
Carbamazepine for Chronic Muscle Pain: A Retrospective Assessment of Indications, Side Effects, and Treatment Response

Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
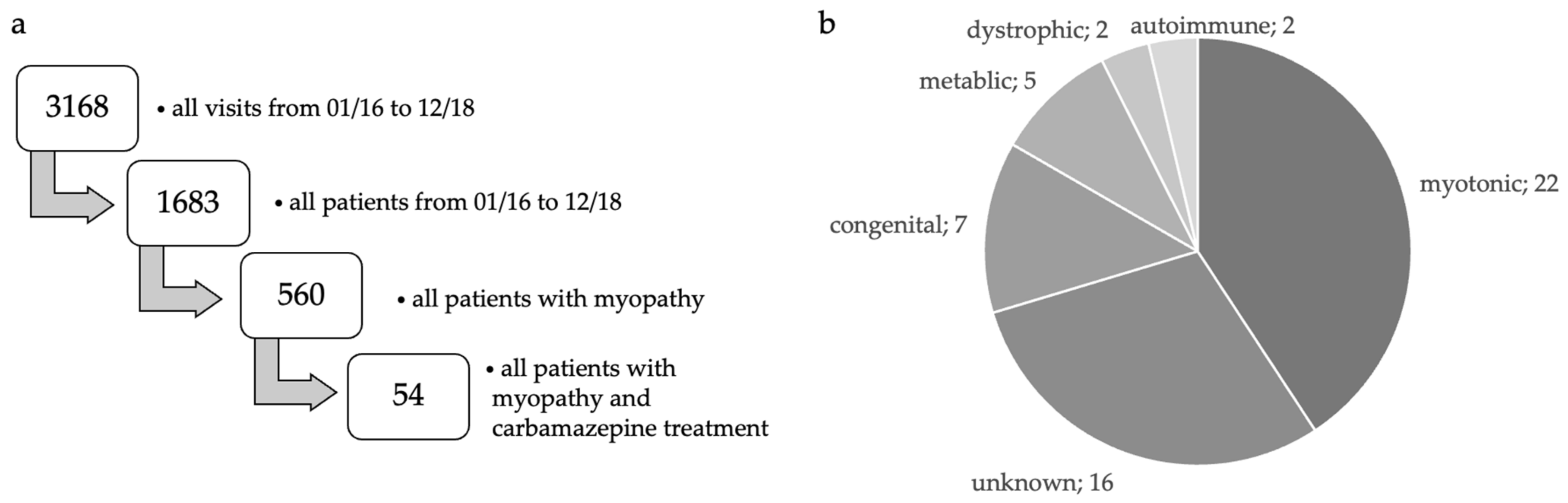
2.2. Patient Selection
2.3. Clinical Interview
2.4. Screening for a Neuropathic Pain Component
2.5. Quantitative Sensory Testing (QST)
2.6. Laboratory Blood Tests
2.7. Statistics
3. Results
3.1. Patient Description
3.2. Pain Assessment
3.3. Clinical Findings
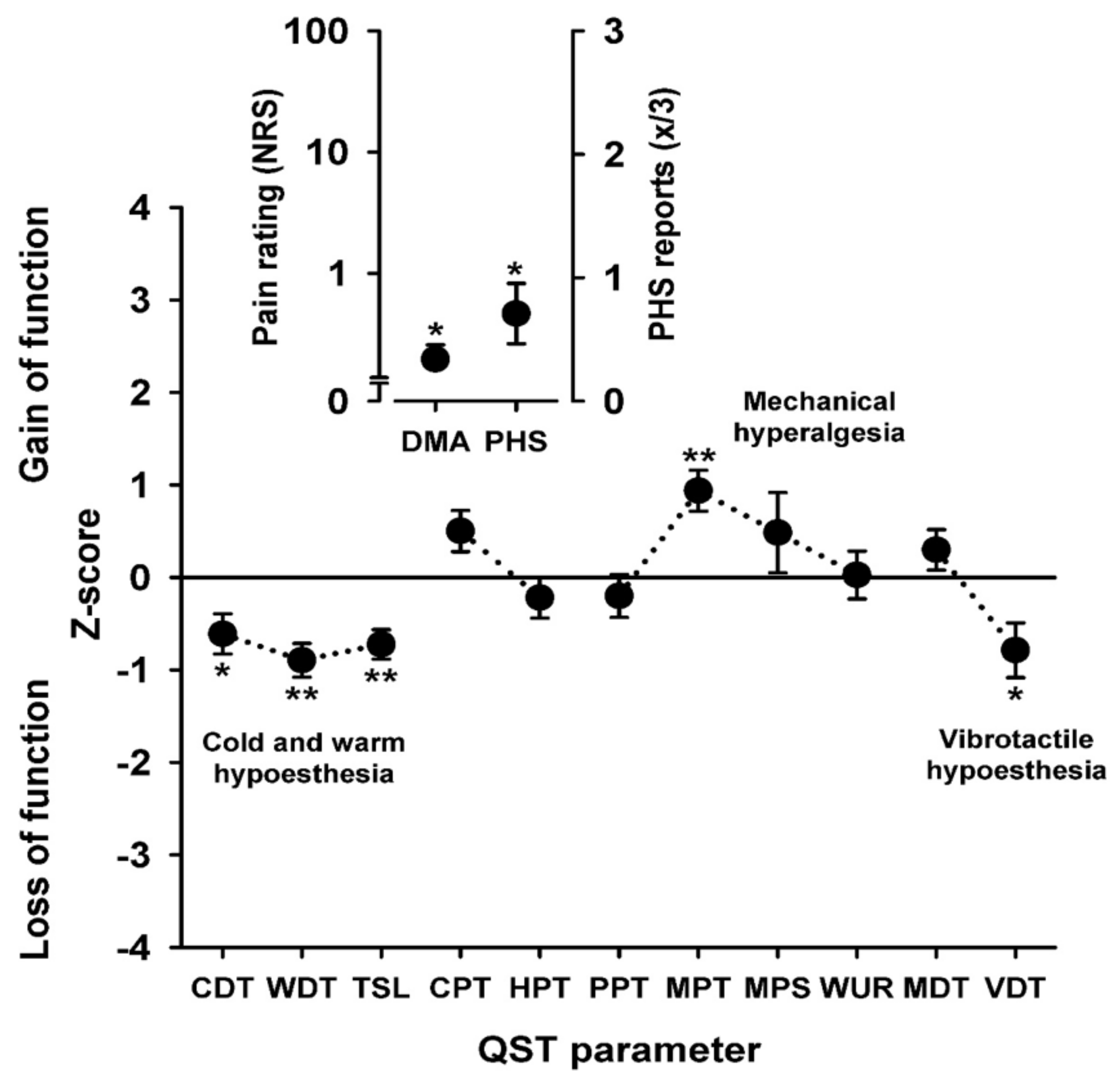
3.4. Sensory Profiles
3.5. Carbamazepine Treatment: Duration, Dosage, Side Effects
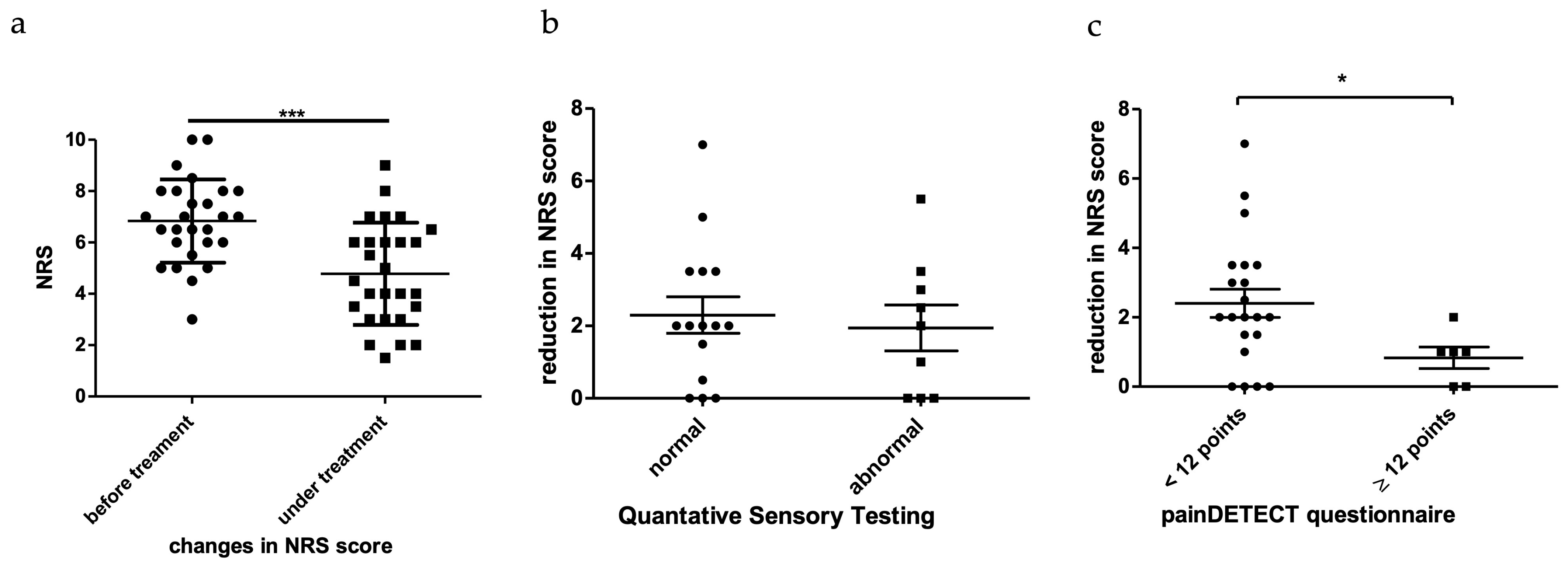
3.6. Response to Carbamazepine
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Rull, J.A.; Quibrera, R.; Gonzalez-Millan, H.; Lozano Castaneda, O. Symptomatic treatment of peripheral diabetic neuropathy with carbamazepine (Tegretol): Double blind crossover trial. Diabetologia 1969, 5, 215–218. [Google Scholar] [CrossRef]
- Blom, S. Trigeminal neuralgia: Its treatment with a new anticonvulsant drug (G-32883). Lancet 1962, 1, 839–840. [Google Scholar] [CrossRef]
- Taylor, J.C.; Brauer, S.; Espir, M.L. Long-term treatment of trigeminal neuralgia with carbamazepine. Postgrad. Med. J. 1981, 57, 16–18. [Google Scholar] [CrossRef] [PubMed]
- Neuromuscular Disease Center, W.U. Muscle Pain & Discomfort. Available online: https://neuromuscular.wustl.edu/mother/mpain.html (accessed on 20 April 2021).
- Jensen, M.P.; Abresch, R.T.; Carter, G.T.; McDonald, C.M. Chronic pain in persons with neuromuscular disease. Arch. Phys. Med. Rehabil. 2005, 86, 1155–1163. [Google Scholar] [CrossRef]
- Jensen, M.P.; Hoffman, A.J.; Stoelb, B.L.; Abresch, R.T.; Carter, G.T.; McDonald, C.M. Chronic pain in persons with myotonic dystrophy and facioscapulohumeral dystrophy. Arch. Phys. Med. Rehabil. 2008, 89, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Kalkman, J.S.; Schillings, M.L.; van der Werf, S.P.; Padberg, G.W.; Zwarts, M.J.; van Engelen, B.G.; Bleijenberg, G. Experienced fatigue in facioscapulohumeral dystrophy, myotonic dystrophy, and HMSN-I. J. Neurol. Neurosurg. Psychiatry 2005, 76, 1406–1409. [Google Scholar] [CrossRef] [PubMed]
- Padua, L.; Aprile, I.; Frusciante, R.; Iannaccone, E.; Rossi, M.; Renna, R.; Messina, S.; Frasca, G.; Ricci, E. Quality of life and pain in patients with facioscapulohumeral muscular dystrophy. Muscle Nerve 2009, 40, 200–205. [Google Scholar] [CrossRef]
- Ponyi, A.; Borgulya, G.; Constantin, T.; Vancsa, A.; Gergely, L.; Danko, K. Functional outcome and quality of life in adult patients with idiopathic inflammatory myositis. Rheumatology 2005, 44, 83–88. [Google Scholar] [CrossRef]
- Abresch, R.T.; Carter, G.T.; Jensen, M.P.; Kilmer, D.D. Assessment of pain and health-related quality of life in slowly progressive neuromuscular disease. Am. J. Hosp. Palliat. Care 2002, 19, 39–48. [Google Scholar] [CrossRef]
- Graham, C.D.; Rose, M.R.; Grunfeld, E.A.; Kyle, S.D.; Weinman, J. A systematic review of quality of life in adults with muscle disease. J. Neurol. 2011, 258, 1581–1592. [Google Scholar] [CrossRef]
- Statland, J.M.; Bundy, B.N.; Wang, Y.; Rayan, D.R.; Trivedi, J.R.; Sansone, V.A.; Salajegheh, M.K.; Venance, S.L.; Ciafaloni, E.; Matthews, E.; et al. Mexiletine for symptoms and signs of myotonia in nondystrophic myotonia: A randomized controlled trial. JAMA 2012, 308, 1357–1365. [Google Scholar] [CrossRef] [PubMed]
- Neuromuscular Disease Center, W.U. Muscle Fiber Activity & Cramps. Available online: https://neuromuscular.wustl.edu/mother/activity.html#mcd (accessed on 20 April 2021).
- Neuromuscular Disease Center, W.U. Inflammatory and Immune Myopathies (IIM): Acquired. Available online: https://neuromuscular.wustl.edu/antibody/infmyop.htm#pain (accessed on 20 April 2021).
- Neuromuscular Disease Center, W.U. Facioscapulohumeral (FSH) Dystrophy. Available online: https://neuromuscular.wustl.edu/pathol/fsh.htm (accessed on 20 April 2021).
- Neuromuscular Disease Center, W.U. Muscular Dystrophy Syndromes. Available online: https://neuromuscular.wustl.edu/musdist/lg.html#lgmdgen (accessed on 20 April 2021).
- Neuromuscular Disease Center, W.U. Glycogen & Glucose Metabolic Disorders. Available online: https://neuromuscular.wustl.edu/msys/glycogen.html#McA (accessed on 20 April 2021).
- Neuromuscular Disease Center, W.U. Mitochondrial Disorders. Available online: http://neuromuscular.wustl.edu/mitosyn.html#myop (accessed on 20 April 2021).
- Santiago, S.; Espinosa, M.L.; Perez-Conde, M.C.; Merino, M.; Ferrer, T. [Small fiber dysfunction in peripheral neuropathies]. Rev. Neurol. 1999, 28, 543–554. [Google Scholar] [PubMed]
- Sene, D. Small fiber neuropathy: Diagnosis, causes, and treatment. Joint Bone Spine 2018, 85, 553–559. [Google Scholar] [CrossRef] [PubMed]
- Lawson, V.H.; Grewal, J.; Hackshaw, K.V.; Mongiovi, P.C.; Stino, A.M. Fibromyalgia syndrome and small fiber, early or mild sensory polyneuropathy. Muscle Nerve 2018, 58, 625–630. [Google Scholar] [CrossRef]
- Martinez-Lavin, M. Fibromyalgia and small fiber neuropathy: The plot thickens! Clin. Rheumatol. 2018, 37, 3167–3171. [Google Scholar] [CrossRef]
- Graven-Nielsen, T.; Mense, S. The peripheral apparatus of muscle pain: Evidence from animal and human studies. Clin. J. Pain 2001, 17, 2–10. [Google Scholar] [CrossRef]
- Graven-Nielsen, T.; Arendt-Nielsen, L. Assessment of mechanisms in localized and widespread musculoskeletal pain. Nat. Rev. Rheumatol. 2010, 6, 599–606. [Google Scholar] [CrossRef]
- Queme, L.F.; Jankowski, M.P. Sex differences and mechanisms of muscle pain. Curr. Opin. Physiol. 2019, 11, 6. [Google Scholar] [CrossRef] [PubMed]
- Williamson, A.; Hoggart, B. Pain: A review of three commonly used pain rating scales. J. Clin. Nurs. 2005, 14, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Rolke, R.; Baron, R.; Maier, C.; Tolle, T.R.; Treede, R.D.; Beyer, A.; Binder, A.; Birbaumer, N.; Birklein, F.; Botefur, I.C.; et al. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): Standardized protocol and reference values. Pain 2006, 123, 231–243. [Google Scholar] [CrossRef]
- Rolke, R.; Magerl, W.; Campbell, K.A.; Schalber, C.; Caspari, S.; Birklein, F.; Treede, R.D. Quantitative sensory testing: A comprehensive protocol for clinical trials. Eur. J. Pain 2006, 10, 77–88. [Google Scholar] [CrossRef]
- Rolke, R.; Rolke, S.; Vogt, T.; Birklein, F.; Geber, C.; Treede, R.D.; Letzel, S.; Voelter-Mahlknecht, S. Hand-arm vibration syndrome: Clinical characteristics, conventional electrophysiology and quantitative sensory testing. Clin. Neurophysiol. 2013, 124, 1680–1688. [Google Scholar] [CrossRef]
- Magerl, W.; Krumova, E.K.; Baron, R.; Tolle, T.; Treede, R.D.; Maier, C. Reference data for quantitative sensory testing (QST): Refined stratification for age and a novel method for statistical comparison of group data. Pain 2010, 151, 598–605. [Google Scholar] [CrossRef]
- Maier, C.; Baron, R.; Tolle, T.R.; Binder, A.; Birbaumer, N.; Birklein, F.; Gierthmuhlen, J.; Flor, H.; Geber, C.; Huge, V.; et al. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): Somatosensory abnormalities in 1236 patients with different neuropathic pain syndromes. Pain 2010, 150, 439–450. [Google Scholar] [CrossRef] [PubMed]
- Doughty, C.T.; Amato, A.A. Toxic Myopathies. Continuum (Minneap Minn) 2019, 25, 1712–1731. [Google Scholar] [CrossRef]
- Azemawah, V.; Movahed, M.R.; Centuori, P.; Penaflor, R.; Riel, P.L.; Situ, S.; Shadmehr, M.; Hashemzadeh, M. State of the Art Comprehensive Review of Individual Statins, Their Differences, Pharmacology, and Clinical Implications. Cardiovasc. Drugs Ther. 2019, 33, 625–639. [Google Scholar] [CrossRef]
- Thompson, P.D.; Clarkson, P.; Karas, R.H. Statin-associated myopathy. JAMA 2003, 289, 1681–1690. [Google Scholar] [CrossRef] [PubMed]
- Preedy, V.R.; Ohlendieck, K.; Adachi, J.; Koll, M.; Sneddon, A.; Hunter, R.; Rajendram, R.; Mantle, D.; Peters, T.J. The importance of alcohol-induced muscle disease. J. Muscle Res. Cell Motil. 2003, 24, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Freynhagen, R.; Tolle, T.R.; Gockel, U.; Baron, R. The painDETECT project—Far more than a screening tool on neuropathic pain. Curr. Med. Res. Opin. 2016, 32, 1033–1057. [Google Scholar] [CrossRef] [PubMed]
- Geber, C.; Klein, T.; Azad, S.; Birklein, F.; Gierthmuhlen, J.; Huge, V.; Lauchart, M.; Nitzsche, D.; Stengel, M.; Valet, M.; et al. Test-retest and interobserver reliability of quantitative sensory testing according to the protocol of the German Research Network on Neuropathic Pain (DFNS): A multi-centre study. Pain 2011, 152, 548–556. [Google Scholar] [CrossRef] [PubMed]
- Mucke, M.; Cuhls, H.; Radbruch, L.; Baron, R.; Maier, C.; Tolle, T.; Treede, R.D.; Rolke, R. Quantitative sensory testing (QST). English version. Schmerz 2021, 35, 153–160. [Google Scholar] [CrossRef]
- Hansson, P.; Backonja, M.; Bouhassira, D. Usefulness and limitations of quantitative sensory testing: Clinical and research application in neuropathic pain states. Pain 2007, 129, 256–259. [Google Scholar] [CrossRef] [PubMed]
- Roicke, H.; Kohler, W.; Baum, P.; Baerwald, C.; Krasselt, M. [Non-inflammatory muscle pain]. Dtsch Med. Wochenschr. 2020, 145, 887–894. [Google Scholar] [CrossRef]
- Filosto, M.; Cotti Piccinelli, S.; Lamperti, C.; Mongini, T.; Servidei, S.; Musumeci, O.; Tonin, P.; Santorelli, F.M.; Simoncini, C.; Primiano, G.; et al. Muscle pain in mitochondrial diseases: A picture from the Italian network. J. Neurol. 2019, 266, 953–959. [Google Scholar] [CrossRef]
- Gerwin, R. The Enigma of Muscle Pain: A Neglected Entity. Pain Med. 2019, 20, 1261–1264. [Google Scholar] [CrossRef]
- Ambrosio, A.F.; Soares-Da-Silva, P.; Carvalho, C.M.; Carvalho, A.P. Mechanisms of action of carbamazepine and its derivatives, oxcarbazepine, BIA 2-093, and BIA 2-024. Neurochem. Res. 2002, 27, 121–130. [Google Scholar] [CrossRef]
- Sánchez-Romero, E.A.; González-Zamorano, Y.; Arribas-Romano, A.; Martínez-Pozas, O.; Fernández Espinar, E.; Pedersini, P.; Villafañe, J.H.; Alonso Pérez, J.L.; Fernández-Carnero, J. Efficacy of Manual Therapy on Facilitatory Nociception and Endogenous Pain Modulation in Older Adults with Knee Osteoarthritis: A Case Series. Appl. Sci. 2021, 11, 1895. [Google Scholar] [CrossRef]
- Sanchez Romero, E.A.; Fernandez Carnero, J.; Villafane, J.H.; Calvo-Lobo, C.; Ochoa Saez, V.; Burgos Caballero, V.; Laguarta Val, S.; Pedersini, P.; Pecos Martin, D. Prevalence of Myofascial Trigger Points in Patients with Mild to Moderate Painful Knee Osteoarthritis: A Secondary Analysis. J. Clin. Med. 2020, 9, 2561. [Google Scholar] [CrossRef]
- Pellock, J.M. Carbamazepine side effects in children and adults. Epilepsia 1987, 28 (Suppl. 3), S64–S70. [Google Scholar] [CrossRef]
- Trivedi, J.R.; Bundy, B.; Statland, J.; Salajegheh, M.; Rayan, D.R.; Venance, S.L.; Wang, Y.; Fialho, D.; Matthews, E.; Cleland, J.; et al. Non-dystrophic myotonia: Prospective study of objective and patient reported outcomes. Brain 2013, 136, 2189–2200. [Google Scholar] [CrossRef]
- Stunnenberg, B.C.; Woertman, W.; Raaphorst, J.; Statland, J.M.; Griggs, R.C.; Timmermans, J.; Saris, C.G.; Schouwenberg, B.J.; Groenewoud, H.M.; Stegeman, D.F.; et al. Combined N-of-1 trials to investigate mexiletine in non-dystrophic myotonia using a Bayesian approach; study rationale and protocol. BMC Neurol. 2015, 15, 43. [Google Scholar] [CrossRef] [PubMed]
- Modoni, A.; D’Amico, A.; Primiano, G.; Capozzoli, F.; Desaphy, J.F.; Lo Monaco, M. Long-Term Safety and Usefulness of Mexiletine in a Large Cohort of Patients Affected by Non-dystrophic Myotonias. Front. Neurol. 2020, 11, 300. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Unknown | Metabolic | Congenital | Myotonic | Dystrophic | Autoimmune | |||
|---|---|---|---|---|---|---|---|---|
| sex | m:f (age in years) | 9:7 (49.5:47.4) | 4:1 (50.65:25) | 5:2 (48.13:56) | 22:0 (55.43) | 1:1 (80:60) | 1:1 (54:46) | |
| general information | AOO (years) | 33.19 | 24.3 | 33 | 35.99 | 52 | 45 | |
| duration (years) | 15.45 | 19.6 | 20.25 | 19.32 | 13 | 4 | ||
| first symptoms | myalgia | 16 | 5 | 6 | 18 | 1 | ||
| muscle weakness | 3 | 2 | 1 | 4 | 2 | |||
| muscle cramps | 5 | 1 | 2 | 12 | 1 | |||
| fasciculations | 3 | 12 | ||||||
| muscle stiffness | 1 | 3 | 1 | |||||
| rhabdomyolysis | 1 | |||||||
| elevated CK levels | 1 | 3 | ||||||
| arthralgia | 1 | |||||||
| current symptoms | myalgia | 16 | 5 | 6 | 18 | 1 | ||
| muscle weakness | 6 | 2 | 2 | 6 | 2 | |||
| muscle cramps | 6 | 1 | 1 | 11 | 1 | |||
| fasciculations | 3 | 8 | ||||||
| muscle stiffness | 2 | 1 | ||||||
| elevated CK levels | 1 | |||||||
| hypermobile joints | 1 | |||||||
| signs of myopathy | unsteady gait | 5 | 1 | 2 | 2 | 1 | ||
| Gower’s sign | 1 | 1 | ||||||
| inability to squat | 6 | 1 | 4 | |||||
| muscle atrophies | 4 | 1 | 2 | 2 | 1 | |||
| scapular winging | 4 | 2 | ||||||
| scoliosis | 4 | 1 | 1 | |||||
| fasciculations | 1 | 3 | ||||||
| myotonia | 1 | 3 | ||||||
| myoclonus | 1 | |||||||
| rippling | 1 | |||||||
| weakness | 1 | |||||||
| ptosis | 1 | 1 | 1 | |||||
| signe des cils | 1 | 2 | ||||||
| deep tendon reflexes | normal | 14 | 4 | 7 | 19 | 1 | ||
| reduced | 2 | 1 | 1 | 3 | 2 | 1 | ||
| MRC [x/5] | proximal weakness | yes | 8 | 3 | 3 | 4 | 2 | 2 |
| no | 8 | 2 | 4 | 18 | ||||
| distal weakness | yes | 6 | 3 | 2 | 3 | 2 | ||
| no | 10 | 2 | 5 | 19 | 2 | |||
| NRS | before treatment | 6.19 | 9 | 7 | 6.19 | no data | 7 | |
| under treatment | 5 | 7.5 | 4.33 | 4 | no data | 6.5 | ||
| carbamazepine | dosage (mg) | 200 | 200 | 200 | 401.39 | 200 | 200 | |
| duration (months) | 4.55 | 12 | 13.83 | 45.6 | 8 | 49 | ||
| improvement | yes | 7 | 5 | 2 | 11 | 1 | ||
| not sure | 3 | 2 | 2 | 1 | ||||
| no | 3 | 2 | 1 | 1 | ||||
| QST | normal | 7 | 2 | 4 | no data | 1 | ||
| abnormal | 3 | 1 | 2 | 3 | no data | |||
| Adverse Side Effects Observed under Carbamazepine | Occurrence | Carbamazepine Stopped |
|---|---|---|
| not specified | 18 | no data |
| none | 8 | 0 |
| fatigue | 8 | 7 |
| no improvement | 6 | 6 |
| liver enzyme elevation | 4 | 4 |
| diarrhea | 2 | 2 |
| hospitalization due to skin condition | 2 | 2 |
| family planning | 1 | 1 |
| hypersomnia | 1 | 1 |
| eczema | 1 | 1 |
| hypersensitivity to sunlight | 1 | 1 |
| carbamazepine-induced LE | 1 | 1 |
| nausea | 1 | 1 |
| mood swings | 1 | 1 |
| depression | 1 | 1 |
| intolerance | 1 | 1 |
| vertigo | 1 | 1 |
| stomach ache | 1 | 1 |
| total | 59 | 32 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dyong, T.M.; Gess, B.; Dumke, C.; Rolke, R.; Dohrn, M.F. Carbamazepine for Chronic Muscle Pain: A Retrospective Assessment of Indications, Side Effects, and Treatment Response. Brain Sci. 2023, 13, 123. https://doi.org/10.3390/brainsci13010123
Dyong TM, Gess B, Dumke C, Rolke R, Dohrn MF. Carbamazepine for Chronic Muscle Pain: A Retrospective Assessment of Indications, Side Effects, and Treatment Response. Brain Sciences. 2023; 13(1):123. https://doi.org/10.3390/brainsci13010123
Chicago/Turabian StyleDyong, Tabea M., Burkhard Gess, Christina Dumke, Roman Rolke, and Maike F. Dohrn. 2023. "Carbamazepine for Chronic Muscle Pain: A Retrospective Assessment of Indications, Side Effects, and Treatment Response" Brain Sciences 13, no. 1: 123. https://doi.org/10.3390/brainsci13010123
APA StyleDyong, T. M., Gess, B., Dumke, C., Rolke, R., & Dohrn, M. F. (2023). Carbamazepine for Chronic Muscle Pain: A Retrospective Assessment of Indications, Side Effects, and Treatment Response. Brain Sciences, 13(1), 123. https://doi.org/10.3390/brainsci13010123