
Safety and Efficacy of Drug Holidays for Women with Sexual Dysfunction Induced by Selective Serotonin Reuptake Inhibitors (SSRIs) Other than Fluoxetine: An Open-Label Randomized Clinical Trial


 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Setting and Design
2.2. Participants
2.3. Data Collection
2.4. Instruments
2.5. Interventions
2.6. Sample Size and Statistical Analysis
2.7. Ethics Approval and Consent to Participate
3. Results
3.1. Total
3.2. Arousal
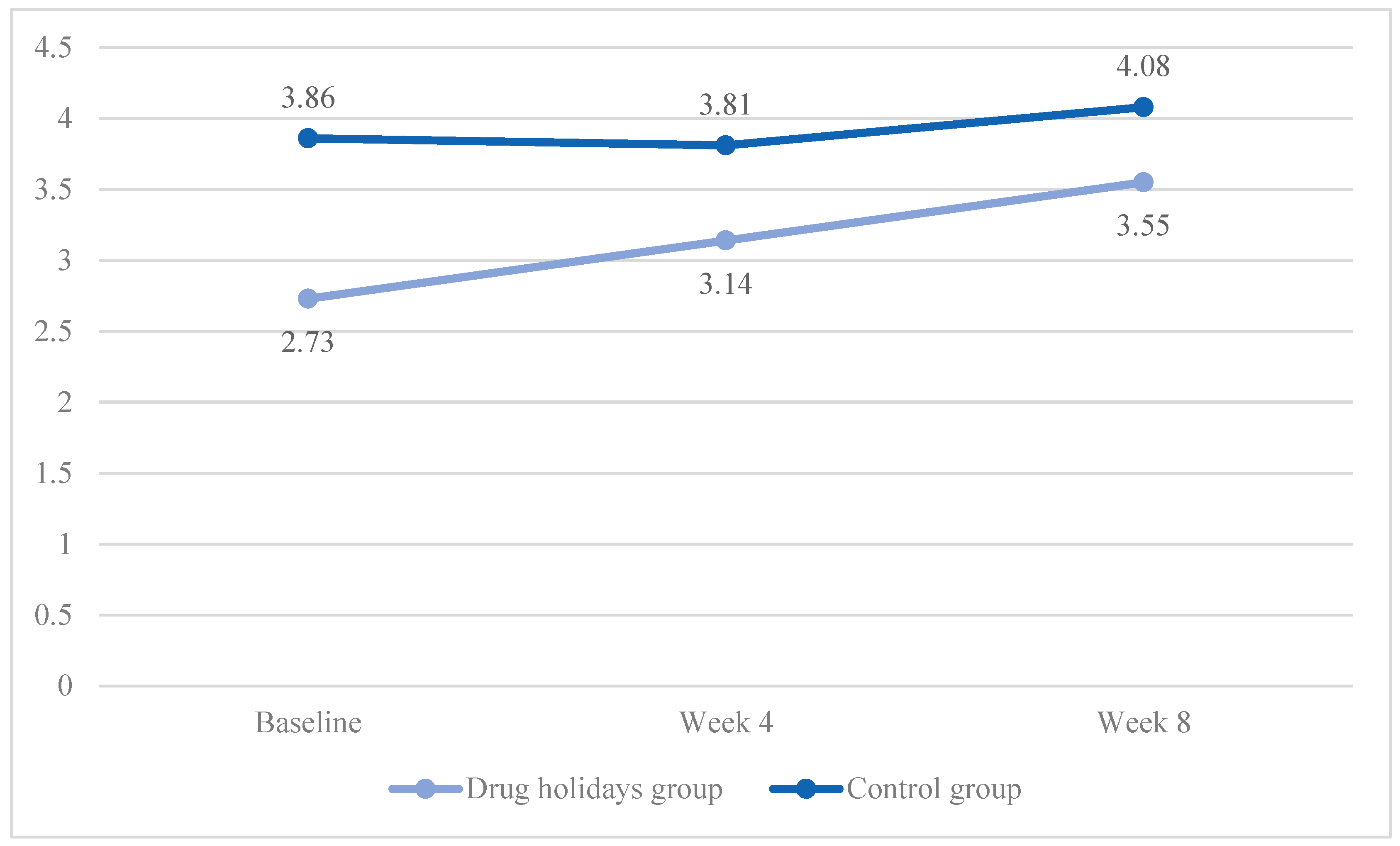
3.3. Desire
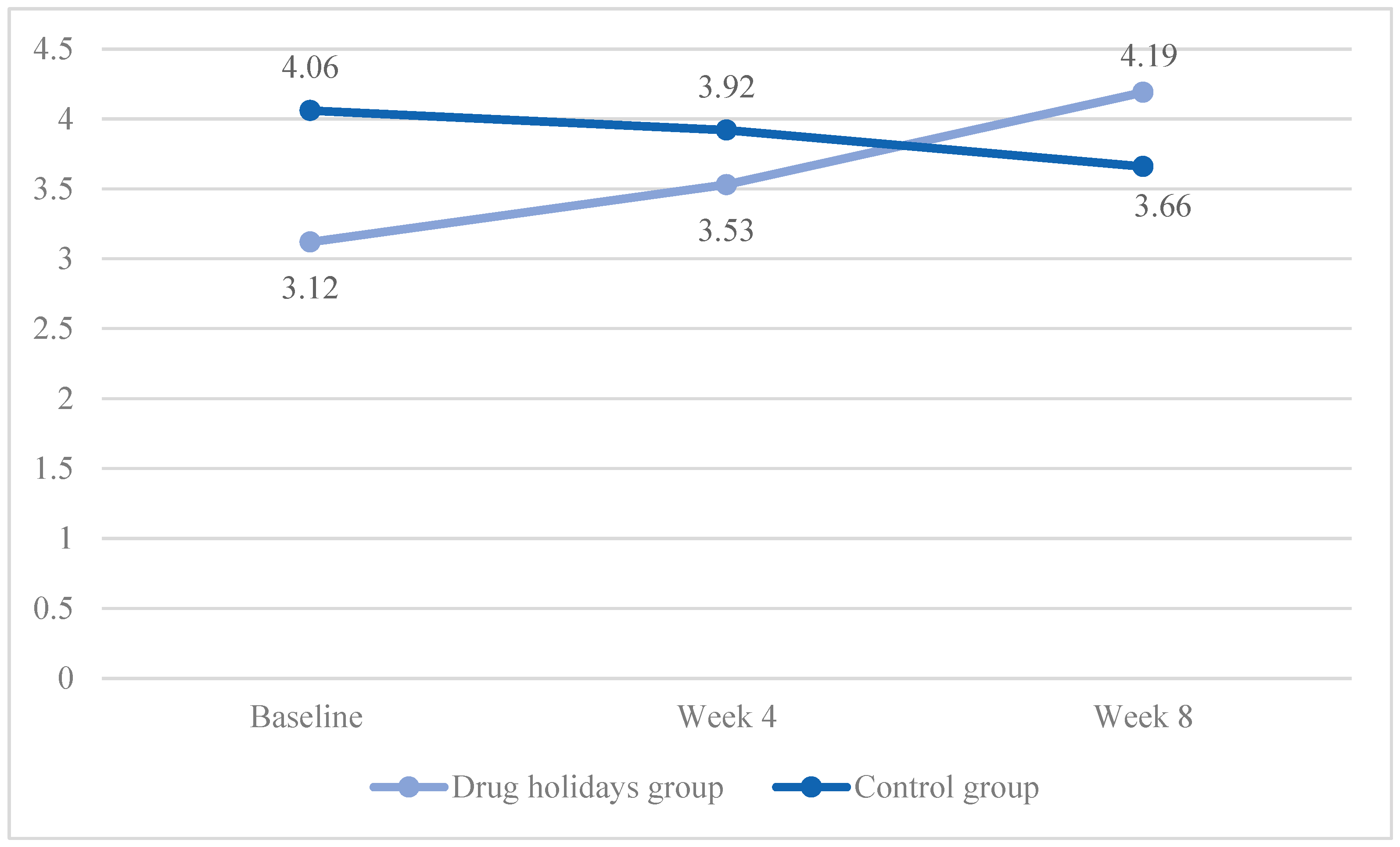
3.4. Orgasm
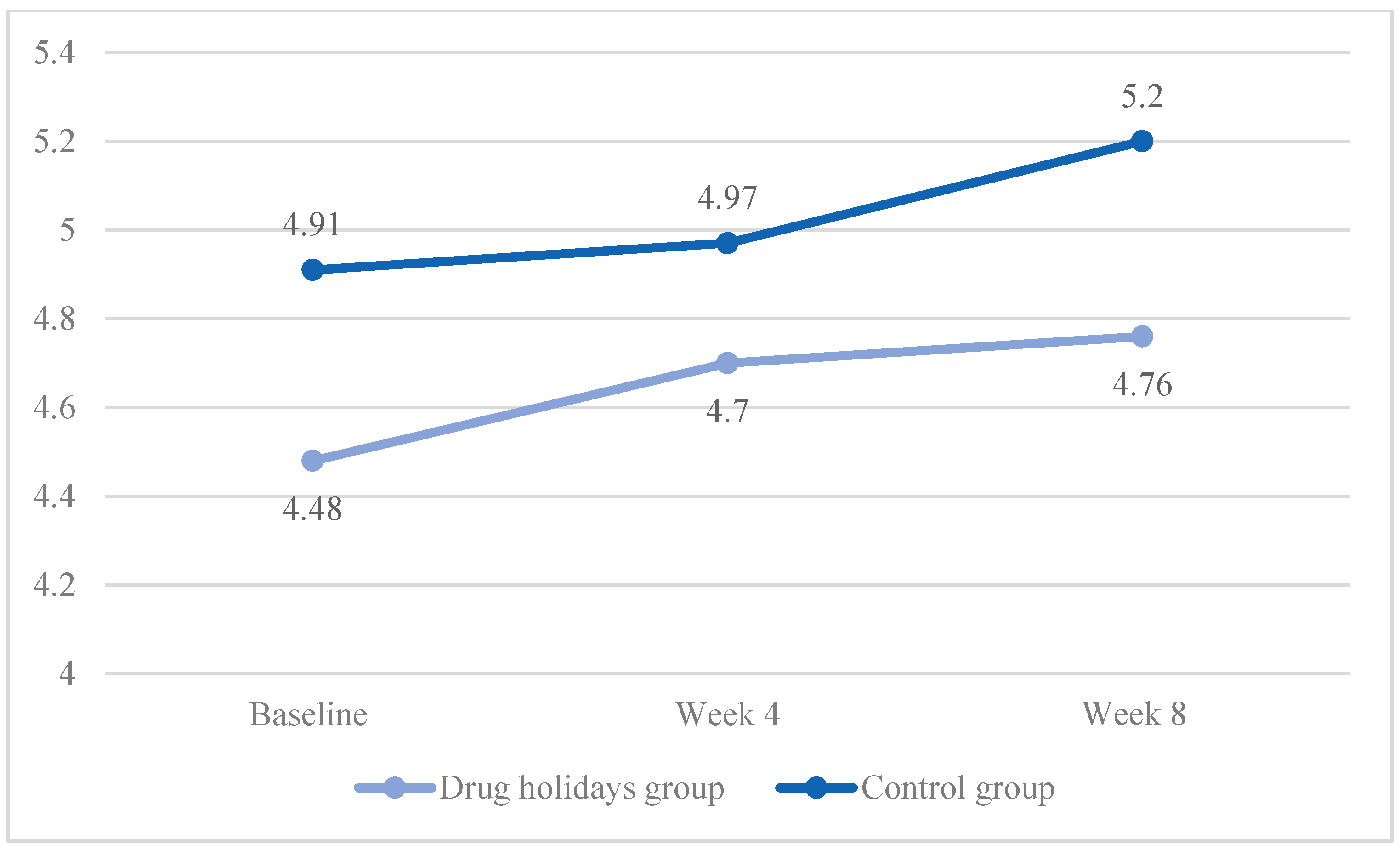
3.5. Pain
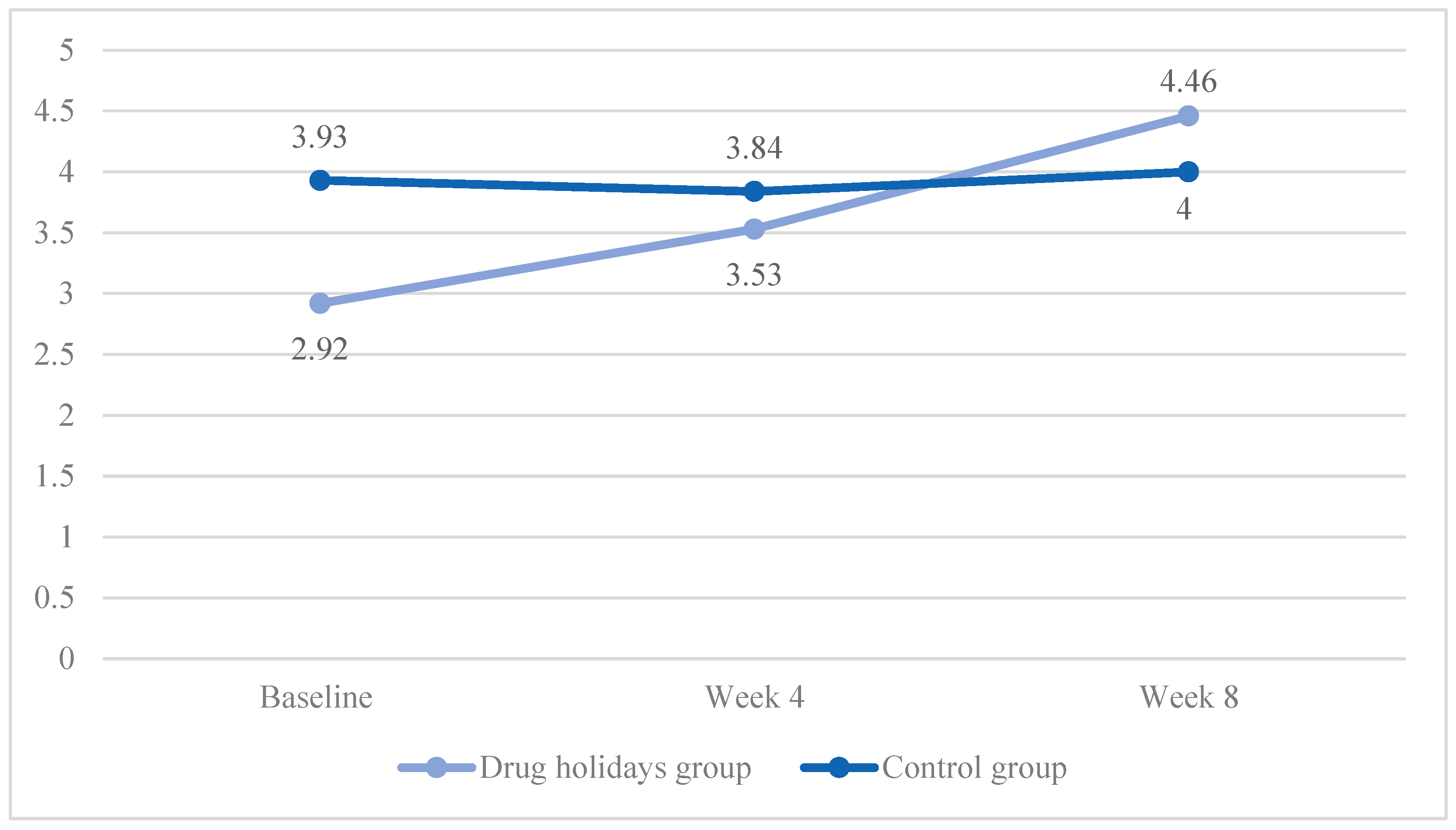
3.6. Satisfaction
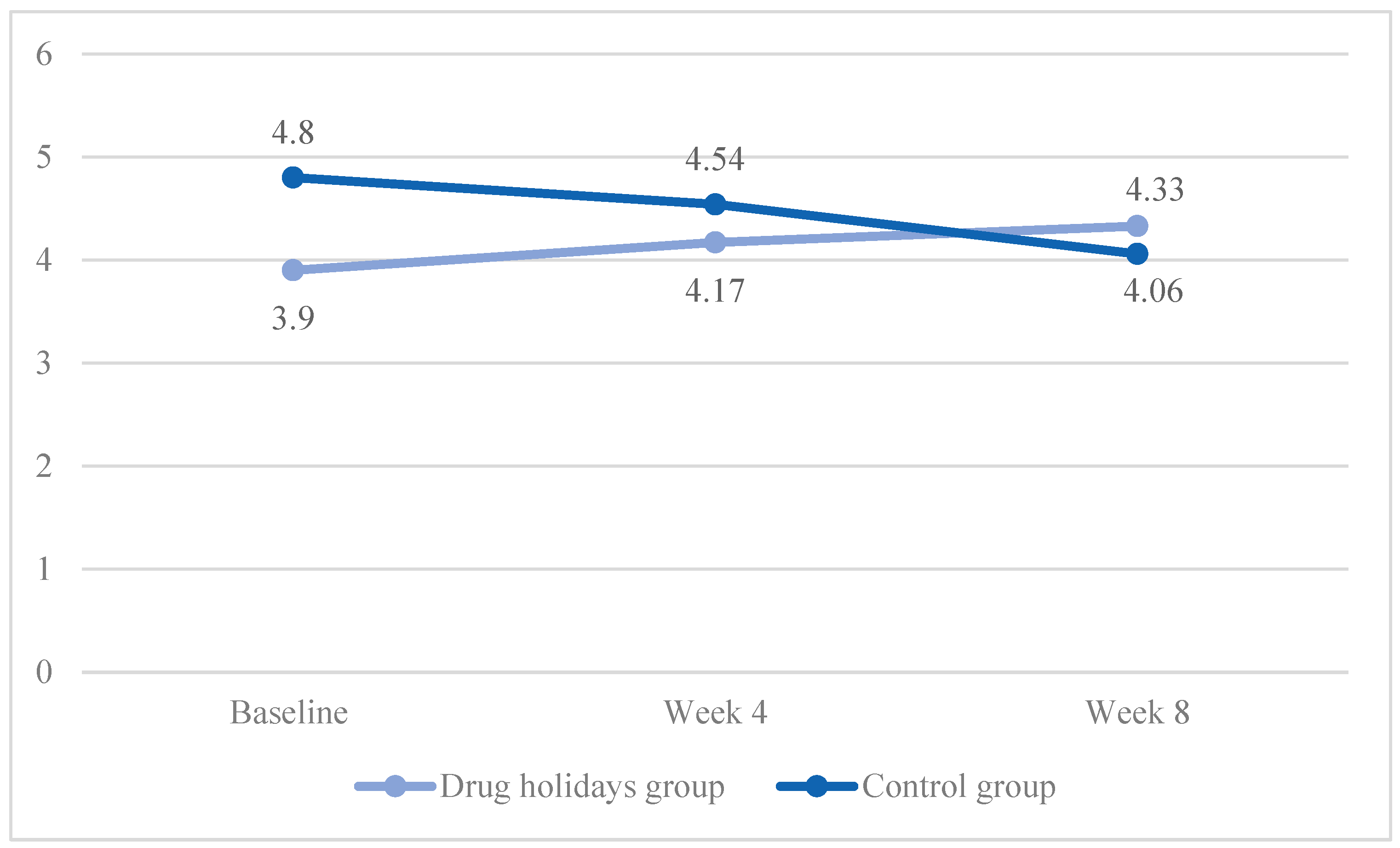
3.7. Lubrication
3.8. GHQ-28
3.9. Adverse Effects
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| SSRIs | Selective serotonin reuptake inhibitors |
| FSFI | Female sexual function index |
| GHQ-28 | 28-question general health questionnaire |
References
- Serretti, A.; Chiesa, A. Treatment-emergent sexual dysfunction related to antidepressants: A meta-analysis. J. Clin. Psychopharmacol. 2009, 29, 259–266. [Google Scholar] [CrossRef]
- Ben-Sheetrit, J.; Aizenberg, D.; Csoka, A.B.; Weizman, A.; Hermesh, H. Post-SSRI Sexual Dysfunction: Clinical Characterization and Preliminary Assessment of Contributory Factors and Dose-Response Relationship. J. Clin. Psychopharmacol. 2015, 35, 273–278. [Google Scholar] [CrossRef]
- Dhir, A.; Kulkarni, S.K. Nitric Oxide (NO) System in Major Depression: Studies on NO Synthase Inhibitors as Antidepressant Agents. Curr. Enzym. Inhib. 2016, 12, 40–48. [Google Scholar] [CrossRef]
- Taylor, M.J.; Rudkin, L.; Bullemor-Day, P.; Lubin, J.; Chukwujekwu, C.; Hawton, K. Strategies for managing sexual dysfunction induced by antidepressant medication. Cochrane Database Syst. Rev. 2013, 5, CD003382. [Google Scholar] [CrossRef]
- Montejo, A.L.; Prieto, N.; de Alarcón, R.; Casado-Espada, N.; de la Iglesia, J.; Montejo, L. Management Strategies for Antidepressant-Related Sexual Dysfunction: A Clinical Approach. J. Clin. Med. 2019, 8, 1640. [Google Scholar] [CrossRef]
- De Filippis, R.; Solerdelcoll, M.; Shalbafan, M. Editorial: Safety and side effects of psychotropic medications. Front. Psychiatry 2023, 14, 1148158. [Google Scholar] [CrossRef]
- Shalbafan, M.; Saeedi, V.; Kamalzadeh, L. Significant improvement of risperidone-induced retrograde ejaculation on drug holidays: A case report. Psychiatry Clin. Psychopharmacol. 2019, 29, 120–122. [Google Scholar] [CrossRef]
- Rothschild, A.J. Selective serotonin reuptake inhibitor-induced sexual dysfunction: Efficacy of a drug holidays. Am. J. Psychiatry 1995, 152, 1514–1516. [Google Scholar] [CrossRef]
- Németh, A.; Arató, M.; Treuer, T.; Vandlik, E. Treatment of fluvoxamine-induced anorgasmia with a partial drug holidays. Am. J. Psychiatry 1996, 153, 1365. [Google Scholar] [CrossRef]
- Alipour-Kivi, A.; Eissazade, N.; Shariat, S.V.; Salehian, R.; Soraya, S.; Askari, S.; Shalbafan, M. The Effect of Drug Holidays on Sexual Dysfunction in Men Treated with Selective Serotonin Reuptake Inhibitors (SSRIs) Other than Fluoxetine: An 8-Week Open-Label Randomized Clinical Trial. Available online: www.researchsquare.com/article/rs-3175920/latest.pdf (accessed on 23 August 2023).
- Rosen, R.; Brown, C.; Heiman, J.; Leiblum, S.; Meston, C.; Shabsigh, R.; Ferguson, D.; D’Agostino, R., Jr. The Female Sexual Function Index (FSFI): A multidimensional self-report instrument for the assessment of female sexual function. J. Sex Marital. Ther. 2000, 26, 191–208. [Google Scholar] [CrossRef]
- Meston, C.M. Validation of the Female Sexual Function Index (FSFI) in women with female orgasmic disorder and in women with hypoactive sexual desire disorder. J. Sex Marital. Ther. 2003, 29, 39–46. [Google Scholar] [CrossRef]
- Mohammadi, K.H.; Heydari, M.; Faghihzadeh, S. The Female Sexual Function Index (FSFI): Validation of the Iranian version. Payesh 2008, 7. [Google Scholar]
- Goldberg, D.P.; Hillier, V.F. A scaled version of the General Health Questionnaire. Psychol. Med. 1979, 9, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Malakouti, S.K.; Fatollahi, P.; Mirabzadeh, A.; Zandi, T. Reliability, validity and factor structure of the GHQ-28 used among elderly Iranians. Int. Psychogeriatr. 2007, 19, 623–634. [Google Scholar] [CrossRef] [PubMed]
- Askari, S.; Mokhtari, S.; Shariat, S.V.; Shariati, B.; Yarahmadi, M.; Shalbafan, M. Memantine augmentation of sertraline in the treatment of symptoms and executive function among patients with obsessive-compulsive disorder: A double-blind placebo-controlled, randomized clinical trial. BMC Psychiatry 2022, 22, 34. [Google Scholar] [CrossRef] [PubMed]
- Gregorian, R.S., Jr.; Golden, K.A.; Bahce, A.; Goodman, C.; Kwong, W.J.; Khan, Z.M. Antidepressant-induced sexual dysfunction. Ann. Pharmacother. 2002, 36, 1577–1589. [Google Scholar] [CrossRef]
- Harvey, K.Y.; Balon, R. Clinical implications of antidepressant drug effects on sexual function. Ann. Clin. Psychiatry 1995, 7, 189–200. [Google Scholar] [CrossRef]
- Keks, N.A.; Hope, J.; Culhane, C. Management of antidepressant-induced sexual dysfunction. Australas Psychiatry 2014, 22, 525–528. [Google Scholar] [CrossRef]
- Lorenz, T.; Rullo, J.; Faubion, S. Antidepressantinduced female sexual dysfunction. Mayo Clin. Proc. 2016, 91, 1280–1286. [Google Scholar] [CrossRef]
- Clayton, A.H.; El Haddad, S.; Iluonakhamhe, J.-P.; Martinez, C.P.; Schuck, A.E. Sexual dysfunction associated with major depressive disorder and antidepressant treatment. Expert Opin. Drug Saf. 2014, 13, 1361–1374. [Google Scholar] [CrossRef]
- Hirsch, M.; Birnbaum, R.J. Sexual Dysfunction Caused by Selective Serotonin Reuptake Inhibitors (SSRIs): Management. UpToDate 24 August 2019. Available online: https://www.uptodate.com/contents/sexual-dysfunction-caused-by-selective-serotonin-reuptake-inhibitors-ssris-management (accessed on 1 August 2023).
- Montejo-Gonzàlez, A.L.; Llorca, G.; Izquierdo, J.A.; Ledesma, A.; Bousono, M.; Calcedo, A.; Carrasco, J.L.; Ciudad, J.; Daniel, E.; De LA Gandara, J.; et al. SSRI-induced sexual dysfunction: Fluoxetine, paroxetine, sertraline, and fluvoxamine in a prospective, multicenter, and descriptive clinical study of 344 patients. J. Sex Marital Ther. 1997, 23, 176–194. [Google Scholar] [CrossRef] [PubMed]
- Francois, D.; Levin, A.M.; Kutscher, E.J.; Asemota, B. Antidepressant-induced sexual side effects: Incidence, assessment, clinical implications, and management. Psychiatr. Ann. 2017, 47, 154–160. [Google Scholar] [CrossRef]
- Jacobsen, P.L.; Mahableshwarkar, A.R.; Chen, Y.; Chrones, L.; Clayton, A.H. Effect of vortioxetine vs. escitalopram on sexual functioning in adults with well-treated major depressive disorder experiencing SSRIinduced sexual dysfunction. J. Sex Med. 2015, 12, 2036–2048. [Google Scholar] [CrossRef]
- Baldwin, D.S.; Manson, C.; Nowak, M. Impact of antidepressant drugs on sexual function and satisfaction. CNS Drugs 2015, 29, 905–913. [Google Scholar] [CrossRef]
- Moore, B.E.; Rothschild, A.J. Treatment of antidepressant-induced sexual dysfunction. Hosp. Pract. 1999, 34, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Atmaca, M. Selective serotonin reuptake inhibitor-induced sexual dysfunction: Current management perspectives. Neuropsychiatr. Dis. Treat. 2020, 16, 1043–1050. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug Holidays’ Group (N = 25) | Control Group (N = 25) | |||||
|---|---|---|---|---|---|---|
| Mean (±SD) | Frequency (%) | Mean (±SD) | Frequency (%) | p-Value | ||
| Age (years) | 35.52 ± 6.52 | 33.36 ± 8.40 | ||||
| Education | High school diploma or lower | 10 (40%) | 13 (52%) | |||
| Higher education | 15 (60%) | 12 (48%) | ||||
| Employment | Employed | 8 (32%) | 5 (20%) | |||
| Unemployed | 17 (68%) | 20 (80%) | ||||
| Medication | Sertraline | 13 (52%) | 13 (52%) | |||
| Escitalopram | 5 (20%) | 6 (24%) | ||||
| Paroxetine | 4 (16%) | 3 (12%) | ||||
| Citalopram | - | 1 (4%) | ||||
| Fluvoxamine | 3 (12%) | 2 (8%) | ||||
| Previous psychiatric diagnosis | Depressive disorders | 17 (68%) | 11 (44%) | |||
| Anxiety disorders | 4 (16%) | 8 (32%) | ||||
| Obsessive-compulsive and related disorders | 4 (16%) | 6 (24%) | ||||
| FSFI scores | ||||||
| Arousal | 2.32 ± 0.94 | 3.70 ± 0.89 | <0.001 * | |||
| Desire | 2.73 ± 1.01 | 3.55 ± 0.66 | <0.001 * | |||
| Orgasm | 3.12 ± 0.92 | 4 ± 1.09 | 0.001 * | |||
| Pain | 4.48 ± 1.26 | 4.91 ± 1 | 0.294 | |||
| Satisfaction | 2.99 ± 1.28 | 3.93 ± 1.11 | 0.012 * | |||
| Lubrication | 3.9 ± 1.09 | 4.8 ± 1.05 | 0.004 * | |||
| Total | 19.55 ± 5.17 | 25.28 ± 4.62 | <0.001 * | |||
| Arousal | Desire | Orgasm | Pain | Satisfaction | Lubrication | Total | ||
|---|---|---|---|---|---|---|---|---|
| Drug holidays’ group | ||||||||
| Baseline | Week 4 | 0.021 * | 0.079 * | 0.135 | 0.885 | 0.018 * | 0.136 | 0.003 * |
| Week 4 | Week 8 | 0.001 * | 0.004 * | <0.001 * | 1 | 0.012 * | 0.999 | 0.001 * |
| Baseline | Week 8 | <0.001 * | 0.002 * | <0.001 * | 0.847 | <0.001 * | 0.041 * | <0.001 * |
| Control group | ||||||||
| Baseline | Week 4 | 1.00 | 1.00 | 0.963 | 1 | 1.00 | 0.269 | 0.896 |
| Week 4 | Week 8 | 1.00 | 0.039 * | 0.356 | 0.43 | 1.00 | 1.00 | 1.00 |
| Baseline | Week 8 | 1.00 | 0.585 | 0.307 | 0.585 | 1.00 | 0.425 | 1.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lalegani, E.; Eissazade, N.; Shalbafan, M.; Salehian, R.; Shariat, S.V.; Askari, S.; Orsolini, L.; Soraya, S. Safety and Efficacy of Drug Holidays for Women with Sexual Dysfunction Induced by Selective Serotonin Reuptake Inhibitors (SSRIs) Other than Fluoxetine: An Open-Label Randomized Clinical Trial. Brain Sci. 2023, 13, 1397. https://doi.org/10.3390/brainsci13101397
Lalegani E, Eissazade N, Shalbafan M, Salehian R, Shariat SV, Askari S, Orsolini L, Soraya S. Safety and Efficacy of Drug Holidays for Women with Sexual Dysfunction Induced by Selective Serotonin Reuptake Inhibitors (SSRIs) Other than Fluoxetine: An Open-Label Randomized Clinical Trial. Brain Sciences. 2023; 13(10):1397. https://doi.org/10.3390/brainsci13101397
Chicago/Turabian StyleLalegani, Elham, Negin Eissazade, Mohammadreza Shalbafan, Razieh Salehian, Seyed Vahid Shariat, Sanaz Askari, Laura Orsolini, and Shiva Soraya. 2023. "Safety and Efficacy of Drug Holidays for Women with Sexual Dysfunction Induced by Selective Serotonin Reuptake Inhibitors (SSRIs) Other than Fluoxetine: An Open-Label Randomized Clinical Trial" Brain Sciences 13, no. 10: 1397. https://doi.org/10.3390/brainsci13101397
APA StyleLalegani, E., Eissazade, N., Shalbafan, M., Salehian, R., Shariat, S. V., Askari, S., Orsolini, L., & Soraya, S. (2023). Safety and Efficacy of Drug Holidays for Women with Sexual Dysfunction Induced by Selective Serotonin Reuptake Inhibitors (SSRIs) Other than Fluoxetine: An Open-Label Randomized Clinical Trial. Brain Sciences, 13(10), 1397. https://doi.org/10.3390/brainsci13101397