
Assessing the Training in Neurosurgery with the Implementation of VITOM-3D Exoscope: Learning Curve on Experimental Model in Neurosurgical Practice

 ,
,  ,
,  ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Protocol
2.2. Evaluation Score
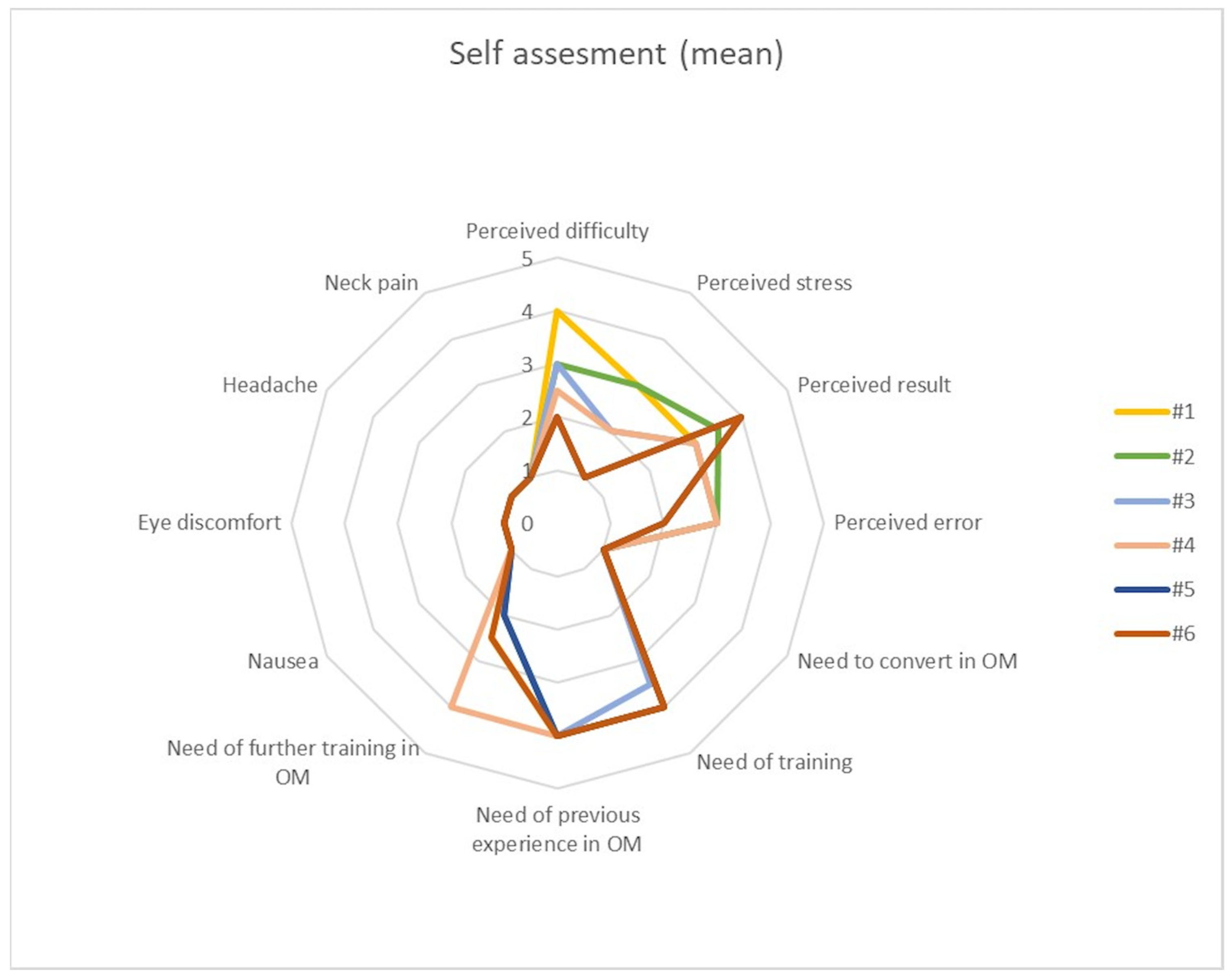
- How much do you rate the difficulty of the task? (0 = None; 5 = Very much)
- How much do you rate the stress during the task? (0 = None; 5 = Very much)
- How much do you rate the results of your performance? (0 = Very poor; 5 = Very good)
- How often do you think you made some mistakes? (0 = Never; 5 = Always)
- How often did you need to convert in microscopy? (0 = Never; 5 = Always)
- How much training do you think is needed in order to obtain an optimal result? (0 = Never; 5 = Always)
- Can a former training in microscopy ensure an optimal result with these tasks in exoscopy? (0 = Strongly disagree; 5 = Strongly agree)
- May a further training in microscopy ensure an optimal result with these tasks in exoscopy? (0 = Strongly disagree; 5 = Strongly agree)
- How often did you have nausea? (0 = Never, 5 = Always)
- How often did you have ocular discomfort? (0 = Never, 5 = Always)
- How often did you have headache? (0 = Never, 5 = Always)
- How often did you have neck stiffness? (0 = Never, 5 = Always)
2.3. Statistical Analysis
3. Results
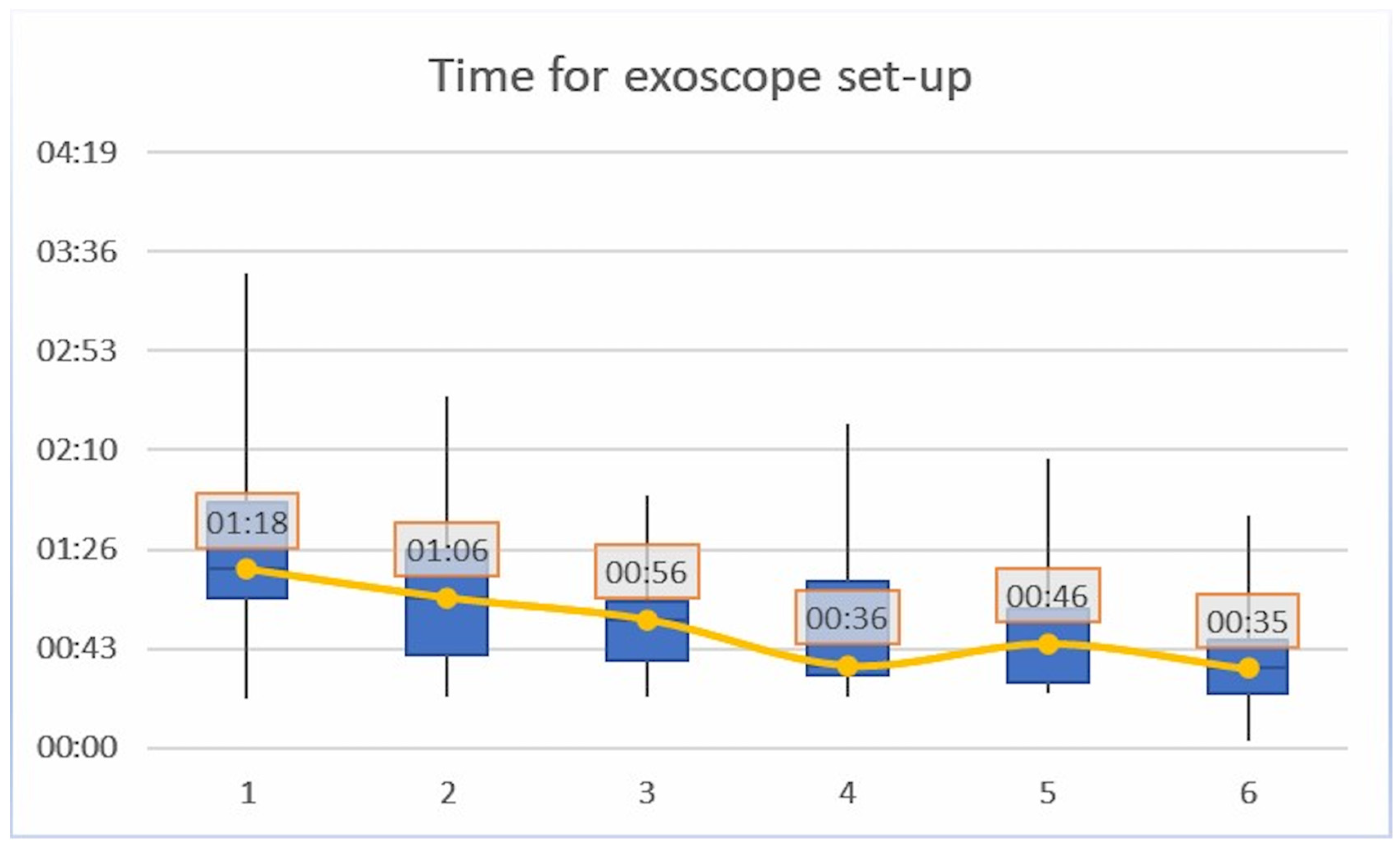
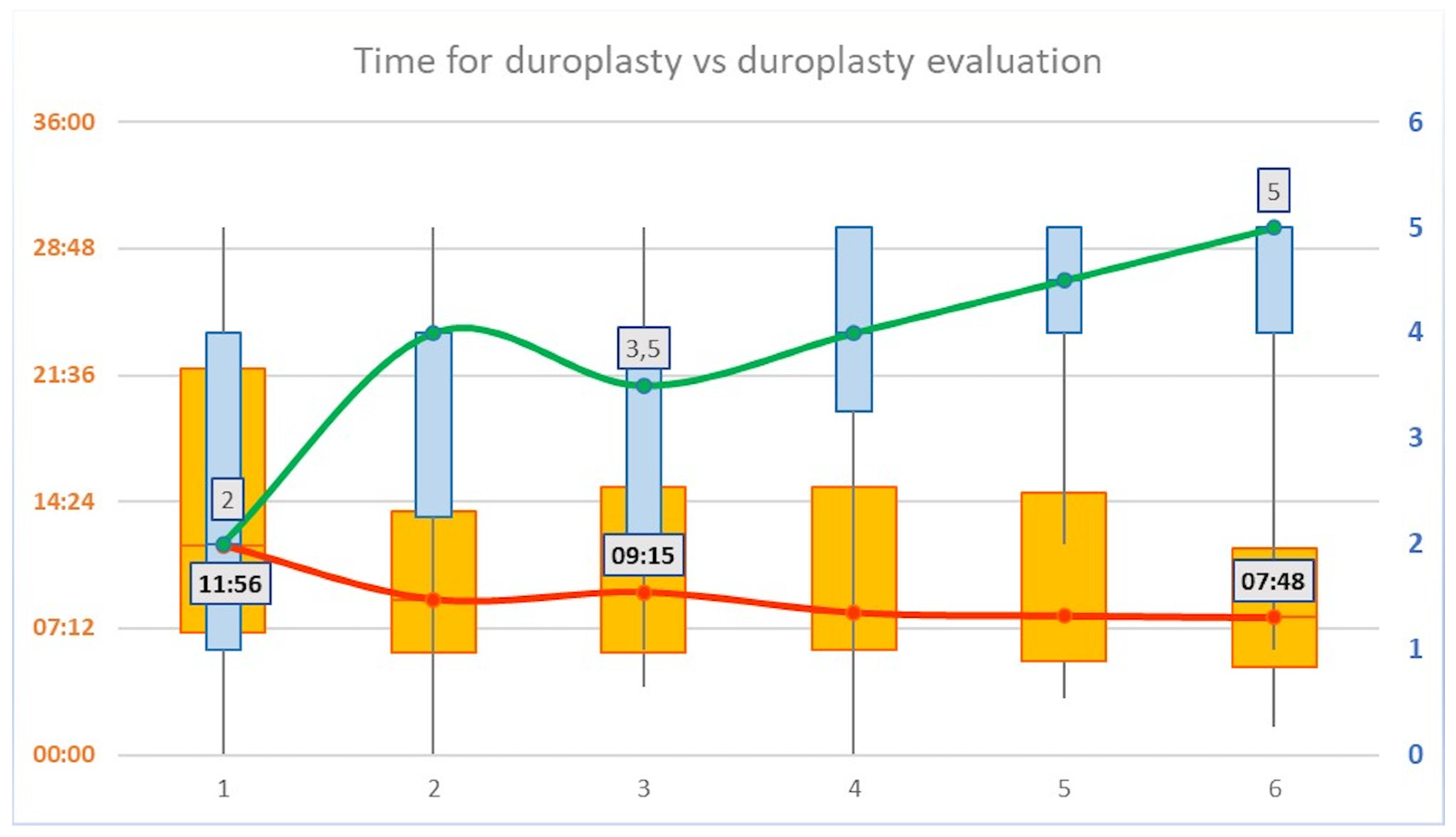
3.1. Timing
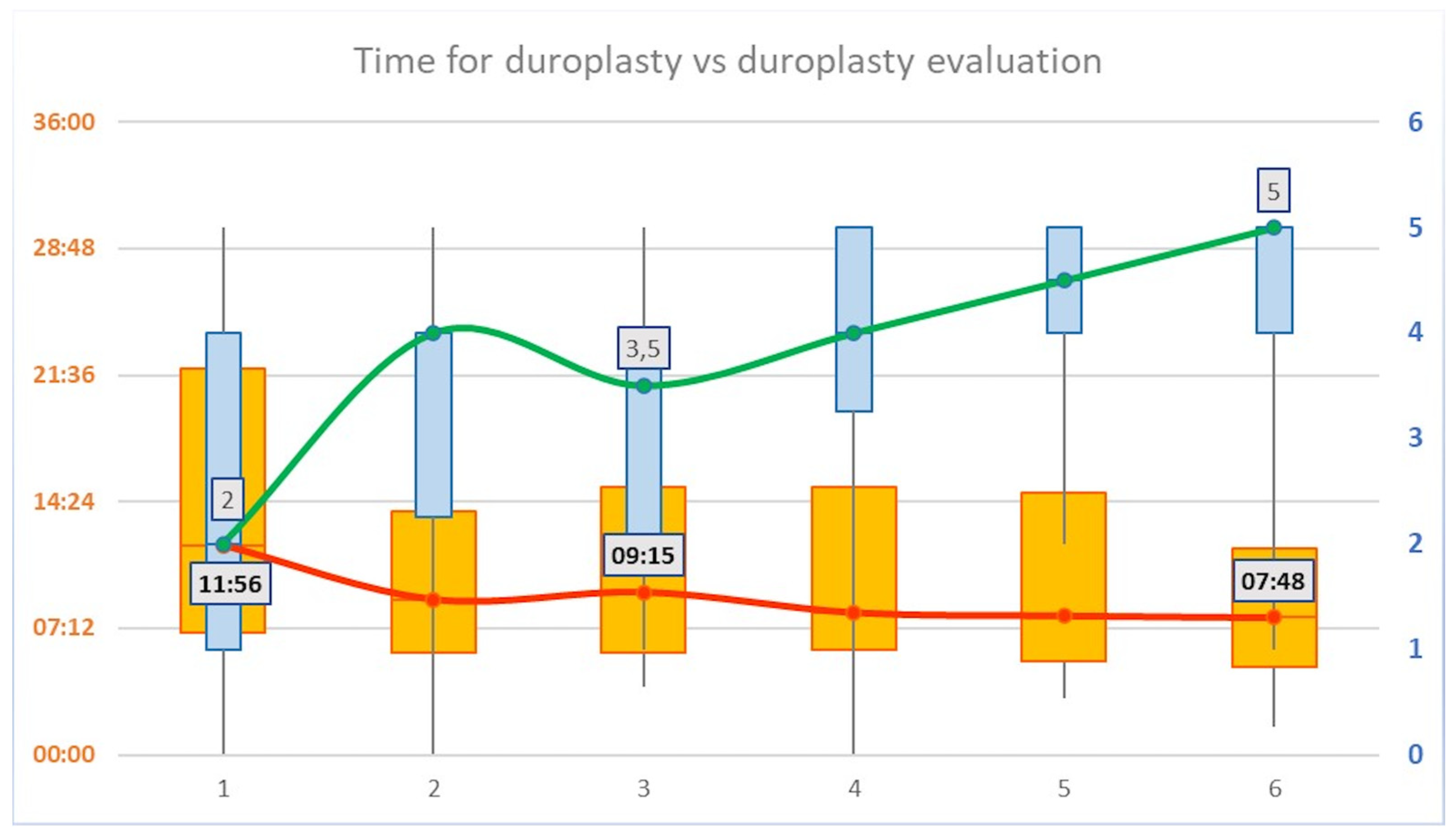
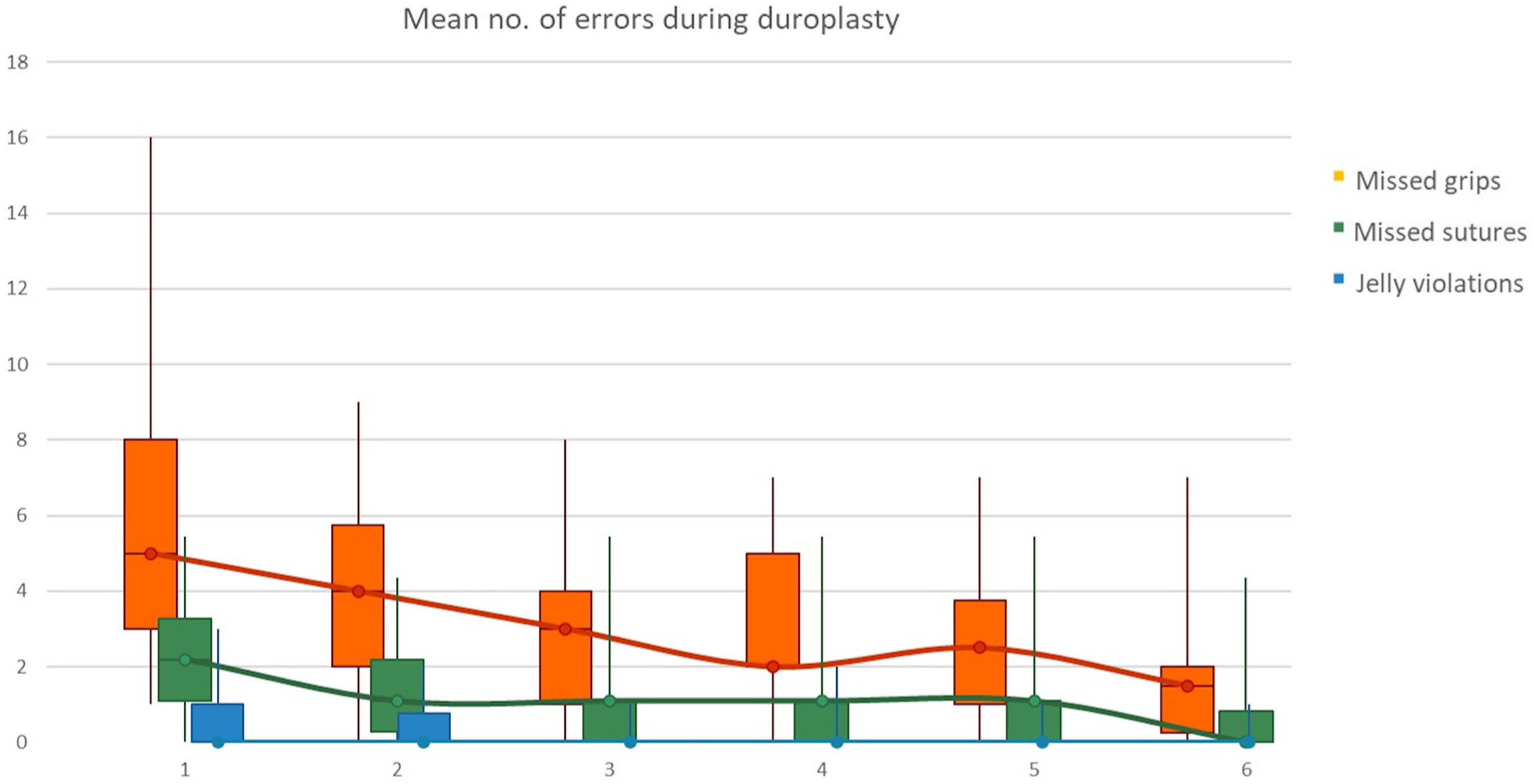
3.2. Evaluation
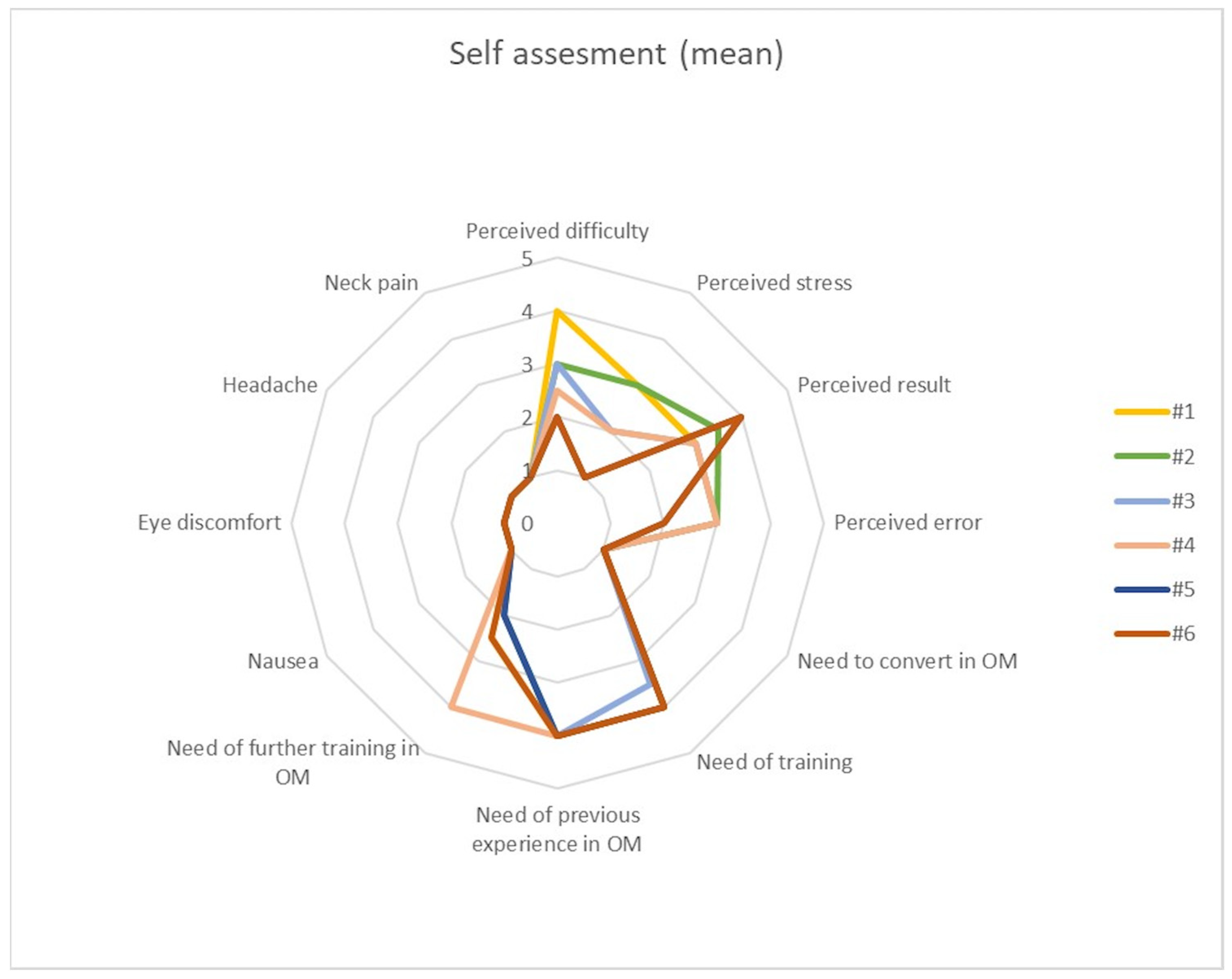
3.3. Self-Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Byvaltsev, V.A.; Akshulakov, S.K.; Polkin, R.A.; Ochkal, S.V.; Stepanov, I.A.; Makhambetov, Y.T.; Kerimbayev, T.T.; Staren, M.; Belykh, E.; Preul, M.C. Microvascular Anastomosis Training in Neurosurgery: A Review. Minim. Invasive Surg. 2018, 2018, 6130286. [Google Scholar] [CrossRef] [PubMed]
- Pafitanis, G.; Hadjiandreou, M.; Alamri, A.; Uff, C.; Walsh, D.; Myers, S. The Exoscope versus Operating Microscope in Microvascular Surgery: A Simulation Non-Inferiority Trial. Arch. Plast. Surg. 2020, 47, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Fiani, B.; Jarrah, R.; Griepp, D.W.; Adukuzhiyil, J. The Role of 3D Exoscope Systems in Neurosurgery: An Optical Innovation. Cureus 2021, 13, e15878. [Google Scholar] [CrossRef] [PubMed]
- Oertel, J.M.; Burkhardt, B.W. Vitom-3D for Exoscopic Neurosurgery: Initial Experience in Cranial and Spinal Procedures. World Neurosurg. 2017, 105, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Maugeri, R.; Giammalva, R.G.; Iacopino, D.G. On the Shoulders of Giants, with a Smartphone: Periscope in Neurosurgery. World Neurosurg. 2016, 92, 569–570. [Google Scholar] [CrossRef] [PubMed]
- Visocchi, M.; Mattogno, P.; Ciappetta, P.; Barbagallo, G.; Signorelli, F. Combined Transoral Exoscope and OArm-Assisted Approach for Craniovertebral Junction Surgery: Light and Shadows in Single-Center Experience with Improving Technologies. J. Craniovertebr. Junction Spine 2020, 11, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Mamelak, A.N.; Nobuto, T.; Berci, G. Initial Clinical Experience with a High-Definition Exoscope System for Microneurosurgery. Neurosurgery 2010, 67, 476–483. [Google Scholar] [CrossRef] [PubMed]
- Visocchi, M.; Mattogno, P.P.; Signorelli, F. Exoscope and OArm: What We Can Learn in Craniovertebral Junction Surgery. J. Neurosurg. Sci. 2021, 65, 616–617. [Google Scholar] [CrossRef] [PubMed]
- Angileri, F.F.; Esposito, F.; Scibilia, A.; Priola, S.M.; Raffa, G.; Germanò, A. Exoscope-Guided (VITOM 3D) Single-Stage Removal of Supratentorial Cavernous Angioma and Hemangioblastoma: 3-Dimensional Operative Video. Oper. Neurosurg. 2019, 17, E164–E165. [Google Scholar] [CrossRef] [PubMed]
- Burkhardt, B.W.; Csokonay, A.; Oertel, J.M. 3D-Exoscopic Visualization Using the VITOM-3D in Cranial and Spinal Neurosurgery. What Are the Limitations? Clin. Neurol. Neurosurg. 2020, 198, 106101. [Google Scholar] [CrossRef] [PubMed]
- Rossini, Z.; Cardia, A.; Milani, D.; Lasio, G.B.; Fornari, M.; D’Angelo, V. VITOM 3D: Preliminary Experience in Cranial Surgery. World Neurosurg. 2017, 107, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Yoon, W.S.; Lho, H.W.; Chung, D.S. Evaluation of 3-Dimensional Exoscopes in Brain Tumor Surgery. J. Korean Neurosurg. Soc. 2021, 64, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Calloni, T.; Antolini, L.; Roumy, L.G.; Nicolosi, F.; Carrabba, G.G.; Di Cristofori, A.; Fon-tanella, M.M.; Giussani, C.G. Exoscope and operative microscope for training in micro-neurosurgery: A laboratory investigation on a model of cranial approach. Front. Surg. 2023, 10, 1150981. [Google Scholar] [CrossRef] [PubMed]
- Beez, T.; Munoz-Bendix, C.; Beseoglu, K.; Steiger, H.-J.; Ahmadi, S.A. First Clinical Applications of a High-Definition Three-Dimensional Exoscope in Pediatric Neurosurgery. Cureus 2018, 10, e2108. [Google Scholar] [CrossRef] [PubMed]
- Birch, K.; Drazin, D.; Black, K.L.; Williams, J.; Berci, G.; Mamelak, A.N. Clinical Experience with a High Definition Exoscope System for Surgery of Pineal Region Lesions. J. Clin. Neurosci. 2014, 21, 1245–1249. [Google Scholar] [CrossRef] [PubMed]
- Silva, J.M.; Rustemi, O.; Vezirska, D.I.; Niemelä, M.; Lehecka, M.; Hafez, A. Taming the exoscope: A one-year prospective laboratory training study. Acta Neurochir. (Wien) 2023, 165, 2037–2044. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Subject | Yrs of NS | Gender | Age |
|---|---|---|---|---|
| Junior | 1 | 0 | M | 25 |
| 2 | 0 | F | 27 | |
| 3 | 0 | F | 25 | |
| 4 | 0 | M | 26 | |
| 5 | 0 | M | 29 | |
| 6 | 1 | M | 32 | |
| 7 | 1 | F | 29 | |
| 8 | 2 | M | 28 | |
| 9 | 3 | F | 27 | |
| 10 | 1 | F | 26 | |
| 11 | 3 | F | 28 | |
| 12 | 3 | F | 27 | |
| 13 | 2 | M | 28 | |
| Senior | 14 | 6 | M | 37 |
| 15 | 7 | F | 33 | |
| 16 | 10 | F | 36 | |
| 17 | 14 | M | 40 | |
| 18 | 20 | M | 45 |
| Group | Subject | Yrs of NS | #1 | #2 | #3 | #4 | #5 | #6 |
|---|---|---|---|---|---|---|---|---|
| Junior | 1 | 0 | 00:02:43 | 00:02:05 | 00:01:05 | 00:01:16 | 00:00:58 | 00:00:47 |
| 2 | 0 | 00:02:54 | 00:00:49 | 00:01:00 | 00:01:34 | 00:00:55 | 00:00:49 | |
| 3 | 0 | 00:01:10 | 00:01:26 | 00:01:33 | 00:02:21 | 00:00:25 | 00:00:39 | |
| 4 | 0 | 00:01:51 | 00:00:57 | 00:01:00 | 00:01:30 | 00:00:53 | 00:00:26 | |
| 5 | 0 | 00:01:00 | 00:00:38 | 00:00:54 | 00:01:02 | 00:01:01 | 00:00:37 | |
| 6 | 1 | 00:03:27 | 00:01:34 | 00:00:59 | 00:01:17 | 00:01:05 | 00:00:46 | |
| 7 | 1 | 00:01:22 | 00:02:33 | 00:01:36 | 00:00:35 | 00:01:55 | 00:01:13 | |
| 8 | 2 | 00:01:30 | 00:02:18 | 00:01:44 | 00:00:59 | 00:02:06 | 00:01:41 | |
| 9 | 3 | 00:00:21 | 00:00:22 | 00:00:24 | 00:00:33 | 00:00:26 | 00:00:21 | |
| 10 | 1 | 00:00:48 | 00:00:57 | 00:01:50 | 00:00:37 | 00:00:28 | 00:00:37 | |
| 11 | 3 | 00:02:50 | 00:01:18 | 00:00:48 | 00:00:35 | 00:00:24 | 00:00:23 | |
| 12 | 3 | 00:01:06 | 00:00:32 | 00:00:37 | 00:00:23 | 00:00:35 | 00:00:03 | |
| 13 | 2 | 00:01:35 | 00:01:14 | 00:00:58 | 00:00:38 | 00:00:52 | 00:00:59 | |
| Senior | 14 | 6 | 00:01:14 | 00:00:34 | 00:00:23 | 00:00:30 | 00:00:31 | 00:00:20 |
| 15 | 7 | 00:00:57 | 00:01:02 | 00:00:33 | 00:00:22 | 00:01:02 | 00:00:30 | |
| 16 | 10 | 00:01:09 | 00:01:25 | 00:00:40 | 00:00:31 | 00:00:28 | 00:00:22 | |
| 17 | 14 | 00:01:22 | 00:01:09 | 00:00:48 | 00:00:33 | 00:00:38 | 00:00:28 | |
| 18 | 20 | 00:01:05 | 00:00:34 | 00:00:22 | 00:00:24 | 00:00:39 | 00:00:32 | |
| Mean | 00:01:18 | 00:01:06 | 00:00:56 | 00:00:36 | 00:00:46 | 00:00:35 | ||
| St Dev | 00:00:49 | 00:00:36 | 00:00:27 | 00:00:31 | 00:00:28 | 00:00:22 |
| Group | Subject | Yrs of NS | #1 | #2 | #3 | #4 | #5 | #6 |
|---|---|---|---|---|---|---|---|---|
| Junior | 1 | 0 | 00:01:37 | 00:01:55 | 00:01:42 | 00:06:08 | 00:02:24 | 00:01:35 |
| 2 | 0 | 00:03:36 | 00:02:05 | 00:01:04 | 00:02:53 | 00:03:09 | 00:01:46 | |
| 3 | 0 | 00:00:50 | 00:01:23 | 00:03:46 | 00:01:28 | 00:00:51 | 00:00:54 | |
| 4 | 0 | 00:02:04 | 00:01:17 | 00:01:32 | 00:00:41 | 00:00:21 | 00:00:14 | |
| 5 | 0 | 00:04:56 | 00:02:15 | 00:01:54 | 00:00:44 | 00:00:56 | 00:01:38 | |
| 6 | 1 | 00:03:26 | 00:03:54 | 00:03:36 | 00:02:15 | 00:01:52 | 00:01:21 | |
| 7 | 1 | 00:04:18 | 00:01:46 | 00:03:00 | 00:01:21 | 00:00:54 | 00:02:14 | |
| 8 | 2 | 00:02:34 | 00:02:17 | 00:01:47 | 00:01:23 | 00:02:02 | 00:01:25 | |
| 9 | 3 | 00:00:23 | 00:00:22 | 00:00:21 | 00:00:29 | 00:00:22 | 00:00:21 | |
| 10 | 1 | 00:01:00 | 00:00:53 | 00:00:34 | 00:00:22 | 00:00:28 | 00:00:26 | |
| 11 | 3 | 00:00:39 | 00:00:19 | 00:00:11 | 00:00:13 | 00:00:11 | 00:00:09 | |
| 12 | 3 | 00:01:35 | 00:00:59 | 00:00:51 | 00:00:46 | 00:00:29 | 00:00:27 | |
| 13 | 2 | 00:01:01 | 00:00:43 | 00:00:38 | 00:00:33 | 00:00:41 | 00:00:29 | |
| Senior | 14 | 6 | 00:00:13 | 00:00:10 | 00:00:09 | 00:00:08 | 00:00:11 | 00:00:10 |
| 15 | 7 | 00:00:49 | 00:01:25 | 00:00:56 | 00:00:31 | 00:00:32 | 00:00:26 | |
| 16 | 10 | 00:00:08 | 00:00:09 | 00:00:59 | 00:00:19 | 00:00:08 | 00:00:08 | |
| 17 | 14 | 00:00:30 | 00:00:34 | 00:00:37 | 00:00:22 | 00:00:22 | 00:00:21 | |
| 18 | 20 | 00:00:37 | 00:00:25 | 00:00:19 | 00:00:24 | 00:00:24 | 00:00:18 | |
| Mean | 00:01:00 | 00:01:08 | 00:00:57 | 00:00:37 | 00:00:30 | 00:00:26 | ||
| St Dev | 00:01:26 | 00:00:57 | 00:01:05 | 00:01:24 | 00:00:51 | 00:00:39 |
| Group | Subject | Yrs of NS | #1 | #2 | #3 | #4 | #5 | #6 |
|---|---|---|---|---|---|---|---|---|
| Junior | 1 | 0 | 00:28:03 | 00:24:47 | 00:22:40 | 00:27:02 | 00:25:31 | 00:12:24 |
| 2 | 0 | 00:23:18 | 00:17:42 | 00:16:15 | 00:20:03 | 00:22:11 | 00:21:30 | |
| 3 | 0 | 00:25:29 | 00:14:02 | 00:17:22 | 00:24:40 | 00:17:28 | 00:17:43 | |
| 4 | 0 | 00:31:16 | 00:12:54 | 00:10:49 | 00:13:36 | 00:13:16 | 00:09:48 | |
| 5 | 0 | 00:18:26 | 00:30:02 | 00:12:00 | 00:15:26 | 00:15:15 | 00:12:32 | |
| 6 | 1 | 00:13:51 | 00:11:05 | 00:11:05 | 00:14:41 | 00:13:44 | 00:09:40 | |
| 7 | 1 | 00:23:11 | 00:15:36 | 00:16:33 | 00:12:22 | 00:08:58 | 00:08:25 | |
| 8 | 2 | 00:18:01 | 00:13:23 | 00:21:05 | 00:21:16 | 00:18:33 | 00:16:12 | |
| 9 | 3 | 00:09:09 | 00:07:15 | 00:08:07 | 00:07:27 | 00:06:16 | 00:05:00 | |
| 10 | 1 | 00:06:18 | 00:07:41 | 00:08:30 | 00:07:30 | 00:08:13 | 00:06:29 | |
| 11 | 3 | 00:10:00 | 00:10:00 | 00:10:01 | 00:08:41 | 00:07:36 | 00:07:11 | |
| 12 | 3 | 00:06:47 | 00:05:42 | 00:06:06 | 00:05:56 | 00:04:58 | 00:05:46 | |
| 13 | 2 | 00:18:07 | 00:06:01 | 00:06:28 | 00:07:00 | 00:06:38 | 00:08:31 | |
| Senior | 14 | 6 | 00:04:19 | 00:04:02 | 00:03:51 | 00:02:35 | 00:03:15 | 00:01:35 |
| 15 | 7 | 00:09:12 | 00:06:51 | 00:05:44 | 00:06:14 | 00:06:43 | 00:05:09 | |
| 16 | 10 | 00:07:23 | 00:05:00 | 00:04:26 | 00:03:46 | 00:04:07 | 00:03:03 | |
| 17 | 14 | 00:05:59 | 00:05:06 | 00:05:41 | 00:05:22 | 00:04:23 | 00:04:35 | |
| 18 | 20 | 00:04:38 | 00:04:24 | 00:04:58 | 00:05:30 | 00:05:01 | 00:04:36 | |
| Mean | 00:11:56 | 00:08:50 | 00:09:15 | 00:08:06 | 00:07:55 | 00:07:48 | ||
| St Dev | 00:08:31 | 00:07:03 | 00:05:41 | 00:07:15 | 00:06:32 | 00:05:13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giammalva, G.R.; Paolini, F.; Meccio, F.; Giovannini, E.A.; Provenzano, A.; Bonosi, L.; Brunasso, L.; Costanzo, R.; Gerardi, R.M.; Di Bonaventura, R.; et al. Assessing the Training in Neurosurgery with the Implementation of VITOM-3D Exoscope: Learning Curve on Experimental Model in Neurosurgical Practice. Brain Sci. 2023, 13, 1409. https://doi.org/10.3390/brainsci13101409
Giammalva GR, Paolini F, Meccio F, Giovannini EA, Provenzano A, Bonosi L, Brunasso L, Costanzo R, Gerardi RM, Di Bonaventura R, et al. Assessing the Training in Neurosurgery with the Implementation of VITOM-3D Exoscope: Learning Curve on Experimental Model in Neurosurgical Practice. Brain Sciences. 2023; 13(10):1409. https://doi.org/10.3390/brainsci13101409
Chicago/Turabian StyleGiammalva, Giuseppe Roberto, Federica Paolini, Flavia Meccio, Evier Andrea Giovannini, Alessandra Provenzano, Lapo Bonosi, Lara Brunasso, Roberta Costanzo, Rosa Maria Gerardi, Rina Di Bonaventura, and et al. 2023. "Assessing the Training in Neurosurgery with the Implementation of VITOM-3D Exoscope: Learning Curve on Experimental Model in Neurosurgical Practice" Brain Sciences 13, no. 10: 1409. https://doi.org/10.3390/brainsci13101409
APA StyleGiammalva, G. R., Paolini, F., Meccio, F., Giovannini, E. A., Provenzano, A., Bonosi, L., Brunasso, L., Costanzo, R., Gerardi, R. M., Di Bonaventura, R., Signorelli, F., Albanese, A., Iacopino, D. G., Maugeri, R., & Visocchi, M. (2023). Assessing the Training in Neurosurgery with the Implementation of VITOM-3D Exoscope: Learning Curve on Experimental Model in Neurosurgical Practice. Brain Sciences, 13(10), 1409. https://doi.org/10.3390/brainsci13101409