
Is Interstitial Chemotherapy with Carmustine (BCNU) Wafers Effective against Local Recurrence of Glioblastoma? A Pharmacokinetic Study by Measurement of BCNU in the Tumor Resection Cavity


 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. Measurement of the Concentration of BCNU in the CSF within the Tumor Resection Cavity
2.3. Measurement of Protein Concentration and Number of Cells in the CSF within the Tumor Cavity
2.4. Imaging Studies
2.5. RNA Isolation and Quantitative Real-Time RT-PCR (qRT-PCR)
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
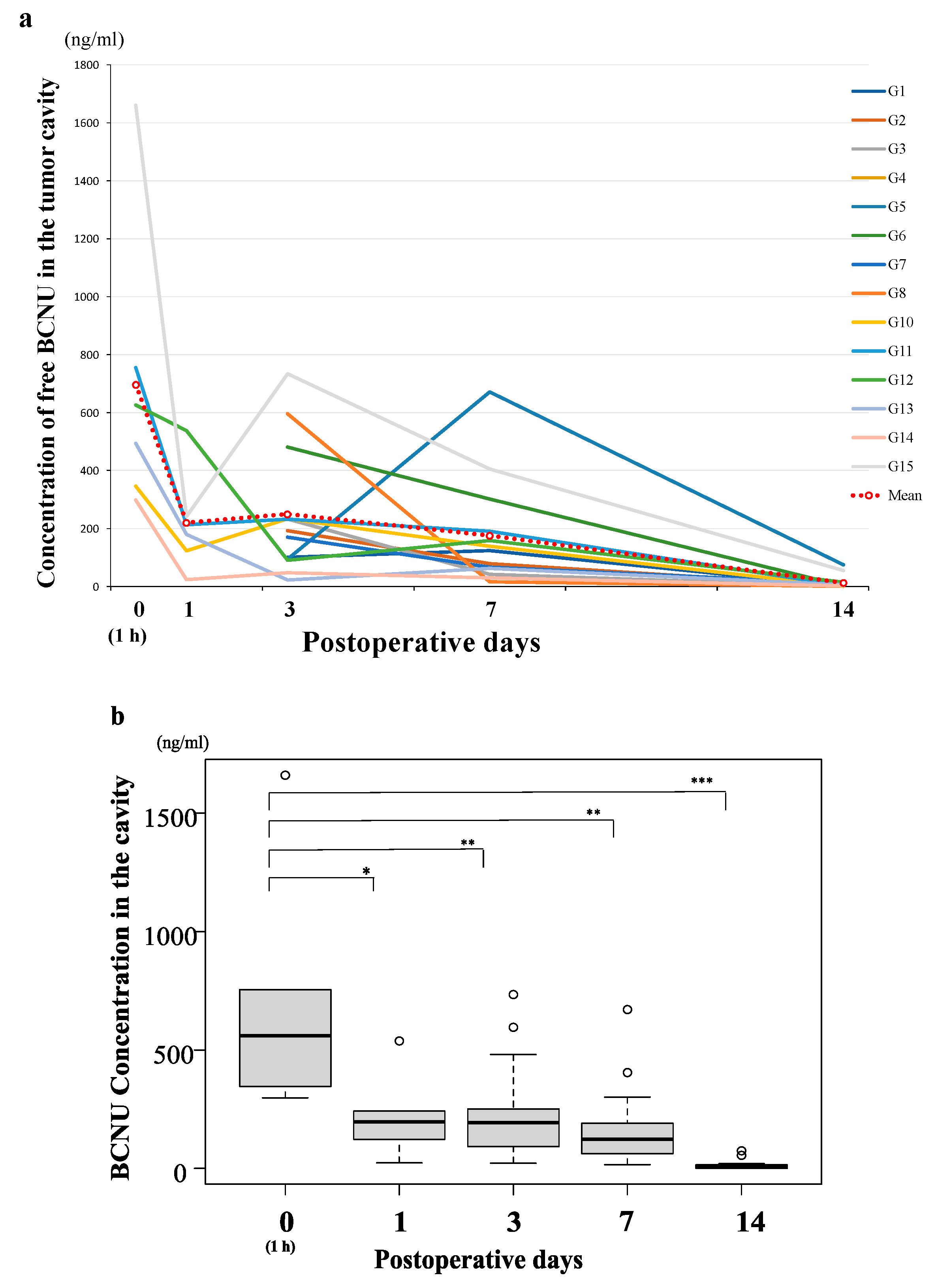
3.2. BCNU Concentration after Implantation of Wafers
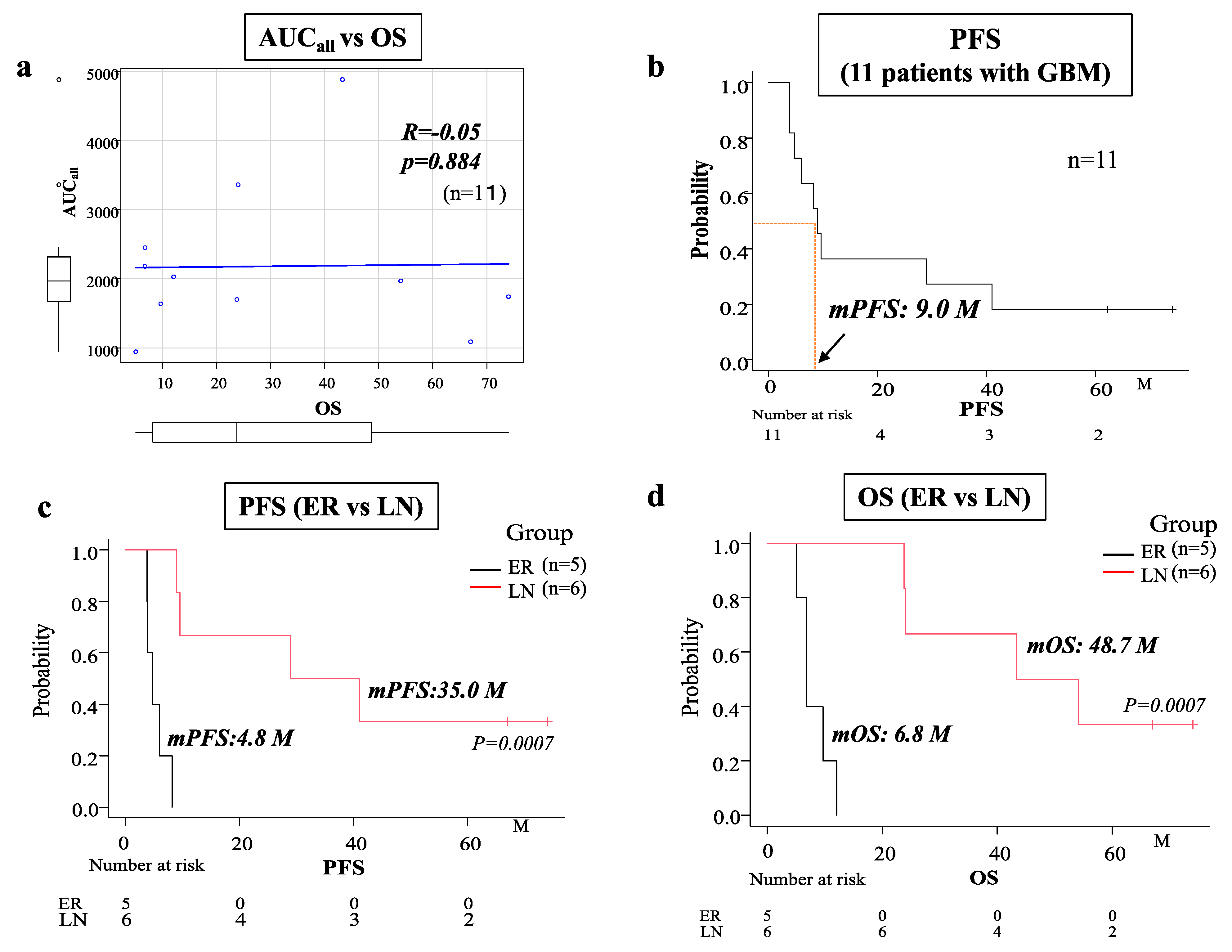
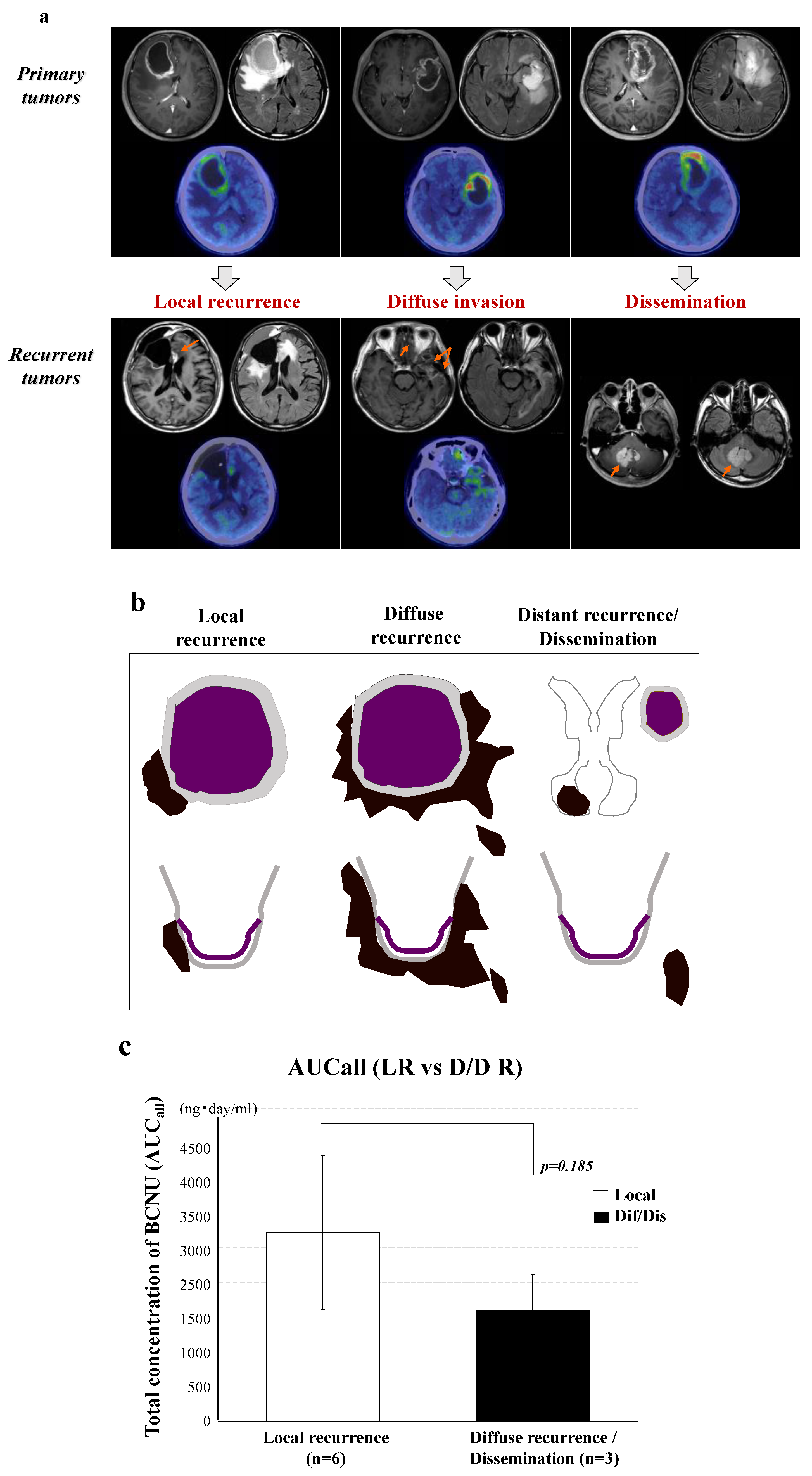
3.3. Calculation of the AUCall and the Relationship between AUCall and Tumor Progression
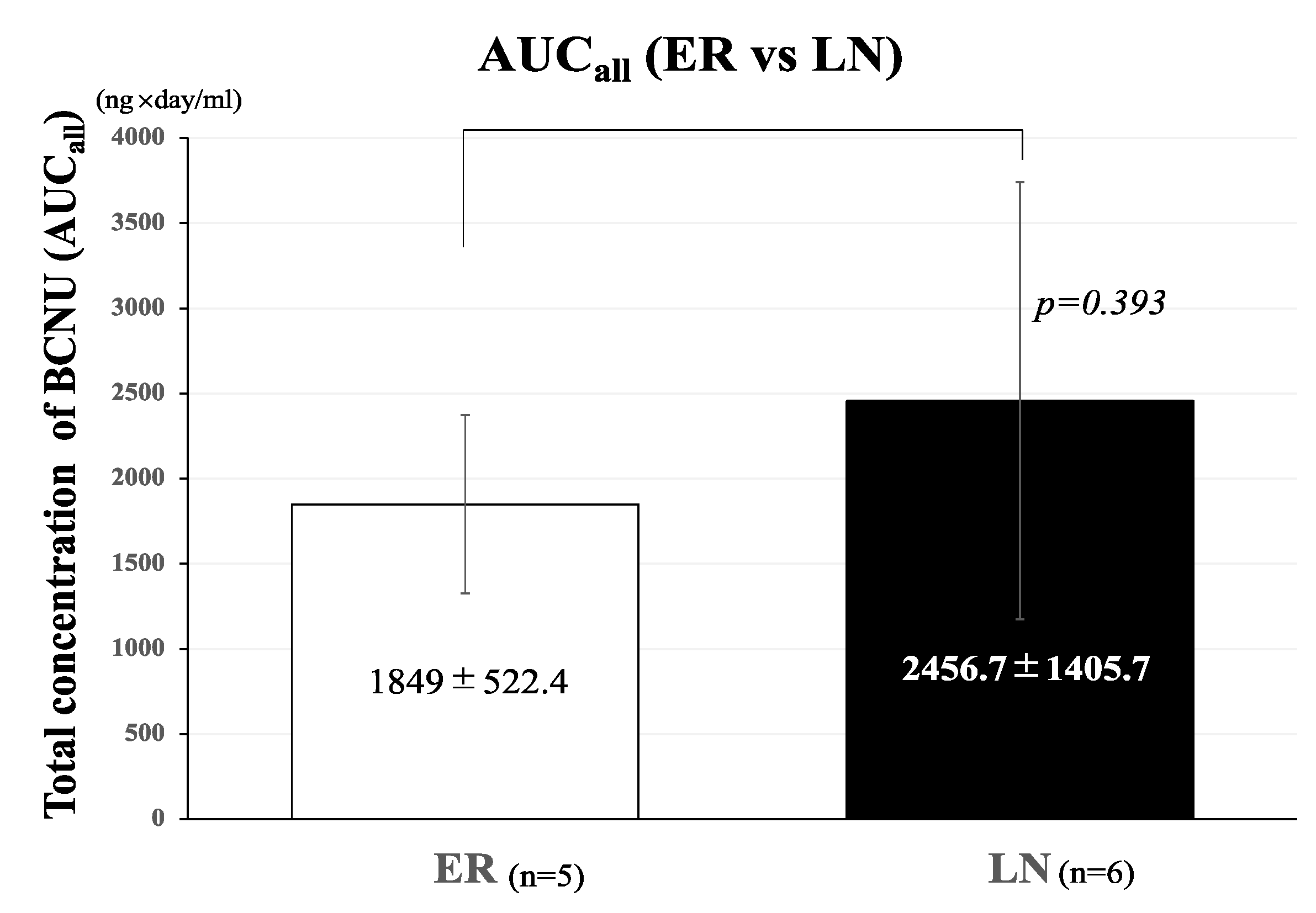
3.4. Relationship between Total BCNU Concentration (AUCall) and Tumor Control
3.5. Imaging Characteristics of the 12 Patients with GBM
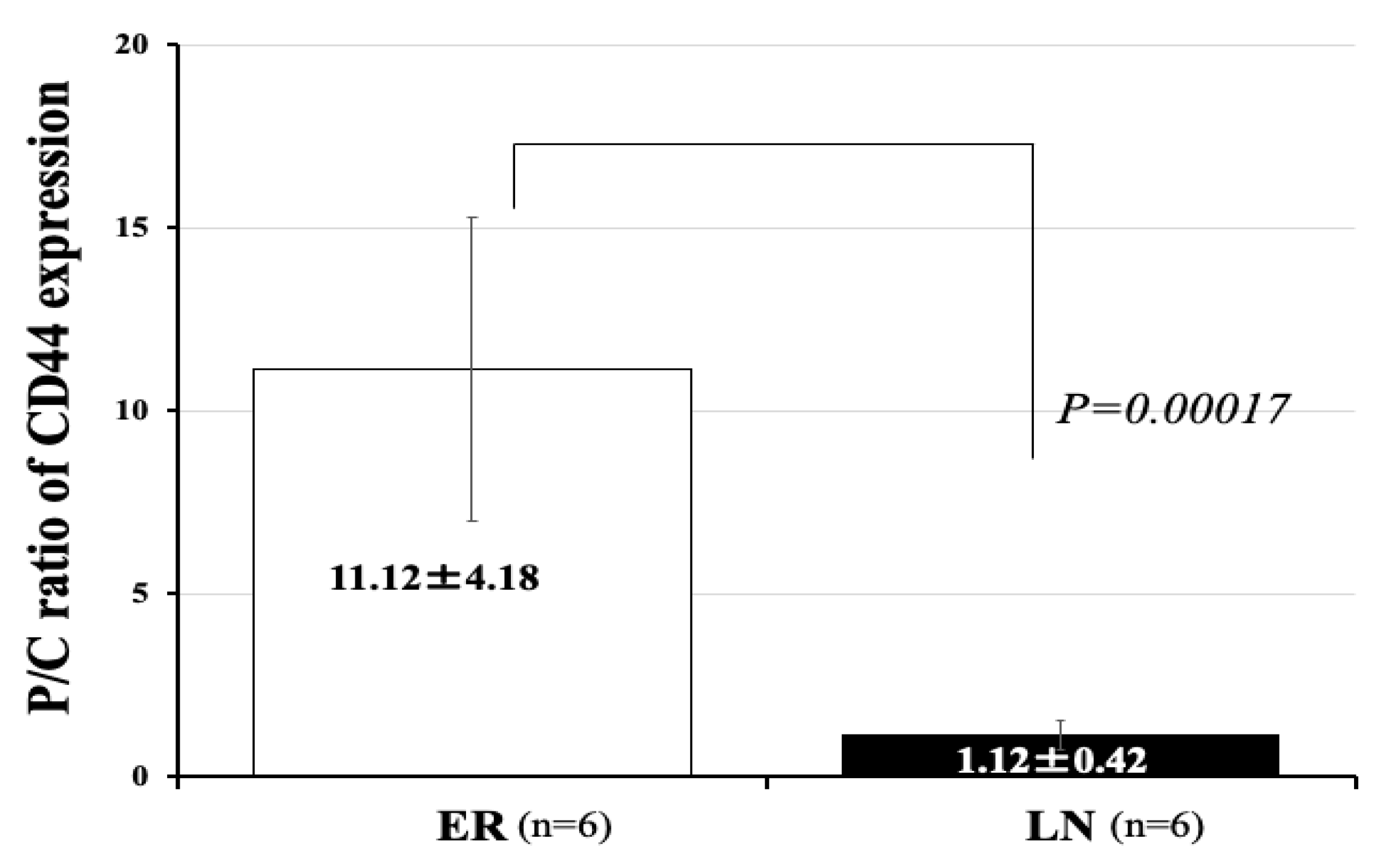
3.6. Expression of mRNA of CD44 in 12 Patients with GBM
3.7. Relationship between the BCNU Concentration and Tumor Recurrence
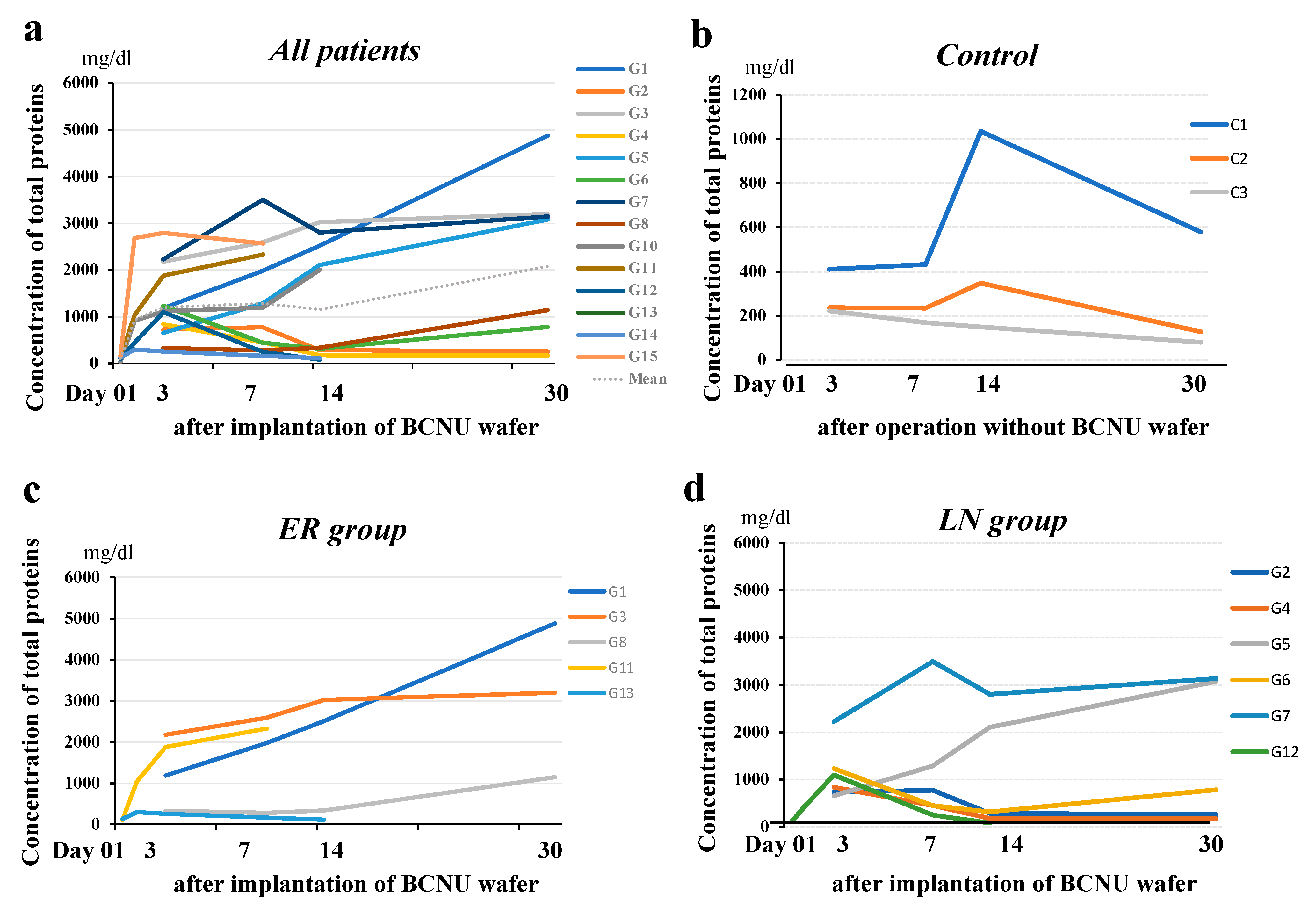
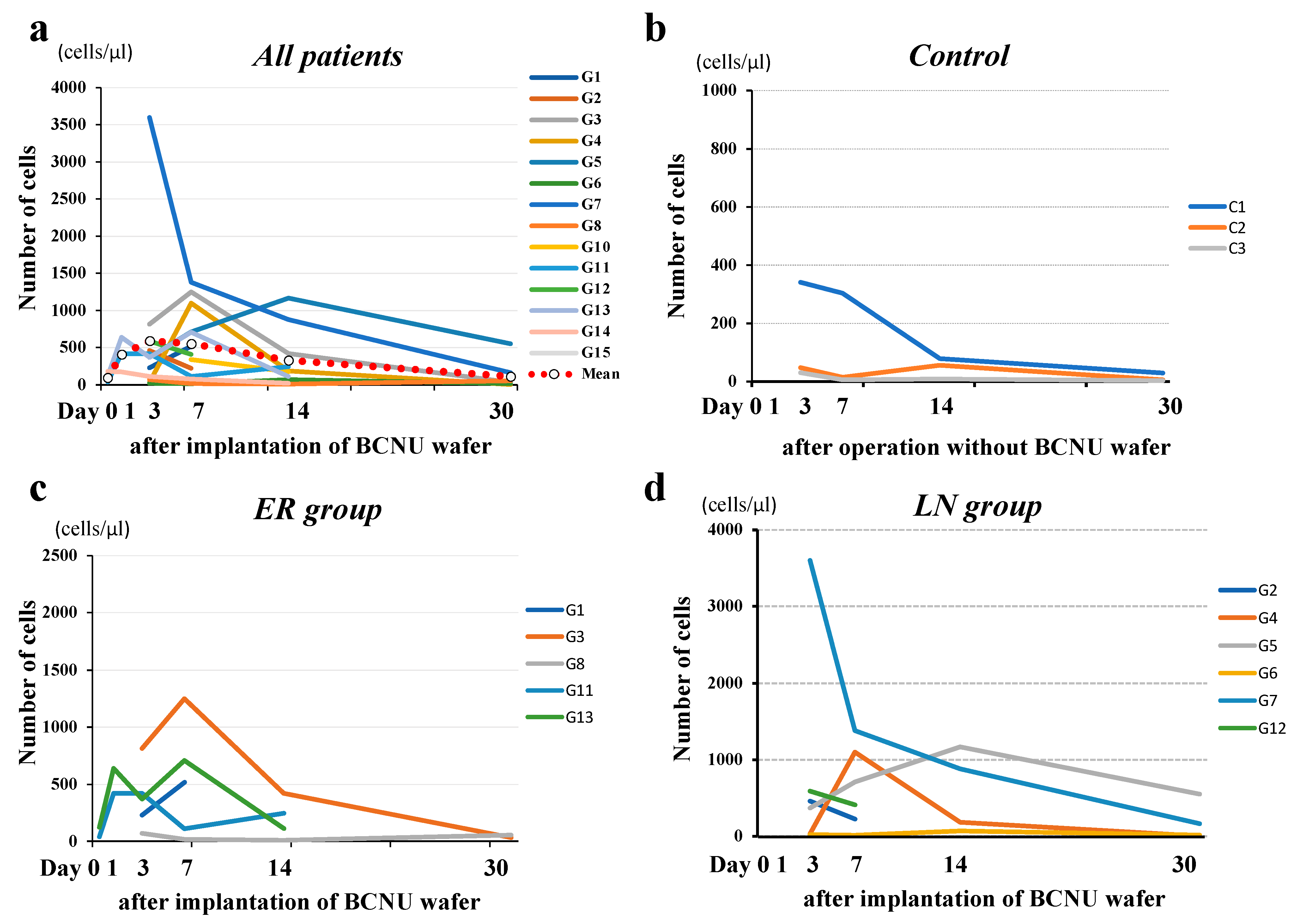
3.8. Time Courses of Protein Concentrations and the Number of Cells in the CSF within the Tumor Cavity in Patients with or without BCNU Wafers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stupp, R.; Hegi, M.E.; Mason, W.P.; van den Bent, M.J.; Taphoorn, M.J.; Janzer, R.C.; Ludwin, S.K.; Allgeier, A.; Fisher, B.; Belanger, K.; et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomized phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009, 10, 459–466. [Google Scholar] [CrossRef]
- GMATG Group. Chemotherapy in adult high-grade glioma: A systematic review and meta-analysis of individual patient data from 12 randomised trials. Lancet 2002, 359, 1011–1018. [Google Scholar] [CrossRef]
- Black, P.M. Brain Tumors. N. Engl. J. Med. 1991, 324, 1555–1564. [Google Scholar] [CrossRef]
- Ohue, S. Using BCNU Wafers in the Treatment of Malignant Gliomas. Jpn. J. Neurosurg. 2016, 25, 882–888. [Google Scholar] [CrossRef][Green Version]
- Attenello, F.J.; Mukherjee, D.; Datoo, G.; McGirt, M.J.; Bohan, E.; Weingart, J.D.; Olivi, A.; Quinones-Hinojosa, A.; Brem, H. Use of Gliadel (BCNU) Wafer in the Surgical Treatment of Malignant Glioma: A 10-Year Institutional Experience. Ann. Surg. Oncol. 2008, 15, 2887–2893. [Google Scholar] [CrossRef]
- Ashby, L.S.; Smith, K.A.; Stea, B. Gliadel wafer implantation combined with standard radiotherapy and concurrent followed by adjuvant temozolomide for treatment of newly diagnosed high-grade glioma: A systematic literature review. World J. Surg. Oncol. 2016, 14, 225. [Google Scholar] [CrossRef]
- Nishikawa, M.; Inoue, A.; Ohnishi, T.; Kohno, S.; Ohue, S.; Matsumoto, S.; Suehiro, S.; Yamashita, D.; Ozaki, S.; Watanabe, H.; et al. Significance of Glioma Stem-Like Cells in the Tumor Periphery That Express High Levels of CD44 in Tumor Invasion, Early Progression, and Poor Prognosis in Glioblastoma. Stem Cells Int. 2018, 2018, 5387041. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, M.; Inoue, A.; Ohnishi, T.; Yano, H.; Kanemura, Y.; Kohno, S.; Ohue, S.; Ozaki, S.; Matsumoto, S.; Suehiro, S.; et al. CD44 expression in the tumor periphery predicts the responsiveness to bevacizumab in the treatment of recurrent glioblastoma. Cancer Med. 2021, 10, 2013–2025. [Google Scholar] [CrossRef] [PubMed]
- Inoue, A.; Nishikawa, M.; Ohnishi, T.; Yano, H.; Kanemura, Y.; Ohtsuka, Y.; Ozaki, S.; Nakamura, Y.; Matsumoto, S.; Suehiro, S.; et al. Prediction of Glioma Stemlike Cell Infiltration in the Non-Contrast-Enhancing Area by Quantitative Measurement of Lactate on Magnetic Resonance Spectroscopy in Glioblastoma. World Neurosurg. 2021, 153, e76–e95. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.B.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef]
- WHO. World Health Organization Classification of Tumours of the Central Nervous System, 5th ed.; Classification of Tumours Editorial Board, Ed.; International Agency for Research on Cancer: Lyon, France, 2021. [Google Scholar]
- Inoue, A.; Ohnishi, T.; Kohno, S.; Ohue, S.; Nishikawa, M.; Suehiro, S.; Matsumoto, S.; Ozaki, S.; Fukushima, M.; Kurata, M.; et al. Met-PET uptake index for total tumor resection: Identification of 11C-methionine uptake index as a goal for total tumor resection including infiltrating tumor cells in glioblastoma. Neurosurg. Rev. 2021, 44, 587–597. [Google Scholar] [CrossRef] [PubMed]
- Okita, Y.; Nonaka, M.; Shofuda, T.; Kanematsu, D.; Yoshioka, E.; Kodama, Y.; Mano, M.; Nakajima, S.; Kanemura, Y. 11C-methinine uptake correlates with MGMT promoter methylation in nonenhancing gliomas. Clin. Neurol. Neurosurg. 2014, 125, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Ohue, S.; Kohno, S.; Inoue, A.; Yamashita, D.; Matsumoto, S.; Suehiro, S.; Kumon, Y.; Kikuchi, K.; Ohnishi, T. Surgical results of tumor resection using tractography-integrated navigation-guided fence-post catheter techniques and motor-evoked potentials for preservation of motor function in patients with glioblastomas near the pyramidal tracts. Neurosurg. Rev. 2015, 38, 293–307. [Google Scholar] [CrossRef] [PubMed]
- Dang, W.; Daviau, T.; Brem, H. Morphological Characterization of Polyanhydride Biodegradable Implant Gliadel® During In Vitro and In Vivo Erosion Using Scanning Electron Microscopy. Pharm. Res. 1996, 13, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Fleming, A.B.; Saltzman, W.M. Pharmacokinetics of the Carmustine Implant. Clin. Pharmacokinet. 2002, 41, 403–419. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Hu, G.; Ouyang, D. A numerical study of the distribution of chemotherapeutic drug carmustine in brain glioblastoma. Drug Deliv. Transl. Res. 2021. [Google Scholar] [CrossRef] [PubMed]
- Aoki, T.; Nishikawa, R.; Sugiyama, K.; Nonoguchi, N.; Kawabata, N.; Mishima, K.; Adachi, J.-I.; Kurisu, K.; Yamasaki, F.; Tominaga, T.; et al. A Multicenter Phase I/II Study of the BCNU Implant (Gliadel® Wafer) for Japanese Patients with Malignant Gliomas. Neurol. Med.-Chir. 2014, 54, 290–301. [Google Scholar] [CrossRef]
- Ohue, S.; Kohno, S.; Inoue, A.; Yamashita, D.; Suehiro, S.; Seno, T.; Kumon, Y.; Kikuchi, K.; Ohnishi, T. Evaluation of serial changes on computed tomography and magnetic resonance imaging after implantation of carmustine wafers in patients with malignant gliomas for differential diagnosis of tumor recurrence. J. Neuro-Oncol. 2016, 126, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Naor, D.; Nedvetzki, S.; Golan, I.; Melnik, L.; Faitelson, Y. CD44 in Cancer. Crit. Rev. Clin. Lab. Sci. 2002, 39, 527–579. [Google Scholar] [CrossRef]
- Chen, C.; Zhao, S.; Karnad, A.; Freeman, J.W. The biology and role of CD44 in cancer progression: Therapeutic implications. J. Hematol. Oncol. 2018, 11, 64. [Google Scholar] [CrossRef] [PubMed]
- Mooney, K.L.; Choy, W.; Sidhu, S.; Pelargos, P.; Bui, T.T.; Voth, B.; Barnette, N.; Yang, I. The role of CD44 in glioblastoma multiforme. J. Clin. Neurosci. 2016, 34, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Si, D.; Yin, F.; Peng, J.; Zhang, G. High Expression of CD44 Predicts a Poor Prognosis in Glioblastomas. Cancer Manag. Res. 2020, 12, 769–775. [Google Scholar] [CrossRef]
- Yan, Y.; Zuo, X.; Wei, D. Concise Review: Emerging Role of CD44 in Cancer Stem Cells: A Promising Biomarker and Therapeutic Target. Stem Cells Transl. Med. 2015, 4, 1033–1043. [Google Scholar] [CrossRef] [PubMed]
- Gaspar, L.E.; Fisher, B.J.; Macdonald, D.R.; Leber, D.V.; Halperin, E.C.; Schold, S.C., Jr.; Cairncross, J.G. Supratentorial malignant glioma: Patterns of recurrence and implications for external beam local treatment. Int. J. Radiat. Oncol. Biol. Phys. 1992, 24, 55–57. [Google Scholar] [CrossRef]
- Oh, J.; Sahgal, A.; Sanghera, P.; Tsao, M.N.; Davey, P.; Lam, K.; Symons, S.; Aviv, R.; Perry, J.R. Glioblastoma: Patterns of Recurrence and Efficacy of Salvage Treatments. Can. J. Neurol. Sci. 2011, 38, 621–625. [Google Scholar] [CrossRef] [PubMed]
- Giese, A.; Kucinski, T.; Knopp, U.; Goldbrunner, R.; Hamel, W.; Mehdorn, H.M.; Tonn, J.C.; Hilt, D.; Westphal, M. Pattern of Recurrence following Local Chemotherapy with Biodegradable Carmustine (BCNU) Implants in Patients with Glioblastoma. J. Neuro-Oncol. 2004, 66, 351–360. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | KPS | Methylation of | Recurrence | Outcome | BCNU (AUCall) (ng × | Phenotype on | CD44 Expression (mRNA) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. | Age/Sex | (%) | Histology | MGMT | EOR | Rec PFS (M) | D/A | OS (M) | day/mL) | MRI/PET | Core | Periphery P/C Ratio | ||
| G1 | 67/M | 70 | GBM | + | GTR | + | 8.2 | D | 12.1 | 2030 | HI | 1 | 16.3 | 15.9 |
| G2 | 64/F | 90 | GBM | − | GTR | − | 74 | A | 74 | 1740 | LI | 2.7 | 5.3 | 1.9 |
| G3 | 71/M | 90 | GBM | − | GTR | + | 6 | D | 9.7 | 1640 | HI | 1.1 | 19.2 | 16.8 |
| G4 | 63/F | 80 | GBM | − | GTR | + | 41 | D | 54.1 | 1970 | LI | 55.2 | 69.1 | 1.3 |
| G5 | 79/F | 70 | GBM | − | PR | + | 29 | D | 43.3 | 4880 | LI | 2.8 | 2.7 | 1 |
| G6 | 30/M | 70 | GBM | − | GTR | + | 9.6 | D | 24 | 3360 | LI | 2.8 | 2.1 | 0.8 |
| G7 | 65/F | 70 | GBM | + | GTR | − | 67 | A | 67 | 1090 | LI | 2.9 | 2.8 | 1 |
| G8 | 67/M | 60 | GBM | + | STR | + | 3.8 | D | 6.8 | 2180 | HI | 1.6 | 13 | 8.2 |
| G9 | 86/M | 80 | GBM | + | GTR | + | 2.4 | D | 2.4 | 2970 | HI | 4.1 | 30.8 | 7.5 |
| G10 | 45/M | 90 | AMG3 | − | STR | − | 62.1 | A | 62.1 | 1820 | na | 1 | 1 | 1 |
| G11 | 71/F | 80 | GBM | − | GTR | + | 4.8 | D | 6.8 | 2450 | HI | 3.1 | 25 | 8 |
| G12 | 65/M | 70 | GBM | + | STR | + | 9 | D | 23.8 | 1700 | LI | 3.3 | 3.1 | 0.9 |
| G13 | 66/M | 70 | GBM | − | GTR | + | 3.9 | D | 5.1 | 945 | HI | 4 | 41.2 | 10.4 |
| G14 | 30/M | 70 | AMG3 | − | PR | − | 58 | A | 58 | 491 | na | 0.8 | 0.7 | 0.9 |
| G15 | 35/F | 90 | AMG3 | + | GTR | − | 57 | A | 57 | 5810 | na | 0.9 | 0.8 | 0.9 |
| Patients without Gliadel (control) | ||||||||||||||
| C1 | 59/M | 70 | GBM | + | PR | − | 2.6 | D | 8.3 | na | ||||
| C2 | 72/M | 90 | AMG3 | − | GTR | − | 30.4 | A | 30.4 | na | ||||
| C3 | 64/F | 80 | GBM | + | GTR | + | 7.4 | D | 23.5 | na | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ohnishi, T.; Yamashita, D.; Inoue, A.; Suehiro, S.; Ohue, S.; Kunieda, T. Is Interstitial Chemotherapy with Carmustine (BCNU) Wafers Effective against Local Recurrence of Glioblastoma? A Pharmacokinetic Study by Measurement of BCNU in the Tumor Resection Cavity. Brain Sci. 2022, 12, 567. https://doi.org/10.3390/brainsci12050567
Ohnishi T, Yamashita D, Inoue A, Suehiro S, Ohue S, Kunieda T. Is Interstitial Chemotherapy with Carmustine (BCNU) Wafers Effective against Local Recurrence of Glioblastoma? A Pharmacokinetic Study by Measurement of BCNU in the Tumor Resection Cavity. Brain Sciences. 2022; 12(5):567. https://doi.org/10.3390/brainsci12050567
Chicago/Turabian StyleOhnishi, Takanori, Daisuke Yamashita, Akihiro Inoue, Satoshi Suehiro, Shiro Ohue, and Takeharu Kunieda. 2022. "Is Interstitial Chemotherapy with Carmustine (BCNU) Wafers Effective against Local Recurrence of Glioblastoma? A Pharmacokinetic Study by Measurement of BCNU in the Tumor Resection Cavity" Brain Sciences 12, no. 5: 567. https://doi.org/10.3390/brainsci12050567
APA StyleOhnishi, T., Yamashita, D., Inoue, A., Suehiro, S., Ohue, S., & Kunieda, T. (2022). Is Interstitial Chemotherapy with Carmustine (BCNU) Wafers Effective against Local Recurrence of Glioblastoma? A Pharmacokinetic Study by Measurement of BCNU in the Tumor Resection Cavity. Brain Sciences, 12(5), 567. https://doi.org/10.3390/brainsci12050567