
CSF, Blood, and MRI Biomarkers in Skogholt’s Disease—A Rare Neurodegenerative Disease in a Norwegian Kindred


 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Diagnostic Criteria
2.3. Skogholt Group
2.4. Laboratory Controls
2.5. Cerebral MRI Controls
2.6. Ethics
2.7. Lab Pre-Analytics
2.8. Lab Analytics
2.9. MRI Systems, Sequence Parameters, and Software for Postprocessing Statistics
2.10. Statistics
3. Results
3.1. Demographics
3.2. CSF Biomarkers
3.3. Plasma Biomarkers
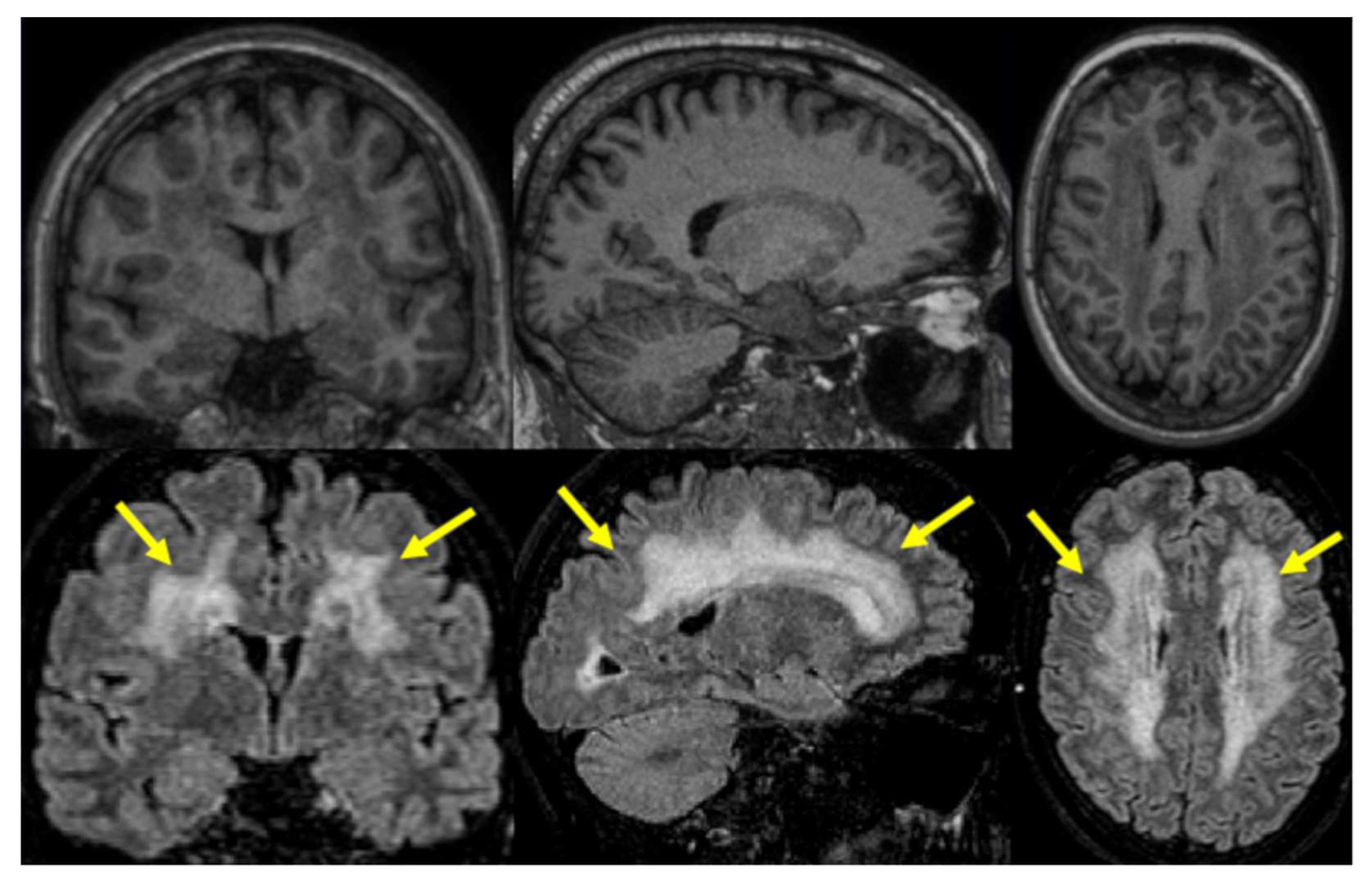
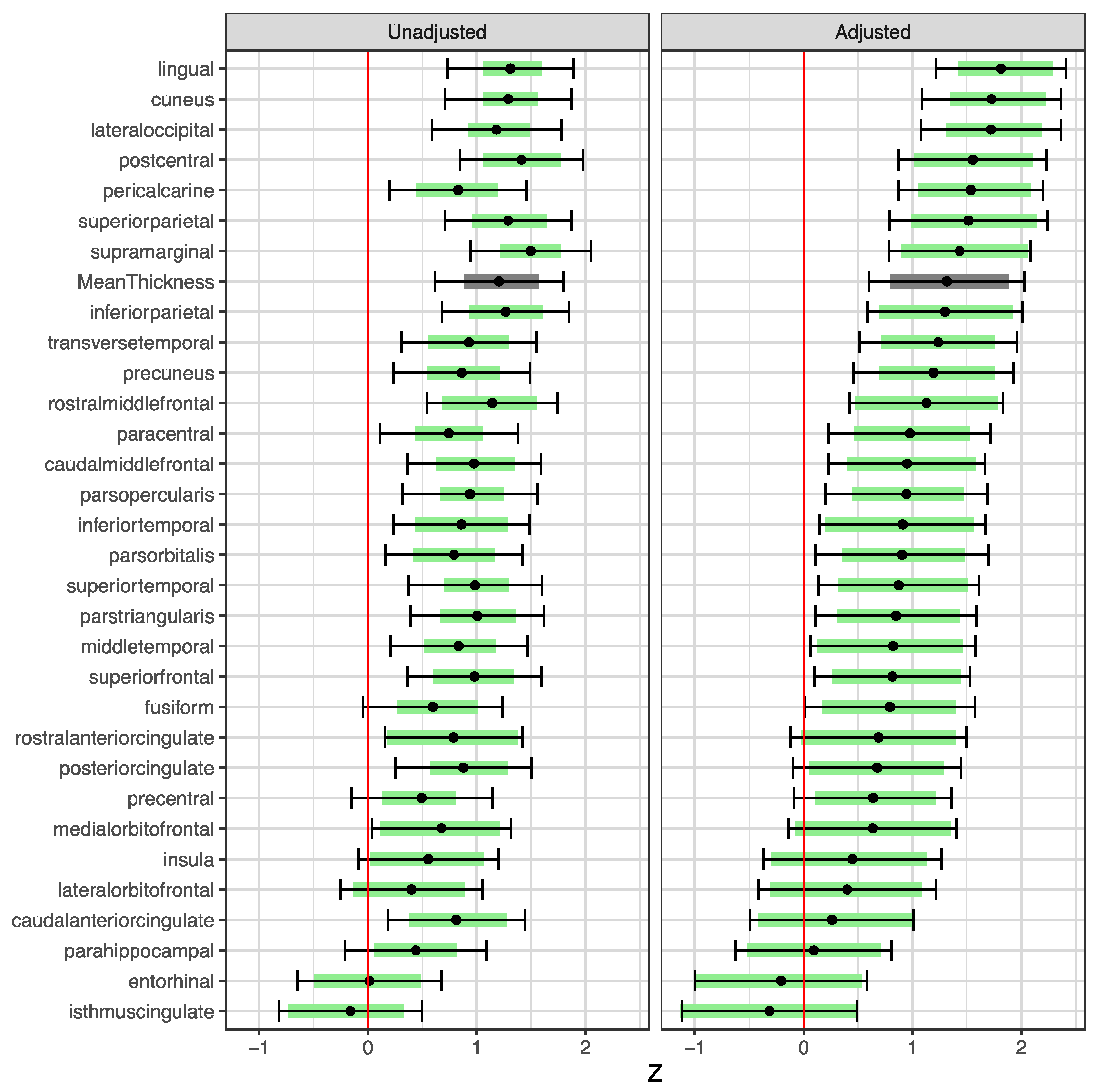
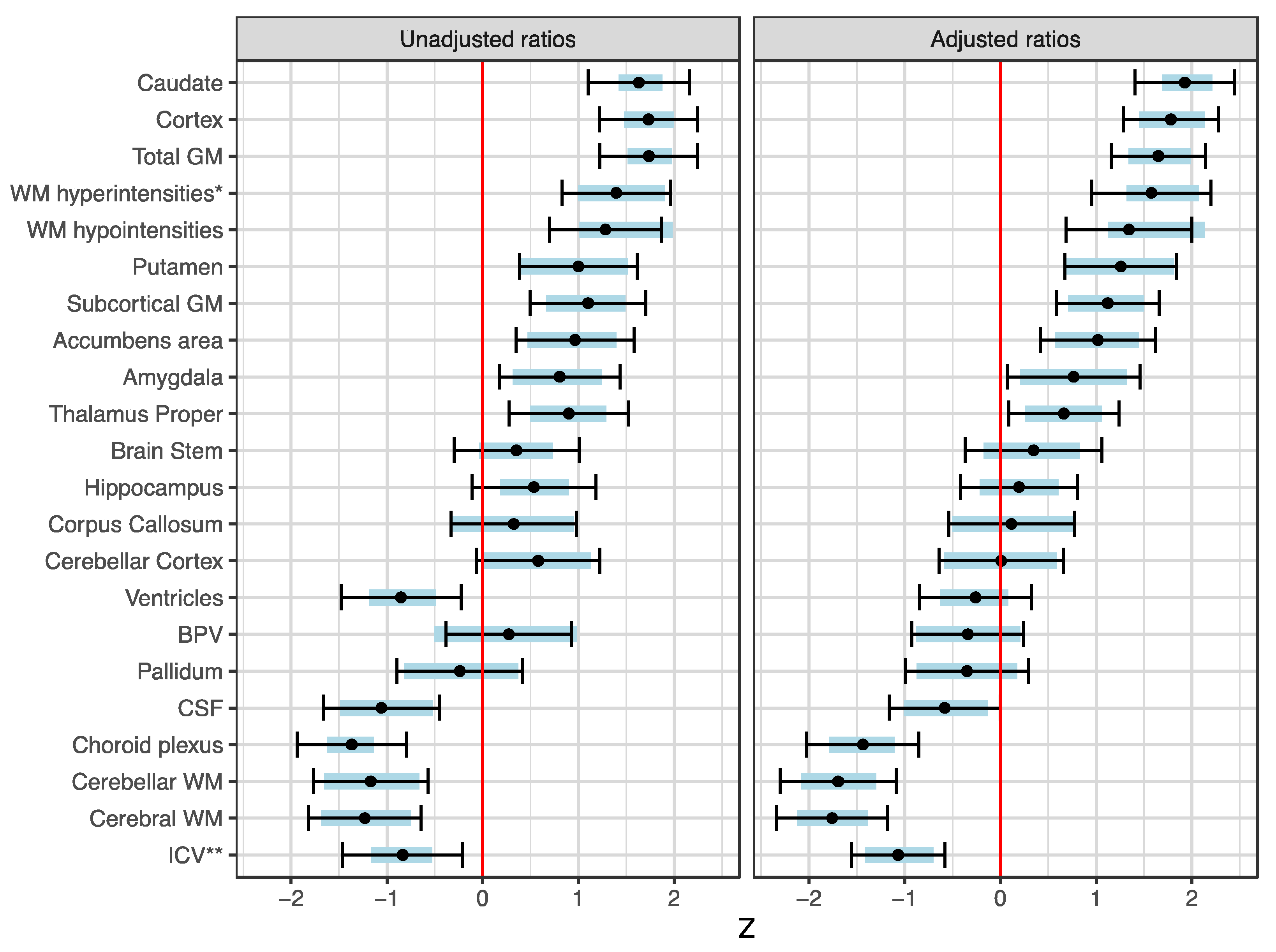
3.4. MRI Findings
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aspli, K.T.; Flaten, T.P.; Roos, P.M.; Holmøy, T.; Skogholt, J.H.; Aaseth, J. Iron and copper in progressive demyelination—New lessons from Skogholt’s disease. J. Trace Elem. Med. Biol. 2015, 31, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Hagen, K.; Boman, H.; Mellgren, S.I.; Lindal, S.; Bovim, G. Progressive central and peripheral demyelinating disease of adult onset in a Norwegian family. Arch. Neurol. 1998, 55, 1467–1472. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Aspli, K.T.; Holmøy, T.; Flaten, T.P.; Whist, J.E.; Aaseth, J.O. Skogholt’s disease—A tauopathy precipitated by iron and copper? J. Trace Elem. Med. Biol. 2022, 70, 126915. [Google Scholar] [CrossRef] [PubMed]
- Gellein, K.; Skogholt, J.H.; Aaseth, J.; Thoresen, G.B.; Lierhagen, S.; Steinnes, E.; Syversen, T.; Flaten, T.P. Trace elements in cerebrospinal fluid and blood from patients with a rare progressive central and peripheral demyelinating disease. J. Neurol. Sci. 2008, 266, 70–78. [Google Scholar] [CrossRef]
- Fladby, T.; Pålhaugen, L.; Selnes, P.; Waterloo, K.; Bråthen, G.; Hessen, E.; Almdahl, I.S.; Arntzen, K.A.; Auning, E.; Eliassen, C.F.; et al. Detecting At-Risk Alzheimer’s Disease Cases. J. Alzheimers Dis. 2017, 60, 97–105. [Google Scholar] [CrossRef]
- Gobom, J.; Parnetti, L.; Rosa-Neto, P.; Vyhnalek, M.; Gauthier, S.; Cataldi, S.; Lerch, O.; Laczo, J.; Cechova, K.; Clarin, M.; et al. Validation of the LUMIPULSE automated immunoassay for the measurement of core AD biomarkers in cerebrospinal fluid. Clin. Chem. Lab. Med. 2022, 60, 207–219. [Google Scholar] [CrossRef]
- Gaetani, L.; Höglund, K.; Parnetti, L.; Pujol-Calderon, F.; Becker, B.; Eusebi, P.; Sarchielli, P.; Calabresi, P.; Di Filippo, M.; Zetterberg, H.; et al. A new enzyme-linked immunosorbent assay for neurofilament light in cerebrospinal fluid: Analytical validation and clinical evaluation. Alzheimer’s Res. Ther. 2018, 10, 8. [Google Scholar] [CrossRef]
- Rosengren, L.E.; Ahlsén, G.; Belfrage, M.; Gillberg, C.; Haglid, K.G.; Hamberger, A. A sensitive ELISA for glial fibrillary acidic protein: Application in CSF of children. J. Neurosci. Methods 1992, 44, 113–119. [Google Scholar] [CrossRef]
- Zetterberg, H. Glial fibrillary acidic protein: A blood biomarker to differentiate neurodegenerative from psychiatric diseases. J. Neurol. Neurosurg. Psychiatry 2021, 92, 1253. [Google Scholar] [CrossRef]
- Henschel, L.; Conjeti, S.; Estrada, S.; Diers, K.; Fischl, B.; Reuter, M. FastSurfer—A fast and accurate deep learning based neuroimaging pipeline. Neuroimage 2020, 219, 117012. [Google Scholar] [CrossRef]
- Henschel, L.; Kügler, D.; Reuter, M. FastSurferVINN: Building resolution-independence into deep learning segmentation methods—A solution for HighRes brain MRI. Neuroimage 2022, 251, 118933. [Google Scholar] [CrossRef] [PubMed]
- Fischl, B.; van der Kouwe, A.; Destrieux, C.; Halgren, E.; Ségonne, F.; Salat, D.H.; Busa, E.; Seidman, L.J.; Goldstein, J.; Kennedy, D.; et al. Automatically parcellating the human cerebral cortex. Cereb. Cortex 2004, 14, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Fischl, B.; Dale, A.M. Measuring the thickness of the human cerebral cortex from magnetic resonance images. Proc. Natl. Acad. Sci. USA 2000, 97, 11050–11055. [Google Scholar] [CrossRef] [PubMed]
- Desikan, R.S.; Ségonne, F.; Fischl, B.; Quinn, B.T.; Dickerson, B.C.; Blacker, D.; Buckner, R.L.; Dale, A.M.; Maguire, R.P.; Hyman, B.T.; et al. An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. Neuroimage 2006, 31, 968–980. [Google Scholar] [CrossRef]
- Wardlaw, J.M.; Smith, E.E.; Biessels, G.J.; Cordonnier, C.; Fazekas, F.; Frayne, R.; Lindley, R.I.; O’Brien, J.T.; Barkhof, F.; Benavente, O.R.; et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. 2013, 12, 822–838. [Google Scholar] [CrossRef]
- Røvang, M.S.; Selnes, P.; MacIntosh, B.J.; Rasmus Groote, I.; Pålhaugen, L.; Sudre, C.; Fladby, T.; Bjørnerud, A. Segmenting white matter hyperintensities on isotropic three-dimensional Fluid Attenuated Inversion Recovery magnetic resonance images: Assessing deep learning tools on a Norwegian imaging database. PLoS ONE 2023, 18, e0285683. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- Gohel, D.; Panagiotis, S. ggiraph: Make ‘ggplot2’ Graphics Interactive, R Package Version 0.8.7; R Foundation for Statistical Computing: Vienna, Austria, 2023. [Google Scholar]
- Wickham, H.; François, R.; Henry, L.; Müller, K.; Vaughan, D. dplyr: A Grammar of Data Manipulation, R Package Version 1.0.7; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Sjoberg, D.D.; Whiting, K.; Curry, M.; Lavery, J.A.; Larmarange, J. Reproducible Summary Tables with the gtsummary Package. R J. 2021, 13, 570–580. [Google Scholar] [CrossRef]
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.D.A.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J. Welcome to the Tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Fazekas, F.; Chawluk, J.B.; Alavi, A.; Hurtig, H.I.; Zimmerman, R.A. MR signal abnormalities at 1.5 T in Alzheimer’s dementia and normal aging. AJR Am. J. Roentgenol. 1987, 149, 351–356. [Google Scholar] [CrossRef]
- Keshavan, A.; Wellington, H.; Chen, Z.; Khatun, A.; Chapman, M.; Hart, M.; Cash, D.M.; Coath, W.; Parker, T.D.; Buchanan, S.M.; et al. Concordance of CSF measures of Alzheimer’s pathology with amyloid PET status in a preclinical cohort: A comparison of Lumipulse and established immunoassays. Alzheimers Dement. 2021, 13, e12131. [Google Scholar] [CrossRef]
- Lafer, I.; Michaelis, S.; Schneider, C.; Baranyi, A.; Schnedl, W.J.; Holasek, S.; Zelzer, S.; Niedrist, T.; Meinitzer, A.; Enko, D. Beta-trace protein concentrations at the blood-cerebrospinal fluid barrier—Acute phase affects protein status. Excli. J. 2021, 20, 1446–1452. [Google Scholar] [CrossRef] [PubMed]
- Reiber, H. Blood-cerebrospinal fluid (CSF) barrier dysfunction means reduced CSF flow not barrier leakage—Conclusions from CSF protein data. Arq. Neuropsiquiatr. 2021, 79, 56–67. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, J.H.; Yalachkov, Y.; Friedauer, L.; Kirchmayr, K.; Miesbach, W.; Wenger, K.J.; Foerch, C.; Schaller-Paule, M.A. Measurement of prothrombin fragment 1 + 2 in cerebrospinal fluid to identify thrombin generation in inflammatory central nervous system diseases. Mult. Scler. Relat. Disord. 2022, 60, 103720. [Google Scholar] [CrossRef]
- Reiber, H. Dynamics of brain-derived proteins in cerebrospinal fluid. Clin. Chim. Acta 2001, 310, 173–186. [Google Scholar] [CrossRef] [PubMed]
- Brettschneider, J.; Petzold, A.; Süssmuth, S.; Tumani, H. Cerebrospinal fluid biomarkers in Guillain-Barré syndrome—Where do we stand? J. Neurol. 2009, 256, 3–12. [Google Scholar] [CrossRef]
- Jhelum, P.; David, S. Ferroptosis: Copper-iron connection in cuprizone-induced demyelination. Neural. Regen. Res. 2022, 17, 89–90. [Google Scholar] [CrossRef]
- Kerkhofs, D.; Wong, S.M.; Zhang, E.; Staals, J.; Jansen, J.F.A.; van Oostenbrugge, R.J.; Backes, W.H. Baseline Blood-Brain Barrier Leakage and Longitudinal Microstructural Tissue Damage in the Periphery of White Matter Hyperintensities. Neurology 2021, 96, e2192–e2200. [Google Scholar] [CrossRef]
- Zhang, C.E.; Wong, S.M.; Uiterwijk, R.; Backes, W.H.; Jansen, J.F.A.; Jeukens, C.; van Oostenbrugge, R.J.; Staals, J. Blood-brain barrier leakage in relation to white matter hyperintensity volume and cognition in small vessel disease and normal aging. Brain Imaging Behav. 2019, 13, 389–395. [Google Scholar] [CrossRef]
- Buchanan, C.R.; Muñoz Maniega, S.; Valdés Hernández, M.C.; Ballerini, L.; Barclay, G.; Taylor, A.M.; Russ, T.C.; Tucker-Drob, E.M.; Wardlaw, J.M.; Deary, I.J.; et al. Comparison of structural MRI brain measures between 1.5 and 3 T: Data from the Lothian Birth Cohort 1936. Hum. Brain Mapp. 2021, 42, 3905–3921. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Skogholt (n = 11) | Lab Control (n = 14) | MRI Control (n = 60) |
|---|---|---|---|
| Sex: Female | 6 (55%) | 11 (79%) | 29 (48%) |
| Male | 5 (45%) | 3 (21%) | 31 (52%) |
| Age (Yrs) | 57 (45, 67) | 64 (56, 70) | 64 (58, 68) |
| Coffee (Cups/d) | 3.0 (2.2, 4.2) | 2.5 (<1, 4.0) | - |
| Smoking (pkgYrs) a | 9 (4, 29) | 1 (<1, 22) | - |
| Alcohol (U/m) b | 9 (3, 14) | 3 (1, 6) | - |
| Exercise (H/w) c | ≥3 (1–2, ≥3) | 1–2 (1–2, ≥3) | - |
| Education (Yrs) | 9 (8, 11) | 12 (12, 16) | 14 (12, 16) |
| Mean (SD) | Median (IQR) | p-Values | Ratio of | |||||
|---|---|---|---|---|---|---|---|---|
| Analyte | Skogholt (n = 7) | Control (n = 11) | Skogholt (n = 7) | Control (n = 11) | t a | U b | Means c | Medians d |
| Aβ1– 42 | 1687 (1214) | 922 (341) | 1464 (950–1718) | 921 (721–1068) | 0.15 | 0.079 | 1.83 | 1.59 |
| Aβ1–40 | 35,385 (7596) | 10,868 (2936) | 38,528 (29,796–40,531) | 10,614 (8788–12,940) | <0.001 | <0.001 | 3.26 | 3.63 |
| p-Tau | 424 (87.1) | 44.2 (29.3) | 464 (346–476) | 36.5 (27.2–49.5) | <0.001 | <0.001 | 9.61 | 12.7 |
| t-Tau | 3147 (467) | 400 (250) | 3160 (2814–3562) | 342 (236–397) | <0.001 | <0.001 | 7.87 | 9.23 |
| Aβ1–42/1–40 | 0.050 (0.0277) | 0.0842 (0.0194) | 0.042 (0.034–0.0485) | 0.091 (0.0885–0.0963) | 0.017 | 0.022 | 0.60 | 0.46 |
| GFAP | 51,497 (10,622) | 16,677 (7867) | 52,373 (45,109–56,718) | 16,974 (9830–22,089) | <0.001 | <0.001 | 3.09 | 3.09 |
| NfL | 9138 (11,486) | 4738 (9626) | 4210 (2851–8818) | 1200 (881–4027) | 0.403 | 0.046 | 1.93 | 3.51 |
| PDGFRβ | 1915 (283) | 422 (118) | 1936 (1752–2051) | 410 (316–523) | <0.001 | <0.001 | 4.53 | 4.72 |
| βTP | 112 (9.41) | 16.6 (3.69) | 108 (107–120) | 16 (15–18.8) | <0.001 | <0.001 | 6.75 | 6.75 |
| Aβx–38 | 5497 (504) | 1812 (631) | 5359 (5211–5829) | 1628 (1370–2302) | <0.001 | <0.001 | 3.03 | 3.29 |
| Aβx–40 | 12,319 (2361) | 4428 (1097) | 13,106 (10,829–14,016) | 4326 (3820–4901) | <0.001 | <0.001 | 2.78 | 3.03 |
| Aβx–42 | 619 (407) | 331 (142) | 558 (340–663) | 307 (266–361) | 0.113 | 0.031 | 1.87 | 1.82 |
| Mean (SD) | Median (IQR) | p-Values | Ratio of | |||||
|---|---|---|---|---|---|---|---|---|
| Analyte | Skogholt (n = 11) | Control (n = 14) | Skogholt (n = 11) | Control (n = 14) | t a | U b | Means c | Medians d |
| tTau | 38.8 (24.6) | 49 (40.8) | 33.2 (28.7–39.2) | 39.3 (24.6–47.7) | 0.447 | 0.536 | 0.791 | 0.844 |
| GFAP | 58.8 (27.8) | 128 (107) | 56.8 (35–81.2) | 82 (68.6–153) | 0.034 | 0.033 | 0.459 | 0.693 |
| NfL | 22.5 (33.7) | 83.3 (186) | 9.49 (8.46–15.7) | 30.1 (14.3–61.2) | 0.251 | 0.025 | 0.270 | 0.316 |
| Aβ40 | 97.6 (20.1) | 108 (28.1) | 92 (89–101) | 94.6 (89.2–123) | 0.306 | 0.647 | 0.906 | 0.973 |
| Aβ42 | 6.66 (0.9) | 6.95 (1.28) | 6.47 (6.18–7.03) | 6.97 (6.3–7.3) | 0.514 | 0.501 | 0.958 | 0.928 |
| pTau181 | 7.74 (3.24) | 8.23 (4.71) | 7.33 (5.92–9.34) | 5.85 (5.45–10.8) | 0.760 | 0.687 | 0.940 | 1.250 |
| Aβ42/Aβ40 | 0.0693 (0.00801) | 0.0668 (0.0132) | 0.0705 (0.063–0.0761) | 0.069 (0.0626–0.0766) | 0.566 | 0.851 | 1.040 | 1.020 |
| Fazekas Score | Skogholt Group n = 11 | MRI Control Group n = 60 |
|---|---|---|
| 0 | 2 (18%) | 13 (23%) |
| 1 | 1 (9.1%) | 36 (64%) |
| 2 | 2 (18%) | 7 (12%) |
| 3 | 6 (55%) | 0 (0%) |
| missing | 0 | 4 |
| Score | GCA | MTA | Koedam |
|---|---|---|---|
| 0 | 6 (55%) | 6 (55%) | 5 (45%) |
| 1 | 3 (27%) | 5 (45%) | 5 (45%) |
| 2 | 2 (18%) | 0 (0%) | 1 (9.1%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aspli, K.T.; Aaseth, J.O.; Holmøy, T.; Blennow, K.; Zetterberg, H.; Kirsebom, B.-E.; Fladby, T.; Selnes, P. CSF, Blood, and MRI Biomarkers in Skogholt’s Disease—A Rare Neurodegenerative Disease in a Norwegian Kindred. Brain Sci. 2023, 13, 1511. https://doi.org/10.3390/brainsci13111511
Aspli KT, Aaseth JO, Holmøy T, Blennow K, Zetterberg H, Kirsebom B-E, Fladby T, Selnes P. CSF, Blood, and MRI Biomarkers in Skogholt’s Disease—A Rare Neurodegenerative Disease in a Norwegian Kindred. Brain Sciences. 2023; 13(11):1511. https://doi.org/10.3390/brainsci13111511
Chicago/Turabian StyleAspli, Klaus Thanke, Jan O. Aaseth, Trygve Holmøy, Kaj Blennow, Henrik Zetterberg, Bjørn-Eivind Kirsebom, Tormod Fladby, and Per Selnes. 2023. "CSF, Blood, and MRI Biomarkers in Skogholt’s Disease—A Rare Neurodegenerative Disease in a Norwegian Kindred" Brain Sciences 13, no. 11: 1511. https://doi.org/10.3390/brainsci13111511
APA StyleAspli, K. T., Aaseth, J. O., Holmøy, T., Blennow, K., Zetterberg, H., Kirsebom, B.-E., Fladby, T., & Selnes, P. (2023). CSF, Blood, and MRI Biomarkers in Skogholt’s Disease—A Rare Neurodegenerative Disease in a Norwegian Kindred. Brain Sciences, 13(11), 1511. https://doi.org/10.3390/brainsci13111511