
Enhancing the Quality of Life of Patients with Multiple Sclerosis: Promising Results on the Role of Cognitive Tele-Rehabilitation Plus Virtual Reality

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Ethics
2.3. Procedures
- -
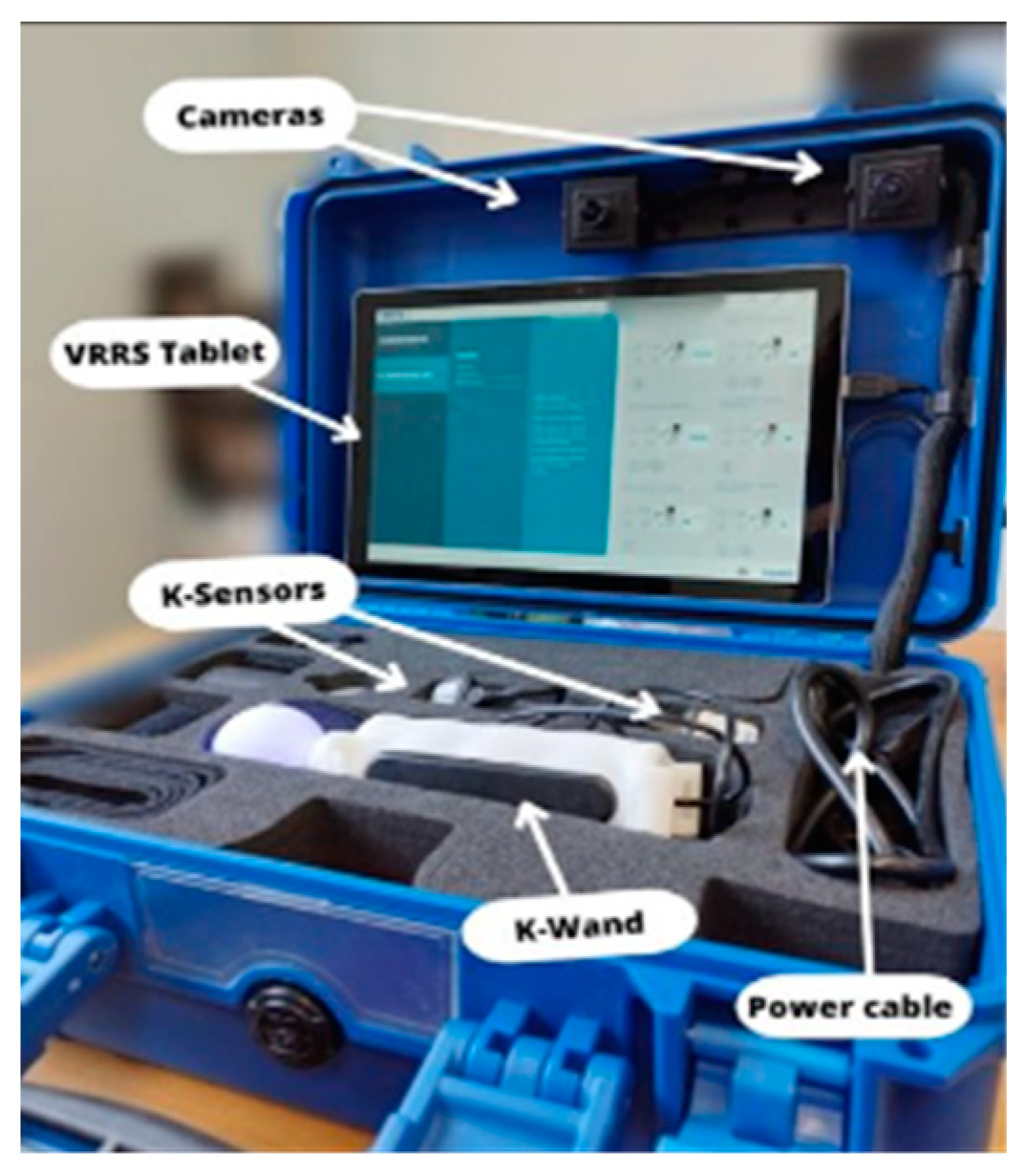
- 2-D Exercises: Patients engage with objects and scenarios through either the touchscreen interface or a specialized magnetic tracking sensor paired with a compressible object. This setup effectively emulates mouse-like interaction skills, enhancing the overall user experience.
- -
- 3-D Exercises: Within this category, patients immerse themselves in three-dimensional scenarios, interacting with virtual objects. This interaction is facilitated by a magnetic tracking sensor positioned above the hand, allowing for precise tracking of the 3-D position of the final effector.
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ghasemi, N.; Razavi, S.; Nikzad, E. Multiple sclerosis: Pathogenesis, symptoms, diagnoses and cell-based therapy. Cell J. 2017, 19, 1–10. [Google Scholar] [PubMed]
- Trojano, M.; Amato, M.P. Multiple sclerosis in 2017: Progress in multiple sclerosis –from diagnosis to therapy. Nat. Rev. Neurol. 2018, 14, 72–74. [Google Scholar] [CrossRef] [PubMed]
- Jeong, I.C.; Karpatkin, H.; Finkelstein, J. Physical Telerehabilitation Improves Quality of Life in Patients with Multiple Sclerosis. Stud. Health Technol. Inform. 2021, 284, 384–388. [Google Scholar] [PubMed]
- Gil Moreno, M.J.; Cerezo García, M.; Marasescu, R.; Pinel González, A.; Lopez Alvarez, L.; Aladro Benito, Y. Neuropsychological syndromes in multiple sclerosis. Psicothema 2012, 25, 452–460. [Google Scholar]
- Frau, J.; Mulasso, A.; Coghe, G.; Melis, M.; Beratto, L.; Cuomo, S.; Lorefice, L.; Fenu, G.; Cocco, E. Multidimensional frailty and its association with quality of life and disability: A cross-sectional study in people with multiple sclerosis. Mult. Scler. Relat. Disord. 2023, 79, 105036. [Google Scholar] [CrossRef] [PubMed]
- Maggio, M.G.; De Luca, R.; Manuli, A.; Buda, A.; Cuzzola, M.F.; Leonardi, S.; D’aleo, G.; Bramanti, P.; Russo, M.; Calabrò, R.S. Do patients with multiple sclerosis benefit from semi-immersive virtual reality? A randomized clinical trial on cognitive and motor outcomes. Appl. Neuropsychol. Adult 2022, 29, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Maresca, G.; Maggio, M.G.; De Luca, R.; Manuli, A.; Tonin, P.; Pignolo, L.; Calabrò, R.S. Tele-Neuro-Rehabilitation in Italy: State of the Art and Future Perspectives. Front. Neurol. 2020, 11, 563375. [Google Scholar] [CrossRef] [PubMed]
- Tacchino, A.; Podda, J.; Bergamaschi, V.; Pedullà, L.; Brichetto, G. Cognitive rehabilitation in multiple sclerosis: Three digital ingredients to address current and future priorities. Front. Hum. Neurosci. 2023, 17, 1130231. [Google Scholar] [CrossRef] [PubMed]
- Pagliari, C.; Di Tella, S.; Jonsdottir, J.; Mendozzi, L.; Rovaris, M.; De Icco, R.; Milanesi, T.; Federico, S.; Agostini, M.; Goffredo, M.; et al. Effects of home-based virtual reality telerehabilitation system in people with multiple sclerosis: A randomized controlled trial. J. Telemed. Telecare 2021. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, N.S.; Truax, P. Clinical significance: A statistical approach to defining meaningful change in psychotherapy research. J. Consult. Clin. Psychol. 1991, 59, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Bauer, S.; Lambert, M.J.; Nielsen, S.L. Clinical significance methods: A comparison of statistical techniques. J. Pers. Assess. 2004, 82, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, S.; Maggio, M.G.; Russo, M.; Bramanti, A.; Arcadi, F.A.; Naro, A.; Calabrò, R.S.; De Luca, R. Cognitive recovery in people with relapsing/remitting multiple sclerosis: A randomized clinical trial on virtual reality-based neurorehabilitation. Clin. Neurol. Neurosurg. 2021, 208, 106828. [Google Scholar] [CrossRef] [PubMed]
- Hughes, A.-M.; Burridge, J.; Freeman, C.T.; Donnovan-Hall, M.; Chappell, P.H.; Lewin, P.L.; Rogers, E.; Dibb, B. Stroke participants’ perceptions of robotic and electrical stimulation therapy: A new approach. Disabil. Rehabil. Assist. Technol. 2011, 6, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Pau, M.; Cocco, E.; Arippa, F.; Casu, G.; Porta, M.; Menascu, S.; Achiron, A.; Kalron, A. An Immersive Virtual Kitchen Training System for People with Multiple Sclerosis: A Development and Validation Study. J. Clin. Med. 2023, 12, 3222. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, A.J.; Benito-Leon, J.; Gonzalez, J.M.; Rivera-Navarro, J. Quality of life and its assessment in multiple sclerosis: Integrating physical and psychological components of wellbeing. Lancet Neurol. 2005, 4, 556–566. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Experimental | Control | All | p-Value | |
|---|---|---|---|---|
| Patients | 20 | 16 | 36 | |
| Age | 47.4 ± 10.2 | 50.5 ± 8.7 | 48.8 ± 9.6 | 0.88 |
| Education | 11.3 ± 3.3 | 11.6 ± 0.8 | 11.9 ± 4.9 | 0.11 |
| Gender | 0.35 | |||
| Male | 8 (30.0%) | 6 (37.5%) | 14 (38.9%) | |
| Female | 12 (70.0%) | 10 (62.5%) | 22 (61.1%) | |
| Disease duration, (years) | 10.7 ± 5.3 | 10.1 ± 6.1 | 10.5 ± 5.8 | 0.71 |
| Median EDSS | 4.7 ± 1.4 | 4.9 ± 0.4 | 4.8 ± 1.0 | 0.82 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maggio, M.G.; Cannavò, A.; Quartarone, A.; Manuli, A.; Tonin, P.; Calabrò, R.S. Enhancing the Quality of Life of Patients with Multiple Sclerosis: Promising Results on the Role of Cognitive Tele-Rehabilitation Plus Virtual Reality. Brain Sci. 2023, 13, 1636. https://doi.org/10.3390/brainsci13121636
Maggio MG, Cannavò A, Quartarone A, Manuli A, Tonin P, Calabrò RS. Enhancing the Quality of Life of Patients with Multiple Sclerosis: Promising Results on the Role of Cognitive Tele-Rehabilitation Plus Virtual Reality. Brain Sciences. 2023; 13(12):1636. https://doi.org/10.3390/brainsci13121636
Chicago/Turabian StyleMaggio, Maria Grazia, Antonino Cannavò, Angelo Quartarone, Alfredo Manuli, Paolo Tonin, and Rocco Salvatore Calabrò. 2023. "Enhancing the Quality of Life of Patients with Multiple Sclerosis: Promising Results on the Role of Cognitive Tele-Rehabilitation Plus Virtual Reality" Brain Sciences 13, no. 12: 1636. https://doi.org/10.3390/brainsci13121636
APA StyleMaggio, M. G., Cannavò, A., Quartarone, A., Manuli, A., Tonin, P., & Calabrò, R. S. (2023). Enhancing the Quality of Life of Patients with Multiple Sclerosis: Promising Results on the Role of Cognitive Tele-Rehabilitation Plus Virtual Reality. Brain Sciences, 13(12), 1636. https://doi.org/10.3390/brainsci13121636