
Effect of Ipsilateral, Contralateral or Bilateral Repetitive Transcranial Magnetic Stimulation in Patients with Lateralized Tinnitus: A Placebo-Controlled Randomized Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Outcome Measures
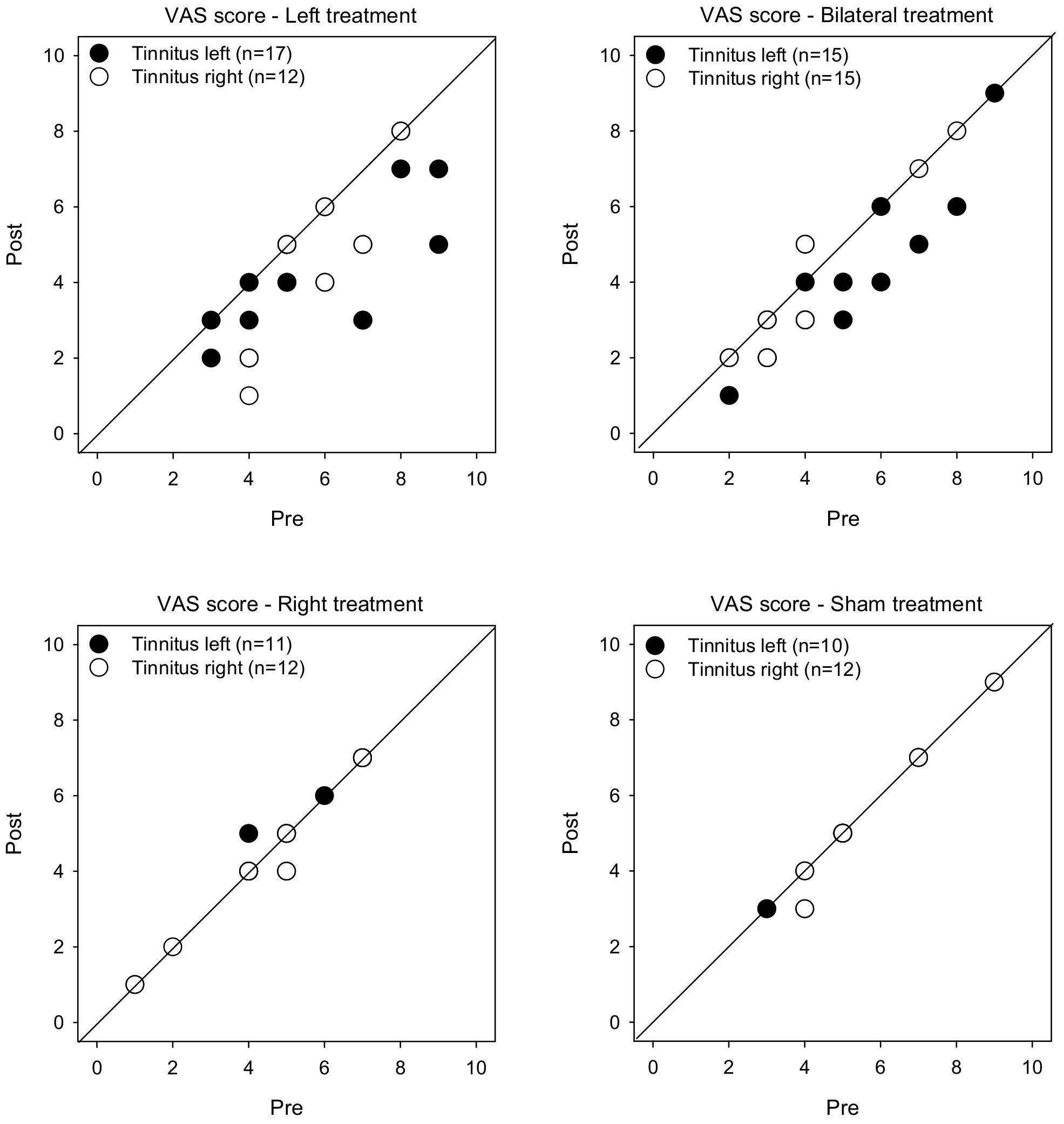
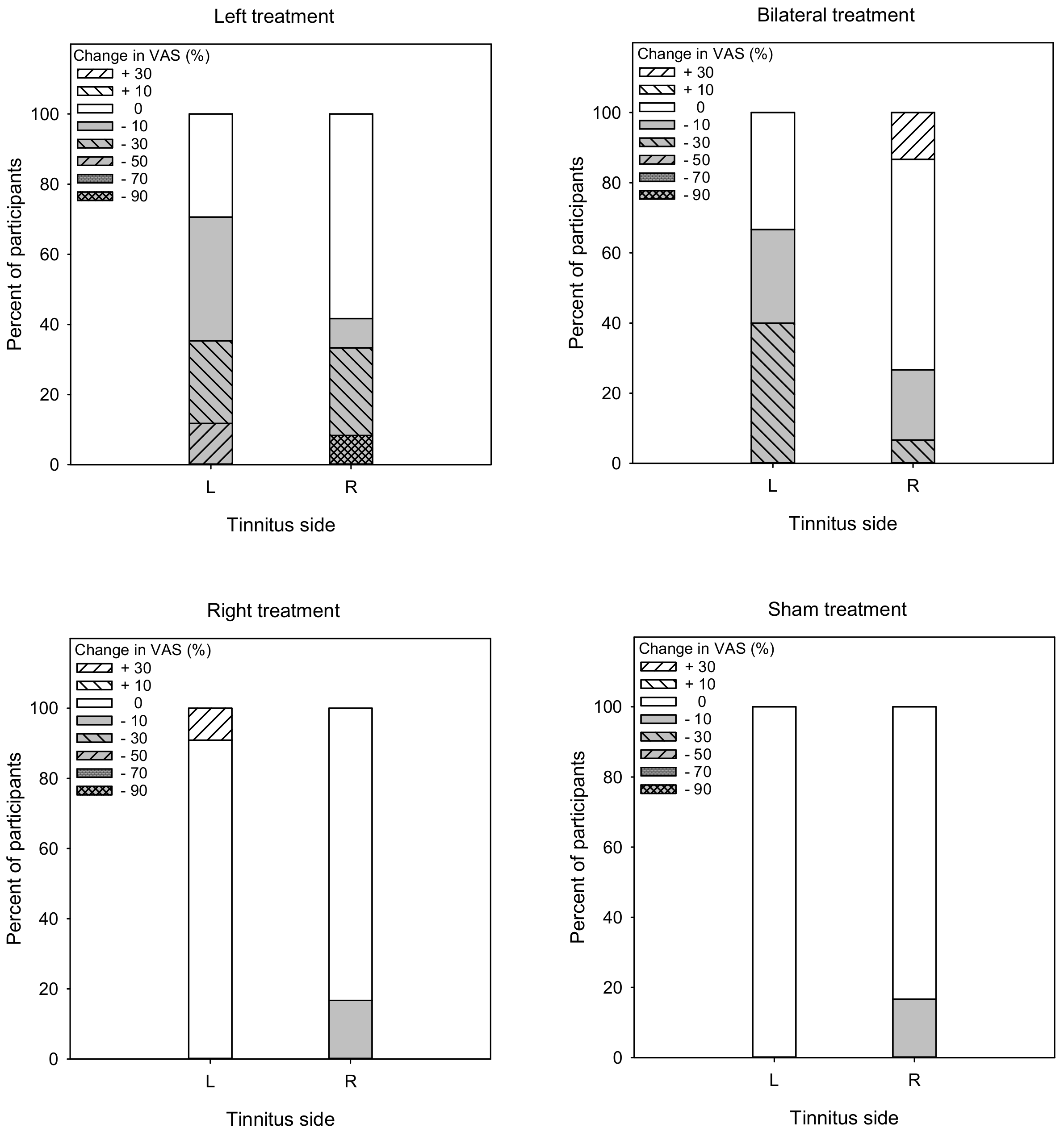
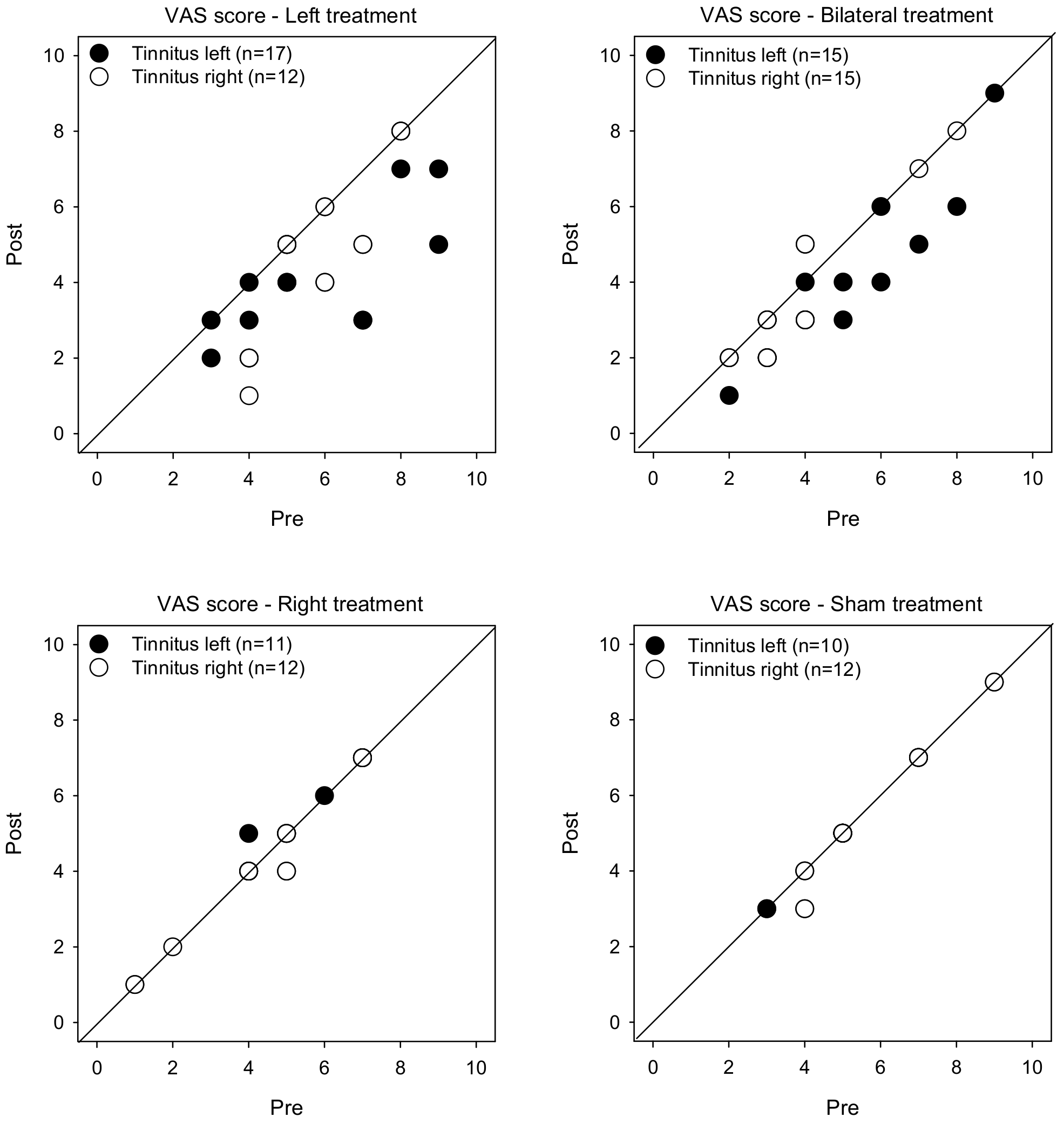
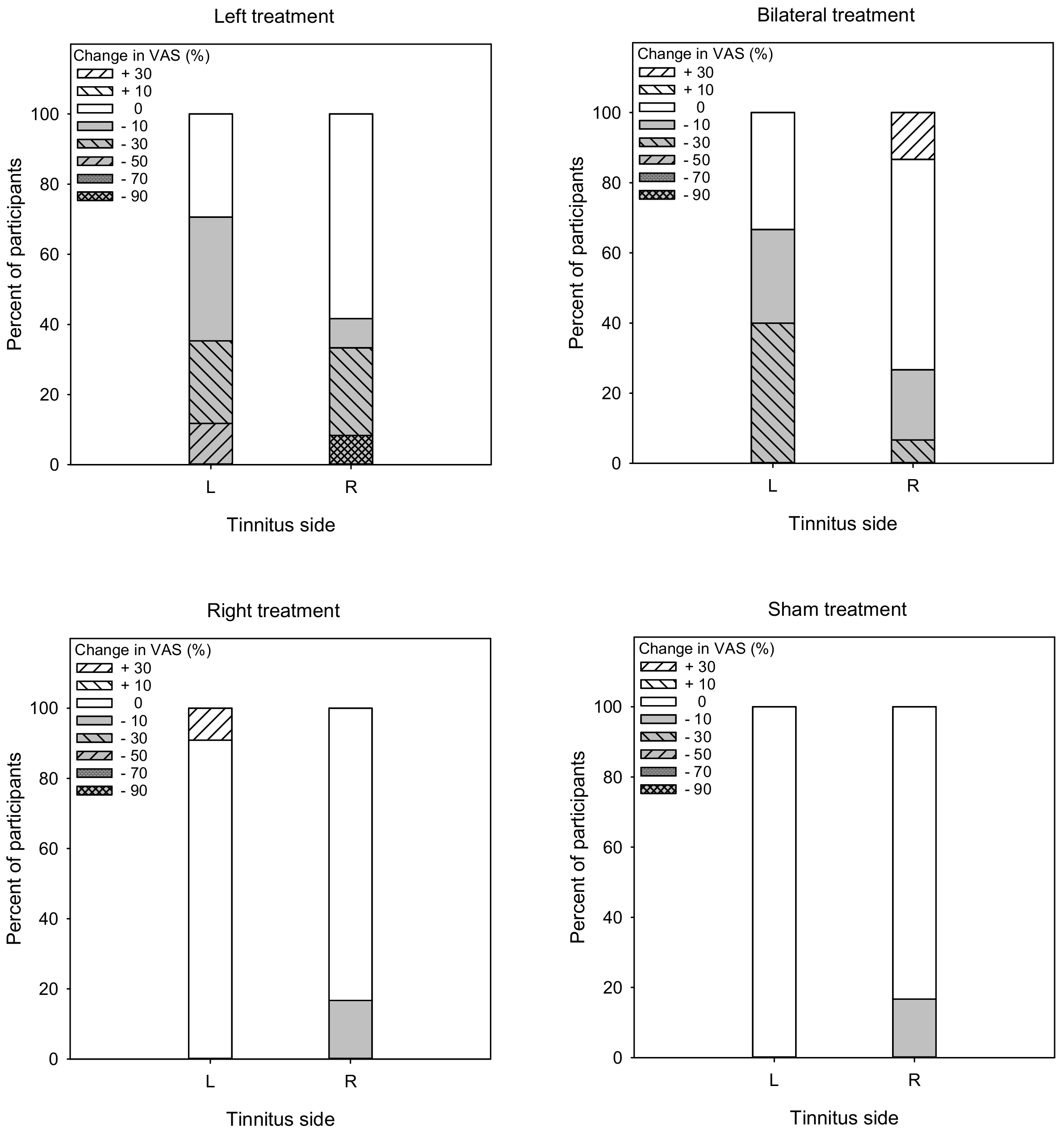
- VAS score of tinnitus severity [23]. Patients were asked to mark their tinnitus severity on a 10-cm line, where 0 = no tinnitus and 10 = worst tinnitus imaginable. Cartoon expressions (e.g., smile, neutral, pain, extreme pain, etc.) were distributed above the line to illustrate the range of tinnitus severity. VAS scores were compared pre- and post-treatment. A response to treatment was considered when VAS scores were reduced by 10% or more [24].
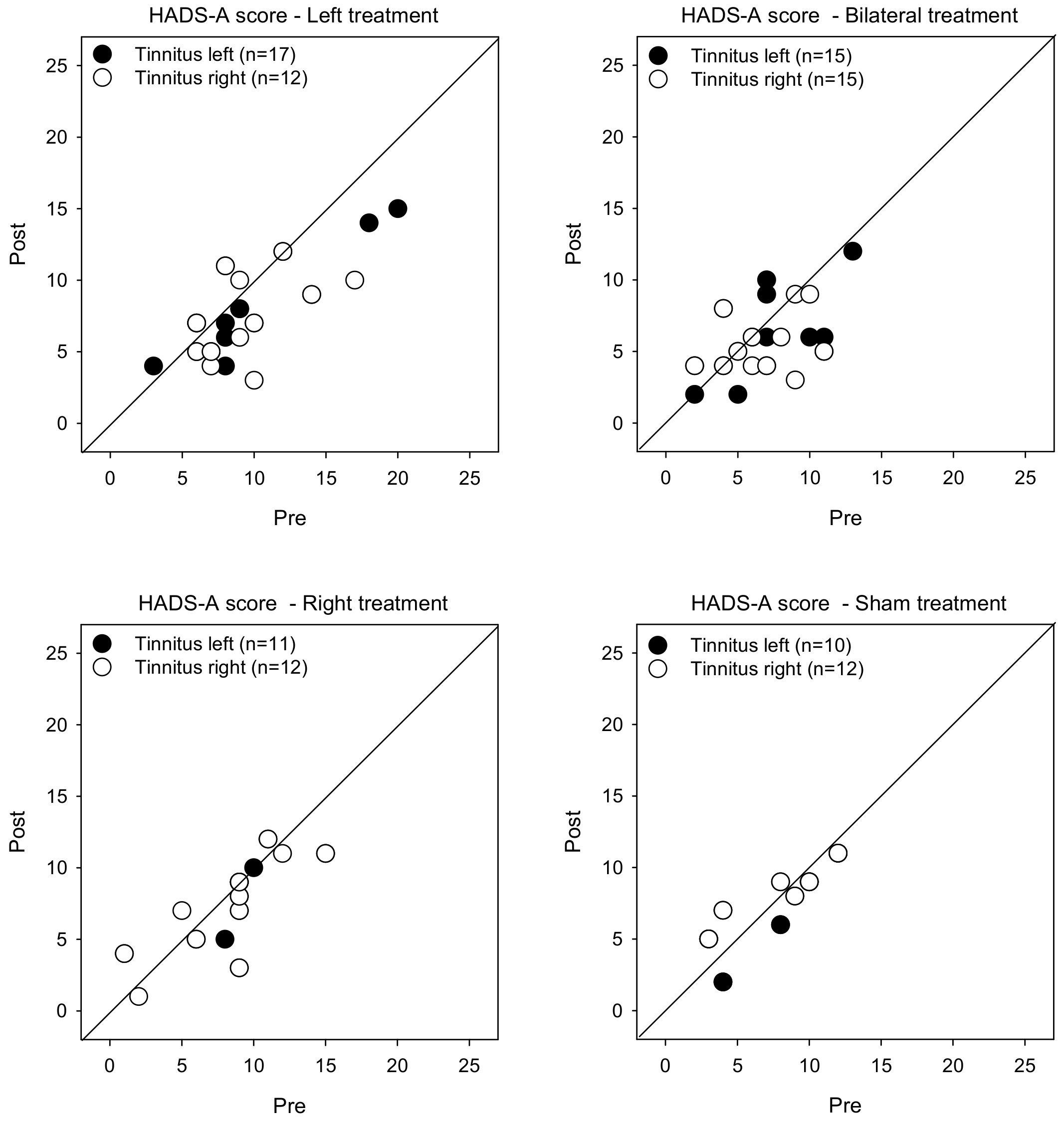
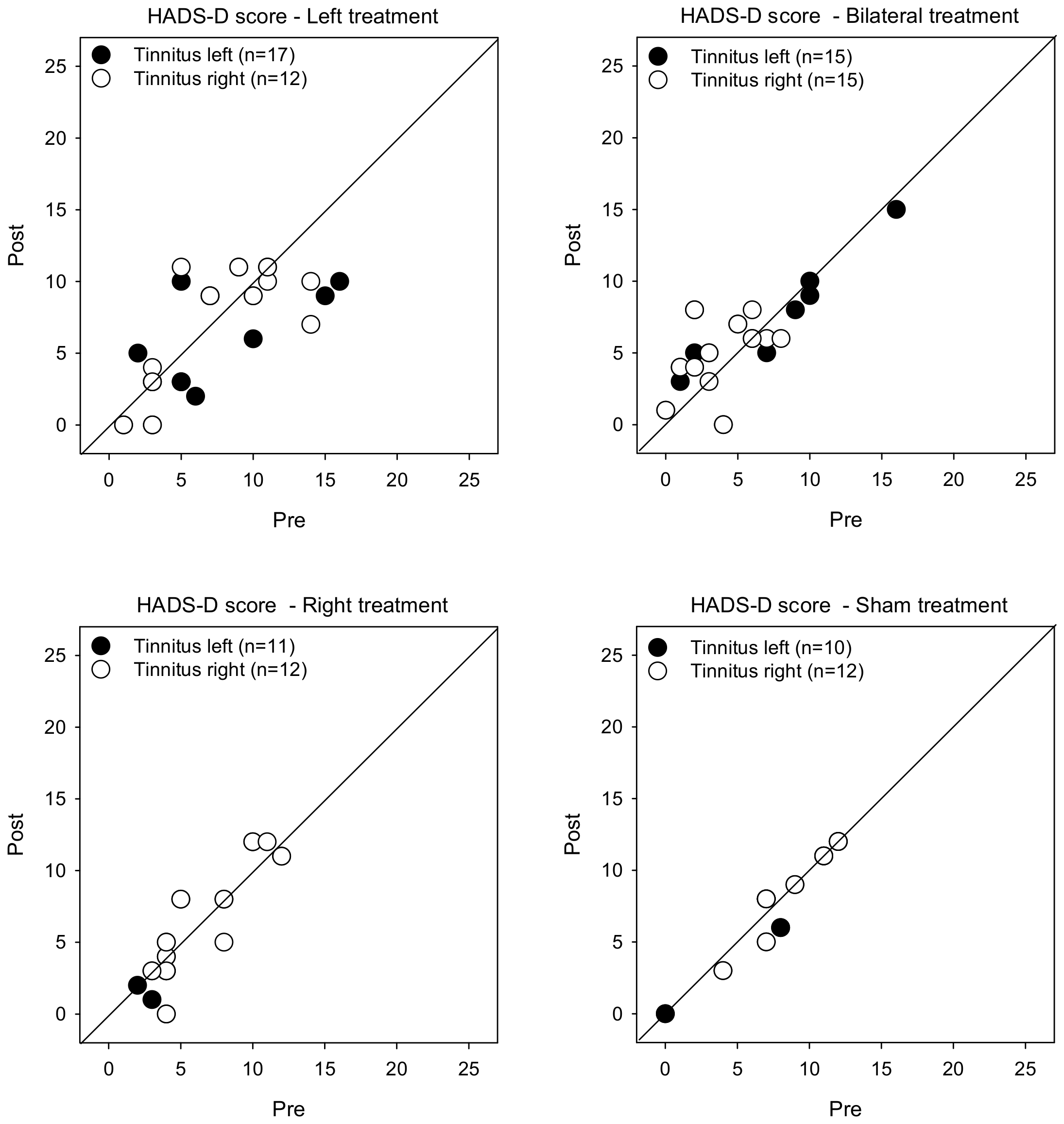
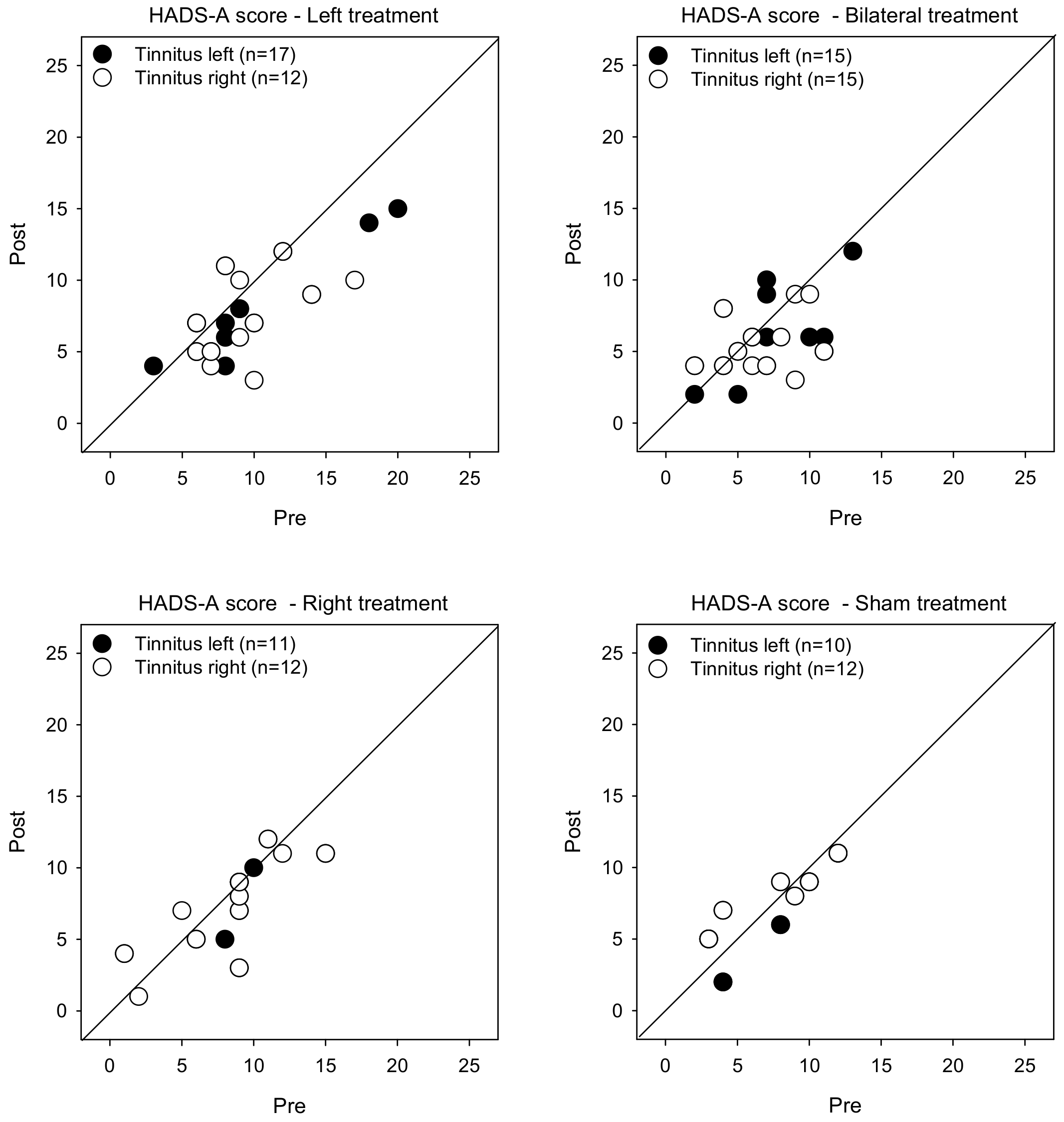
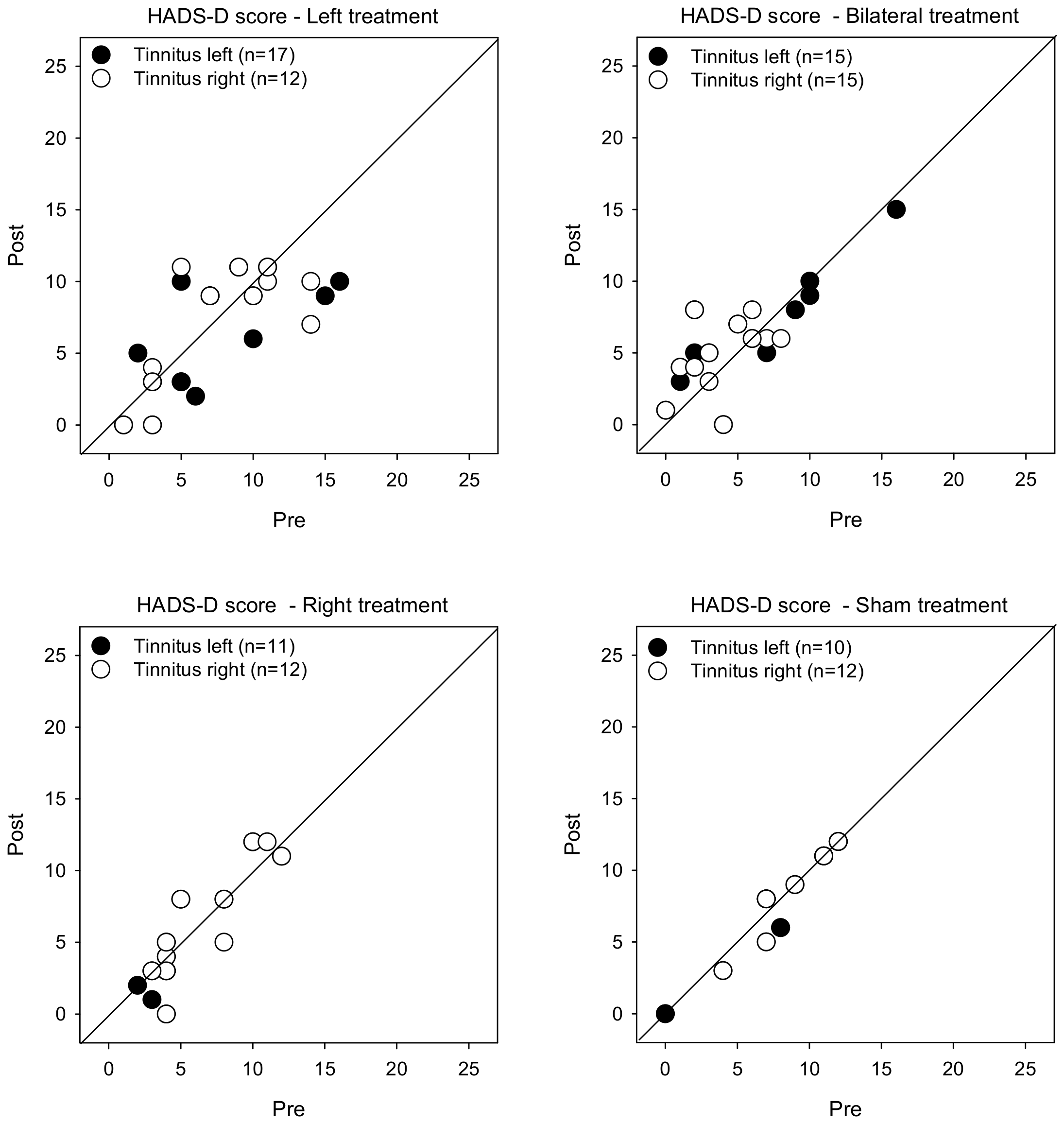
- Hospital Anxiety and Depression Scale (HADS) [29]. Patient mood was characterized using the HADS questionnaire, which includes two subscales consisting of 7 questions each to assess anxiety (HADS-A) and depression (HADS-D). Eight or more points was considered to be clinically significant anxiety or depression.
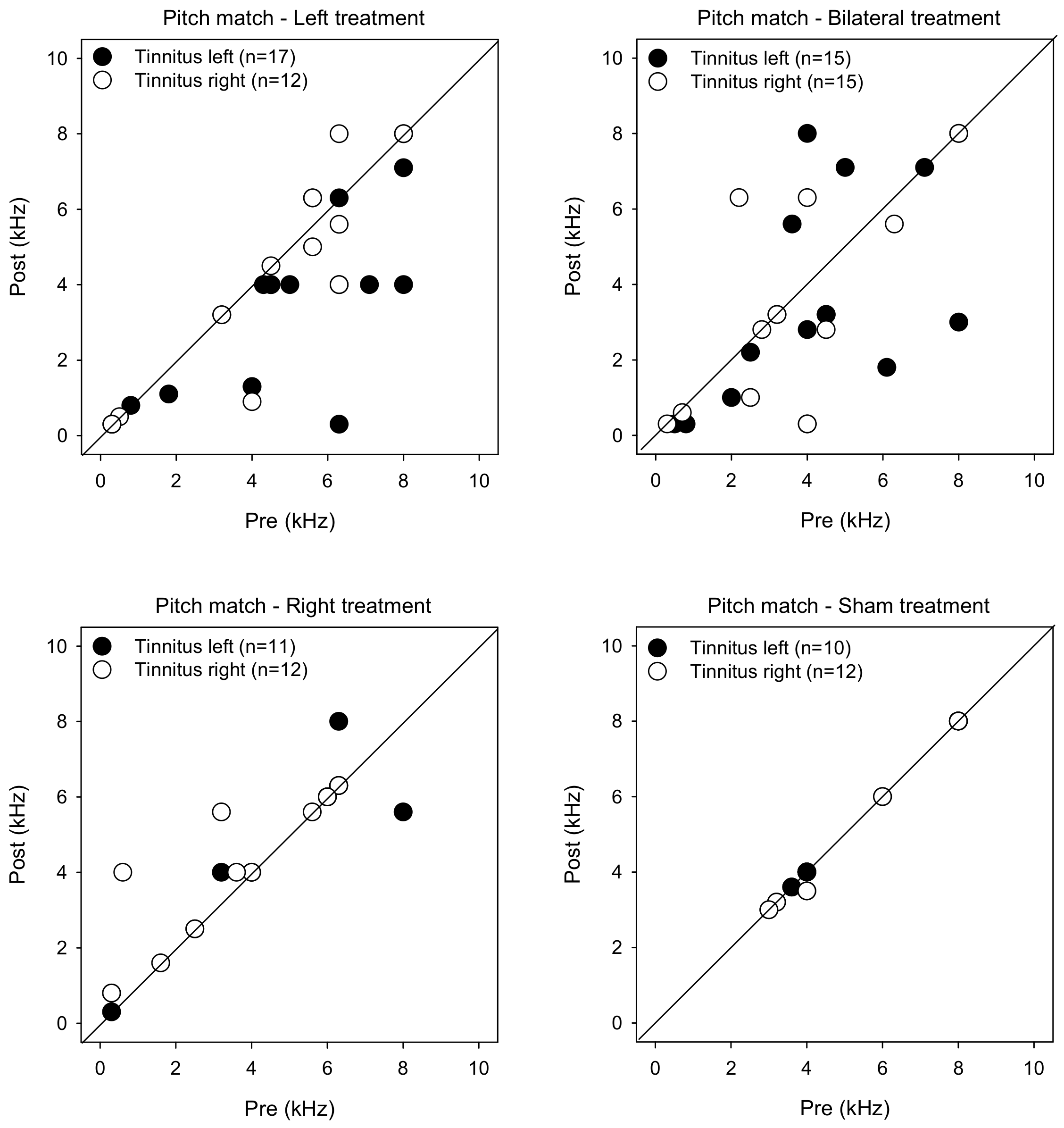
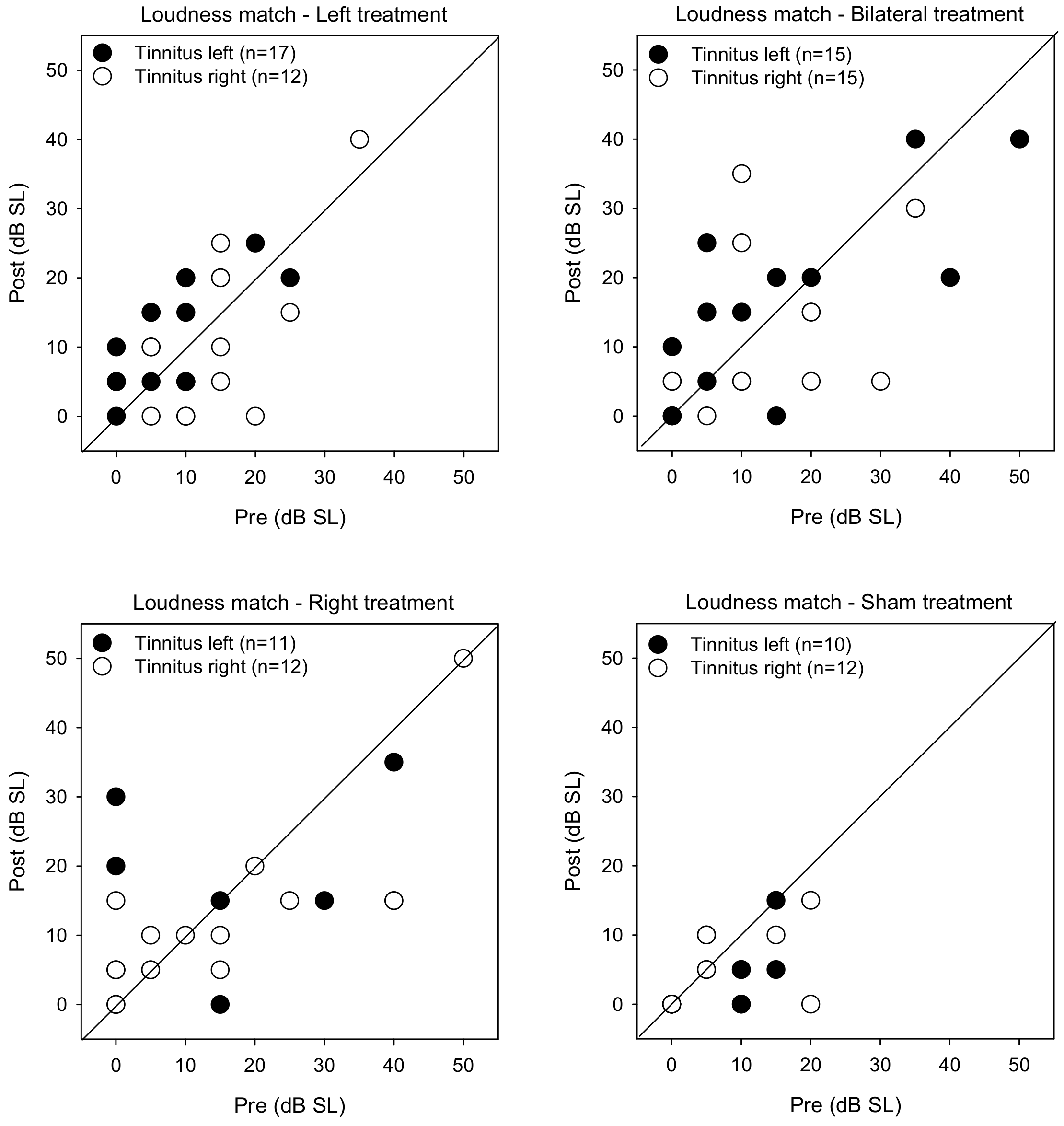
- Pitch matching was performed using pure-tone stimuli delivered over headphones; stimuli were presented at 10 dB sensation level (SL) relative to hearing threshold. During testing, two sounds with different frequencies (e.g., 1 kHz and 8 kHz) were presented to the ear contralateral to the tinnitus, and the patient indicated which sound was closer to the pitch of the tinnitus. The frequencies were adjusted according to patient response, continuously narrowing the range until the frequency that best matched the pitch of the tinnitus was found.
- After identifying the frequency that best matched the pitch of the tinnitus, the loudness of the tinnitus was estimated. The stimulus level in the contralateral ear was adjusted to match the level of the tinnitus (5 dB initial step size, 1 dB final step size). This measurement of tinnitus was performed twice, with a short break between test runs. The final adjusted level was averaged across both runs and was expressed in terms of dB sensation level (SL), relative to the hearing threshold of the pitch-matched frequency.
2.3. rTMS
2.4. Statical Analyses
3. Results
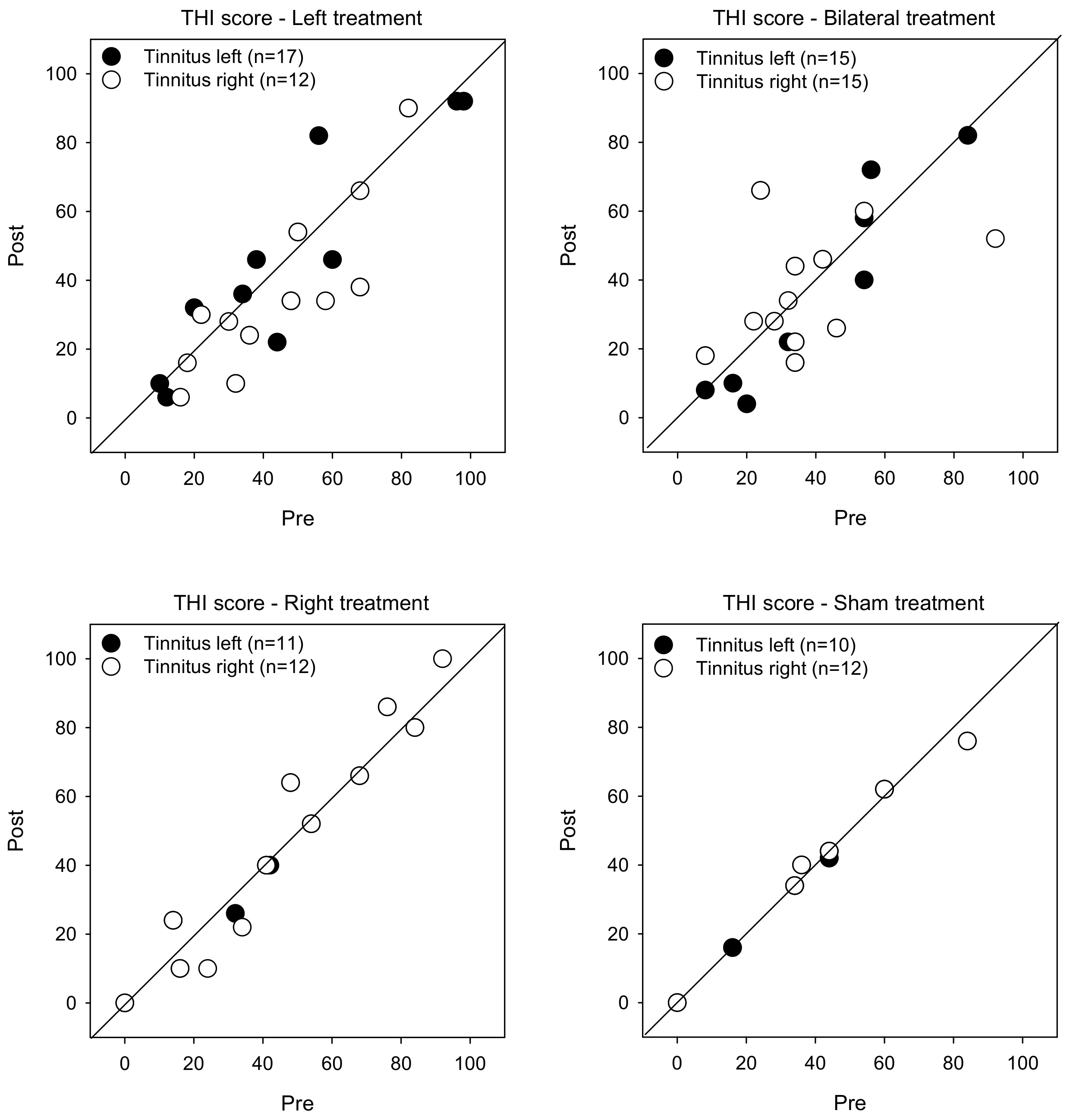
3.1. Tinnitus Severity
3.2. HADS Scores
3.3. Psychoacoustic Measures
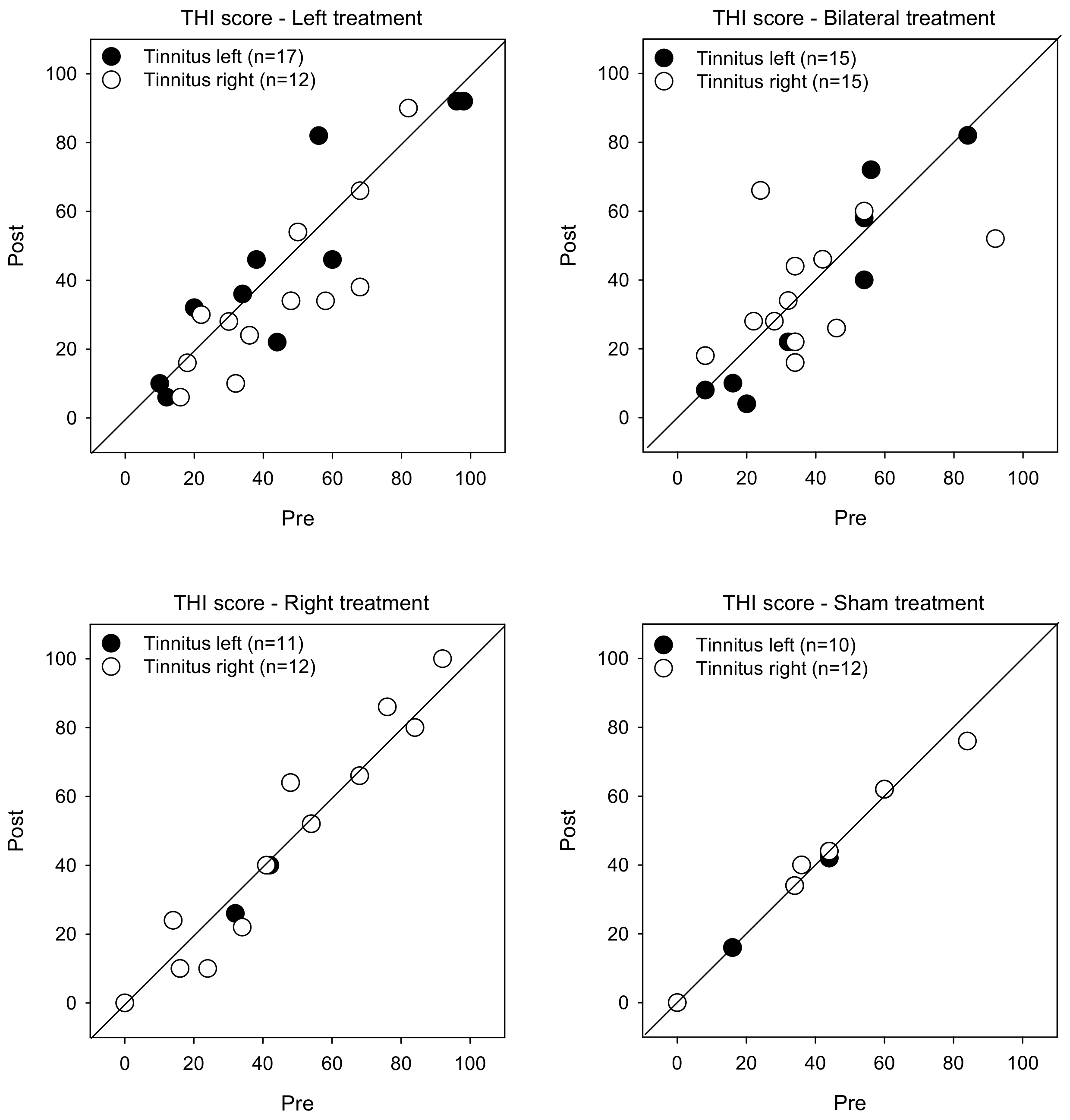
3.4. Pre- versus Post-Treatment
3.5. Treatment Response
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Langguth, B.; Landgrebe, M.; Kleinjung, T.; Sand, G.P.; Hajak, G. Tinnitus and depression. World J. Biol. Psychiatry 2011, 12, 489–500. [Google Scholar] [CrossRef] [PubMed]
- Langguth, B.; Kreuzer, P.M.; Kleinjung, T.; De Ridder, D. Tinnitus: Causes and clinical management. Lancet Neurol. 2013, 12, 920–930. [Google Scholar] [CrossRef]
- Elgoyhen, A.B.; Langguth, B. Pharmacological approaches to the treatment of tinnitus. Drug Discov. Today 2010, 15, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Cima, R.F.; Maes, I.H.; Joore, M.A.; Scheyen, D.J.; El Refaie, A.; Baguley, D.M.; Anteunis, L.J.; van Breukelen, G.J.; Vlaeyen, J.W. Specialised treatment based on cognitive behaviour therapy versus usual care for tinnitus: A randomised controlled trial. Lancet 2012, 379, 1951–1959. [Google Scholar] [CrossRef]
- Hobson, J.; Chisholm, E.; El Refaie, A. Sound therapy (masking) in the management of tinnitus in adults. Cochrane Database Syst. Rev. 2010, 8, CD006371. [Google Scholar] [CrossRef]
- Hoare, D.J.; Kowalkowski, V.L.; Kang, S.; Hall, D.A. Systematic review and meta-analyses of randomized controlled trials examining tinnitus management. Laryngoscope 2011, 121, 1555–1564. [Google Scholar] [CrossRef] [Green Version]
- Theodoroff, S.M.; Folmer, R.L. Repetitive transcranial magnetic stimulation as a treatment for chronic tinnitus: A critical review. Otol. Neurotol. 2013, 34, 199–208. [Google Scholar] [CrossRef]
- Anders, M.; Dvorakova, J.; Rathova, L.; Havrankova, P.; Pelcova, P.; Vaneckova, M.; Jech, R.; Holcat, M.; Seidl, Z.; Raboch, J. Efficacy of repetitive transcranial magnetic stimulation for the treatment of refractory chronic tinnitus: A randomized, placebo controlled study. Neuroendocrinol. Lett. 2010, 31, 238–249. [Google Scholar]
- Barwood, C.H.; Wilson, W.J.; Malicka, A.N.; McPherson, B.; Lloyd, D.; Munt, K.; Murdoch, B.E. The effect of rTMS on auditory processing in adults with chronic, bilateral tinnitus: A placebo-controlled pilot study. Brain Stimul. 2013, 6, 752–759. [Google Scholar] [CrossRef]
- Folmer, R.L.; Theodoroff, S.M.; Casiana, L.; Shi, Y.; Griest, S.; Vachhani, J. Repetitive transcranial magnetic stimulation treatment for chronic tinnitus: A randomized clinical trial. JAMA Otolaryngol. Head. Neck Surg. 2015, 141, 716–722. [Google Scholar] [CrossRef] [Green Version]
- Lefaucheur, J.P.; Aleman, A.; Baeken, C.; Benninger, D.H.; Brunelin, J.; Di Lazzaro, V.; Filipović, S.R.; Grefkes, C.; Hasan, A.; Hummel, F.; et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): An update (2014–2018). Clin. Neurophysiol. 2020, 131, 474–528. [Google Scholar] [CrossRef]
- Marcondes, R.A.; Sanchez, T.G.; Kii, M.A.; Ono, C.R.; Buchpiguel, C.A.; Langguth, B.; Marcolin, M.A. Repetitive transcranial magnetic stimulation improve tinnitus in normal hearing patients: A double-blind controlled, clinical and neuroimaging outcome study. Eur. J. Neurol. 2010, 17, 38–44. [Google Scholar] [CrossRef]
- Frank, G.; Kleinjung, T.; Landgrebe, M.; Vielsmeier, V.; Steffenhagen, C.; Burger, J.; Frank, E.; Vollberg, G.; Hajak, G.; Langguth, B. Left temporal low-frequency rTMS for the treatment of tinnitus: Clinical predictors of treatment outcome—a retrospective study. Eur. J. Neurol. 2010, 17, 951–956. [Google Scholar] [CrossRef]
- Khedr, E.M.; Abo-Elfetoh, N.; Rothwell, J.C.; El-Atar, A.; Sayed, E.; Khalifa, H. Contralateral versus ipsilateral rTMS of temporoparietal cortex for the treatment of chronic unilateral tinnitus: Comparative study. Eur. J. Neurol. 2010, 17, 976–983. [Google Scholar] [CrossRef]
- Kim, B.G.; Kim, D.Y.; Kim, S.K.; Kim, J.M.; Baek, S.H.; Moon, I.S. Comparison of the outcomes of repetitive transcranial magnetic stimulation to the ipsilateral and contralateral auditory cortex in unilateral tinnitus. Electromagn. Biol. Med. 2014, 33, 211–215. [Google Scholar] [CrossRef]
- Rossi, S.; De Capua, A.; Ulivelli, M.; Bartalini, S.; Falzarano, V.; Filippone, G.; Passero, S. Effects of repetitive transcranial magnetic stimulation on chronic tinnitus: A randomised, crossover, double blind, placebo controlled study. J. Neurol. Neurosurg. Psychiatry 2007, 78, 857–863. [Google Scholar] [CrossRef] [Green Version]
- Soleimani, R.; Jalali, M.M.; Hasandokht, T. Therapeutic impact of repetitive transcranial magnetic stimulation (rTMS) on tinnitus: A systematic review and meta-analysis. Eur. Arch. Otorhinolaryngol. 2016, 273, 1663–1675. [Google Scholar] [CrossRef]
- Hoekstra, C.E.; Versnel, H.; Neggers, S.F.; Niesten, M.E.; van Zanten, G.A. Bilateral low-frequency repetitive transcranial magnetic stimulation of the auditory cortex in tinnitus patients is not effective: A randomised controlled trial. Audiol. Neurootol. 2013, 18, 362–373. [Google Scholar] [CrossRef]
- Landgrebe, M.; Hajak, G.; Wolf, S.; Padberg, F.; Klupp, P.; Fallgatter, A.J.; Polak, T.; Höppner, J.; Haker, R.; Cordes, J.; et al. 1-Hz rTMS in the treatment of tinnitus: A sham-controlled, randomized multicenter trial. Brain Stimul. 2017, 10, 1112–1120. [Google Scholar] [CrossRef]
- Sahlsten, H.; Virtanen, J.; Joutsa, J.; Niinivirta-Joutsa, K.; Löyttyniemi, E.; Johansson, R.; Paavola, J.; Taiminen, T.; Sjösten, N.; Salonen, J.; et al. Electric field-navigated transcranial magnetic stimulation for chronic tinnitus: A randomized, placebo-controlled study. Int. J. Audiol. 2017, 56, 692–700. [Google Scholar] [CrossRef]
- Li, X.T. The distribution of left and right handedness in Chinese people. Acta Psychol. 1983, 3, 268–276. [Google Scholar]
- Kushner, H.I. Why are there (almost) no left-handers in China? Endeavour 2012, 37, 71–81. [Google Scholar] [CrossRef]
- Figueiredo, R.R.; Azevedo, A.A.; Oliveira, P. Correlation analysis of the visual-analogue scale and the Tinnitus Handicap Inventory in tinnitus patients. Braz. J. Otorhinolaringol. 2009, 75, 76–79. [Google Scholar] [CrossRef] [Green Version]
- De Ridder, D.; Song, J.J.; Vanneste, S. Frontal cortex TMS for tinnitus. Brain Stimul. 2013, 6, 355–362. [Google Scholar] [CrossRef]
- Newman, C.W.; Jacobson, G.P.; Spitzer, J.B. Development of the tinnitus handicap inventory. Arch. Otolaryngol. Head Neck Surg. 1996, 122, 143–148. [Google Scholar] [CrossRef]
- McCombe, A.; Baguley, D.; Coles, R.; McKenna, L.; McKinney, C.; Windle-Taylor, P.; British Association of Otolaryngologists, Head and Neck Surgeons. Guidelines for the grading of tinnitus severity: The results of a working group commissioned by the British Association of Otolaryngologists, Head and Neck Surgeons, 1999. Clin. Otolaryngol. Allied Sci. 2001, 26, 388–393. [Google Scholar] [CrossRef]
- Sahlsten, H.; Holm, A.; Rauhala, E.; Takala, M.; Löyttyniemi, E.; Karukivi, M.; Nikkilä, J.; Ylitalo, K.; Paavola, J.; Johansson, R.; et al. Neuronavigated versus non-navigated repetitive transcranial magnetic stimulation for chronic tinnitus: A randomized study. Trends Hear. 2019, 23, 2331216518822198. [Google Scholar] [CrossRef]
- Yang, H.; Cheng, G.; Liang, Z.; Deng, W.; Huang, X.; Gao, M.; Zheng, Y. Efficacy of repetitive transcranial magnetic stimulation (rTMS) for Tinnitus: A retrospective study. Ear Nose Throat J. 2021; 1455613211016896, Online ahead of print. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Rossini, P.M.; Barker, A.T.; Berardelli, A.; Caramia, M.D.; Caruso, G.; Cracco, R.Q.; Dimitrijević, M.R.; Hallett, M.; Katayama, Y.; Lücking, C.H. Non-invasive electrical and magnetic stimulation of the brain, spinal cord and roots: Basic principles and procedures for routine clinical application. Report of an IFCN committee. Electroencephalogr. Clin. Neurophysiol. 1994, 91, 79–92. [Google Scholar] [CrossRef]
- Langguth, B.; Eichhammer, P.; Kreutzer, A.; Maenner, P.; Marienhagen, J.; Kleinjung, T.; Sand, P.; Hajak, G. The impact of auditory cortex activity on characterizing and treating patients with chronic tinnitus—First results from a PET study. Acta Otolaryngol. Suppl. 2006, 556, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Boyen, K.; Langers, D.R.; de Kleine, E.; van Dijk, P. Gray matter in the brain: Differences associated with tinnitus and hearing loss. Hear Res. 2013, 295, 67–78. [Google Scholar] [CrossRef] [PubMed]
- Plewnia, C.; Reimold, M.; Najib, A.; Reischl, G.; Plontke, S.K.; Gerloff, C. Moderate therapeutic efficacy of positron emission tomography-navigated repetitive transcranial magnetic stimulation for chronic tinnitus: A randomised, controlled pilot study. J. Neurol. Neurosurg. Psychiatry 2007, 78, 152–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smits, M.; Kovacs, S.; de Ridder, D.; Peeters, R.; van Hecke, P.; Sunaert, S. Lateralization of functional magnetic resonance imaging (fMRI) activation in the auditory pathway of patients with lateralized tinnitus. Neuroradiology 2007, 49, 669–679. [Google Scholar] [CrossRef] [Green Version]
- Yilmaz, M.; Yener, M.H.; Turgut, N.F.; Aydin, F.; Altug, T. Effectiveness of transcranial magnetic stimulation application in treatment of tinnitus. J. Craniofac. Surg. 2014, 25, 1315–1318. [Google Scholar] [CrossRef]
- Wang, H.; Li, B.; Wu, H.; Shi, H.; Yin, S. Combination of gaps in noise detection and visual analog scale for measuring tinnitus components in patients treated with repetitive transcranial magnetic stimulation. Auris Nasus Larynx 2016, 43, 254–258. [Google Scholar] [CrossRef]
- Cacace, A.T.; Hu, J.; Romero, S.; Xuan, Y.; Burkard, R.F.; Tyler, R.S. Glutamate is down- regulated and tinnitus loudness-levels decreased following rTMS over auditory cortex of the left hemisphere: A prospective randomized single-blinded sham-controlled cross-over study. Hear Res. 2018, 358, 59–73. [Google Scholar] [CrossRef]
- Piccirillo, J.F.; Garcia, K.S.; Nicklaus, J.; Pierce, K.; Burton, H.; Vlassenko, A.G.; Mintun, M.; Duddy, D.; Kallogjeri, D.; Spitznagel, E.L., Jr. Low-frequency repetitive transcranial magnetic stimulation to the temporoparietal junction for tinnitus. Arch. Otolaryngol. Head Neck Surg. 2011, 137, 221–228. [Google Scholar] [CrossRef] [Green Version]
- Plewnia, C.; Vonthein, R.; Wasserka, B.; Arfeller, C.; Naumann, A.; Schraven, S.P.; Plontke, S.K. Treatment of chronic tinnitus with θ burst stimulation: A randomized controlled trial. Neurology 2012, 78, 1628–1634. [Google Scholar] [CrossRef]
- Langguth, B.; Landgrebe, M.; Frank, E.; Schecklmann, M.; Sand, P.G.; Vielsmeier, V.; Hajak, G.; Kleinjung, T. Efficacy of different protocols of transcranial magnetic stimulation for the treatment of tinnitus: Pooled analysis of two randomized controlled studies. World J. Biol. Psychiatry 2014, 15, 276–285. [Google Scholar] [CrossRef]
- De Ridder, D.; Verstraeten, E.; Van der Kelen, K.; De Mulder, G.; Sunaert, S.; Verlooy, J.; Van de Heyning, P.; Moller, A. Transcranial magnetic stimulation for tinnitus: Influence of tinnitus duration on stimulation parameter choice and maximal tinnitus suppression. Otol. Neurotol. 2005, 26, 616–619. [Google Scholar] [CrossRef]
- Jastreboff, P.J.; Hazell, J.W.; Graham, R.L. Neurophysiological model of tinnitus: Dependence of the minimal masking level on treatment outcome. Hear Res. 1994, 80, 216–232. [Google Scholar] [CrossRef]
- Udupi, V.A.; Uppunda, A.K.; Mohan, K.M.; Alex, J.; Mahendra, M.H. The relationship of perceived severity of tinnitus with depression, anxiety, hearing status, age and gender in individuals with tinnitus. Int. Tinnitus J. 2013, 18, 29–34. [Google Scholar] [CrossRef]
- Mühlau, M.; Rauschecker, J.P.; Oestreicher, E.; Gaser, C.; Röttinger, M.; Wohlschläger, A.M.; Simon, F.; Etgen, T.; Conrad, B.; Sander, D. Structural brain changes in tinnitus. Cereb. Cortex 2006, 16, 1283–1288. [Google Scholar] [CrossRef]
- Crottaz-Herbette, S.; Menon, V. Where and when the anterior cingulate cortex modulates attentional response: Combined fMRI and ERP evidence. J. Cogn. Neurosci. 2006, 18, 766–780. [Google Scholar] [CrossRef]
- Hullfish, J.; Sedley, W.; Vanneste, S. Prediction and perception: Insights for (and from) tinnitus. Neurosci. Biobehav. Rev. 2019, 102, 1–12. [Google Scholar] [CrossRef]
- Antony, M.; Bieling, P.J.; Cox, B.J.; Enns, M.W.; Swinson, R.P. Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales in clinical groups and community a sample. Psychol. Assess. 1998, 10, 176–181. [Google Scholar] [CrossRef]
- Husain, W.; Suhailah, W.; Othman, A.; Othman, N.; Adilah, N.; Mohamad, W.; Najibah, W.; Mohd, Z. Determining the internal and external reliability of Depression, Anxiety and Stress Scales (DASS-21) in assessing psychological symptoms among patients with tinnitus. NeuroQuantology 2018, 16, 97–102. [Google Scholar] [CrossRef]
- Sahlsten, H.; Isohanni, J.; Haapaniemi, J.; Salonen, J.; Paavola, J.; Löyttyniemi, E.; Johansson, R.; Jääskeläinen, S.K. Electric field navigated transcranial magnetic stimulation for chronic tinnitus: A pilot study. Int. J. Audiol. 2015, 54, 899–909. [Google Scholar] [CrossRef]
- Meikle, M.B.; Vernon, J.; Johnson, R.M. The perceived severity of tinnitus. Some observations concerning a large population of tinnitus clinic patients. Otolaryngol. Head Neck Surg. 1984, 92, 689–696. [Google Scholar] [CrossRef]
- Folmer, R.L.; Griest, S.E.; Martin, W.H. Chronic tinnitus as phantom auditory pain. Otolaryngol. Head Neck Surg. 2001, 124, 394–400. [Google Scholar] [CrossRef]
- Henry, J.A.; Dennis, K.C.; Schechter, M. General review of tinnitus: Prevalence, mechanisms, effects, and management. J. Speech Lang. Hear Res. 2005, 48, 1204–1235. [Google Scholar] [CrossRef]
- Raj-Koziak, D.; Gos, E.; Świerniak, W.; Karpiesz, L.; Niedziałek, I.; Włodarczyk, E.; Skarżyński, H.; Skarżyński, P.H. Relationship between tinnitus loudness measure by visual analogue scale and psychoacoustic matching of tinnitus loudness. Otol. Neurotol. 2019, 40, 16–21. [Google Scholar] [CrossRef]
- Sandlin, R.E.; Olsson, R.J. Evaluation and selection of maskers and other devices used in the treatment of tinnitus and hyperacusis. Trends Amplif. 1999, 4, 6–26. [Google Scholar] [CrossRef] [Green Version]
- Hiller, W.; Goebel, G. When tinnitus loudness and annoyance are discrepant: Audiological characteristics and psychological profile. Audiol. Neurootol. 2007, 12, 391–400. [Google Scholar] [CrossRef]
- Meikle, M.; Taylor-Walsh, E. Characteristics of tinnitus and related observations in over 1800 tinnitus clinic patients. J. Laryngol. Otol. Suppl. 1984, 9, 17–21. [Google Scholar] [CrossRef]
- Hiller, W.; Goebel, G. Factors influencing tinnitus loudness and annoyance. Arch. Otolaryngol. Head Neck Surg. 2006, 132, 1323–1330. [Google Scholar] [CrossRef] [Green Version]
- Folmer, L.R.; Griest, S.E.; Meikle, M.B.; Martin, W.H. Tinnitus severity, loudness, and depression. Otolaryngol. Head Neck Surg. 1999, 121, 48–51. [Google Scholar] [CrossRef]
- Mennemeier, M.; Munn, T.; Allensworth, M.; Lenow, J.K.; Brown, G.; Allen, S.; Dornhoffer, J.; Williams, D. Laterality, frequency and replication of rTMS treatment for chronic tinnitus: Pilot studies and a review of maintenance treatment. Hear Res. 2013, 295, 30–37. [Google Scholar] [CrossRef] [Green Version]
- Ruohonen, J.; Karhu, J. Navigated transcranial magnetic stimulation. Neurophysiol. Clin. 2010, 40, 7–17. [Google Scholar] [CrossRef]
- Julkunen, P.; Säisänen, L.; Danner, N.; Niskanen, E.; Hukkanen, T.; Mervaala, E.; Könönen, M. Comparison of navigated and non-navigated transcranial magnetic stimulation for motor cortex mapping, motor threshold and motor evoked potentials. Neuroimage 2009, 44, 790–795. [Google Scholar] [CrossRef] [PubMed]
- Noh, T.S.; Rah, Y.C.; Kyong, J.S.; Kim, J.S.; Park, M.K.; Lee, J.H.; Oh, S.H.; Chung, C.K.; Suh, M.W. Comparison of treatment outcomes between 10 and 20 EEG electrode location system-guided and neuronavigation-guided repetitive transcranial magnetic stimulation in chronic tinnitus patients and target localization in the Asian brain. Acta Oto-Laryngol. 2010, 137, 945–951. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment Group | ||||||||
|---|---|---|---|---|---|---|---|---|
| Left | Right | Bilateral | Sham | Statistic | p-Value | Post-Hoc (p < 0.05) | ||
| Sex (n) | Male | 17 | 14 | 14 | 14 | χ2 (3) = 1.9 | 0.600 | |
| Female | 12 | 9 | 16 | 8 | ||||
| Tinnitus side (n) | Left | 17 | 11 | 15 | 10 | χ2 (3) = 1.9 | 0.789 | |
| Right | 12 | 12 | 15 | 12 | ||||
| Age (years) | Mean | 44.2 | 40.8 | 36.4 | 39.9 | H (3) = 5.3 | 0.151 | |
| STD | 13.3 | 10.8 | 11.7 | 10.2 | ||||
| PTA (dB HL) | Mean | 34.3 | 38.9 | 22.2 | 35.5 | H (3) = 14.6 | 0.002 * | Right, Sham > Bilateral |
| STD | 19.2 | 17.9 | 11.8 | 20.2 | ||||
| Duration of tinnitus (years) | Mean | 3.2 | 3.2 | 1.6 | 1.8 | H (3) = 8.6 | 0.034 * | Left > Bilateral |
| STD | 3.0 | 3.0 | 2.0 | 1.2 | ||||
| RMT/% MSO | Mean | 30.2 | 33.2 | 34.3 | 33.1 | H (3) = 11.6 | 0.009 * | Bilateral > Right |
| STD | 11.4 | 5 | 8.6 | 5.7 | ||||
| Tinnitus | Test | VAS | THI | HADS- | HADS- | Pitch | Loudness | ||
|---|---|---|---|---|---|---|---|---|---|
| Side | A | D | (kHz) | (dB SL) | |||||
| Left treatment | Left | Pre | Mean | 5.8 | 47.4 | 9.4 | 6.9 | 4.9 | 7.9 |
| STD | 2.0 | 26.8 | 4.4 | 4.4 | 2.4 | 7.3 | |||
| Post | Mean | 4.3 * | 43.8 | 7.9 * | 6.1 | 3.7 * | 11.5 | ||
| STD | 1.9 | 29.0 | 3.3 | 3.9 | 2.4 | 7.7 | |||
| Right | Pre | Mean | 5.8 | 44.0 | 9.6 | 7.6 | 4.2 | 14.6 | |
| STD | 1.4 | 21.7 | 3.3 | 4.5 | 2.7 | 8.9 | |||
| Post | Mean | 4.8 * | 35.8 * | 7.4 * | 7.1 | 3.9 | 11.3 | ||
| STD | 2.0 | 24.1 | 2.9 | 4.2 | 2.9 | 12.3 | |||
| All | Pre | Mean | 5.8 | 46.0 | 9.5 | 7.2 | 4.6 | 10.7 | |
| STD | 1.8 | 24.5 | 3.9 | 4.4 | 2.5 | 8.5 | |||
| Post | Mean | 4.5 * | 40.5 * | 7.7 * | 6.5 | 3.8 * | 11.4 | ||
| STD | 1.9 | 26.9 | 3.1 | 4 | 2.6 | 9.6 | |||
| Right treatment | Left | Pre | Mean | 4.9 | 43.2 | 8.7 | 5.4 | 4.5 | 13.2 |
| STD | 1.8 | 26.6 | 3.4 | 3.2 | 2.6 | 16.3 | |||
| Post | Mean | 5.0 | 45.9 | 7.5 | 5.2 | 4.5 | 13.2 | ||
| STD | 1.8 | 29.7 | 3.0 | 4.0 | 2.5 | 11.7 | |||
| Right | Pre | Mean | 4.7 | 44.4 | 8.1 | 6.4 | 3.8 | 15.4 | |
| STD | 1.9 | 28.0 | 4.0 | 3.2 | 2.2 | 16.2 | |||
| Post | Mean | 4.5 | 46.2 | 7.3 | 6.2 | 4.4 | 13.3 | ||
| STD | 1.9 | 33.3 | 3.4 | 4.0 | 1.9 | 12.9 | |||
| All | Pre | Mean | 4.8 | 44.6 | 8.4 | 5.9 | 4.1 | 14.3 | |
| STD | 1.8 | 27.7 | 3.7 | 3.2 | 2.4 | 15.9 | |||
| Post | Mean | 4.7 | 45.3 | 7.4 | 5.7 | 4.5 | 13.3 | ||
| STD | 1.8 | 30.2 | 3.2 | 3.9 | 2.1 | 12.0 | |||
| Bilateral treatment | Left | Pre | Mean | 4.6 | 36.4 | 6.7 | 5.2 | 4.3 | 14.0 |
| STD | 2.2 | 20.5 | 3.3 | 4.5 | 2.3 | 15.8 | |||
| Post | Mean | 3.7 * | 35.6 | 5.9 | 6.0 | 3.6 | 14.3 | ||
| STD | 2.1 | 24.9 | 2.8 | 3.7 | 2.9 | 13.5 | |||
| Right | Pre | Mean | 4.3 | 38.8 | 7.7 | 5.3 | 3.5 | 17.0 | |
| STD | 2.1 | 23.0 | 3.1 | 4.0 | 2.3 | 12.9 | |||
| Post | Mean | 4.2 | 36.9 | 6.1 * | 5.7 | 3.6 | 17.3 | ||
| STD | 2.2 | 20.7 | 2.5 | 3.5 | 2.7 | 13.7 | |||
| All | Pre | Mean | 4.5 | 37.6 | 7.2 | 5.2 | 3.9 | 15.5 | |
| STD | 2.1 | 21.5 | 3.2 | 4.2 | 2.3 | 14.3 | |||
| Post | Mean | 3.9 * | 36.3 | 6.0 * | 5.9 | 3.6 | 15.8 | ||
| STD | 2.2 | 22.5 | 2.6 | 3.6 | 2.7 | 13.5 | |||
| Sham treatment | Left | Pre | Mean | 5.0 | 39.6 | 7.4 | 7.6 | 5.5 | 7.5 |
| STD | 1.3 | 15.2 | 3.6 | 4.5 | 2.2 | 5.9 | |||
| Post | Mean | 5.0 | 39.6 | 6.6 | 7.4 | 5.5 | 3.5 | ||
| STD | 1.3 | 15.7 | 3.3 | 4.5 | 2.2 | 4.7 | |||
| Right | Pre | Mean | 5.7 | 43.0 | 7.7 | 8.3 | 5.4 | 6.3 | |
| STD | 1.9 | 26.8 | 3.3 | 2.8 | 2.2 | 7.7 | |||
| Post | Mean | 5.5 | 42.7 | 8.2 | 8.0 | 5.3 | 5.0 | ||
| STD | 2.1 | 24.8 | 2.0 | 3.3 | 2.3 | 5.6 | |||
| All | Pre | Mean | 5.4 | 41.5 | 7.6 | 8.0 | 5.4 | 6.8 | |
| STD | 1.7 | 21.9 | 3.4 | 3.6 | 2.1 | 6.8 | |||
| Post | Mean | 5.3 | 41.3 | 7.5 | 7.7 | 5.4 | 4.3 | ||
| STD | 1.8 | 20.8 | 2.7 | 3.8 | 2.2 | 5.2 |
| VAS | THI | HADS- A | HADS- D | Pitch (kHz) | Loudness (dB SL) | |||
|---|---|---|---|---|---|---|---|---|
| Left treatment | Left ear | Mean | −1.5 | −3.6 | −1.5 | −0.9 | −1.3 | 3.5 |
| STD | 1.4 | 14.4 | 2.3 | 3.1 | 1.8 | 5.8 | ||
| Right ear | Mean | −0.9 | −8.2 | −2.2 | −0.5 | −0.4 | −3.3 | |
| STD | 1.2 | 12.6 | 3.2 | 3.3 | 1.3 | 9.1 | ||
| All | Mean | −1.2 | −5.5 | −1.8 | −0.7 | −0.9 | 0.7 | |
| STD | 1.3 | 13.6 | 2.6 | 3.1 | 1.6 | 8.0 | ||
| Right treatment | Left ear | Mean | 0.1 | 1.2 | 1.2 | −0.2 | 0.1 | 0.0 |
| STD | 0.3 | 7.4 | 2.5 | 1.9 | 1.0 | 15.7 | ||
| Right ear | Mean | −0.2 | 0.3 | −0.8 | −0.3 | 0.6 | −2.1 | |
| STD | 0.4 | 9.1 | 2.4 | 2.0 | 1.1 | 9.9 | ||
| All | Mean | 0.0 | 0.7 | −1.0 | −0.2 | 0.3 | −1.1 | |
| STD | 0.4 | 8.2 | 2.4 | 1.9 | 1.1 | 12.7 | ||
| Bilateral treatment | Left ear | Mean | −0.9 | −0.8 | −0.8 | 0.8 | −0.7 | 0.3 |
| STD | 0.8 | 16.3 | 2.9 | 2.5 | 2.4 | 10.1 | ||
| Right ear | Mean | −0.1 | −1.9 | −1.6 | 0.5 | 0.0 | 0.3 | |
| STD | 0.6 | 18.1 | 2.8 | 2.5 | 1.8 | 13.4 | ||
| All | Mean | −0.5 | −1.3 | −1.2 | 0.6 | −0.4 | 0.3 | |
| STD | 0.8 | 16.9 | 2.9 | 2.4 | 2.1 | 11.7 | ||
| Sham treatment | Left ear | Mean | 0.0 | 0.0 | −0.8 | −0.2 | 0.0 | −4.0 |
| STD | 0.0 | 1.3 | 1.7 | 1.0 | 0.0 | 4.4 | ||
| Right ear | Mean | −0.2 | −0.3 | 0.5 | −0.3 | −0.1 | −1.3 | |
| STD | 0.4 | 3.9 | 1.7 | 1.0 | 0.2 | 6.8 | ||
| All | Mean | −0.1 | −0.2 | −0.1 | −0.3 | 0.0 | −2.5 | |
| STD | 0.3 | 3.0 | 1.7 | 1.0 | 0.1 | 5.9 |
| PTA | Dur tin | VAS | THI | HADS-A | HADS-D | Pitch | Loudness | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (kHz) | (dB SL) | |||||||||||||||
| r | p | r | p | r | p | r | p | r | p | r | p | r | p | r | p | |
| Age | 0.15 | 0.129 | 0.34 | < 0.001 * | 0.07 | 0.484 | −0.05 | 0.641 | −0.25 | 0.010 | −0.09 | 0.343 | 0.07 | 0.490 | −0.18 | 0.070 |
| PTA | 0.22 | 0.028 | 0.10 | 0.309 | 0.14 | 0.154 | 0.07 | 0.493 | −0.05 | 0.583 | 0.17 | 0.080 | −0.13 | 0.180 | ||
| Dur tin | 0.10 | 0.293 | 0.01 | 0.953 | −0.03 | 0.769 | −0.24 | 0.014 | 0.21 | 0.030 | −0.05 | 0.648 | ||||
| VAS | 0.63 | < 0.001 * | 0.30 | 0.002 * | 0.32 | 0.001 * | 0.21 | 0.031 | −0.13 | 0.197 | ||||||
| THI | 0.60 | < 0.001 * | 0.49 | < 0.001 * | 0.14 | 0.146 | −0.01 | 0.950 | ||||||||
| HADS-A | 0.57 | < 0.001 * | 0.09 | 0.375 | 0.06 | 0.568 | ||||||||||
| HADS-D | 0.07 | 0.509 | 0.02 | 0.853 | ||||||||||||
| Pitch | −0.09 | 0.388 | ||||||||||||||
| Forward Stepwise Regression (F to Enter = 4.0, p < 0.48) | |||||||
|---|---|---|---|---|---|---|---|
| Dependent Variable | Variable | Coef. | Std. Coeff. | Std. Error | F-to-Remove | p | r2 |
| VAS | Constant | 2.94 | 0.32 | ||||
| THI | 0.04 | 0.51 | 0.01 | 35.7 | <0.001 | 0.26 | |
| ANOVA: F(1, 102) = 35.7, p < 0.001 | |||||||
| THI | Constant | −12.9 | 4.98 | ||||
| VAS | 3.8 | 0.30 | 0.89 | 18.0 | <0.001 | 0.57 | |
| HADS-A | 5.1 | 0.60 | 0.60 | 73.0 | <0.001 | 0.49 | |
| ANOVA: F(1, 102) = 66.9, p < 0.001 | |||||||
| Forward Stepwise Regression (F to Enter = 4.0, p < 0.48) | |||||||
|---|---|---|---|---|---|---|---|
| Dependent Variable | Variable | Coef. | Std. Coeff. | Std. Error | F-to-Remove | p | r2 |
| VAS | Constant | 0.44 | 0.15 | ||||
| THI | 0.02 | 0.24 | 0.01 | 4.20 | 0.045 | 0.14 | |
| HADS-A | 0.14 | 0.34 | 0.05 | 8.00 | 0.007 | 0.33 | |
| Pitch | 0.28 | 0.47 | 0.07 | 18.40 | <0.001 | 0.37 | |
| ANOVA: F(3, 55) = 10.9, p < 0.001 | |||||||
| THI | Constant | 0.28 | 2.02 | ||||
| HADS-A | 2.07 | 0.37 | 0.66 | 9.97 | 0.003 | 0.42 | |
| HADS-D | 1.52 | 0.28 | 0.63 | 5.81 | 0.019 | 0.50 | |
| ANOVA: F(1, 57) = 11.9, p = 0.001 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Shen, Y.-C.; Galvin, J.J., III; Liu, J.-S.; Tao, D.-D. Effect of Ipsilateral, Contralateral or Bilateral Repetitive Transcranial Magnetic Stimulation in Patients with Lateralized Tinnitus: A Placebo-Controlled Randomized Study. Brain Sci. 2022, 12, 733. https://doi.org/10.3390/brainsci12060733
Li Y, Shen Y-C, Galvin JJ III, Liu J-S, Tao D-D. Effect of Ipsilateral, Contralateral or Bilateral Repetitive Transcranial Magnetic Stimulation in Patients with Lateralized Tinnitus: A Placebo-Controlled Randomized Study. Brain Sciences. 2022; 12(6):733. https://doi.org/10.3390/brainsci12060733
Chicago/Turabian StyleLi, Yi, Yong-Cong Shen, John J. Galvin, III, Ji-Sheng Liu, and Duo-Duo Tao. 2022. "Effect of Ipsilateral, Contralateral or Bilateral Repetitive Transcranial Magnetic Stimulation in Patients with Lateralized Tinnitus: A Placebo-Controlled Randomized Study" Brain Sciences 12, no. 6: 733. https://doi.org/10.3390/brainsci12060733
APA StyleLi, Y., Shen, Y.-C., Galvin, J. J., III, Liu, J.-S., & Tao, D.-D. (2022). Effect of Ipsilateral, Contralateral or Bilateral Repetitive Transcranial Magnetic Stimulation in Patients with Lateralized Tinnitus: A Placebo-Controlled Randomized Study. Brain Sciences, 12(6), 733. https://doi.org/10.3390/brainsci12060733