
Deep Brain Stimulation in Early-Stage Parkinson’s Disease: Patient Experience after 11 Years


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
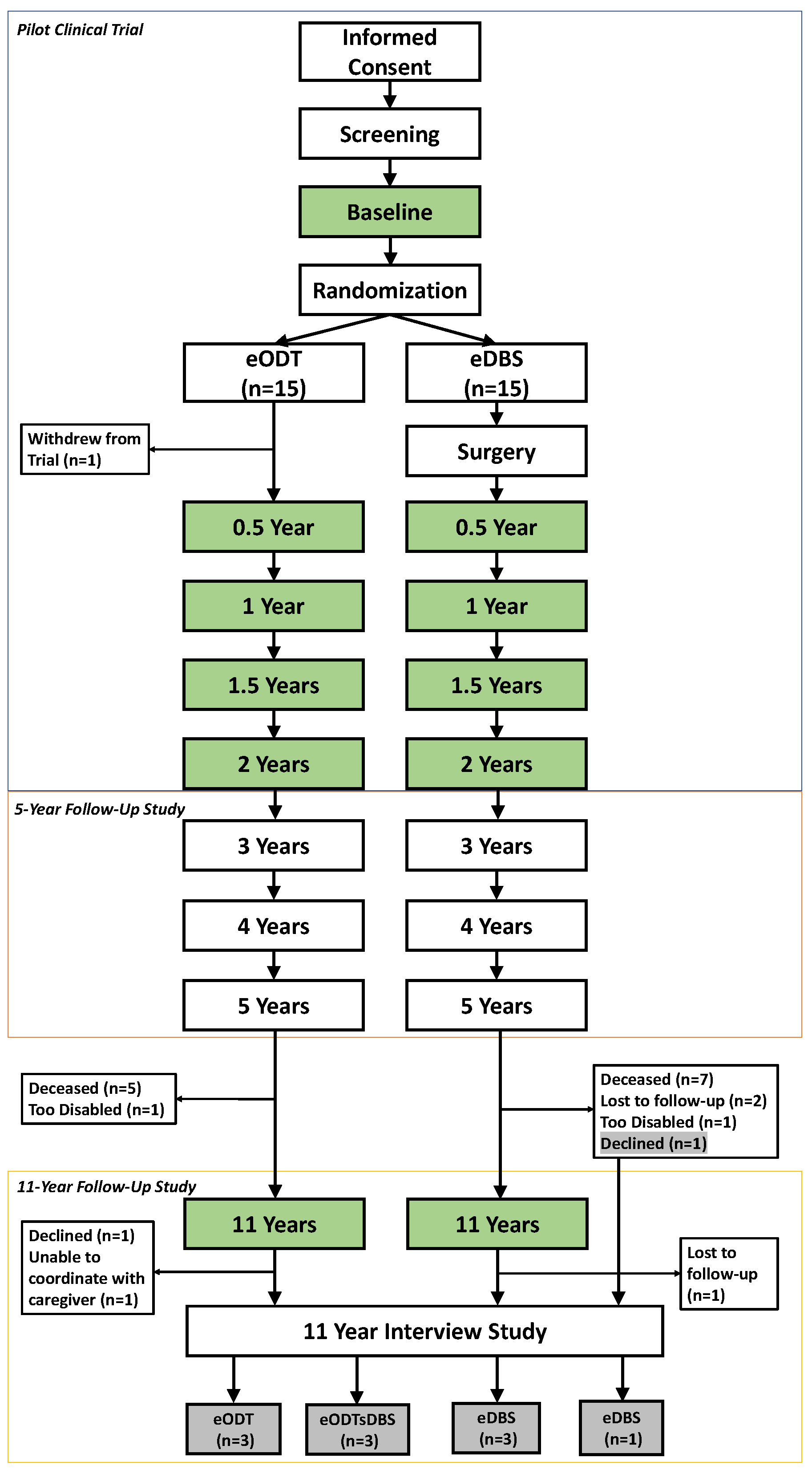
2.1.1. DBS in Early PD Pilot Trial
2.1.2. Interview Study
2.2. Data Collection
2.3. Data Analysis
3. Results
3.1. Patients
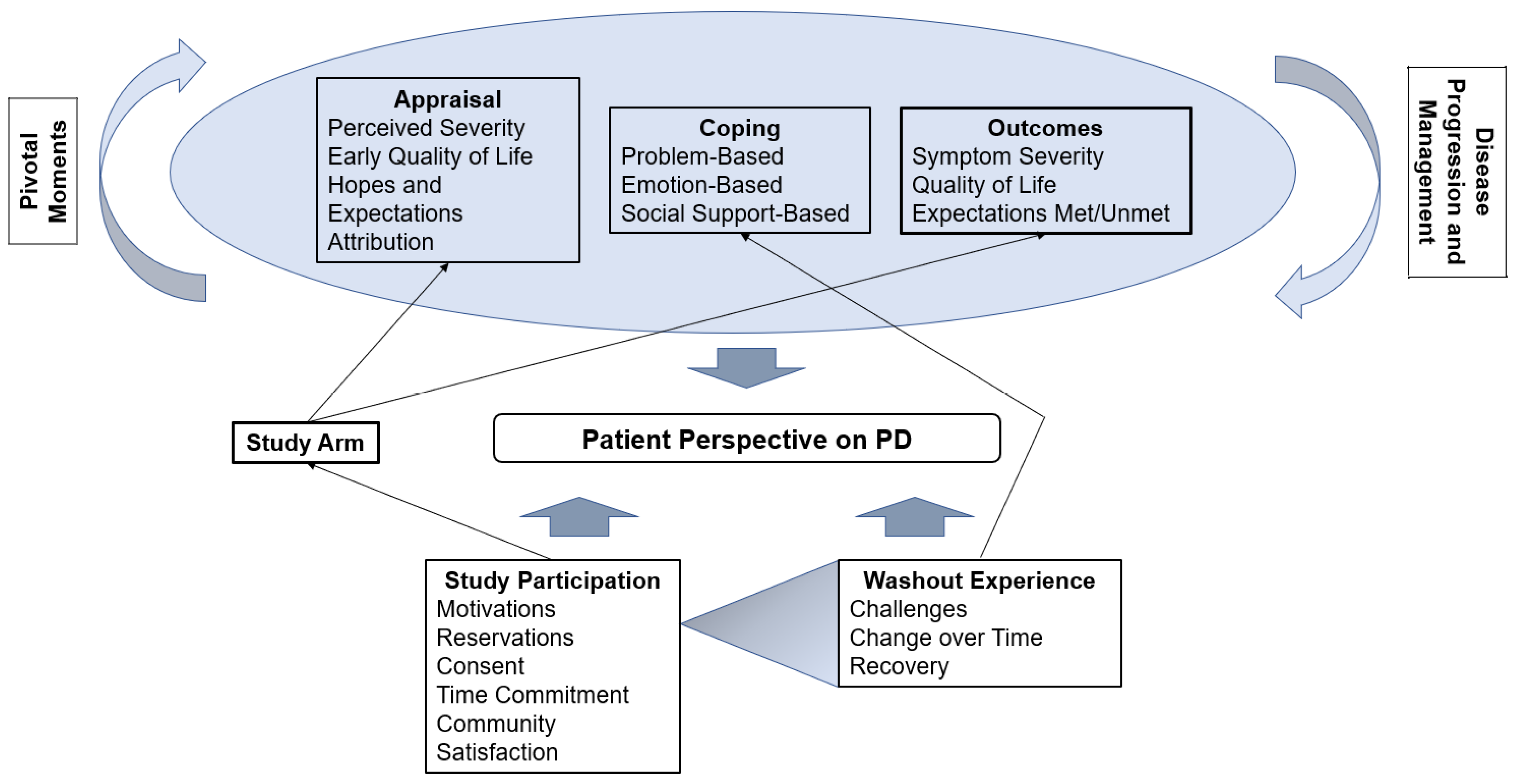
3.2. Framework Overview
3.3. Study Participations
3.3.1. Motivations
My hope was that [DBS] would slow or stop progress of the disease. At first, when I was diagnosed, [my] neurologist said, “Well, you probably ought to start thinking about getting your affairs in ordering and retiring,” which I didn’t like the idea of that. So, anything that would slow the progress of disease, I was all for. (Participant 9, eDBS)
Knowing what DBS was intended to do, it just concerned me that it was not made available to people who were diagnosed with Parkinson’s and otherwise healthy, and if it could be an extra tool to help combat the disease or make things easier, then why not make it available to people with early [stage PD]. I was quite hopeful during this selection process that I would get selected and [was] glad I did. (Participant 7, eDBS)
I regarded it as an altruistic move on my part, to take part in the study. I did not see... how I was going to benefit from it at all… But it would provide useful information for the curing of Parkinson’s. (Participant 1, eDBS)
3.3.2. Reservations
He was functioning just fine, at that time. He continued to drive, he continued to do his activities of daily living independently... one of the doctors said that they had expected that they wouldn’t have enough volunteers because who would want to have brain surgery when they weren’t having any problems? Because that can be a scary process, regardless of your diagnosis. (Participant 1, eDBS, Caregiver)
The thought of having brain surgery while still conscious was not very appealing to me. (Participant 1, eDBS)
I didn’t hesitate to get the operation. … I was not afraid of it... I think some people would be bothered by the idea of brain surgery, but it didn’t bother me. (Participant 9, eDBS)
Well, with my wife, there were concerns in the family as to whether or not I was doing the right thing. Again, back then, not a lot known about Parkinson’s. (Participant 7, eDBS)
3.3.3. Informed Consent
It’s not something that once you sign a piece of paper, they say, “Well, come on. We’ll do it.” With the study, it’s a very thoughtful process. (Participant 7, eDBS)
Of course, once I understood the program, I was very anxious to get the device, be proactive about it... I remember saying [to the medical ethicist], “I understand that there’s a 5% chance of a brain bleed during the operation, but I also understand there’s a 30% chance of early-stage dementia with Parkinson’s. What would you do? It’s an easy decision for me.” (Participant 9, eDBS)
3.3.4. Time Commitment
If I told them to consider it, I hope they would be in it for the long haul, because trust me, five years is a long time going every six months. If they’re going to go, I would hope that they would stick it out and finish it, because that’s the only way that, I guess, we got this far. I mean, we’ve stuck it out not only spiritually, but mentally... we didn’t miss a time. And yes, it was stressful, because we knew six months from that time, we would be going back into the hospital. (Participant 10, eODTsDBS, Caregiver)
I would not feel what I considered back to where I had been prior to the stay for maybe a week. And that’s really what caused me to step back from my position at work at that time. Because I was out eight days and it’d take me about a week to get straightened out. So every six months, I was two weeks out. And when you’re on production quotas and recruiting quotas and you get so far behind, then it’s just a stressful situation trying to keep up. (Participant 3, eODTsDBS)
3.3.5. Community
It was really, to be honest, the first time or the second time I was there, I found it very comforting to have other guys around with similar problems. (Participant 10, eODTsDBS)
My wife and my family were very sympathetic, but they couldn’t really understand what I was going through. These guys could. So going in and staying for eight days at a time off medication was a challenge. But it was interesting to have other folks there to do that with… Yeah, that’s been a lifelong impact. … I expect to be connected to those guys. As long as you struggle with this thing. (Participant 3, eODTsDBS)
The best thing that happened to me recently was meeting [study neurologist] and getting into the program. That gives me people to associate with who are positive and enthusiastic and it gives me some directions. It’s a shame that everyone who has Parkinson’s can’t be connected with the people that have the best advice like I have. (Participant 6, eDBS)
3.3.6. Satisfaction
He was taken very good care of and he always feels very safe and that eventually, somehow, this is going to help. (Participant 4, eODT, Caregiver)It’s just been neat to have opportunities to feel like you have a framework in which to fight back against this disease. (Participant 3, eODTsDBS)
I would say if that’s the only way you can get the device during the early stages, I’d say do it for sure… I would recommend that people get deep brain stimulation early, by hook or by crook. I realize that … I got [the] operation at least, for free, so I certainly appreciate that. That was worth the investment of my time. (Participant 9, eDBS)
There were some very disappointed patients... some were very upset that their number was not chosen as one of the surgery patients. (Participant 1, eDBS, Caregiver)
I did not receive it [DBS], originally. … It would have been nice if I’d had it sooner, but in reflection, I guess it’s kind of worked out just about right. They advanced… the electrodes going into the skull... I got one of the later models. (Participant 10, eODTsDBS)
3.4. Washout Experience
3.4.1. Washouts: Early-Stage PD, Years 0–2
3.4.2. Washouts: Mid/Late-Stage PD, Year 11
3.5. Appraisal, Coping, and Outcomes
3.5.1. Appraisal
Early DBS
I hoped that [DBS] would … slow down my Parkinson’s, and make me be able to maneuver around without the albatross of having wires hanging over my head. (Participant 6, eDBS)
[I hoped] that I would not become more dependent on others, that I would still be capable of dealing so much. (Participant 7, eDBS)
I did not know... how I dreamt of it. I just assumed it [DBS] would do no harm. (Participant 1, eDBS)
3.5.2. Coping
Early DBS
The problem I have with [medications] is remembering to take them and trying to remember if I did take a dose and remembering to take the next dose. Fortunately, with the DBS, once it’s on, it’s on. (Participant 7, eDBS)
Our goal when we went to [doctor], was to get him to enable [patient] to speak more clearly. That was my goal that I stated. That if he could just speak more clearly and they did indeed see that an adjustment could be made for that purpose. And he does speak more clearly now. (Participant 1, eDBS, Caregiver).
At one point, the settings might have been a little bit too high. So it just seemed to intensify my movements. Dyskinesia… I believe at one point, they decided to move from one set of leads down to another in their fine-tuning. I think that helped a lot. Again, it’s a learning process for the patient and the doctors. (Participant 7, eDBS).
3.5.3. Outcomes
Symptom Severity and Quality of Life
Early DBS
Well, it seemed to help a lot with my tremors in the hand and the tenseness, stiffness in my hands and feet and shoulders. That was one thing that just went away. That was no longer a huge event. So that was the biggest thing. (Participant 7, eDBS)
He didn’t feel different than when he didn’t have it, other than his tremor was ended. (Participant 1, eDBS, Caregiver)
Well, I remember going to [the study neurologist] … after surgery and feeling that I was disappointed that I could see no improvements in 30 days... I’m only saying that because the light bulb just went on. I totally understand now. I get it, what’s going on. I went in one day and said, “I understand how my brain is working to support the DBS.”... I expected it to be like turning it on and everything will be super. Instead, DBS, it didn’t work. It was a step forward success. It wasn’t a great success. It was another tool that we used to move forward. (Participant 6, eDBS).
Instead, the impact of early DBS was discussed in terms of prevention of major quality of life changes due to PD:
Since I had the DBS, everything’s going kind of smoothly. I’m anticipating it getting worse, and quite frankly, I’m at a point it’s starting to slow me down and I’m feeling the effects of Parkinson’s. But up until recently, I was really unaware every day that I had Parkinson’s… It helped me in my attitude. It gave me a lot of confidence because I knew that I had an extra gun in my pocket. (Participant 6, eDBS)
So far, [PD has] not affected me very much. I still work full time as a lawyer. I still play golf, a lot. It’s not affected much about my everyday life. It’s a little more difficult to put on my pants, for example, because of balance problems, but in general, have not been affected very much. (Participant 9, eDBS)
It still prevents that tremor in the right hand. I don’t know that it’s helping me in any other way, because it’s hard to say. Because if it is, it’s been doing it for a long time and it’s not something that I notice any longer. (Participant 1, eDBS)
I have always felt it probably mitigated some symptoms that he might have if he did not have the DBS, but again that’s nebulous because we don’t know what those would be. We never turn [the DBS] off. (Participant 1, eDBS, Caregiver)
When I was off the device… I could tell that my coordination was substantially compromised. But with the medication and on the device, I didn’t have any particular trouble whatsoever, and most people would not know that I have Parkinson’s disease. (Participant 9, eDBS)
Expectations Met/Unmet
Early DBS
It was the best thing that I had ever done. A very positive thing for me. (Participant 6, eDBS)
Glad I started early on, would not want to have done it any other way. I know it’s not a cure-all, but I’m glad I got it. To have waited till I got really bad with no hope that there would be no turning back any progression. I would not have liked being put in that situation… I don’t see any negativity with having DBS in my sense at an early stage. (Participant 7, eDBS)
It was early in the diagnosis, but it was not early in my age, I was 74 years old and—I believe that was okay… I appreciate it today, the effect from that. (Participant 1, eDBS)
Medication that’s available now has not been shown, I believe in any way to slow or stop progression. That’s why the study was done for early [DBS] to see what impact it does possibly have on slowing or stopping progression. In my case, I would have to say it does. But that’s me. In my unique Parkinson’s situation, I believe it has slowed. (Participant 7, eDBS)
It’s been 16 years [since joining the study] and until recently, you literally couldn’t tell I had Parkinson’s... I told [study neurologist] the other day … “I probably wouldn’t be here today,” if I hadn’t had all this exchange with him and the team, I probably would have passed away, I think. (Participant 6, eDBS)
I’d tell them to not hesitate, to do [early DBS] for sure. (Participant 11, eDBS)
DBS I see not having any kind of a negative factor in any of those situations. I would encourage it greatly… I would encourage anyone that had a noticeable impact in their life due to Parkinson’s, a confirmed diagnosis regardless of whether or not medication was tolerable or they thought it was making a good impact… knowing that medication is time-based, it’s not constant, and Parkinson’s is a progressive disease. (Participant 7, eDBS)
3.6. PDQ-39 Quality of Life Assessment
4. Discussion
4.1. Washout Experience
4.2. Early DBS and Standard of Care DBS
4.3. Qualitative and Quantitative Analysis of Quality of Life
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Charles, P.D.; Padaliya, B.B.; Newman, W.J.; Gill, C.E.; Covington, C.D.; Fang, J.Y.; So, S.A.; Tramontana, M.G.; Konrad, P.E.; Davis, T.L. Deep brain stimulation of the subthalamic nucleus reduces antiparkinsonian medication costs. Parkinsonism Relat. Disord. 2004, 10, 475. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.; Gill, S.; Varma, T.; Jenkinson, C.; Quinn, N.; Mitchell, R.; Scott, R.; Ives, N.; Rick, C.; Daniels, J.; et al. Deep brain stimulation plus best medical therapy versus best medical therapy alone for advanced Parkinson’s disease (PD SURG trial): A randomised, open-label trial. Lancet Neurol. 2010, 9, 581. [Google Scholar] [CrossRef]
- Okun, M.; Gallo, B.V.; Mandybur, G.; Jagid, J.; Foote, K.; Revilla, F.J.; Alterman, R.; Jankovic, J.; Simpson, R.; Junn, F.; et al. Subthalamic deep brain stimulation with a constant-current device in Parkinson’s disease: An open-label randomised controlled trial. Lancet Neurol. 2012, 11, 140. [Google Scholar] [CrossRef]
- Follett, K.A.; Weaver, F.M.; Stern, M.; Hur, K.; Harris, C.L.; Luo, P.; Marks, W.J.; Rothlind, J.; Sagher, O.; Moy, C.; et al. Pallidal versus subthalamic deep-brain stimulation for Parkinson’s disease. N. Engl. J. Med. 2010, 362, 2077–2091. [Google Scholar] [CrossRef]
- Odekerken, V.J.; van Laar, T.; Staal, M.J.; Mosch, A.; Hoffmann, C.F.; Nijssen, P.C.; Beute, G.N.; van Vugt, J.P.; Lenders, M.W.; Contarino, M.F.; et al. Subthalamic nucleus versus globus pallidus bilateral deep brain stimulation for advanced Parkinson’s disease (NSTAPS study): A randomised controlled trial. Lancet Neurol. 2013, 12, 37–44. [Google Scholar] [CrossRef]
- Schuepbach, W.; Rau, J.; Knudsen, K.; Volkmann, J.; Krack, P.; Timmermann, L.; Hälbig, T.; Hesekamp, H.; Navarro, S.; Meier, N.; et al. Neurostimulation for Parkinson’s disease with early motor complications. N. Engl. J. Med. 2013, 368, 610–622. [Google Scholar] [CrossRef]
- Mathers, J.; Rick, C.; Jenkinson, C.; Garside, R.; Pall, H.; Mitchell, R.; Bayliss, S.; Jones, L.L. Patients’ experiences of deep brain stimulation for Parkinson’s disease: A qualitative systematic review and synthesis. BMJ Open 2016, 6, e011525. [Google Scholar] [CrossRef]
- Haahr, A.; Kirkevold, M.; Hall, E.O.C.; Østergaard, K. Living with advanced Parkinson’s disease: A constant struggle with unpredictability. J. Adv. Nurs. 2011, 67, 408–417. [Google Scholar] [CrossRef]
- Haahr, A.; Kirkevold, M.; Hall, E.O.C.C.; Østergaard, K. From miracle to reconciliation: A hermeneutic phenomenological study exploring the experience of living with Parkinson’s disease following Deep Brain Stimulation. Int. J. Nurs. Stud. 2010, 47, 1228–1236. [Google Scholar] [CrossRef]
- Spieles-Engemann, A.L.; Behbehani, M.M.; Collier, T.J.; Wohlgenant, S.L.; Steece-Collier, K.; Paumier, K.; Daley, B.F.; Gombash, S.; Madhavan, L.; Mandybur, G.T.; et al. Stimulation of the rat subthalamic nucleus is neuroprotective following significant nigral dopamine neuron loss. Neurobiol. Dis. 2010, 39, 105-15. [Google Scholar] [CrossRef]
- Wallace, B.A.; Ashkan, K.; E Heise, C.; Foote, K.D.; Torres, N.; Mitrofanis, J.; Benabid, A.-L. Survival of midbrain dopaminergic cells after lesion or deep brain stimulation of the subthalamic nucleus in MPTP-treated monkeys. Brain 2007, 130, 2129–2145. [Google Scholar] [CrossRef] [PubMed]
- Maesawa, S.; Kaneoke, Y.; Kajita, Y.; Usui, N.; Misawa, N.; Nakayama, A.; Yoshida, J. Long-term stimulation of the subthalamic nucleus in hemiparkinsonian rats: Neuroprotection of dopaminergic neurons. J. Neurosurg. 2004, 100, 679. [Google Scholar] [CrossRef] [PubMed]
- Temel, Y.; Visser-Vandewalle, V.; Kaplan, S.; Kozan, R.; Daemen, M.A.; Blokland, A.; Schmitz, C.; Steinbusch, H.W. Protection of nigral cell death by bilateral subthalamic nucleus stimulation. Brain Res. 2006, 1120, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Charles, D.; Konrad, P.E.; Neimat, J.S.; Molinari, A.L.; Tramontana, M.G.; Finder, S.G.; Gill, C.; Bliton, M.J.; Kao, C.; Phibbs, F.T.; et al. Subthalamic nucleus deep brain stimulation in early stage Parkinson’s disease. Park. Relat. Disord. 2014, 20, 731–737. [Google Scholar] [CrossRef]
- Hacker, M.L.; Turchan, M.; Heusinkveld, L.E.; Currie, A.D.; Millan, S.H.; Molinari, A.L.; Konrad, P.E.; Davis, T.L.; Phibbs, F.T.; Hedera, P.; et al. Deep brain stimulation in early-stage Parkinson disease: Five-year outcomes. Neurology 2020, 95, E393–E401. [Google Scholar] [CrossRef]
- Charles, P.; Dolhun, R.; Gill, C.; Davis, T.; Bliton, M.; Tramontana, M.; Salomon, R.; Wang, L.; Hedera, P.; Phibbs, F.; et al. Deep brain stimulation in early Parkinson’s disease: Enrollment experience from a pilot trial. Park. Relat. Disord. 2012, 18, 268–273. [Google Scholar] [CrossRef]
- Finder, S.G.; Bliton, M.J.; Gill, C.E.; Davis, T.L.; Konrad, P.E.; Charles, P.D. Potential subjects’ responses to an ethics questionnaire in a phase I study of deep brain stimulation in early Parkinson’s disease. J. Clin. Ethics 2012, 23, 207. [Google Scholar] [PubMed]
- Azungah, T. Qualitative research: Deductive and inductive approaches to data analysis. Qual Res. J. 2018, 18, 383–400. [Google Scholar] [CrossRef]
- Fereday, J.; Muir-Cochrane, E. Demonstrating Rigor Using Thematic Analysis: A Hybrid Approach of Inductive and Deductive Coding and Theme Development. Int. J. Qual. Methods 2006, 5, 80–92. [Google Scholar] [CrossRef]
- Borell-Carrió, F.; Suchman, A.L.; Epstein, R.M. The biopsychosocial model 25 years later: Principles, practice, and scientific inquiry. Ann. Fam. Med. 2004, 2, 576–582. [Google Scholar] [CrossRef]
- Engel, G.L. The Clinical Application of the Biopsychosocial Model. Am. J. Psychiatry 1980, 137, 535–544. [Google Scholar] [PubMed]
- Bandura, A. Social Cognitive Theory of Self-Regulation. Organ. Behav. Hum. Decis. Process. 1991, 50, 248–287. [Google Scholar] [CrossRef]
- Mischel, W. Toward a Cognitive Social Learning Reconceptualization of Personality. Psychol. Rev. 1973, 80, 252–283. [Google Scholar] [CrossRef] [PubMed]
- Carver, C.S.; Scheier, M.F.; Weintraub, J.K. Assessing Coping Strategies: A Theoretically Based Approach. J. Pers. Soc. Psychol. 1989, 56, 267–283. [Google Scholar] [CrossRef]
- Krägeloh, C.U.; Chai, P.P.M.; Shepherd, D.; Billington, R. How Religious Coping is Used Relative to Other Coping Strategies Depends on the Individual’s Level of Religiosity and Spirituality. J Relig Health 2012, 51, 1137–1151. [Google Scholar] [CrossRef]
- Penley, J.A.; Tomaka, J.; Wiebe, J.S. The Association of Coping To Physical and Psychological Health Outcomes: A Meta-Analytic Review. J. Behav. Med. 2002, 25, 551–603. [Google Scholar] [CrossRef]
- Cabrera, L.Y.; Kelly-Blake, K.; Sidiropoulos, C. Perspectives on deep brain stimulation and its earlier use for Parkinson’s disease: A qualitative study of us patients. Brain Sci. 2020, 10, 34. [Google Scholar] [CrossRef]
- Kim, M.-R.; Yun, J.Y.; Jeon, B.; Lim, Y.H.; Kim, K.R.; Yang, H.-J.; Paek, S.H. Patients‘ reluctance to undergo deep brain stimulation for Parkinson’s disease. Parkinsonism Relat. Disord. 2016, 23. [Google Scholar] [CrossRef]
- Hamberg, K.; Hariz, G.-M. The decision-making process leading to deep brain stimulation in men and women with parkinson’s disease—An interview study. BMC Neurol. 2014, 14, 89. [Google Scholar] [CrossRef]
- Heusinkveld, L.; Hacker, M.; Turchan, M.; Bollig, M.; Tamargo, C.; Fisher, W.; McLaughlin, L.; Martig, A.; Charles, D. Patient Perspectives on Deep Brain Stimulation Clinical Research in Early Stage Parkinson’s Disease. J. Parkinsons Dis. 2017, 7, 89–94. [Google Scholar] [CrossRef]
- Cannard, K.G.; Hacker, M.L.; Molinari, A.; Heusinkveld, L.E.; Currie, A.D.; Charles, D. Recruitment and retention in clinical trials of deep brain stimulation in early-stage Parkinson’s disease: Past experiences and future considerations. J. Parkinsons Dis. 2018, 8, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Hacker, M.L.; Delong, M.R.; Turchan, M.; Heusinkveld, L.E.; Ostrem, J.L.; Molinari, A.L.; Currie, A.D.; Konrad, P.E.; Davis, T.L.; Phibbs, F.T.; et al. Effects of deep brain stimulation on rest tremor progression in early stage Parkinson disease. Neurology 2018, 91, e463–e471. [Google Scholar] [CrossRef] [PubMed]
- Hariz, G.-M.; Limousin, P.; Hamberg, K. DBS means everything—For some time. Patients’ Perspectives on Daily Life with Deep Brain Stimulation for Parkinson’s Disease. J. Parkinsons Dis. 2016, 6, 335–347. [Google Scholar] [CrossRef] [PubMed]
- Ibrahimoğlu, Ö.; Mersin, S.; Akyol, E. The Experiences of Patients with Deep Brain Stimulation in Parkinson’s Disease: Challenges, Expectations, and Accomplishments. Acta Med. Acad. 2020, 49, 36–43. [Google Scholar] [CrossRef]
- Lin, H.Y.; Hasegawa, H.; Mundil, N.; Samuel, M.; Ashkan, K. Patients’ Expectations and Satisfaction in Subthalamic Nucleus Deep Brain Stimulation for Parkinson Disease: 6-Year Follow-up. World Neurosurg. 2019, 121, e654–e660. [Google Scholar] [CrossRef]
- Hitti, F.; Ramayya, A.G.; McShane, B.J.; Yang, A.I.; Vaughan, K.A.; Baltuch, G.H. Long-term outcomes following deep brain stimulation for Parkinson’s disease. J. Neurosurg. 2019, 137, 1–6. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| At Enrollment | At 11-Year Interview | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Patient | Treatment Group * | Medication Duration (Years) | Age (Years) | PDQ-39 Summary Index | DBS Duration (Years) | Medication Duration (Years) | Age (Years) | PDQ-39 Summary Index | 11-Year Washout Duration (Days) |
| 1 | eDBS | 1.0 | 73.9 | 7.5 | 10.4 | 12.1 | 85.0 | d.n.p. | d.n.p. |
| 2 | eODTsDBS | 0.9 | 63.2 | 19.5 | 5.2 | 14.3 | 76.6 | 15.2 | 4 |
| 3 | eODTsDBS | 3.9 | 55.5 | 14.6 | 0.5 | 16.8 | 68.3 | 14.3 | 5 |
| 4 | eODT | 3.0 | 59.7 | 9.6 | n.a. | 15.6 | 72.3 | 15.6 | 7 |
| 5 | eODT | 1.3 | 67.9 | 24.9 | n.a. | 12.2 | 78.8 | 36.8 | w.n.a. |
| 6 | eDBS | 1.7 | 56.4 | 19.7 | 13.0 | 15.0 | 69.7 | 18.1 | w.n.a. |
| 7 | eDBS | 0.6 | 55.4 | 14.3 | 10.9 | 11.7 | 66.5 | 51.8 | 7 |
| 8 | eODT | 1.4 | 52.3 | 14.5 | n.a. | 14.1 | 64.9 | 30.0 | 7 |
| 9 | eDBS | 1.4 | 53.6 | 6.8 | 13.3 | 15.2 | 67.4 | 15.8 | 2.5 |
| 10 | eODTsDBS | 3.5 | 60.8 | 20.3 | 7.6 | 17.1 | 74.4 | 35.2 | 4 |
| Mean ± SD (Range) | 1.9 ± 1.2 (0.6–3.9) | 59.9 ± 6.8 (52.3–73.9) | 15.2 ± 6.0 (6.8–24.9) | 8.7 ± 4.6 (0.5–13.3) | 14.4 ± 1.9 (11.7–17.1) | 72.4 ± 6.3 (64.9–85.0) | 25.9 ± 13.3 (14.3–51.8) | 5.2 ± 1.7 (0–7) | |
| Theme | Representative Quotation |
|---|---|
| Washouts: Early-Stage PD Years 0–2 | |
| Gradual symptom worsening |
|
| Emotional difficultly | Depression was the biggest thing for me. Huge depression. (Participant 6, eDBS) |
| No significant effect/alleviation of symptoms |
|
| Coping Strategies |
|
| Treatment readjustment after washout |
|
| Washouts: Mid/Late-Stage PD Year 11 | |
| Exacerbation of physical symptoms |
|
| Emotional difficulties |
|
| Difficulty completing study assessments |
|
| Importance of CRC staff support |
|
| Newfound recognition of difficulties without PD treatment |
|
| Theme Subtheme | Thematic Description | Representative Quotation |
|---|---|---|
| APPRAISAL—All Patients | ||
| Perceived Severity | Reaction to diagnosis |
|
| Perceived severity changed with progression |
| |
| Hopes and Expectations | Expectation of progression |
|
| Desire not to be pitied |
| |
| Early QoL | PD caused embarrassment at work |
|
| Attribution | Patients unsure which symptoms to attribute to PD versus normal aging |
|
| COPING—All Patients | ||
| Problem-Based | Medication management |
|
| DBS management |
| |
| Information seeking |
| |
| Symptom-specific coping strategies |
| |
| Emotion-Based | Acceptance |
|
| Faith |
| |
| Social comparison |
| |
| Perseverance/determination |
| |
| Positivity |
| |
| Social Support-Based | Caregiver impact |
|
| PD support groups |
| |
| OUTCOMES—Standard of Care DBS Patients | ||
| Symptom Severity | Noticed clear symptomatic benefit after receiving DBS |
|
| Accepted that DBS is not a cure-all |
| |
| Quality of Life | Drastically improved quality of life in the short-term |
|
| Expectations met/unmet | Satisfied with DBS treatment despite continued symptoms |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stoehr, K.; Pazira, K.; Bonnet, K.; Schlundt, D.; Charles, D.; Hacker, M. Deep Brain Stimulation in Early-Stage Parkinson’s Disease: Patient Experience after 11 Years. Brain Sci. 2022, 12, 766. https://doi.org/10.3390/brainsci12060766
Stoehr K, Pazira K, Bonnet K, Schlundt D, Charles D, Hacker M. Deep Brain Stimulation in Early-Stage Parkinson’s Disease: Patient Experience after 11 Years. Brain Sciences. 2022; 12(6):766. https://doi.org/10.3390/brainsci12060766
Chicago/Turabian StyleStoehr, Kaitlyn, Kian Pazira, Kemberlee Bonnet, David Schlundt, David Charles, and Mallory Hacker. 2022. "Deep Brain Stimulation in Early-Stage Parkinson’s Disease: Patient Experience after 11 Years" Brain Sciences 12, no. 6: 766. https://doi.org/10.3390/brainsci12060766
APA StyleStoehr, K., Pazira, K., Bonnet, K., Schlundt, D., Charles, D., & Hacker, M. (2022). Deep Brain Stimulation in Early-Stage Parkinson’s Disease: Patient Experience after 11 Years. Brain Sciences, 12(6), 766. https://doi.org/10.3390/brainsci12060766