
Sex Differences in Substance Use, Prevalence, Pharmacological Therapy, and Mental Health in Adolescents with Attention-Deficit/Hyperactivity Disorder (ADHD)

 , , ,
, , , 
Abstract
1. Introduction
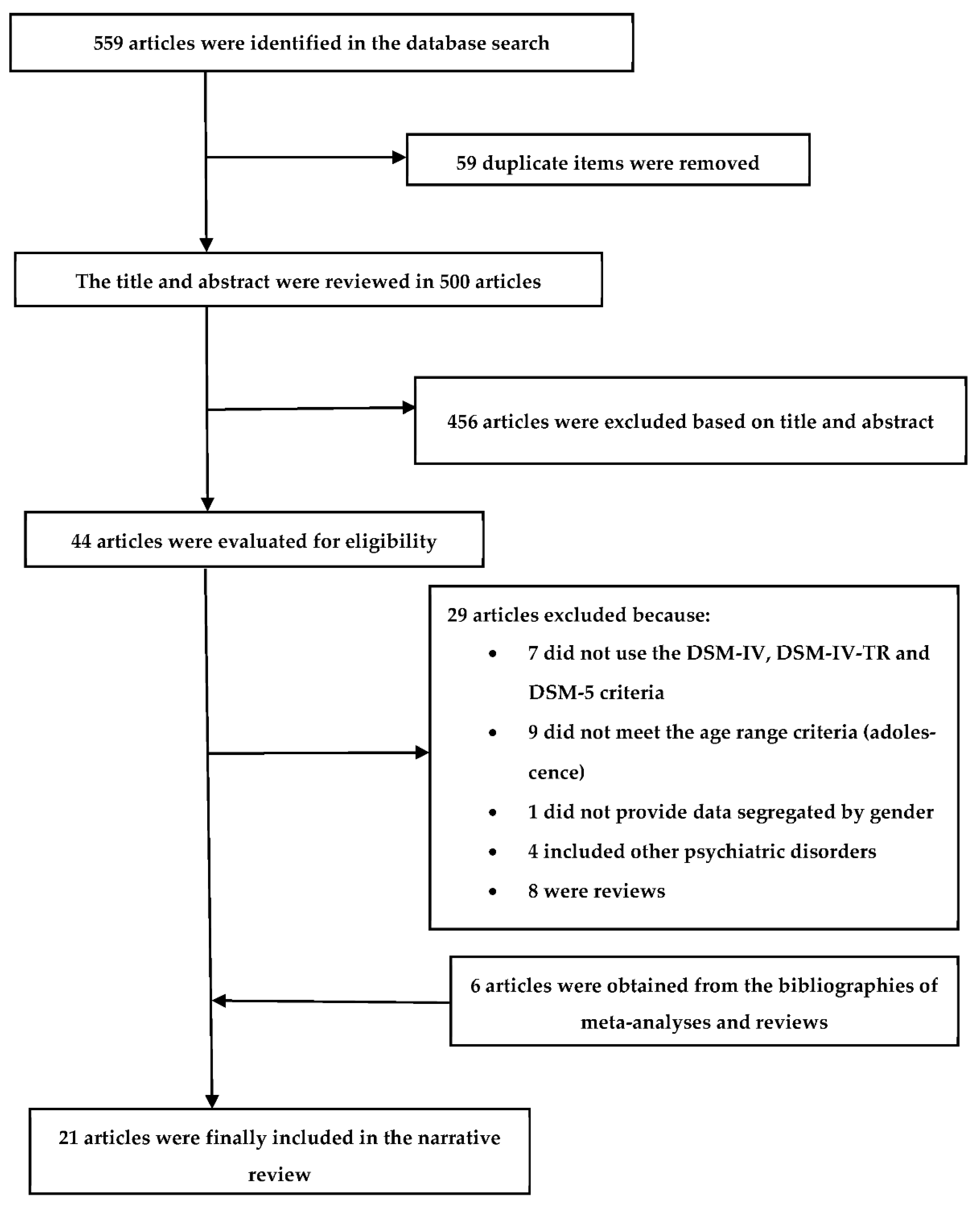
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Quality Assessment
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chandra, P.S.; Satyanarayana, V.A. Gender disadvantage and common mental disorders in women. Int. Rev. Psychiatry 2010, 22, 513–524. [Google Scholar] [CrossRef] [PubMed]
- Howard, L.M. Gender differences in mental health. Int. Rev. Psychiatry 2010, 22, 415–416. [Google Scholar] [CrossRef] [PubMed]
- Torrens-Melich, M.; Orengo, T.; de Fonseca, F.R.; Almodóvar, I.; Baquero, A.; Benito, A. Gender Perspective in Dual Diagnosis. Brain Sci. 2021, 11, 1101. [Google Scholar] [CrossRef]
- Herting, M.M.; Sowell, E.R. Puberty and structural brain development in humans. Front. Neuroendocrinol. 2017, 44, 122–137. [Google Scholar] [CrossRef] [PubMed]
- Blakemore, S.J.; Burnett, S.; Dahl, R.E. The role of puberty in the developing adolescent brain. Hum. Brain Mapp. 2010, 31, 926–933. [Google Scholar] [CrossRef]
- Vijayakumar, N.; Op de Macks, Z.; Shirtcliff, E.A.; Pfeifer, J.H. Puberty and the human brain: Insights into adolescent development. Neurosci. Biobehav. Rev. 2018, 92, 417–436. [Google Scholar] [CrossRef]
- Kurth, F.; Gaser, C.; Luders, E. Development of sex differences in the human brain. Cogn. Neurosci. 2021, 12, 155–162. [Google Scholar] [CrossRef]
- Goddings, A.L.; Beltz, A.; Peper, J.; Crone, E.A.; Braams, B.R. Understanding the Role of Puberty in Structural and Functional Development of the Adolescent Brain. J. Res. Adolesc. 2019, 29, 32–53. [Google Scholar] [CrossRef]
- Lenroot, R.K.; Gogtay, N.; Greenstein, D.K.; Wells, E.M.; Wallace, G.L.; Clasen, L.S.; Blumenthal, J.D.; Lerch, J.; Zijdenbos, A.P.; Evans, A.C.; et al. Sexual dimorphism of brain developmental trajectories during childhood and adolescence. Neuroimage 2007, 36, 1065–1073. [Google Scholar] [CrossRef]
- Peper, J.S.; Burke, S.M.; Wierenga, L.M. Sex differences and brain development during puberty and adolescence. Handb. Clin. Neurol. 2020, 175, 25–54. [Google Scholar]
- Wagner, F.A.; Anthony, J.C. From first drug use to drug dependence; developmental periods of risk for dependence upon marijuana, cocaine, and alcohol. Neuropsychopharmacology 2002, 26, 479–488. [Google Scholar] [CrossRef]
- Jordan, C.J.; Andersen, S.L. Sensitive periods of substance abuse: Early risk for the transition to dependence. Dev. Cogn. Neurosci. 2017, 25, 29–44. [Google Scholar] [CrossRef] [PubMed]
- Gruber, S.A.; Dahlgren, M.K.; Sagar, K.A.; Gönenç, A.; Lukas, S.E. Worth the wait: Effects of age of onset of marijuana use on white matter and impulsivity. Psychopharmacology 2014, 231, 1455–1465. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, M.R.; Weiss, V.G.; Beas, B.S.; Morgan, D.; Bizon, J.L.; Setlow, B. Adolescent risk taking, cocaine self-administration, and striatal dopamine signaling. Neuropsychopharmacology 2014, 39, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Enoch, M.A. The role of early life stress as a predictor for alcohol and drug dependence. Psychopharmacology 2011, 214, 17–31. [Google Scholar] [CrossRef] [PubMed]
- Mannuzza, S.; Klein, R.G.; Truong, N.L.; Moulton, J.L.; Roizen, E.R.; Howell, K.H.; Castellanos, F.X. Age of methylphenidate treatment initiation in children with ADHD and later substance abuse: Prospective follow-up into adulthood. Am. J. Psychiatry 2008, 165, 604–609. [Google Scholar] [CrossRef]
- Polanczyk, G.; de Lima, M.S.; Horta, B.L.; Biederman, J.; Rohde, L.A. The worldwide prevalence of ADHD: A systematic review and metaregression analysis. Am. J. Psychiatry 2007, 164, 942–948. [Google Scholar] [CrossRef]
- Rucklidge, J.J. Gender differences in ADHD: Implications for psychosocial treatments. Expert Rev. Neurother. 2008, 8, 643–655. [Google Scholar] [CrossRef]
- Willcutt, E.G. The prevalence of DSM-IV attention-deficit/hyperactivity disorder: A meta-analytic review. Neurotherapeutics 2012, 9, 490–499. [Google Scholar] [CrossRef]
- Biederman, J.; Monuteaux, M.C.; Mick, E.; Spencer, T.; Wilens, T.E.; Silva, J.M.; Snyder, L.E.; Faraone, S.V. Young adult outcome of attention deficit hyperactivity disorder: A controlled 10-year follow-up study. Psychol. Med. 2006, 36, 167–179. [Google Scholar] [CrossRef]
- Faraone, S.V.; Biederman, J. What is the prevalence of adult ADHD? Results of a population screen of 966 adults. J. Atten. Disord. 2005, 9, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Okie, S. ADHD in adults. N. Engl. J. Med. 2006, 354, 2637–2641. [Google Scholar] [CrossRef] [PubMed]
- Barkley, R.A. Major life activity and health outcomes associated with attention-deficit/hyperactivity disorder. J. Clin. Psychiatry 2002, 63 (Suppl. 12), 10–15. [Google Scholar]
- Sibley, M.H.; Kuriyan, A.B.; Evans, S.W.; Waxmonsky, J.G.; Smith, B.H. Pharmacological and psychosocial treatments for adolescents with ADHD: An updated systematic review of the literature. Clin. Psychol. Rev. 2014, 34, 218–232. [Google Scholar] [CrossRef]
- Visser, S.N.; Danielson, M.L.; Bitsko, R.H.; Holbrook, J.R.; Kogan, M.D.; Ghandour, R.M.; Perou, R.; Blumberg, S.J. Trends in the parent-report of health care provider- diagnosed and medicated attention-deficit/hyperactivity disorder: United States, 2003–2011. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 34–46. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Faraone, S.V.; Biederman, J.; Mick, E. The age-dependent decline of attention deficit hyperactivity disorder: A meta-analysis of follow-up studies. Psychol. Med. 2006, 36, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Molina, B.S.G.; Howard, A.L.; Swanson, J.M.; Stehli, A.; Mitchell, J.T.; Kennedy, T.M.; Epstein, J.N.; Arnold, L.E.; Hechtman, L.; Vitiello, B.; et al. Substance use through adolescence into early adulthood after childhood-diagnosed ADHD: Findings from the MTA longitudinal study. J. Child Psychol. Psychiatry 2018, 59, 692–702. [Google Scholar] [CrossRef]
- Ottosen, C.; Petersen, L.; Larsen, J.T.; Dalsgaard, S. Gender Differences in Associations Between Attention-Deficit/Hyperactivity Disorder and Substance Use Disorder. J. Am. Acad. Child Adolesc. Psychiatry 2015, 55, 227–234.e4. [Google Scholar] [CrossRef][Green Version]
- Zhang-James, Y.; Chen, Q.; Kuja-Halkola, R.; Lichtenstein, P.; Larsson, H.; Faraone, S.V. Machine-Learning prediction of comorbid substance use disorders in ADHD youth using Swedish registry data. J. Child Psychol. Psychiatry 2020, 61, 1370–1379. [Google Scholar] [CrossRef]
- Howard, A.L.; Kennedy, T.M.; Mitchell, J.T.; Sibley, M.H.; Hinshaw, S.P.; Arnold, L.E.; Roy, A.; Stehli, A.; Swanson, J.M.; Molina, B.S.G. Early substance use in the pathway from childhood attention-deficit/hyperactivity disorder (ADHD) to young adult substance use: Evidence of statistical mediation and substance specificity. Psychol. Addict. Behav. 2020, 34, 281–292. [Google Scholar] [CrossRef]
- Dalsgaard, S.; Mortensen, P.B.; Frydenberg, M.; Thomsen, P.H. ADHD, stimulant treatment in childhood and subsequent substance abuse in adulthood—A naturalistic long-term follow-up study. Addict. Behav. 2013, 39, 325–328. [Google Scholar] [CrossRef] [PubMed]
- Galera, C.; Fombonne, E.; Chastang, J.F.; Bouvard, M. Childhood hyperactivity-inattention symptoms and smoking in adolescence. Drug Alcohol Depend. 2008, 78, 101–108. [Google Scholar] [CrossRef]
- Osland, S.; Hirsch, L.; Pringsheim, T. Smoking, alcohol and drug use in youth and adults with attention-deficit hyperactivity disorder. BJPsych Open 2017, 3, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and metaanalyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; Tex Reviewed; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Metaanalyses. 2019. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 20 December 2020).
- Modesti, P.A.; Reboldi, G.; Cappuccio, F.P.; Agyemang, C.; Remuzzi, G.; Rapi, S.; Perruolo, E.; Parati, G.; ESH Working Group on CV Risk in Low Resource Settings. Panethnic Differences in Blood Pressure in Europe: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0147601. [Google Scholar] [CrossRef]
- Barbaresi, W.J.; Katusic, S.K.; Colligan, R.C.; Weaver, A.L.; Leibson, C.L.; Jacobsen, S.J. Long-term stimulant medication treatment of attention-deficit/hyperactivity disorder: Results from a population-based study. J. Dev. Behav. Pediatr. 2006, 27, e0147601. [Google Scholar] [CrossRef] [PubMed]
- Byrd, H.C.M.; Curtin, C.; Anderson, S.E. Attention-Deficit/Hyperactivity Disorder and obesity in US males and females, age 8–15 years: National Health and Nutrition Examination Survey 2001–2004. Pediatr. Obes. 2013, 8, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Cole, W.R.; Mostofsky, S.H.; Larson, J.C.; Denckla, M.B.; Mahone, E.M. Age-related changes in motor subtle signs among girls and boys with ADHD. Neurology 2008, 71, 1514–1520. [Google Scholar] [CrossRef] [PubMed]
- Disney, E.R.; Elkins, I.J.; McGue, M.; Iacono, W.G. Effects of ADHA, Conduct Disorder and gender on substance use and abuse in adolescence. Am. J. Psychiatry 1999, 156, 1515–1521. [Google Scholar] [CrossRef]
- Elkins, I.J.; Saunders, G.R.B.; Malone, S.M.; Wilson, S.; McGue, M.; Iacono, W.G. Mediating pathways from childhood ADHA to adolescent tobacco and marijuana problems: Roles of peer impairment, internalizing, adolescent ADHD symptoms and gender. J. Child Psychol. Psychiatry 2018, 59, 1083–1093. [Google Scholar] [CrossRef]
- Elkins, I.J.; Saunders, G.R.B.; Malone, S.M.; Keyes, M.A.; McGue, M.; Iacono, W.G. Associations between childhood ADHD, gender, and adolescents alcohol and marijuana involvement: A causally informative design. Drug Alcohol Depend. 2018, 184, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Elkins, I.J.; Saunders, G.; Malone, S.M.; Wilson, S.; McGue, M.; Iacono, W.G. Differential implications of persistent, remitted, and late-onset ADHD symptoms for substance abuse in women and men: A twin study from ages 11 to 24. Drug Alcohol Depend. 2020, 212, 107947. [Google Scholar] [CrossRef] [PubMed]
- Gökçe, S.; Yusufoğlu, C.; Akin, E.; Ayaz, M. Effect of gender differences on impulsivity in adolescents with attention-deficit/hyperactivity disorder. Anadolu Psikiyatr. Derg. 2017, 18, 379–386. [Google Scholar]
- Hurtig, T.; Taanila, A.; Moilanen, I.; Nordström, T.; Ebeling, H. Suicidal and self-harm behaviour associated with adolescent attention deficit hyperactivity disorder-a study in the Northern Finland Birth Cohort 1986. Nord. J. Psychiatry 2012, 66, 320–328. [Google Scholar] [CrossRef]
- Huss, M.; Hölling, H.; Kurth, B.M.; Schlack, R. How often are German children and adolescents diagnosed with ADHD? Prevalence based on the judgment of health care professionals: Results of the German health and examination survey (KiGGS). Eur. Child Adolesc. Psychiatry 2008, 1, 52–58. [Google Scholar] [CrossRef]
- Kessler, R.C.; Adler, L.A.; Berglund, P.; Green, J.G.; McLaughlin, K.A.; Fayyad, J.; Russo, L.J.; Sampson, N.A.; Shahly, V.; Zaslavsky, A.M. The effects of temporally secondary co-morbid mental disorders on the associations of DSM-IV ADHD with adverse outcomes in the US National Comorbidity Survey Replication Adolescent Supplement (NCS-A). Psychol. Med. 2014, 44, 1779–1792. [Google Scholar] [CrossRef]
- Latimer, W.W.; Stone, A.L.; Voight, A.; Winters, K.C.; August, G.J. Gender differences in psychiatric comorbidity among adolescents with substance use disorders. Exp. Clin. Psychopharmacol. 2002, 10, 310–315. [Google Scholar] [CrossRef]
- Lee, C.T.; Clark, T.T.; Kollins, S.H.; McClernon, F.J.; Fuemmeler, B.F. Attention Deficit Hyperactivity Disorder symptoms and smoking trajectories: Race and gender differences. Drug Alcohol Depend. 2015, 148, 180–187. [Google Scholar] [CrossRef]
- Madsen, A.G.; Dalsgaard, S. Prevalence of smoking, alcohol and substance use among adolescents with attention-deficit/hyperactivity disorder in Denmark compared with the general population. Nord. J. Psychiatry 2013, 68, 53–59. [Google Scholar] [CrossRef]
- Pineda, D.; Ardila, A.; Rosselli, M.; Arias, B.E.; Henao, G.C.; Gomez, L.F.; Mejia, S.E.; Miranda, M.L. Prevalence of attention-deficit/hyperactivity disorder symptoms in 4- to 17-year-old children in the general population. J. Abnorm. Child Psychol. 1999, 27, 455–462. [Google Scholar] [CrossRef]
- Regan, T.; Tubman, J. Attention Deficit Hyperactivity Disorder (ADHD) Subtypes, Co-Occurring Psychiatric Symptoms and Sexual Risk Behaviors among Adolescents Receiving Substance Abuse Treatment. Subst. Use Misuse 2020, 55, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Rucklidge, J.J. Gender differences in neuropsychological functioning of New Zealand adolescents with and without attention deficit hyperactivity disorder. Int. J. Disabil. Dev. Educ. 2006, 53, 47–66. [Google Scholar] [CrossRef]
- Rucklidge, J.J.; Tannock, R. Psychiatric, psychosocial, and cognitive functioning of female adolescents with ADHD. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 530–540. [Google Scholar] [CrossRef] [PubMed]
- Seidman, L.J.; Biederman, J.; Monuteaux, M.C.; Valera, E.; Doyle, A.E.; Faraone, S.V. Impact of gender and age on executive functioning: Do girls and boys with and without attention deficit hyperactivity disorder differ neuropsychologically in preteen and teenage years? Dev. Neuropsychol. 2005, 27, 79–105. [Google Scholar] [CrossRef] [PubMed]
- Selinus, E.N.; Molero, Y.; Lichtenstein, P.; Anckarsäter, H.; Lundström, S.; Bottai, M.; Hellner Gumpert, C. Subthreshold and threshold attention deficit hyperactivity disorder symptoms in childhood: Psychosocial outcomes in adolescence in boys and girls. Acta Psychiatr. Scand. 2016, 134, 533–545. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, D.; Ciftci, A.; Yalcin, O. Substance use patterns, psychosocial traumas, psychiatric comorbidities, and gender differences among adolescent inpatients at an addiction treatment center. Dusunen Adam 2020, 33, 190–202. [Google Scholar]
- Elkins, I.J.; Saunders, G.R.B.; Malone, S.M.; Keyes, M.A.; Samek, D.R.; McGue, M.; Iacono, W.G. Increased risk of smoking in female adolescents who had childhood ADHD. Am. J. Psychiatry. 2017, 175, 63–70. [Google Scholar] [CrossRef]
- Matthies, S.; Holzner, S.; Feige, B.; Scheel, C.; Perlov, E.; Ebert, D.; van Elst, L.T.; Philipsen, A. ADHD as a serious risk factor for early smoking and nicotine dependence in adulthood. J. Atten. Disord. 2013, 17, 176–186. [Google Scholar] [CrossRef]
- Korsgaard, H.O.; Torgersen, S.; Wentzel-Larsen, T.; Ulberg, R. Substance abuse and personality disorder comorbidity in adolescent outpatients: Are girls more severely ill than boys? Child Adolesc. Psychiatry Ment. Health 2016, 10, 8. [Google Scholar] [CrossRef]
- Yarmush, D.E.; Manchery, L.; Luehring-Jones, P.; Erblich, J. Gender and impulsivity: Effects on cue-induced alcohol craving. Alcohol. Clin. Exp. Res. 2016, 40, 1052–1057. [Google Scholar] [CrossRef]
- Biederman, J.; Mick, E.; Faraone, S.V.; Braaten, E.; Doyle, A.; Spencer, T.; Wilens, T.E.; Frazier, E.; Johnson, M.A. Influence of Gender on Attention Deficit Hyperactivity Disorder in Children Referred to a Psychiatric Clinic. Am. J. Psychiatry 2002, 159, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Biederman, J.; Faraone, S.V. The Massachusetts General Hospital studies of gender influences on attention-deficit/hyperactivity disorder in youth and relatives. Psychiatr. Clin. N. Am. 2004, 27, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Ottosen, C.; Tidselbak, J.; Faraone, S.V.; Chen, Q.; Hartman, C.; Larsson, H.; Dalsgaard, S. Sex differences in comorbidity patterns of attention-deficit/hyperactivity disorder. J. Am. Child Adolesc. Psychiatry 2019, 58, 412–422. [Google Scholar] [CrossRef] [PubMed]
- Steinhausen, H.C.; Bisgaard, C. Substance use disorders in association with attention-deficit/hyperactivity disorder, co-morbid mental disorders, and medication in a nationwide sample. Eur. Neuropsychopharmacol. 2014, 24, 232–241. [Google Scholar] [CrossRef]
- Molina, B.S.; Hinshaw, S.P.; Arnold, L.E.; Swanson, J.M.; Pelham, J.W.E.; Hechtman, L.; Hoza, B.; Epstein, J.N.; Wigal, T.; Abikoff, H.B.; et al. Adolescent substance use in the multimodal treatment study of attention-deficit/hyperactivity disorder (ADHD) (MTA) as a function of childhood ADHD, random assignment to childhood treatments, and subsequent medication. J. Am. Acad. Child Adolesc. Psychiatry 2013, 52, 250–263. [Google Scholar] [CrossRef]
- Quinn, P.D.; Chang, Z.; Hur, K.; Gibbons, R.D.; Lahey, B.B.; Rickert, M.E.; Sjölander, A.; Lichtenstein, P.; Larsson, H.; D’Onofrio, B.M. ADHD Medication and Substance-Related Problems. Am. J. Psychiatry 2017, 174, 877–885. [Google Scholar] [CrossRef]
- Byun, H.; Yang, J.; Lee, M.; Jang, W.; Yang, J.; Kim, J.; Hong, S.D.; Joung, Y.S.; Yang, J.-W. Psychiatric comorbidity in Korean children and adolescents with attention-deficit hyperactivity disorder: Psychopathology according to subtype. Yonsei Med. J. 2006, 47, 113–121. [Google Scholar] [CrossRef]
- Gaub, M.; Carlson, C.L. Gender differences in ADHD: A meta-analysis and critical review. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 1036–1045. [Google Scholar] [CrossRef]
- Nøvik, T.S.; Hervase, A.; Ralston, S.J.; Dalsgaard, S.; Pereira, R.R.; Lorenzo, M.J. Influence of gender on attention-deficit/hyperactivity disorder in Europe—ADORE. Eur. Child Adolesc. Psychiatry 2006, 15, 15–24. [Google Scholar] [CrossRef]
- Yang, P.; Jong, Y.J.; Chung, L.C.; Chen, C.S. Gender differences in a clinic referred sample of Taiwanese attention-deficit/hyperactivity disorder children. Psychiatry Clin. Neurosci. 2004, 58, 619–623. [Google Scholar] [CrossRef]
- Lau, T.W.I.; Lim, C.G.; Acharryya, S.; Lim-Ashworth, N.; Tan, Y.R.; Fung, S.S.D. Gender differences in externalizing and internalizing problems in Singaporean children and adolescents with attention-deficit/hyperactivity disorder. Child Adolesc. Psychiatry Ment. Health 2021, 15, 3. [Google Scholar] [CrossRef] [PubMed]
- Vingilis, E.; Erickson, P.G.; Toplak, M.E.; Kolla, N.J.; Mann, R.E.; Seeley, J.; vander Maas, M.; Daigle, D.S. Attention Deficit Hyperactivity Disorder Symptoms, Comorbidities, Substance Use, and Social Outcomes among Men and Women in a Canadian Sample. Biomed. Res. Int. 2015, 2015, 982072. [Google Scholar] [CrossRef]
- Dalsgaard, S.; Thorsteinsson, E.; Trabjerg, B.B.; Schullehner, J.; Plana-Ripoll Brikell, I.; Pedersen, C.B. Incidence rates and cumulative incidences of the full spectrum of diagnosed mental disorders in childhood and adolescence. JAMA Psychiatry 2019, 77, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Loyer Carbonneau, M.; Demers, M.; Bigras, M.; Guay, M.C. Meta-Analysis of Sex Differences in ADHD Symptoms and Associated Cognitive Deficits. J. Atten. Disord. 2021, 25, 1640–1656. [Google Scholar] [CrossRef]
- Staller, J.; Faraone, S.V. Attention-deficit hyperactivity disorder in girls: Epidemiology and management. CNS Drugs 2006, 20, 107–123. [Google Scholar] [CrossRef]
- Dalsgaard, S.; Østergaard, S.D.; Leckman, J.F.; Mortensen, P.B.; Pedersen, M.G. Mortality in children, adolescents, and adults with attention deficit hyperactivity disorder: A nationwide cohort study. Lancet 2015, 385, 2190–2196. [Google Scholar] [CrossRef]
- Mahone, E.M. Why fewer females than males are diagnosed with attention-deficit-hyperactivity disorder: It might not be hormones. Dev. Med. Child Neurol. 2010, 52, 790–791. [Google Scholar] [CrossRef]
- Nussbaum, N.L. ADHD and female specific concerns: A review of the literature and clinical implications. J. Attent. Disord. 2012, 16, 87–100. [Google Scholar] [CrossRef] [PubMed]
- Roberts, W.; Milich, R.; Barkley, R.A. Primary symptoms, diagnostic criteria, subtyping, and prevalence of ADHD. In Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment; Barkley, R.A., Ed.; Guilford Press: New York, NY, USA, 2014; pp. 51–80. [Google Scholar]
- Hasson, R.; Fine, J.G. Gender differences among children with ADHD on continuous performance tests: A meta-analytic review. J Atten. Disord. 2012, 16, 190–198. [Google Scholar] [CrossRef]
- Rucklidge, J.J. Gender differences in attention-deficit/hyperactivity disorder. Psychiatr. Clin. N. Am. 2010, 33, 357–373. [Google Scholar] [CrossRef]
- Biederman, J.; Petty, C.R.; Doyle, A.E.; Spencer, T.; Henderson, C.S.; Marion, B.; Fried, R.; Faraone, S.V. Stability of executive function deficits in girls with ADHD: A prospective longitudinal follow-up study into adolescence. Dev. Neuropsychol. 2008, 33, 44–61. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.P.; McBurnett, K.; Hinshaw, S.P.; Pfiffner, L.J. Negative social preference in relation to internalizing symptoms among children with ADHD predominantly inattentive type: Girls fare worse than boys. J. Clin. Child Adolesc. Psychol. 2013, 42, 784–795. [Google Scholar] [CrossRef] [PubMed]
- DuPaul, G.J.; Gormley, M.; Laracy, S.D. Comorbidity of LD and ADHD: Implications of DSM-5 for assessment and treatment. J. Learn Disabil. 2013, 46, 43–51. [Google Scholar] [CrossRef]
- Eme, R. Male adolescent substance use disorder and attention-deficit hyperactivity disorder: A review of the literature. ISRN Addict. 2012, 2013, 815096. [Google Scholar] [CrossRef] [PubMed]
- Breslau, J.; Miller, E.; Joanie Chung, W.J.; Schweitzer, J.B. Childhood and adolescent onset psychiatric disorders, substance use, and failure to graduate high school on time. J. Psychiatr. Res. 2011, 45, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Galéra, C.; Bouvard, M.P.; Encrenaz, G.; Messiah, A.; Fombonne, E. Hyperactivity-inattention symptoms in childhood and suicidal behaviors in adolescence: The youth Gazel cohort. Acta Psychiatr. Scand. 2008, 118, 480–489. [Google Scholar] [CrossRef] [PubMed]
- Ruchkin, V.; Koposov, R.A.; Koyanagi, A.; Stickley, A. Suicidal Behavior in Juvenile Delinquents: The Role of ADHD and Other Comorbid Psychiatric Disorders. Child Psychiatry Hum. Dev. 2017, 48, 691–698. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| (a) | |||||
|---|---|---|---|---|---|
| 1st Author Year | Country | Population | Age | Sample | ADHD Assessment |
| Barbaresi et al., 2006 | USA | School records and medical records (Rochester) | 17 years | N = 379 | DSM-IV |
| Byrd et al., 2013 | USA | Data (NHANES) | 12–15 years | N = 1906 | DISC-IV (DSM-IV criteria) |
| Cole et al., 2008 | USA | Sample obtained from clinics, pediatricians, schools, etc. | 14 years | N = 268 | Interview DICA-R/DICA-IV (DSM-III-R/DSM-IV criteria) |
| Disney et al., 1999 | USA | Minnesota Twin Family Study | 17-years | N = 1252 | DICA-R (Clinical Interview, DSM-III-R) |
| Elkins et al., 2018a | USA | Minnesota Twin Family Study | 14–18 years | N = 2510 | DICA-R, SCID (DSM-IV, and DSM-III-R clinical interviews) |
| Elkins et al. 2018b | USA | Minnesota Twin Family Study participants | 17 years | N = 3762 | DICA–R (DSM-IV) |
| Elkins et al., 2020 | USA | Minnesota Twin Study | 14–17 years | N = 998 | DICA–R (DSM-IV)DSM-5 |
| Gökçe et al., 2017 | Turkey | Hospital for Psychiatry and Neurology, Child and Adolescent Clinic | 11–18 years | N = 156 | SNAP-IV (DSM-IV criteria) |
| Hurtig et al., 2012 | Finland | General population | 16–18 years | N = 273 | SWAN (DSM-IV-TR) |
| Huss et al., 2008 | Germany | Children and adolescents in the KiGGS study | 14–17 years | N = 236 | Clinical interview (physician or professional psychologist) |
| Kessler et al., 2014 | USA | The U.S. National Comorbidity Survey Replication Adolescent Supplement | 13–17 years | N = 6483 | Interview (CIDI) DSM-IV |
| Latimer et al., 2002 | USA | Schools and clinics and mental health and justice centers | 12–19 years | N = 135 | DSM-IV |
| Lee et al., 2015 | USA | National Longitudinal Study of Adolescent to Adult Health | 13 years | N = 9719 | DSM-IV |
| Madsen and Dalsgaard, 2013 | Denmark | Psychiatric and Neurology Centre | 13–18 years | N = 219 | DAWBA (clinical interview) |
| Pineda et al., 1999 | Colombia | Schools in Manizales | 12–17 years | N = 177 | DSM-IV |
| Regan and Tubman, 2020 | USA | Adolescents with ADHD and outpatient treatment for substance use | 12–18 years | N = 394 | Entrevista clínica (UM-CIDI) |
| Rucklidge, 2006 | New Zeland | Participants referred to a specialised psychiatric service | 13–17 years | N = 114 | DSM-IV-TR clinical interview |
| Rucklidge and Tannock, 2001 | Canadá | Deparment of Psychiatry and Hospital for Sick Children | 13–16 years | N = 107 | Clinical interview (DSM-IV) |
| Seidman et al., 2005 | USA | Data provided by two previous studies | 13–17 years | N = 105 | DSM-III, DSM-III-R, DSM-IV, andDSM-IV-TR |
| Selinus et al., 2016 | Suecia | The Child and Adolescent Twin Study in Sweden (CATSS) | 15 years | N = 506 | DSM-IV |
| Yildiz et al., 2020 | Turkey | Hospitalized adolescents (CEMATEM clinic) | Adolescents aged < 18 years | N = 105 | DSM-IV |
| (b) | |||||
| 1st Author Year | Study Type | NOS Quality | |||
| Barbaresi et al., 2006 | Cohort | 8 | |||
| Byrd et al., 2013 | Case-control | 9 | |||
| Cole et al., 2008 | Case-control | 7 | |||
| Disney et al., 1999 | Case-control | 8 | |||
| Elkins et al., 2018a | Cohort | 7 | |||
| Elkins et al., 2018b | Cohort | 7 | |||
| Elkins et al., 2020 | Case-control | 9 | |||
| Gökçe et al., 2017 | Comparative | 5 | |||
| Hurtig et al., 2012 | Case-control | 8 | |||
| Huss et al., 2008 | Case-control | 6 | |||
| Kessler et al., 2014 | Cohort | 9 | |||
| Latimer et al., 2002 | Comparative | 5 | |||
| Lee et al., 2015 | Cohort | 6 | |||
| Madsen and Dalsgaard, 2013 | Case-control | 7 | |||
| Pineda et al.,1999 | Comparative | 8 | |||
| Regan and Tubman, 2020 | Case-control | 9 | |||
| Rucklidge, 2006 | Case-control | 7 | |||
| Rucklidge and Tannock, 2001 | Case-control | 7 | |||
| Seidman et al., 2005 | Case-control | 8 | |||
| Selinus et al., 2016 | Cohort | 8 | |||
| Yildiz et al., 2020 | Comparative | 4 | |||
| Substance Use | Girls/Boys | No Sex Differences |
|---|---|---|
| Nicotine | Adolescent girls with ADHD patients suffered more frequently nicotine use disorder [43,44], with a probability of nicotine use up to 5 times higher than adolescent boys with ADHD [46]. However, white males smoked more throughout adolescence [52]. | |
| Alcohol | Adolescent boys with ADHD and SUD consumed more alcohol, with male sex being a risk factor for these behaviors [60]. However, adolescent girls with more hyperactive–impulsive symptoms consumed more alcohol [45] and suffered more frequently from SUD than boys with ADHD [46,55]. In contrast, boys receiving pharmacological treatment for ADHD consumed less alcohol than those in the control group although this finding was not the same for adolescent girls with and without ADHD [53]. | Adolescent boys and girls with more severe childhood ADHD initiated alcohol use earlier and drank alcohol more frequently, with the risk being similar for both sexes [45,59]. |
| Marijuana and cannabis | Adolescent girls with ADHD had more problems with cannabis [43] and marijuana use than boys with ADHD [44,45]. | Adolescents with more severe childhood ADHD initiated marijuana use earlier and used it more frequently, with the risk being similar for both sexes [45]. |
| Other substances | Adolescent girls with ADHD suffered more SUD on other substances compared to boys with the same disorder [43] and girls without ADHD [59]. In turn, adolescent boys with SUD had more symptoms of ADHD and conduct disorder than female swith SUD [51]. |
| Girls/Boys | No Sex Differences | |
|---|---|---|
| Prevalence | Girls were diagnosed with ADHD less frequently than boys (1 in 43 versus 1 in 10, respectively) [49] and presented fewer symptoms [49,54]. The prevalence of ADHD was lower in girls than in boys [41,50]. | Hyperactive–impulsive type ADHD was most frequent and the combined type was the least frequent in both sexes [54]. |
| Pharmacological therapy | Adolescent girls with ADHD were less likely to receive treatment (18.7%) than boys (28.4%) [40]. |
| Girls/Boys | No Sex Differences | |
|---|---|---|
| Cognitive functioning | Adolescent girls with ADHD scored higher for cognitive impulsivity and motor impulsivity [47]; they made made more errors of omission and had more deficits in design memory, general visual memory, verbal arithmetic skills, and working memory skills [56]; they also had higher processing and encoding speed scores, greater inhibitory control, and lower vocabulary scores than boys with ADHD [57]. Compared to boys, girls with ADHD had a more impaired neuropsychological profile in terms of executive functions [58]. | |
| Academic functioning | ADHD was associated with poor academic performance (course repetitions, low grades, etc.) in both girls and boys [50]. No sex differences were found in any of the WISC-III subtests (block design, digits, symbol search, and arithmetic) [57]. |
| Girls/Boys | No Sex Differences | |
|---|---|---|
| Self-harm, suicidal ideation, and suicidal acts | ADHD was associated with a higher tendency towards suicidal acts, suicidal ideation, and self-harm in girls [48]. However, suicide attempts were significantly higher in boys with ADHD [50]. | The results of the study by Kessler et al. (2014) [50] indicated that suicidal ideation and suicide planning occured at the same rate in adolescent boys and girls with ADHD. |
| Psychological problems | ADHD was associated with more psychological problems, distress, and stress in both sexes [50]. | |
| Motor function development | Both girls with ADHD the control group showed better motor development with age, while boys with ADHD showed minimal improvements [42]. | |
| Obesity | Adolescent boys and girls with ADHD who received medication for the condition showed a lower prevalence of obesity but to a lesser extent in girls [41]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castellano-García, F.; Benito, A.; Jovani, A.; Fuertes-Sáiz, A.; Marí-Sanmillán, M.I.; Haro, G. Sex Differences in Substance Use, Prevalence, Pharmacological Therapy, and Mental Health in Adolescents with Attention-Deficit/Hyperactivity Disorder (ADHD). Brain Sci. 2022, 12, 590. https://doi.org/10.3390/brainsci12050590
Castellano-García F, Benito A, Jovani A, Fuertes-Sáiz A, Marí-Sanmillán MI, Haro G. Sex Differences in Substance Use, Prevalence, Pharmacological Therapy, and Mental Health in Adolescents with Attention-Deficit/Hyperactivity Disorder (ADHD). Brain Sciences. 2022; 12(5):590. https://doi.org/10.3390/brainsci12050590
Chicago/Turabian StyleCastellano-García, Francisca, Ana Benito, Antonio Jovani, Alejandro Fuertes-Sáiz, María Isabel Marí-Sanmillán, and Gonzalo Haro. 2022. "Sex Differences in Substance Use, Prevalence, Pharmacological Therapy, and Mental Health in Adolescents with Attention-Deficit/Hyperactivity Disorder (ADHD)" Brain Sciences 12, no. 5: 590. https://doi.org/10.3390/brainsci12050590
APA StyleCastellano-García, F., Benito, A., Jovani, A., Fuertes-Sáiz, A., Marí-Sanmillán, M. I., & Haro, G. (2022). Sex Differences in Substance Use, Prevalence, Pharmacological Therapy, and Mental Health in Adolescents with Attention-Deficit/Hyperactivity Disorder (ADHD). Brain Sciences, 12(5), 590. https://doi.org/10.3390/brainsci12050590