

Dysfunction of the Lenticular Nucleus Is Associated with Dystonia in Wilson’s Disease
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Clinical and Muscle Biomechanical Assessment
2.3. MRI Acquisition
2.4. Data Preprocessing
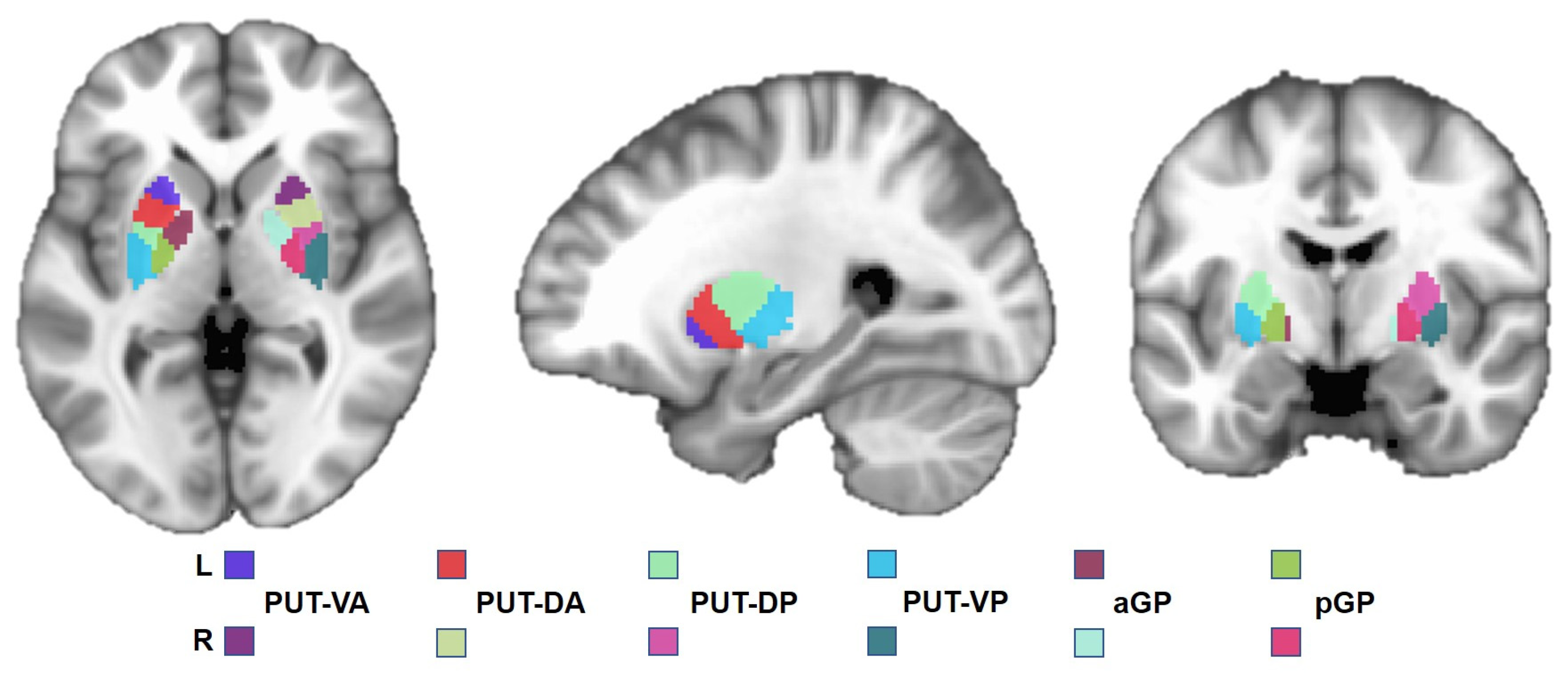
2.5. Regions of Interest
2.6. Functional Connectivity Analysis
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Muscle Tension
3.3. Group Comparison of FC between WD and HCs
3.4. Correlation between FC and UWDRS Score
3.5. Correlations between FC and Muscle Tension
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Aggarwal, A.; Bhatt, M. Wilson disease. Curr. Opin. Neurol. 2020, 33, 534–542. [Google Scholar] [CrossRef] [PubMed]
- Bandmann, O.; Weiss, K.H.; Kaler, S.G. Wilson’s disease and other neurological copper disorders. Lancet Neurol. 2015, 14, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Kalita, J.; Kumar, V.; Misra, U.K.; Kumar, S. Movement Disorder in Wilson Disease: Correlation with MRI and Biomarkers of Cell Injury. J. Mol. Neurosci. 2021, 71, 338–346. [Google Scholar] [CrossRef] [PubMed]
- King, A.D.; Walshe, J.M.; Kendall, B.E.; Chinn, R.J.; Paley, M.N.; Wilkinson, I.D.; Halligan, S.; Hall-Craggs, M.A. Cranial MR imaging in Wilson’s disease. Am. J. Roentgenol. 1996, 167, 1579–1584. [Google Scholar] [CrossRef] [PubMed]
- Hikosaka, O.; Takikawa, Y.; Kawagoe, R. Role of the basal ganglia in the control of purposive saccadic eye movements. Physiol. Rev. 2000, 80, 953–978. [Google Scholar] [CrossRef]
- Ikemoto, S.; Yang, C.; Tan, A. Basal ganglia circuit loops, dopamine and motivation: A review and enquiry. Behav. Brain Res. 2015, 290, 17–31. [Google Scholar] [CrossRef]
- Lanciego, J.L.; Luquin, N.; Obeso, J.A. Functional neuroanatomy of the basal ganglia. Cold Spring Harb. Perspect. Med. 2012, 2, a009621. [Google Scholar] [CrossRef]
- Richter, D.; Katsanos, A.H.; Schroeder, C.; Tsivgoulis, G.; Paraskevas, G.P.; Müller, T.; Alexandrov, A.V.; Gold, R.; Tönges, L.; Krogias, C. Lentiform Nucleus Hyperechogenicity in Parkinsonian Syndromes: A Systematic Review and Meta-Analysis with Consideration of Molecular Pathology. Cells 2019, 9, 2. [Google Scholar] [CrossRef]
- Walter, U.; Dressler, D.; Wolters, A.; Wittstock, M.; Benecke, R. Transcranial brain sonography findings in clinical subgroups of idiopathic Parkinson’s disease. Mov. Disord. Off. J. Mov. Disord. Soc. 2007, 22, 48–54. [Google Scholar] [CrossRef]
- Kim, T.J.; Kim, I.O.; Kim, W.S.; Cheon, J.E.; Moon, S.G.; Kwon, J.W.; Seo, J.K.; Yeon, K.M. MR imaging of the brain in Wilson disease of childhood: Findings before and after treatment with clinical correlation. Am. J. Neuroradiol. 2006, 27, 1373–1378. [Google Scholar]
- Zou, L.; Song, Y.; Zhou, X.; Chu, J.; Tang, X. Regional morphometric abnormalities and clinical relevance in Wilson’s disease. Mov. Disord. Off. J. Mov. Disord. Soc. 2019, 34, 545–554. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.; Xu, C.; Wang, Y.; Dong, T.; Wu, H.; Wang, A.; Li, C.; Qiu, B. Basal ganglia-orbitofrontal circuits are associated with prospective memory deficits in Wilson’s disease. Brain Imaging Behav. 2022, 16, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Jing, R.; Han, Y.; Cheng, H.; Han, Y.; Wang, K.; Weintraub, D.; Fan, Y. Altered large-scale functional brain networks in neurological Wilson’s disease. Brain Imaging Behav. 2020, 14, 1445–1455. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Cheng, H.; Toledo, J.B.; Wang, X.; Li, B.; Han, Y.; Wang, K.; Fan, Y. Impaired functional default mode network in patients with mild neurological Wilson’s disease. Park. Relat. Disord. 2016, 30, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Svetel, M.; Kozić, D.; Stefanova, E.; Semnic, R.; Dragasevic, N.; Kostic, V.S. Dystonia in Wilson’s disease. Mov. Disord. Off. J. Mov. Disord. Soc. 2001, 16, 719–723. [Google Scholar] [CrossRef]
- EASL Clinical Practice Guidelines: Wilson’s disease. J. Hepatol. 2012, 56, 671–685. [CrossRef]
- Romano, M.; Bagnato, S.; Altavista, M.C.; Avanzino, L.; Belvisi, D.; Bologna, M.; Bono, F.; Carecchio, M.; Castagna, A.; Ceravolo, R.; et al. Diagnostic and therapeutic recommendations in adult dystonia: A joint document by the Italian Society of Neurology, the Italian Academy for the Study of Parkinson’s Disease and Movement Disorders, and the Italian Network on Botulinum Toxin. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2022, 43, 6929–6945. [Google Scholar] [CrossRef]
- Albanese, A.; Bhatia, K.; Bressman, S.B.; Delong, M.R.; Fahn, S.; Fung, V.S.; Hallett, M.; Jankovic, J.; Jinnah, H.A.; Klein, C.; et al. Phenomenology and classification of dystonia: A consensus update. Mov. Disord. Off. J. Mov. Disord. Soc. 2013, 28, 863–873. [Google Scholar] [CrossRef]
- Nardocci, N. Myoclonus-dystonia syndrome. Handb. Clin. Neurol. 2011, 100, 563–575. [Google Scholar] [CrossRef]
- Lozeron, P.; Poujois, A.; Meppiel, E.; Masmoudi, S.; Magnan, T.P.; Vicaut, E.; Houdart, E.; Guichard, J.P.; Trocello, J.M.; Woimant, F.; et al. Inhibitory rTMS applied on somatosensory cortex in Wilson’s disease patients with hand dystonia. J. Neural Transm. 2017, 124, 1161–1170. [Google Scholar] [CrossRef]
- Cao, Z.; Rao, R.; Wu, T.; Chen, S.; Xing, S.; Han, Y. Botulinum toxin type A treatment of four cases of Wilson disease with lower limb dystonia: A prospective study. Toxicon Off. J. Int. Soc. Toxinol. 2022, 221, 106959. [Google Scholar] [CrossRef] [PubMed]
- Kukke, S.N.; Sanger, T.D. Contributors to excess antagonist activity during movement in children with secondary dystonia due to cerebral palsy. J. Neurophysiol. 2011, 105, 2100–2107. [Google Scholar] [CrossRef] [PubMed]
- Rome, S.; Grünewald, R.A. Abnormal perception of vibration-induced illusion of movement in dystonia. Neurology 1999, 53, 1794–1800. [Google Scholar] [CrossRef]
- Ando, R.; Sato, S.; Hirata, N.; Tanimoto, H.; Imaizumi, N.; Suzuki, Y.; Hirata, K.; Akagi, R. Relationship between resting medial gastrocnemius stiffness and drop jump performance. J. Electromyogr. Kinesiol. Off. J. Int. Soc. Electrophysiol. Kinesiol. 2021, 58, 102549. [Google Scholar] [CrossRef]
- Cazeau, C.; Stiglitz, Y. Effects of gastrocnemius tightness on forefoot during gait. Foot Ankle Clin. 2014, 19, 649–657. [Google Scholar] [CrossRef]
- Marusiak, J.; Jaskólska, A.; Koszewicz, M.; Budrewicz, S.; Jaskólski, A. Myometry revealed medication-induced decrease in resting skeletal muscle stiffness in Parkinson’s disease patients. Clin. Biomech. 2012, 27, 632–635. [Google Scholar] [CrossRef]
- Wang, J.S. Therapeutic effects of massage and electrotherapy on muscle tone, stiffness and muscle contraction following gastrocnemius muscle fatigue. J. Phys. Ther. Sci. 2017, 29, 144–147. [Google Scholar] [CrossRef]
- Huang, J.; Qin, K.; Tang, C.; Zhu, Y.; Klein, C.S.; Zhang, Z.; Liu, C. Assessment of Passive Stiffness of Medial and Lateral Heads of Gastrocnemius Muscle, Achilles Tendon, and Plantar Fascia at Different Ankle and Knee Positions Using the MyotonPRO. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2018, 24, 7570–7576. [Google Scholar] [CrossRef] [PubMed]
- Sohirad, S.; Wilson, D.; Waugh, C.; Finnamore, E.; Scott, A. Feasibility of using a hand-held device to characterize tendon tissue biomechanics. PLoS ONE 2017, 12, e0184463. [Google Scholar] [CrossRef]
- Hao, W.; Wei, T.; Yang, W.; Yang, Y.; Cheng, T.; Li, X.; Dong, W.; Jiang, H.; Qian, N.; Wang, H.; et al. Effects of High-Frequency Repetitive Transcranial Magnetic Stimulation on Upper Limb Dystonia in Patients with Wilson’s Disease: A Randomized Controlled Trial. Front. Neurol. 2021, 12, 783365. [Google Scholar] [CrossRef]
- Yan, C.G.; Wang, X.D.; Zuo, X.N.; Zang, Y.F. DPABI: Data Processing & Analysis for (Resting-State) Brain Imaging. Neuroinformatics 2016, 14, 339–351. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Margulies, D.S.; Breakspear, M.; Zalesky, A. Topographic organization of the human subcortex unveiled with functional connectivity gradients. Nat. Neurosci. 2020, 23, 1421–1432. [Google Scholar] [CrossRef] [PubMed]
- Członkowska, A.; Litwin, T. Wilson disease—currently used anticopper therapy. Handb. Clin. Neurol. 2017, 142, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Członkowska, A.; Litwin, T.; Dzieżyc, K.; Karliński, M.; Bring, J.; Bjartmar, C. Characteristics of a newly diagnosed Polish cohort of patients with neurological manifestations of Wilson disease evaluated with the Unified Wilson’s Disease Rating Scale. BMC Neurol. 2018, 18, 34. [Google Scholar] [CrossRef]
- Członkowska, A.; Litwin, T.; Dusek, P.; Ferenci, P.; Lutsenko, S.; Medici, V.; Rybakowski, J.K.; Weiss, K.H.; Schilsky, M.L. Wilson disease. Nat. Rev. Dis. Prim. 2018, 4, 21. [Google Scholar] [CrossRef]
- Martikainen, M.H.; Ng, Y.S.; Gorman, G.S.; Alston, C.L.; Blakely, E.L.; Schaefer, A.M.; Chinnery, P.F.; Burn, D.J.; Taylor, R.W.; McFarland, R.; et al. Clinical, Genetic, and Radiological Features of Extrapyramidal Movement Disorders in Mitochondrial Disease. JAMA Neurol. 2016, 73, 668–674. [Google Scholar] [CrossRef]
- Tanabe, L.M.; Kim, C.E.; Alagem, N.; Dauer, W.T. Primary dystonia: Molecules and mechanisms. Nat. Rev. Neurol. 2009, 5, 598–609. [Google Scholar] [CrossRef][Green Version]
- Song, Y.; Zou, L.; Zhao, J.; Zhou, X.; Huang, Y.; Qiu, H.; Han, H.; Yang, Z.; Li, X.; Tang, X.; et al. Whole brain volume and cortical thickness abnormalities in Wilson’s disease: A clinical correlation study. Brain Imaging Behav. 2021, 15, 1778–1787. [Google Scholar] [CrossRef]
- Dusek, P.; Lescinskij, A.; Ruzicka, F.; Acosta-Cabronero, J.; Bruha, R.; Sieger, T.; Hajek, M.; Dezortova, M. Associations of Brain Atrophy and Cerebral Iron Accumulation at MRI with Clinical Severity in Wilson Disease. Radiology 2021, 299, 662–672. [Google Scholar] [CrossRef]
- Shribman, S.; Bocchetta, M.; Sudre, C.H.; Acosta-Cabronero, J.; Burrows, M.; Cook, P.; Thomas, D.L.; Gillett, G.T.; Tsochatzis, E.A.; Bandmann, O.; et al. Neuroimaging correlates of brain injury in Wilson’s disease: A multimodal, whole-brain MRI study. Brain A J. Neurol. 2022, 145, 263–275. [Google Scholar] [CrossRef]
- Hu, S.; Xu, C.; Dong, T.; Wu, H.; Wang, Y.; Wang, A.; Kan, H.; Li, C. Structural and Functional Changes Are Related to Cognitive Status in Wilson’s Disease. Front. Hum. Neurosci. 2021, 15, 610947. [Google Scholar] [CrossRef]
- Vogt, B.A. Cingulate cortex in the three limbic subsystems. Handb. Clin. Neurol. 2019, 166, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Philippi, C.L.; Motzkin, J.C.; Pujara, M.S.; Koenigs, M. Subclinical depression severity is associated with distinct patterns of functional connectivity for subregions of anterior cingulate cortex. J. Psychiatr. Res. 2015, 71, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Glickstein, M.; Doron, K. Cerebellum: Connections and functions. Cerebellum 2008, 7, 589–594. [Google Scholar] [CrossRef] [PubMed]
- Shen, B.; Pan, Y.; Jiang, X.; Wu, Z.; Zhu, J.; Dong, J.; Zhang, W.; Xu, P.; Dai, Y.; Gao, Y.; et al. Altered putamen and cerebellum connectivity among different subtypes of Parkinson’s disease. CNS Neurosci. Ther. 2020, 26, 207–214. [Google Scholar] [CrossRef]
- Filip, P.; Lungu, O.V.; Bareš, M. Dystonia and the cerebellum: A new field of interest in movement disorders? Clin. Neurophysiol. 2013, 124, 1269–1276. [Google Scholar] [CrossRef]
- Glickman, A.; Nguyen, P.; Shelton, E.; Peterson, D.A.; Berman, B.D. Basal ganglia and cerebellar circuits have distinct roles in blepharospasm. Park. Relat. Disord. 2020, 78, 158–164. [Google Scholar] [CrossRef]
- Giannì, C.; Pasqua, G.; Ferrazzano, G.; Tommasin, S.; De Bartolo, M.I.; Petsas, N.; Belvisi, D.; Conte, A.; Berardelli, A.; Pantano, P. Focal Dystonia: Functional Connectivity Changes in Cerebellar-Basal Ganglia-Cortical Circuit and Preserved Global Functional Architecture. Neurology 2022, 98, e1499–e1509. [Google Scholar] [CrossRef]
- Stezin, A.; George, L.; Jhunjhunwala, K.; Lenka, A.; Saini, J.; Netravathi, M.; Yadav, R.; Pal, P.K. Exploring cortical atrophy and its clinical and biochemical correlates in Wilson’s disease using voxel based morphometry. Park. Relat. Disord. 2016, 30, 52–57. [Google Scholar] [CrossRef]
- Tinaz, S.; Arora, J.; Nalamada, K.; Vives-Rodriguez, A.; Sezgin, M.; Robakis, D.; Patel, A.; Constable, R.T.; Schilsky, M.L. Structural and functional brain changes in hepatic and neurological Wilson disease. Brain Imaging Behav. 2021, 15, 2269–2282. [Google Scholar] [CrossRef]
- Starosta-Rubinstein, S.; Young, A.B.; Kluin, K.; Hill, G.; Aisen, A.M.; Gabrielsen, T.; Brewer, G.J. Clinical assessment of 31 patients with Wilson’s disease. Correlations with structural changes on magnetic resonance imaging. Arch. Neurol. 1987, 44, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Schuurman, P.R.; de Bie, R.M.; Speelman, J.D.; Bosch, D.A. Posteroventral pallidotomy in movement disorders. Acta Neurochir. Suppl. 1997, 68, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Fung, W.K.W.; Peall, K.J. What is the role of the cerebellum in the pathophysiology of dystonia? J. Neurol. 2019, 266, 1549–1551. [Google Scholar] [CrossRef] [PubMed]
- Iannone, A.; Cruz, A.P.; Brasil-Neto, J.P.; Boechat-Barros, R. Transcranial magnetic stimulation and transcranial direct current stimulation appear to be safe neuromodulatory techniques useful in the treatment of anxiety disorders and other neuropsychiatric disorders. Arq. De Neuro-Psiquiatr. 2016, 74, 829–835. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.M.; Li, C.T.; Tsai, S.J. Current Updates on Newer Forms of Transcranial Magnetic Stimulation in Major Depression. Adv. Exp. Med. Biol. 2021, 1305, 333–349. [Google Scholar] [CrossRef]
- Depping, M.S.; Schmitgen, M.M.; Kubera, K.M.; Wolf, R.C. Cerebellar Contributions to Major Depression. Front. Psychiatry 2018, 9, 634. [Google Scholar] [CrossRef]
- Ebert, D.; Feistel, H.; Barocka, A.; Kaschka, W.; Mokrusch, T. A test-retest study of cerebral blood flow during somatosensory stimulation in depressed patients with schizophrenia and major depression. Eur. Arch. Psychiatry Clin. Neurosci. 1993, 242, 250–254. [Google Scholar] [CrossRef]
- Yeganeh-Doost, P.; Gruber, O.; Falkai, P.; Schmitt, A. The role of the cerebellum in schizophrenia: From cognition to molecular pathways. Clinics 2011, 66 (Suppl. S1), 71–77. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Patient |
|---|---|
| Gender (man/woman) Symptoms (neurological/neuropsychiatric) Age (years) Handedness Duration (years) UWDRS-N UWDRS-P K-F ring (+/−) CER U-cu | 20/17 37/26 12–37 (23.95 ± 6.95) 37 right-handed 1–24 (9.59 ± 5.39) 1–29 (10.49 ± 7.56) 0–10 (3.49 ± 2.55) 34/3 <0.1 g/L >100 µg/24 h |
| ROIs | Regions | MNI Coordinate | Peak Z Value | ||
|---|---|---|---|---|---|
| x | y | z | |||
| L-PUT-VA | Left cerebellum | −26 | −68 | −60 | −3.95 |
| Right MCC | 4 | 0 | 42 | −3.97 | |
| L-PUT-DA | Left cerebellum | 0 | −66 | −18 | −4.34 |
| Right MCC | 4 | 0 | 44 | −4.23 | |
| L-PUT-VP | Right cerebellum | 30 | −60 | −54 | −4.68 |
| Right MCC | 2 | 0 | 44 | −4.20 | |
| L-PUT-DP | Left cerebellum | −10 | −64 | −14 | −4.65 |
| Right MCC | 4 | 2 | 44 | −4.40 | |
| R_PUT-VA | Right cerebellum | 10 | −64 | −14 | −5.04 |
| Right MCC | 2 | 2 | 44 | −4.62 | |
| R-PUT-DA | Right cerebellum | 10 | −66 | −14 | −4.78 |
| Right MCC | 2 | 0 | 44 | −4.21 | |
| R-PUT-VP | Left cerebellum | −10 | −74 | −48 | −4.94 |
| R-PUT-DP | Right cerebellum | 28 | −64 | −20 | −4.83 |
| Right MCC | 2 | −2 | 44 | −4.68 | |
| ROIs | Regions | MNI Coordinate | Peak Z Value | ||
|---|---|---|---|---|---|
| x | y | z | |||
| L-pGP | R cerebellum | 6 | −76 | −24 | −4.22 |
| L-aGP | R cerebellum | 10 | −76 | −24 | −4.99 |
| R-pGP | Left MCC | 0 | 8 | 42 | −3.92 |
| Left cerebellum | −12 | −78 | −48 | −4.78 | |
| R-aGP | Right MCC | 2 | 4 | 42 | −4.46 |
| Right cerebellum | −28 | −72 | −24 | −5.14 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, Y.; Wei, T.; Yang, W.; Hu, S.; Jiang, H.; Dong, W.; Hao, W.; Yang, Y.; Qian, N.; Ding, Y. Dysfunction of the Lenticular Nucleus Is Associated with Dystonia in Wilson’s Disease. Brain Sci. 2023, 13, 7. https://doi.org/10.3390/brainsci13010007
Yang Y, Wei T, Yang W, Hu S, Jiang H, Dong W, Hao W, Yang Y, Qian N, Ding Y. Dysfunction of the Lenticular Nucleus Is Associated with Dystonia in Wilson’s Disease. Brain Sciences. 2023; 13(1):7. https://doi.org/10.3390/brainsci13010007
Chicago/Turabian StyleYang, Yulong, Taohua Wei, Wenming Yang, Sheng Hu, Hailin Jiang, Wei Dong, Wenjie Hao, Yue Yang, Nannan Qian, and Yufeng Ding. 2023. "Dysfunction of the Lenticular Nucleus Is Associated with Dystonia in Wilson’s Disease" Brain Sciences 13, no. 1: 7. https://doi.org/10.3390/brainsci13010007
APA StyleYang, Y., Wei, T., Yang, W., Hu, S., Jiang, H., Dong, W., Hao, W., Yang, Y., Qian, N., & Ding, Y. (2023). Dysfunction of the Lenticular Nucleus Is Associated with Dystonia in Wilson’s Disease. Brain Sciences, 13(1), 7. https://doi.org/10.3390/brainsci13010007