zhou, L.-F.; Tang, W.-J.; Hu, J.; Song, Y.-Y.; Hong, X.-N.; Du, G.-H. Clinical evaluation and follow-up outcome of diffusion tensor imaging-based functional neuronavigation: A prospective, controlled study in patients with gliomas involving pyramidal tracts clinical studies. Neurosurgery 2007, 61, 935. [Google Scholar] [CrossRef] [PubMed]
- Zhylka, A.; Sollmann, N.; Kofler, F.; Radwan, A.; de Luca, A.; Gempt, J.; Wiestler, B.; Menze, B.; Krieg, S.M.; Zimmer, C.; et al. Tracking the Corticospinal Tract in Patients with High-Grade Glioma: Clinical Evaluation of Multi-Level Fiber Tracking and Comparison to Conventional Deterministic Approaches. Front. Oncol. 2021, 11, 761169. [Google Scholar] [CrossRef] [PubMed]
- Sparacia, G.; Parla, G.; lo Re, V.; Cannella, R.; Mamone, G.; Carollo, V.; Midiri, M.; Grasso, G. Resting-State Functional Connectome in Patients with Brain Tumors Before and After Surgical Resection. World Neurosurg. 2020, 141, e182–e194. [Google Scholar] [CrossRef] [PubMed]
- Sparacia, G.; Parla, G.; Mamone, G.; Caruso, M.; Torregrossa, F.; Grasso, G. Resting-State Functional Magnetic Resonance Imaging for Surgical Neuro-Oncology Planning: Towards a Standardization in Clinical Settings. Brain Sci. 2021, 11, 1613. [Google Scholar] [CrossRef] [PubMed]
- Sparacia, G.; Parla, G.; Cannella, R.; Perri, A.; lo Re, V.; Mamone, G.; Miraglia, R.; Torregrossa, F.; Grasso, G. Resting-State Functional Magnetic Resonance Imaging for Brain Tumor Surgical Planning: Feasibility in Clinical Setting. World Neurosurg. 2019, 131, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Morales, H. Current and Future Challenges of Functional MRI and Diffusion Tractography in the Surgical Setting: From Eloquent Brain Mapping to Neural Plasticity. Semin. Ultrasound CT MRI 2021, 42, 474–489. [Google Scholar] [CrossRef] [PubMed]
- Unsgaard, G.; Gronningsaeter, A.; Ommedal, S.; Nagelhus Hernes, T.A.; Schramm, J.; van Roost, D.; Chandler, W.F.; Langmoen, I.A.; Kelly, P.J. Brain Operations Guided by Real-Time Two-Dimensional Ultrasound: New Possibilities as a Result of Improved Image Quality. Neurosurgery 2002, 51, 402–412. [Google Scholar] [CrossRef] [PubMed]
- del Bene, M.; Perin, A.; Casali, C.; Legnani, F.; Saladino, A.; Mattei, L.; Vetrano, I.G.; Saini, M.; DiMeco, F.; Prada, F. Advanced Ultrasound Imaging in Glioma Surgery: Beyond Gray-Scale B-Mode. Front. Oncol. 2018, 8, 576. [Google Scholar] [CrossRef] [PubMed]
- Prada, F.; Perin, A.; Martegani, A.; Aiani, L.; Solbiati, L.; Lamperti, M.; Casali, C.; Legnani, F.; Mattei, L.; Saladino, A.; et al. Intraoperative Contrast-Enhanced Ultrasound for Brain Tumor Surgery. Neurosurgery 2014, 74, 542–552. [Google Scholar] [CrossRef] [PubMed]
- Prada, F.; Mattei, L.; del Bene, M.; Aiani, L.; Saini, M.; Casali, C.; Filippini, A.; Legnani, F.G.; Perin, A.; Saladino, A.; et al. Intraoperative Cerebral Glioma Characterization with Contrast Enhanced Ultrasound. Biomed. Res. Int. 2014, 2014, 484261. [Google Scholar] [CrossRef]
- Prada, F.; del Bene, M.; Fornaro, R.; Vetrano, I.G.; Martegani, A.; Aiani, L.; Sconfienza, L.M.; Mauri, G.; Solbiati, L.; Pollo, B.; et al. Identification of Residual Tumor with Intraoperative Contrast-Enhanced Ultrasound during Glioblastoma Resection. Neurosurg. Focus 2016, 40, E7. [Google Scholar] [CrossRef]
- Prada, F.; Vitale, V.; del Bene, M.; Boffano, C.; Sconfienza, L.M.; Pinzi, V.; Mauri, G.; Solbiati, L.; Sakas, G.; Kolev, V.; et al. Contrast-Enhanced MR Imaging versus Contrast-Enhanced US: A Comparison in Glioblastoma Surgery by Using Intraoperative Fusion Imaging. Radiology 2017, 285, 242–249. [Google Scholar] [CrossRef]
- Wang, J.; Liu, X.; Ba, Y.M.; Yang, Y.L.; Gao, G.D.; Wang, L.; Duan, Y.Y. Effect of sonographically guided cerebral glioma surgery on survival time. J. Ultrasound Med. 2012, 31, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Prada, F.; del Bene, M.; Mattei, L.; Lodigiani, L.; Debeni, S.; Kolev, V.; Vetrano, I.; Solbiati, L.; Sakas, G.; Dimeco, F. Preoperative Magnetic Resonance and Intraoperative Ultrasound Fusion Imaging for Real-Time Neuronavigation in Brain Tumor Surgery. Ultraschall Der Med. 2014, 9, 174–186. [Google Scholar] [CrossRef]
- Prada, F.; del Bene, M.; Mattei, L.; Casali, C.; Filippini, A.; Legnani, F.; Mangraviti, A.; Saladino, A.; Perin, A.; Richetta, C.; et al. Fusion Imaging for Intra-Operative Ultrasound-Based Navigation in Neurosurgery. J. Ultrasound 2014, 17, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Bal, J.; Camp, S.J.; Nandi, D. The Use of Ultrasound in Intracranial Tumor Surgery. Acta Neurochir. 2016, 158, 1179–1185. [Google Scholar] [PubMed]
- Unsgaard, G.; Rygh, O.M.; Selbekk, T.; Müller, T.B.; Kolstad, F.; Lindseth, F.; Hernes, T.A.N. Intra-Operative 3D Ultrasound in Neurosurgery. Acta Neurochir. 2006, 148, 235–253. [Google Scholar]
- Mahboob, S.; McPhillips, R.; Qiu, Z.; Jiang, Y.; Meggs, C.; Schiavone, G.; Button, T.; Desmulliez, M.; Demore, C.; Cochran, S.; et al. Intraoperative Ultrasound-Guided Resection of Gliomas: A Meta-Analysis and Review of the Literature. World Neurosurg. 2016, 92, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Barak, T.; Vetsa, S.; Nadar, A.; Jin, L.; Gupte, T.P.; Fomchenko, E.I.; Miyagishima, D.F.; Yalcin, K.; Vasandani, S.; Gorelick, E.; et al. Surgical Strategies for Older Patients with Glioblastoma. J. Neurooncol. 2021, 155, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Rogers, C.M.; Jones, P.S.; Weinberg, J.S. Intraoperative MRI for Brain Tumors. J. Neurooncol. 2021, 151, 479–490. [Google Scholar] [CrossRef] [PubMed]
- Ille, S.; Schroeder, A.; Wagner, A.; Negwer, C.; Kreiser, K.; Meyer, B.; Krieg, S.M. Intraoperative MRI–Based Elastic Fusion for Anatomically Accurate Tractography of the Corticospinal Tract: Correlation with Intraoperative Neuromonitoring and Clinical Status. Neurosurg. Focus 2021, 50, E9. [Google Scholar] [CrossRef] [PubMed]
- Bander, E.D.; Magge, R.; Ramakrishna, R. Advances in Glioblastoma Operative Techniques. World Neurosurg. 2018, 116, 529–538. [Google Scholar] [CrossRef]
- Noh, T.; Mustroph, M.; Golby, A.J. Intraoperative Imaging for High-Grade Glioma Surgery. Neurosurg. Clin. N. Am. 2021, 32, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Hatiboglu, M.A.; Weinberg, J.S.; Suki, D.; Rao, G.; Prabhu, S.S.; Shah, K.; Jackson, E.; Sawaya, R. Impact of Intraoperative High-Field Magnetic Resonance Imaging Guidance on Glioma Surgery: A Prospective Volumetric Analysis. Neurosurgery 2009, 64, 1073–1081. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, M.; Vaz, G.; Lawson, T.M.; Docquier, M.A.; van Maanen, A.; Duprez, T.; Raftopoulos, C. Glioblastoma Surgery with and without Intraoperative MRI at 3.0T. Neurochirurgie 2014, 60, 143–150. [Google Scholar] [CrossRef]
- Golub, D.; Hyde, J.; Dogra, S.; Nicholson, J.; Kirkwood, K.A.; Gohel, P.; Loftus, S.; Schwartz, T.H. Intraoperative MRI versus 5-ALA in High-Grade Glioma Resection: A Network Meta-Analysis. J. Neurosurg. 2021, 134, 484–498. [Google Scholar] [CrossRef] [PubMed]
- Khan, I.; Waqas, M.; Shamim, M.S. Role of Intra-Operative MRI (IMRI) in Improving Extent of Resection and Survival in Patients with Glioblastoma Multiforme. J. Pak. Med. Assoc. 2017, 67, 1121–1123. [Google Scholar]
- Kuhnt, D.; Becker, A.; Ganslandt, O.; Bauer, M.; Buchfelder, M.; Nimsky, C. Correlation of the Extent of Tumor Volume Resection and Patient Survival in Surgery of Glioblastoma Multiforme with High-Field Intraoperative MRI Guidance. Neuro. Oncol. 2011, 13, 1339–1348. [Google Scholar] [CrossRef] [PubMed]
- Staartjes, V.E.; Togni-Pogliorini, A.; Stumpo, V.; Serra, C.; Regli, L. Impact of Intraoperative Magnetic Resonance Imaging on Gross Total Resection, Extent of Resection, and Residual Tumor Volume in Pituitary Surgery: Systematic Review and Meta-Analysis. Pituitary 2021, 24, 644–656. [Google Scholar] [CrossRef] [PubMed]
- Heßelmann, V.; Mager, A.-K.; Goetz, C.; Detsch, O.; Theisgen, H.-K.; Friese, M.; Schwindt, W.; Gottschalk, J.; Kremer, P. Accuracy of High-Field Intraoperative MRI in the Detectability of Residual Tumor in Glioma Grade IV Resections. RöFo Fortschr. Geb. Röntgenstrahlen Bildgeb. Verfahr. 2017, 189, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Dodo, K.; Fujita, K.; Sodeoka, M. Raman Spectroscopy for Chemical Biology Research. J. Am. Chem. Soc. 2022, 144, 19651–19667. [Google Scholar] [CrossRef] [PubMed]
- Broadbent, B.; Tseng, J.; Kast, R.; Noh, T.; Brusatori, M.; Kalkanis, S.N.; Auner, G.W. Shining Light on Neurosurgery Diagnostics Using Raman Spectroscopy. J. Neurooncol. 2016, 130, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Livermore, L.J.; Isabelle, M.; Bell, I.M.; Edgar, O.; Voets, N.L.; Stacey, R.; Ansorge, O.; Vallance, C.; Plaha, P. Raman Spectroscopy to Differentiate between Fresh Tissue Samples of Glioma and Normal Brain: A Comparison with 5-ALA–Induced Fluorescence-Guided Surgery. J. Neurosurg. 2021, 135, 469–479. [Google Scholar] [CrossRef]
- le Reste, P.; Pilalis, E.; Aubry, M.; McMahon, M.; Cano, L.; Etcheverry, A.; Chatziioannou, A.; Chevet, E.; Fautrel, A. Integration of Raman Spectra with Transcriptome Data in Glioblastoma Multiforme Defines Tumour Subtypes and Predicts Patient Outcome. J. Cell. Mol. Med. 2021, 25, 10846–10856. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Liu, C.-H.; Wu, B.; Yu, X.; Cheng, G.; Zhu, K.; Wang, K.; Zhang, C.; Zhao, M.; Zong, R.; et al. Optical Biopsy Identification and Grading of Gliomas Using Label-Free Visible Resonance Raman Spectroscopy. J. Biomed. Opt. 2019, 24, 1. [Google Scholar] [CrossRef] [PubMed]
- Iturrioz-Rodríguez, N.; de Pasquale, D.; Fiaschi, P.; Ciofani, G. Discrimination of Glioma Patient-Derived Cells from Healthy Astrocytes by Exploiting Raman Spectroscopy. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2022, 269, 120773. [Google Scholar] [CrossRef] [PubMed]
- Kast, R.; Auner, G.; Yurgelevic, S.; Broadbent, B.; Raghunathan, A.; Poisson, L.M.; Mikkelsen, T.; Rosenblum, M.L.; Kalkanis, S.N. Identification of Regions of Normal Grey Matter and White Matter from Pathologic Glioblastoma and Necrosis in Frozen Sections Using Raman Imaging. J. Neurooncol. 2015, 125, 287–295. [Google Scholar] [CrossRef]
- Grasso, G.; Torregrossa, F. Magnetic Resonance Spectrobiopsy for Prediction of Isocitrate Dehydrogenase Mutation in Glioma. World Neurosurg. 2020, 134, 187–189. [Google Scholar] [CrossRef]
- Hollon, T.; Lewis, S.; Freudiger, C.W.; Sunney Xie, X.; Orringer, D.A. Improving the Accuracy of Brain Tumor Surgery via Raman-Based Technology. Neurosurg. Focus 2016, 40, E9. [Google Scholar] [CrossRef]
- Villard, A.; Breuskin, I.; Casiraghi, O.; Asmandar, S.; Laplace-Builhe, C.; Abbaci, M.; Moya Plana, A. Confocal Laser Endomicroscopy and Confocal Microscopy for Head and Neck Cancer Imaging: Recent Updates and Future Perspectives. Oral Oncol. 2022, 127, 105826. [Google Scholar] [CrossRef]
- Kakaletri, I.; Linxweiler, M.; Ajlouni, S.; Charalampaki, P. Development, Implementation and Application of Confocal Laser Endomicroscopy in Brain, Head and Neck Surgery—A Review. Diagnostics 2022, 12, 2697. [Google Scholar] [CrossRef] [PubMed]
- Restelli, F.; Pollo, B.; Vetrano, I.G.; Cabras, S.; Broggi, M.; Schiariti, M.; Falco, J.; de Laurentis, C.; Raccuia, G.; Ferroli, P.; et al. Confocal Laser Microscopy in Neurosurgery: State of the Art of Actual Clinical Applications. J. Clin. Med. 2021, 10, 2035. [Google Scholar] [CrossRef]
- Höhne, J.; Schebesch, K.-M.; Zoubaa, S.; Proescholdt, M.; Riemenschneider, M.J.; Schmidt, N.O. Intraoperative Imaging of Brain Tumors with Fluorescein: Confocal Laser Endomicroscopy in Neurosurgery. Clinical and User Experience. Neurosurg. Focus 2021, 50, E19. [Google Scholar] [CrossRef] [PubMed]
- Martirosyan, N.L.; Eschbacher, J.M.; Kalani, M.Y.S.; Turner, J.D.; Belykh, E.; Spetzler, R.F.; Nakaji, P.; Preul, M.C. Prospective Evaluation of the Utility of Intraoperative Confocal Laser Endomicroscopy in Patients with Brain Neoplasms Using Fluorescein Sodium: Experience with 74 Cases. Neurosurg. Focus 2016, 40, E11. [Google Scholar] [CrossRef]
- Abramov, I.; Park, M.T.; Belykh, E.; Dru, A.B.; Xu, Y.; Gooldy, T.C.; Scherschinski, L.; Farber, S.H.; Little, A.S.; Porter, R.W.; et al. Intraoperative Confocal Laser Endomicroscopy: Prospective in Vivo Feasibility Study of a Clinical-Grade System for Brain Tumors. J. Neurosurg. 2022, 1, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Belykh, E.; Cavallo, C.; Gandhi, S.; Zhao, X.; Veljanoski, D.; Izady Yazdanabadi, M.; Martirosyan, N.L.; Byvaltsev, V.A.; Eschbacher, J.; Preul, M.C.; et al. Utilization of Intraoperative Confocal Laser Endomicroscopy in Brain Tumor Surgery. J. Neurosurg. Sci. 2018, 62, 704–717. [Google Scholar] [CrossRef] [PubMed]
- Restelli, F.; Mathis, A.M.; Höhne, J.; Mazzapicchi, E.; Acerbi, F.; Pollo, B.; Quint, K. Confocal Laser Imaging in Neurosurgery: A Comprehensive Review of Sodium Fluorescein-Based CONVIVO Preclinical and Clinical Applications. Front. Oncol. 2022, 12, 998384. [Google Scholar] [CrossRef]


{kind=link}
| Author, Year | Country | Study Design | N° Patients | M/F Ratio | Age (Mean) |
|---|---|---|---|---|---|
| Sollmann N. et al., 2018 [22] | Germany | Prospective study | 60 | 1.72 | 47.6 |
| Neira J.A. et al., 2017 [23] | USA | Prospective study | 32 | 1 | 63.9 |
| Marongiu A. et al., 2017 [24] | Italy | Retrospective study | 114 | 1.15 | 62.3 |
| Moiraghi A. et al., 2019 [25] | Italy, Switzerland | Case series | 60 | 1.72 | 55.32 |
| Barbagallo G.M.V. et al., 2021 [26] | Italy | Retrospective study | 100 | 0.88 | 64 |
| Incekara F. et al., 2021 [27] | Netherlands | Randomized controlled trial | 50 | 1.47 | 63 |
| Barbagallo G.M.V. et al., 2021 [28] | Italy | Retrospective study | 20 | 1.5 | 54.5 |
| Bassaganyas-Vancells C. et al., 2019 [29] | Spain | Retrospective study | 118 | 1.51 | N/A |
| Nickel K. et al., 2017 [30] | Germany | Multicenter cross sectional study | 170 | 1.46 | 55 |
| Luzzi S. et al., 2021 [31] | Italy | Retrospective study | 117 | 1.43 | 55 |
| Raffa G. et al., 2019 [32] | Italy | Retrospective study | 82 | 1.56 | 58 |
| Chen D. et al., 2019 [33] | China | Retrospective study | 95 | 0.9 | 48.5 |
| Hong J. et al., 2019 [34] | China | Retrospective study | 82 | 1.1 | 51 |
| Francaviglia N. et al., 2017 [35] | Italy | Retrospective study | 47 | 1.13 | 60.3 |
| Lu M. et al., 2020 [36] | China | Retrospective study | 46 | 1.3 | 45.1 |
| Picart T. et al., 2017 [37] | France | Retrospective study | 51 | 1.28 | 47 |
| Bettag C. et al., 2020 [38] | Germany | Retrospective study | 20 | 2 | 72 |
| Catapano G. et al., 2017 [39] | Italy | Retrospective study | 48 | 1.52 | 57 |
| Author, Year | Number of Patients with HGG (Number of GBM) | Intraoperative Technique | Preoperative Mean Tumoral Volume (cm3) | % of Eloquent Area HGG | Surgical Outcomes (EOR or GTR) | Functional Outcomes | Follow up (mo) |
|---|---|---|---|---|---|---|---|
| SOLLMANN N. et al., 2018 [22] | 46 (21) | AS; nTMS-based DTI-FT; DES; IONM | ~26.51 | 100% | GTR: 80% | Mean KPS: Preop 90; Postop 85; FU 90 | 3 |
| NEIRA J.A. et al., 2017 [23] | 20 (18) | NN; SF | N/A | N/A | GTR: 93.1% | Mean KPS (GBM group only): Preop 85.5; Postop 81.5 | N/A |
| MARONGIU A. et al., 2017 [24] | 78 (78) A group 35 (35) B group | ioMRI; NN and DTI (A) vs. NN; preoperative MRI and DTI (B) | 28.4 (A) 30.6 (B) | 62.8% (A) 30.6% (B) | GTR: 88.5% (A group) 44.4% (B group) | KPS (at discharge): Improved in 20.5% (A group) Improved in 13.8% (B group) | 1, 3, 6 |
| MOIRAGHI A. et al., 2019 [25] | 60 (51) 31 (N-ioUS groups) 29 (standard NN) | N-ioUS and preoperative mri vs. standard NN and preoperative MRI | 36.69 36.21 (N-ioUS) 37.14 (standard NN) | 33.3% 31% (N-ioUS) 35.5% (standard NN) | EOR (only GBM group): ~96% NN group ~97% N-ioUS group | ΔKPS (only GBM group): ~6 for the N-ioUS group (p < 0.01 for GBM cohort) ~5 for the NN (p < 0.01 for GBM cohort) | N/A |
| BARBAGALLO G.M. V. et al., 2021 [26] | 100 (92) A: 48 (45) (=>65 years old) B: 52 (47) (<65 years old) | 5-ALA; NN; MEP; SEP; DES; i-CT; NN; IoUS | ~42.45 | N/A | GTR obtained in: 93.8% (>65 y) 92.3% (<65 y) | KPS: Preoperative: 73.3 (A) vs. 76.5 (B) Postoperative ~74 (A) vs. ~75 (B) | 5 |
| INCEKARA F. et al., 2021 [27] | 47 (47) 23 in IoUS guided surgery vs. 24 in standard NN | IoUS vs. NN | 38.6 (IoUS group) 32.3 (standard NN group) | 39.0% (IoUS group) 42.0% (standard NN group) | Median EOR: 97% (IoUS group) 95% (standard NN group) | Mean KPS, (at pre and post operative FU) IoUS group: Preop 90; Postop 90; 90; 90 NN group: Preop 90, Postop 90; 90; 70. | 7 weeks, 3, 6 |
| BARBAGALLO G.M.V. et al., 2021 [28] | 20 (18) | NN; iCT; 5-ALA; IoUS; IONM; DES; DTI | N/A | 100% | EOR: 100% in all except 2 patients | Mean KPS: Preop 80; Postop 75 and then 70 (last FU) | 120 (one long survivors) |
| BASSAGANYAS-VANCELLS C. et al., 2019 [29] | 60 (52) 5 ALA group 19 (9) IoMRI group 39 (36) IoMRI + 5-ALA group | 5-ALA vs. IoMRI vs. 5-ALA + IoMRI | N/A | 26.7% (5-ALA group) 42.1% (IoMRI group) 35.9% (5-ALA + IoMRI group) | EOR => 90%: 75% (5-ALA group) 73.7% (IoMRI group) 71.8% (IoMRI + 5-ALA group) | Mean KPS: 5-ALA: Preop 87.8; Postop 82.6 IoMRI: Preop 91.6; Postop 86.8 5-ALA + IoMRI: Preop 89.7; Postop 85.4 | 1 |
| NICKEL K. et al., 2017 [30] | 170 (123) | AS; 5-ALA; IoMRI (in various combination) | N/A | 53.5% | Mean EOR: 95% (5-ALA and IoMRI) 94% (IoMRI) 74% (5-ALA) | Mean KPS: AS group: Preop 45.6 and Postop 64.4 5-ALA + IoMRI: Preop 50.2 and Postop 72.3 Mean postop EORTC: AS: 53.4; IoMRI + 5-ALA: 65.5; IoMRI 63.2; 5-ALA 59.9; no imaging 56.5. | 12 |
| LUZZI S. et al., 2021 [31] | 117 (95) 54 (32) AR HDFT group 63 (53) standard NN group | AR HDFT + SF vs. NN, brain mapping and SF | 12.5 (AR HDFT group) 15.1 (standard NN group) | N/A | EOR: GTR + NTR: 85% (AR HDFT + SF group) GTR + NTR: 65% (control group) | Mean NANO score: AR HDFT group: Preop 5.1 ± 2; Postop 3.8 ± 2 Control group: preop 4.9 ± 2; post op 5.2± 4 | 12.2 |
| RAFFA G, et al., 2019 [32] | 82 (59) 41 (31)–multimodal group 41 (28)–control group | nTMS, SF, IONM (multimodal group) vs. control group | 20.3 (multimodal group) 21.1 (control group) | 100% | EOR: GTR: 73.17% (group multimodal) GTR: 51.22% (control group) | KPS at 3 months FU: Multimodal group: stable in 58.54%; improved in 29.27% Control group: stable in 53.66%, improved in 14.63% | 3 |
| CHEN D. et al., 2019 [33] | 95 (44) | DTI and SF (observation group) vs. control | 73.8 (in observation group) 69.2 (in control group) | 100% | GTR: In 83.6% (observation group) In 45.6% (control group) | KPS Post op: improved in 73.4% (observation group) Post op: improved in 47.8% (control group) | 1 |
| HONG J. et al., 2019 [34] | 82 (36) 42 (18)–fluorescein group 40 (18)–no fluorescein group | SF vs. no SF group | 31.2 (SF group) 30.1 (no SF group) | N/A | EOR: GTR obtained in 85.7% in SF group GTR obtained in 62.5% in no SF group | Mean KPS: SF group: 82 No SF: 75 | 6 |
| FRANCAVIGLIA N. et al., 2017 [35] | 47 (33) | SF | N/A | N/A | EOR: GTR obtained in 53.2% | Mean KPS: Preop: 85.1; Postop 83.4. | 10.2 |
| LU M. et al., 2020 [36] | 46 (46) 18 (18) (AS group) 28 (28) (AS and SF) | AS + SF vs. AS alone | 55.84 (total) 60.47 (AS) 53.13 (AS and SF) | 58.7% (total) 30.4% (AS) 28.3% (AS and SF) | EOR: GTR obtained in 100%; a median of 31.90% resection of T2 flair hyperintensity (AS + SF group) GTR obtained in 100%; a median of 16.04% resection of T2 flair hyperintensity (AS alone group) | Mean KPS: AS + SF group: Preop 78.62; Postop 97. AS group: Preop 80; Postop 72. | 1 |
| PICART T. et al., 2017 [37] | 51 (51) 24 (24) 5-ALA group 27 (27) white light group | 5-ALA vs. white light | 64.53 (5-ALA group) 78.51 (white light group) | 100% | EOR GTR obtained in 67.7% of patients of 5-ALA group GTR obtained in 51.8% of white light group | Mean KPS 5-ALA group: Preop 78.3; Postop 78.5 White light group: Preop 72.6; Postop 74.8 | 3 |
| BETTAG C. et al., 2020 [38] | 20 (20) | 5-ALA | 29.15 | N/A | EOR: GTR obtained in 95% of patients | Mean KPS: Post op 89.3 | N/A |
| CATAPANO G. et al., 2017 [39] | 48 (46) 23 (22) SF group 25 (24) control group | SF vs. no SF guidance | 30.3 (SF group) 34.9 (control group) | 17.3% (SF group) 20% (control group) | EOR: GTR obtained in 82.6% (SF group) GTR obtained in 52% (control group) | Mean KPS: SF group: Preop 80.4; Postop 76.1 Control group: Preop 79.2; Postop 74.8 | N/A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonosi, L.; Marrone, S.; Benigno, U.E.; Buscemi, F.; Musso, S.; Porzio, M.; Silven, M.P.; Torregrossa, F.; Grasso, G. Maximal Safe Resection in Glioblastoma Surgery: A Systematic Review of Advanced Intraoperative Image-Guided Techniques. Brain Sci. 2023, 13, 216. https://doi.org/10.3390/brainsci13020216
Bonosi L, Marrone S, Benigno UE, Buscemi F, Musso S, Porzio M, Silven MP, Torregrossa F, Grasso G. Maximal Safe Resection in Glioblastoma Surgery: A Systematic Review of Advanced Intraoperative Image-Guided Techniques. Brain Sciences. 2023; 13(2):216. https://doi.org/10.3390/brainsci13020216
Chicago/Turabian StyleBonosi, Lapo, Salvatore Marrone, Umberto Emanuele Benigno, Felice Buscemi, Sofia Musso, Massimiliano Porzio, Manikon Poullay Silven, Fabio Torregrossa, and Giovanni Grasso. 2023. "Maximal Safe Resection in Glioblastoma Surgery: A Systematic Review of Advanced Intraoperative Image-Guided Techniques" Brain Sciences 13, no. 2: 216. https://doi.org/10.3390/brainsci13020216
APA StyleBonosi, L., Marrone, S., Benigno, U. E., Buscemi, F., Musso, S., Porzio, M., Silven, M. P., Torregrossa, F., & Grasso, G. (2023). Maximal Safe Resection in Glioblastoma Surgery: A Systematic Review of Advanced Intraoperative Image-Guided Techniques. Brain Sciences, 13(2), 216. https://doi.org/10.3390/brainsci13020216