
Autoimmune Vestibulopathy—A Case Series




Abstract
1. Introduction
2. Cases
2.1. A: Case 1
2.2. B: Case 1—Discussion
2.3. A: Case 2
2.4. B: Case 2—Discussion
2.5. A: Case 3
2.6. B: Case 3—Discussion
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McCabe, B.F. Autoimmune sensorineural hearing loss. 1979. Ann. Otol. Rhinol. Laryngol. 2004, 113, 526–530. [Google Scholar] [CrossRef] [PubMed]
- Ciorba, A.; Corazzi, V.; Bianchini, C.; Aimoni, C.; Pelucchi, S.; Skarżyński, P.H.; Hatzopoulos, S. Autoimmune inner ear disease (AIED): A diagnostic challenge. Int. J. Immunopathol. Pharmacol. 2018, 32. [Google Scholar] [CrossRef] [PubMed]
- Goodall, A.F.; Siddiq, M.A. Current understanding of the pathogenesis of autoimmune inner ear disease: A review. Clin. Otolaryngol. 2015, 40, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Mijovic, T.; Zeitouni, A.; Colmegna, I. Autoimmune sensorineural hearing loss: The otology-rheumatology interface. Rheumatology 2013, 52, 780–789. [Google Scholar] [CrossRef] [PubMed]
- Bovo, R.; Ciorba, A.; Martini, A. The diagnosis of autoimmune inner ear disease: Evidence and critical pitfalls. Eur. Arch. Oto-RhinoLaryngol. 2009, 266, 37–40. [Google Scholar] [CrossRef] [PubMed]
- Agrup, C.; Luxon, L.M. Immune-mediated inner-ear disorders in neuro-otology. Curr. Opin. Neurol. 2006, 19, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.P.; Weisman, M.H.; Derebery, J.M.; Espeland, M.A.; Gantz, B.J.; Gulya, A.J.; Hammerschlag, P.E.; Hannley, M.; Hughes, G.B.; Moscicki, R.; et al. Treatment of corticosteroid-responsive autoimmune inner ear disease with methotrexate: A randomized controlled trial. JAMA 2003, 290, 1875–1883. [Google Scholar] [CrossRef]
- García-Berrocal, J.R.; Trinidad, A.; Ramírez-Camacho, R.; Lobo, D.; Verdaguer, M.; Ibáñez, A. Immunologic work-up study for inner ear disorders: Looking for a rational strategy. Acta Otolaryngol. 2005, 125, 814–818. [Google Scholar] [CrossRef]
- Campbell, K.C.; Klemens, J.J. Sudden hearing loss and autoimmune inner ear disease. J. Am. Acad. Audiol. 2000, 11, 361–367. [Google Scholar]
- Mancini, P.; Atturo, F.; Di Mario, A.; Portanova, G.; Ralli, M.; De Virgilio, A.; de Vincentiis, M.; Greco, A. Hearing loss in autoimmune disorders: Prevalence and therapeutic options. Autoimmun. Rev. 2018, 17, 644–652. [Google Scholar] [CrossRef]
- Ralli, M.; D’Aguanno, V.; Di Stadio, A.; De Virgilio, A.; Croce, A.; Longo, L.; Greco, A.; de Vincentiis, M. Audiovestibular Symptoms in Systemic Autoimmune Diseases. J. Immunol. Res. 2018, 2018, 5798103. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.P.; Sharp, P.A. Inner ear autoantibodies in patients with rapidly progressive sensorineural hearing loss. Laryngoscope 1990, 100, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Matsuoka, A.J.; Harris, J.P. Autoimmune inner ear disease: A retrospective review of forty-seven patients. Audiol. Neurootol. 2013, 18, 228–239. [Google Scholar] [CrossRef] [PubMed]
- Ianuale, C.; Cadoni, G.; De Feo, E.; Liberati, L.; Simo, R.K.; Paludetti, G.; Ricciardi, W.; Boccia, S. A systematic review and meta-analysis of the diagnostic accuracy of anti-heat shock protein 70 antibodies for the detection of autoimmune hearing loss. Otol. Neurotol. 2013, 34, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.O.; Billings, P.B.; Keithley, E.M.; Harris, J.P. Comparison of anti-heat shock protein 70 (anti-hsp70) and anti-68-kDa inner ear protein in the sera of patients with Meniere’s disease. Laryngoscope 1997, 107, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Gottschlich, S.; Billings, P.B.; Keithley, E.M.; Weisman, M.H.; Harris, J.P. Assessment of serum antibodies in patients with rapidly progressive sensorineural hearing loss and Menière’s disease. Laryngoscope 1995, 105, 1347–1352. [Google Scholar] [CrossRef] [PubMed]
- Brant, J.A.; Eliades, S.J.; Ruckstein, M.J. Systematic review of treatments for autoimmune inner ear disease. Otol. Neurotol. 2015, 36, 1585–1592. [Google Scholar] [CrossRef]
- Girasoli, L.; Cazzador, D.; Padoan, R.; Nardello, E.; Felicetti, M.; Zanoletti, E.; Schiavon, F.; Bovo, R. Update on Vertigo in Autoimmune Disorders, from Diagnosis to Treatment. J. Immunol. Res. 2018, 2018, 5072582. [Google Scholar] [CrossRef]
- Russo, F.Y.; Ralli, M.; De Seta, D.; Mancini, P.; Lambiase, A.; Artico, M.; de Vincentiis, M.; Greco, A. Autoimmune vertigo: An update on vestibular disorders associated with autoimmune mechanisms. Immunol. Res. 2018, 66, 675–685. [Google Scholar] [CrossRef]
- McGarvie, L.A.; MacDougall, H.G.; Halmagyi, G.M.; Burgess, A.M.; Weber, K.P.; Curthoys, I.S. The Video Head Impulse Test (vHIT) of Semicircular Canal Function—Age-Dependent Normative Values of VOR Gain in Healthy Subjects. Front. Neurol. 2015, 6, 154. [Google Scholar] [CrossRef]
- Sepahdari, A.R.; Ishiyama, G.; Vorasubin, N.; Peng, K.A.; Linetsky, M.; Ishiyama, A. Delayed intravenous contrast-enhanced 3D FLAIR MRI in Meniere’s disease: Correlation of quantitative measures of endolymphatic hydrops with hearing. Clin. Imaging 2015, 39, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Baráth, K.; Schuknecht, B.; Naldi, A.M.; Schrepfer, T.; Bockisch, C.J.; Hegemann, S.C. Detection and grading of endolymphatic hydrops in Menière disease using MR imaging. AJNR Am. J. Neuroradiol. 2014, 35, 1387–1392. [Google Scholar] [CrossRef] [PubMed]
- Balaban, C. Mechanisms of Vestibular Compensation: An Overview. J. Korean Balance Soc. 2006, 5, 139–148. [Google Scholar]
- Fishman, J.M.; Burgess, C.; Waddell, A. Corticosteroids for the treatment of idiopathic acute vestibular dysfunction (vestibular neuritis). Cochrane Database Syst. Rev. 2011, 11, CD008607. [Google Scholar] [CrossRef] [PubMed]
- Goudakos, J.K.; Markou, K.D.; Franco-Vidal, V.; Vital, V.; Tsaligopoulos, M.; Darrouzet, V. Corticosteroids in the treatment of vestibular neuritis: A systematic review and meta-analysis. Otol. Neurotol. 2010, 31, 183–189. [Google Scholar] [CrossRef]
- Batuecas-Caletrío, A.; Yañez-Gonzalez, R.; Sanchez-Blanco, C.; Pérez, P.B.; González-Sanchez, E.; Sanchez, L.A.; Kaski, D. Glucocorticoids improve acute dizziness symptoms following acute unilateral vestibulopathy. J. Neurol. 2015, 262, 2578–2582. [Google Scholar] [CrossRef] [PubMed]
- Frejo, L.; Soto-Varela, A.; Santos-Perez, S.; Aran, I.; Batuecas-Caletrio, A.; Perez-Guillen, V.; Perez-Garrigues, H.; Fraile, J.; Martin-Sanz, E.; Tapia, M.C.; et al. Clinical Subgroups in Bilateral Meniere Disease. Front. Neurol. 2016, 7, 182. [Google Scholar] [CrossRef]
- Biscetti, L.; De Vanna, G.; Cresta, E.; Corbelli, I.; Gaetani, L.; Cupini, L.; Calabresi, P.; Sarchielli, P. Headache and immunological/autoimmune disorders: A comprehensive review of available epidemiological evidence with insights on potential underlying mechanisms. J. Neuroinflamm. 2021, 18, 259. [Google Scholar] [CrossRef]
- Cavestro, C.; Ferrero, M. Migraine in Systemic Autoimmune Diseases. Endocr. Metab. Immune Disord. Drug Targets 2018, 18, 124–134. [Google Scholar] [CrossRef]
- D’Aguanno, V.; Ralli, M.; de Vincentiis, M.; Greco, A. Optimal management of Cogan’s syndrome: A multidisciplinary approach. J. Multidiscip. Healthc. 2017, 11, 1–11. [Google Scholar] [CrossRef]
- Shamriz, O.; Tal, Y.; Gross, M. Autoimmune Inner Ear Disease: Immune Biomarkers, Audiovestibular Aspects, and Therapeutic Modalities of Cogan’s Syndrome. J. Immunol. Res. 2018, 2018, 1498640. [Google Scholar] [CrossRef]
- Greco, A.; Gallo, A.; Fusconi, M.; Magliulo, G.; Turchetta, R.; Marinelli, C.; Macri, G.F.; De Virgilio, A.; de Vincentiis, M. Cogan’s syndrome: An autoimmune inner ear disease. Autoimmun. Rev. 2013, 12, 396–400. [Google Scholar] [CrossRef]
- Padoan, R.; Cazzador, D.; Pendolino, A.L.; Felicetti, M.; De Pascalis, S.; Zanoletti, E.; Bovo, R.; Martini, A.; Schiavon, F. Cogan’s syndrome: New therapeutic approaches in the biological era. Expert Opin. Biol. Ther. 2019, 19, 781–788. [Google Scholar] [CrossRef] [PubMed]
- Van de Berg, R.; van Tilburg, M.; Kingma, H. Bilateral Vestibular Hypofunction: Challenges in Establishing the Diagnosis in Adults. ORL J. Otorhinolaryngol. Relat. Spec. 2015, 77, 197–218. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Oh, Y.M.; Koo, J.W.; Kim, J.S. Bilateral vestibulopathy: Clinical characteristics and diagnostic criteria. Otol. Neurotol. 2011, 32, 812–817. [Google Scholar] [CrossRef]
- Espinoza, G.M.; Wheeler, J.; Temprano, K.K.; Keller, A.P. Cogan’s Syndrome: Clinical Presentations and Update on Treatment. Curr. Allergy Asthma Rep. 2020, 20, 46. [Google Scholar] [CrossRef] [PubMed]
- Grasland, A.; Pouchot, J.; Hachulla, E.; Blétry, O.; Papo, T.; Vinceneux, P. Study Group for Cogan’s Syndrome. Typical and atypical Cogan’s syndrome: 32 cases and review of the literature. Rheumatology 2004, 43, 1007–1015. [Google Scholar] [CrossRef] [PubMed]
- Pollard, Z.F.; Greenberg, M.; Bashinsky, A.; Bordenca, M. Uveitis associated with atypical cogan syndrome in children. Arch. Ophthalmol. 2007, 125, 1574–1575. [Google Scholar] [CrossRef]
- Morgan, R.F.; Baumgartner, C.J. Ménière’s disease complicated by recurrent interstitial keratitis: Excellent result following cervical ganglionectomy. West. J. Surg. 1934, 42, 628–631. [Google Scholar]
- Tayer-Shifman, O.E.; Ilan, O.; Tovi, H.; Tal, Y. Cogan’s syndrome--clinical guidelines and novel therapeutic approaches. Clin. Rev. Allergy Immunol. 2014, 47, 65–72. [Google Scholar] [CrossRef]
- Durtette, C.; Hachulla, E.; Resche-Rigon, M.; Papo, T.; Zénone, T.; Lioger, B.; Deligny, C.; Lambert, M.; Landron, C.; Pouchot, J.; et al. Cogan syndrome: Characteristics, outcome and treatment in a French nationwide retrospective study and literature review. Autoimmun. Rev. 2017, 16, 1219–1223. [Google Scholar] [CrossRef] [PubMed]
- Medicines & Healthcare Products Regulatory Agency. Coronavirus Vaccine–Weekly Summary of Yellow Card Reporting. Medicines & Healthcare Products Regulatory Agency. 2021. Available online: https://www.gov.uk/government/publications/coronavirus-covid-19-vaccine-adverse-reactions/coronavirus-vaccine-summary-of-yellow-card-reporting (accessed on 10 December 2021).
- Fathy, R.A.; McMahon, D.E.; Le e, C.; Chamberlin, G.C.; Rosenbach, M.; Lipoff, J.B.; Tyagi, A.; Desai, S.R.; French, L.E.; Lim, H.W.; et al. Varicella-zoster and herpes simplex virus reactivation post-COVID-19 vaccination: A review of 40 cases in an International Dermatology Registry. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e6–e9. [Google Scholar] [CrossRef] [PubMed]
- Xu, R.; Zhou, Y.; Cai, L.; Wang, L.; Han, J.; Yang, X.; Chen, J.; Chen, J.; Ma, C.; Shen, L. Co-reactivation of the human herpesvirus alpha subfamily (herpes simplex virus-1 and varicella zoster virus) in a critically ill patient with COVID-19. Br. J. Dermatol. 2020, 183, 1145–1147. [Google Scholar] [CrossRef]
- Maldonado, M.D.; Romero-Aibar, J.; Pérez-San-Gregorio, M.A. COVID-19 pandemic as a risk factor for the reactivation of herpes viruses. Epidemiol Infect. 2021, 149, e145. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J. Vestibular neuritis after COVID-19 vaccination. Hum. Vaccin. Immunother. 2021, 13, 1–3. [Google Scholar] [CrossRef]
- Malayala, S.V.; Raza, A. A Case of COVID-19-Induced Vestibular Neuritis. Cureus 2020, 12, e8918. [Google Scholar] [CrossRef] [PubMed]
- Vanaparthy, R.; Malayala, S.V.; Balla, M. COVID-19-Induced Vestibular Neuritis, Hemi-Facial Spasms and Raynaud’s Phenomenon: A Case Report. Cureus 2020, 12, e11752. [Google Scholar] [CrossRef]
- Giannantonio, S.; Scorpecci, A.; Montemurri, B.; Marsella, P. Case of COVID-19-induced vestibular neuritis in a child. BMJ Case Rep. 2021, 14, e242978. [Google Scholar] [CrossRef]
- Mat, Q.; Noël, A.; Loiselet, L.; Tainmont, S.; Chiesa-Estomba, C.M.; Lechien, J.R.; Duterme, J.P. Vestibular Neuritis as Clinical Presentation of COVID-19. Ear Nose Throat J. 2021, 11, 145561321995021. [Google Scholar] [CrossRef]
- Halalau, A.; Halalau, M.; Carpenter, C.; Abbas, A.E.; Sims, M. Vestibular neuritis caused by severe acute respiratory syndrome coronavirus 2 infection diagnosed by serology: Case report. SAGE Open Med. Case Rep. 2021, 9. [Google Scholar] [CrossRef]
- Ahmed, M.U.; Hanif, M.; Ali, M.J.; Haider, M.A.; Kherani, D.; Memon, G.M.; Karim, A.H.; Sattar, A. Neurological Manifestations of COVID-19 (SARS-CoV-2): A Review. Front. Neurol. 2020, 11, 518. [Google Scholar] [CrossRef] [PubMed]
- Segal, Y.; Shoenfeld, Y. Vaccine-induced autoimmunity: The role of molecular mimicry and immune crossreaction. Cell. Mol. Immunol. 2018, 15, 586–594. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Xu, Z.; Wang, P.; Li, X.M.; Shuai, Z.W.; Ye, D.Q.; Pan, H.F. New-onset autoimmune phenomena post COVID-19 vaccination. Immunology 2021. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Rojas, M.; Restrepo-Jiménez, P.; Monsalve, D.M.; Pacheco, Y.; Acosta-Ampudia, Y.; Ramírez-Santana, C.; Leung, P.S.C.; Ansari, A.A.; Gershwin, M.E.; Anaya, J.M. Molecular mimicry and autoimmunity. J. Autoimmun. 2018, 95, 100–123. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Peng, Y.; Xu, H.; Cui, Z.; Williams, R.O., 3rd. The COVID-19 Vaccine Race: Challenges and Opportunities in Vaccine Formulation. AAPS PharmSciTech 2020, 21, 225. [Google Scholar] [CrossRef] [PubMed]
- Soy, M.; Keser, G.; Atagunduz, P.; Mutlu, M.Y.; Gunduz, A.; Koybaşi, G.; Bes, C. A practical approach for vaccinations including COVID-19 in autoimmune/autoinflammatory rheumatic diseases: A non-systematic review. Clin. Rheumatol. 2021, 40, 3533–3545. [Google Scholar] [CrossRef]
- Garg, R.K.; Paliwal, V.K. Spectrum of neurological complications following COVID-19 vaccination. Neurol. Sci. 2021, 43, 1–38. [Google Scholar] [CrossRef]
- Shimizu, M.; Ogaki, K.; Nakamura, R.; Kado, E.; Nakajima, S.; Kurita, N.; Watanabe, M.; Yamashiro, K.; Hattori, N.; Urabe, T. An 88-year-old woman with acute disseminated encephalomyelitis following messenger ribonucleic acid-based COVID-19 vaccination. eNeurologicalSci 2021, 25, 100381. [Google Scholar] [CrossRef]
- Rinaldi, V.; Bellucci, G.; Romano, A.; Bozzao, A.; Salvetti, M. ADEM after ChAdOx1 nCoV-19 vaccine: A case report. Mult. Scler. 2021, 30. [Google Scholar] [CrossRef]
- Ciodaro, F.; Freni, F.; Alberti, G.; Forelli, M.; Gazia, F.; Bruno, R.; Sherdell, E.P.; Galletti, B.; Galletti, F. Application of Cervical Vestibular-Evoked Myogenic Potentials in Adults with Moderate to Profound Sensorineural Hearing Loss: A Preliminary Study. Int. Arch. Otorhinolaryngol. 2020, 24, e5–e10. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. National Library of Medicine (USA). Risk Factors for the Development of Bilateral Ménière’s Disease and the Establishment of a National Ménière’s Disease Registry. 2020. Available online: https://clinicaltrials.gov/ct2/show/NCT04438538 (accessed on 30 January 2022).
- ACCORD Collaborators. ACCORD: A Multicentre, Seamless, Phase 2 Adaptive Randomisation Platform Study to Assess the Efficacy and Safety of Multiple Candidate Agents for the Treatment of COVID-19 in Hospitalised Patients: A structured summary of a study protocol for a randomised controlled trial. Trials 2020, 21, 691. [Google Scholar] [CrossRef]
- Naganawa, S.; Nakashima, T. Visualization of endolymphatic hydrops with MR imaging in patients with Ménière’s disease and related pathologies: Current status of its methods and clinical significance. Jpn. J. Radiol. 2014, 32, 191–204. [Google Scholar] [CrossRef] [PubMed]
- Conte, G.; Lo Russo, F.M.; Calloni, S.F.; Sina, C.; Barozzi, S.; Di Berardino, F.; Scola, E.; Palumbo, G.; Zanetti, D.; Triulzi, F.M. MR imaging of endolymphatic hydrops in Ménière’s disease: Not all that glitters is gold. Acta Otorhinolaryngol. Ital. 2018, 38, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Lobo, D.; Tuñón, M.; Villarreal, I.; Brea, B.; García-Berrocal, J.R. Intratympanic gadolinium magnetic resonance imaging supports the role of endolymphatic hydrops in the pathogenesis of immune-mediated inner-ear disease. J. Laryngol. Otol. 2018, 132, 554–559. [Google Scholar] [CrossRef]
- Hida, K.; Takano, K.; Yoshimitsu, K.; Fukae, J.; Hokao, K. Inner ear enhancement on gadolinium-enhanced 3D FLAIR images in a patient with Vogt-Koyanagi-Harada disease. BJR Case Rep. 2016, 3, 20160090. [Google Scholar] [CrossRef]
- National Institute for Health Research. The STARFISH Trial: A randomised Controlled Trial of STeroid Administration Routes for Idiopathic Sudden Sensorineural Hearing Loss. (NIHR Award ID: NIHR131528). 2021. Available online: https://fundingawards.nihr.ac.uk/award/NIHR131528 (accessed on 30 January 2022).
- Lee, J.; Biggs, K.; Muzaffar, J.; Bance, M.; Monksfield, P. Hearing loss in inner ear and systemic autoimmune disease: A systematic review of post-cochlear implantation outcomes. Laryngoscope Investig. Otolaryngol. 2021, 6, 469–487. [Google Scholar] [CrossRef]
- Aftab, S.; Semaan, M.T.; Murray, G.S.; Megerian, C.A. Cochlear implantation outcomes in patients with autoimmune and immune-mediated inner ear disease. Otol. Neurotol. 2010, 31, 1337–1342. [Google Scholar] [CrossRef]
- Rubinstein, J.T.; Ling, L.; Nowack, A.; Nie, K.; Phillips, J.O. Results From a Second-Generation Vestibular Implant in Human Subjects: Diagnosis May Impact Electrical Sensitivity of Vestibular Afferents. Otol. Neurotol. 2020, 41, 68–77. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Autoimmune Condition Associated with Secondary AIED | Prevalence of Hearing Loss | Prevalence of Vestibulopathy |
|---|---|---|
| Sjögren’s syndrome | 46% | Unknown |
| Relapsing polytonicities | 46% | Unknown |
| Behçet’s syndrome | 30–63% | Orthostatic disequilibrium in 50% but prevalence of vestibulopathy is unknown. |
| Rheumatoid arthritis | 25–72% | Unknown |
| Vogt–Koyanagi–Harada disease | 49–51% | Unknown |
| Cogan syndrome | 31–41% | 90% |
| Systemic lupus erythematosus | 6–70% | Unknown |
| Giant cell arteritis | 7–100% | Unknown |
| Wegener’s granulomatosis | 8–63% | Unknown |
| Mixed cryoglobinaemia | 22% | Unknown |
| Ulcerative colitis | 2% | Unknown |
| Systemic sclerosis | Unknown | Unknown |
| Antiphospholipid syndrome | Unknown | Unknown |
| Polyarteritis nodosa | Unknown | Unknown |
| Pyoderma gangrenosum | Unknown | Unknown |
| Takayasu’s arteritis | Unknown | Unknown |
| Hashimoto’s thyroiditis | Unknown | Unknown |
| Clinical Examination | Audiovestibular Testing | Imaging |
|---|---|---|
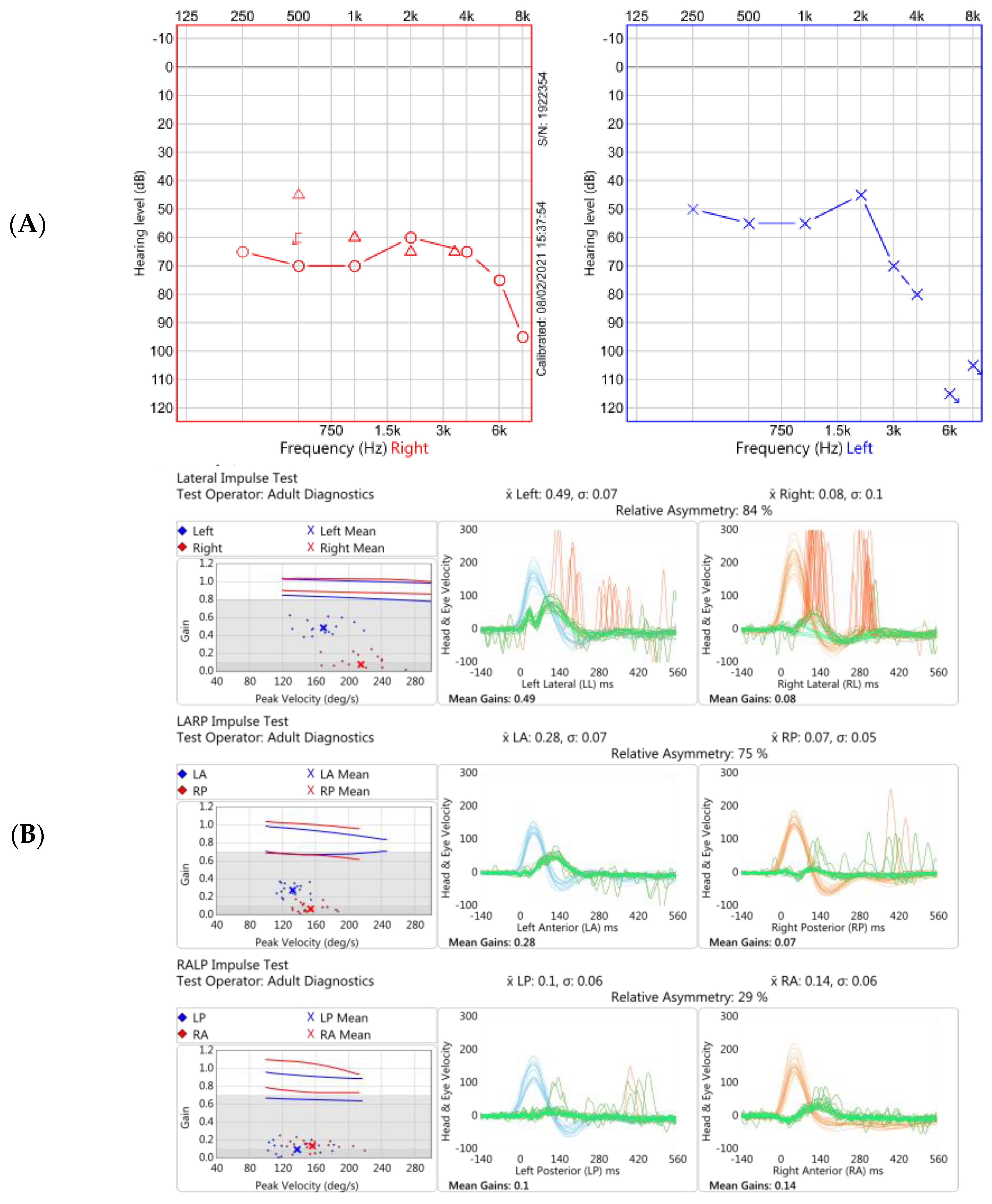
| Subtle left-beating nystagmus on left gaze only Bilateral catch up saccades in the horizontal plane on clinical head thrust testing (bilateral loss of vestibular function). Positive Romberg test Ataxic gait Normal positional (Dix-Hallpike) testing Summary: bilateral vestibular impairment, more marked on the right. Evidence of impaired dynamic and static balance. | Pure tone audiogram: bilateral moderate-to-severe SNHL, worse on the left Vestibular testing: Video head impulse test: bilateral low gain in both horizontal and vertical canals, with prominent covert and overt catch-up saccades on horizontal canal testing Impulsive rotational testing; minimal nystagmus generated bilaterally. Summary: bilateral audiovestibular dysfunction with hearing marginally worse on the left and vestibulopathy worse on the right. | Contrast-enhanced MRI four hours after IV Gadolinium: right cochlea enhancement, bilateral cochlear and vestibular hydrops and additional hydrops in the left lateral semicircular canal. |
| Examination | Blood Tests | Other | |
|---|---|---|---|
| Rheumatological | No rash | CRP, ESR: normal | |
| No synovitis | ANCA, ANA, ENA: negative | ||
| Ro, La, * SM, * RNP, SCL-70, JO-1: negative | |||
| Centromere antibodies: negative | |||
| IgG and IgM anti-Anticardiolipin: negative | |||
| IgG and IgM anti-Beta-2-glycoprotein: negative | |||
| DRVVT | |||
| Neurological | Peripheral and cranial nerve examination: normal | Purkinje cells: negative | |
| Anti-Tr antibodies (screen): negative | |||
| Other cerebellar cells: negative | |||
| IgG white matter (myelin): negative | |||
| Anti-Hu antibodies: negative | |||
| Anti-Yo antibodies: negative | |||
| Anti-Ri antibodies: negative | |||
| MPO ELISA: normal | |||
| PR3 ELISA: normal | |||
| Other | HR 70 regular, BP 138/84. | FBC, U&Es, LFTs, bone profile, thyroid function: normal | Urine analysis: normal |
| Heart sounds: normal | Syphilis, HIV, hepatitis B serology, hepatitis C serology: not detected | ||
| Chest: clear. |
| Clinical Examination | Audiovestibular Testing | Imaging |
|---|---|---|
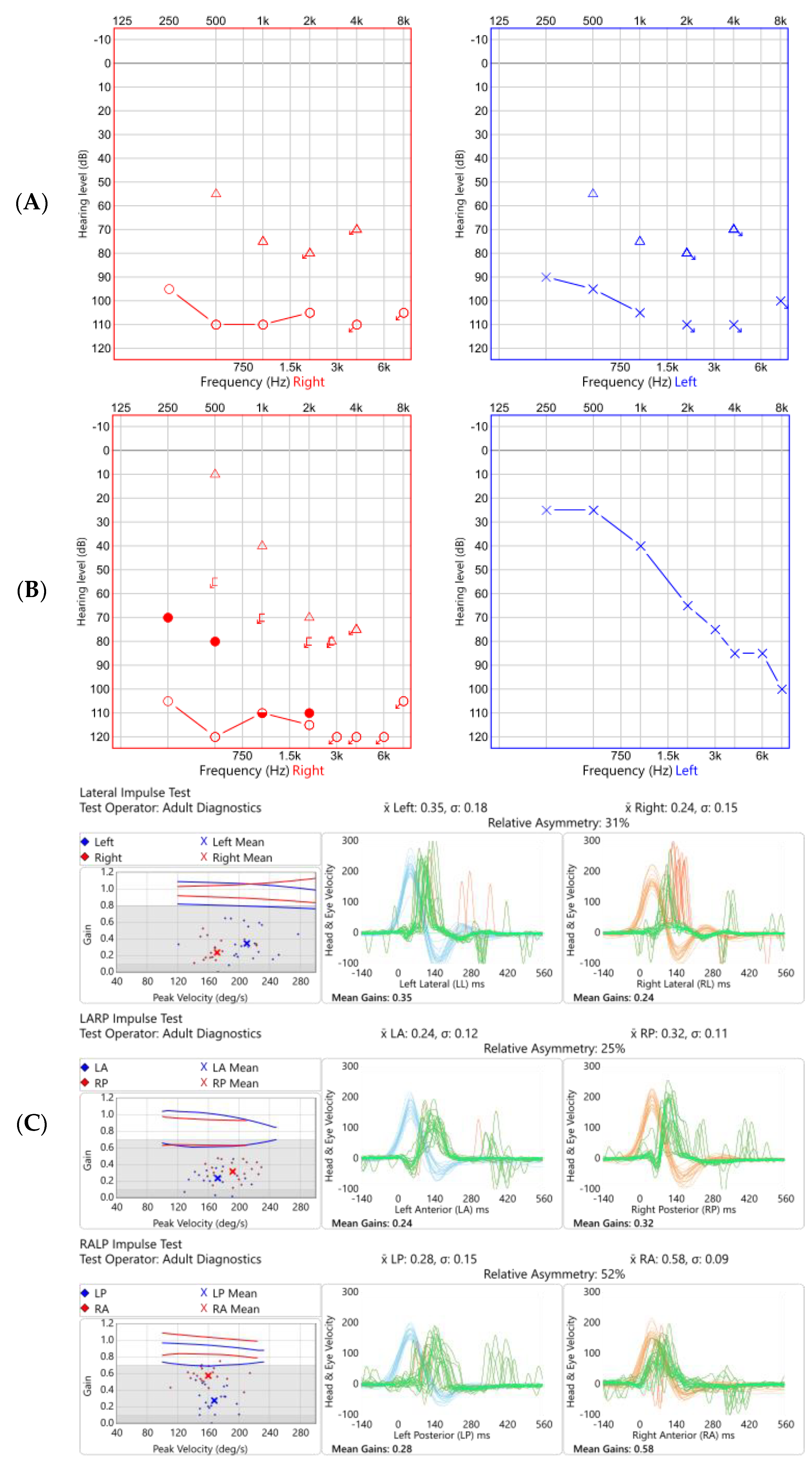
| No spontaneous- or gaze-evoked nystagmus, normal saccades and normal smooth pursuit. Bilateral catch-up saccades in the horizontal plane, more obvious on the right on head thrust testing. Positive Romberg test Ataxic gait–marked Impaired tandem gait Positional (Dix-Hallpike) testing: normal Remaining neurological examination–normal apart from global peripheral hyporeflexia. Summary: bilateral vestibular impairment, more so on the left. Evidence of impaired dynamic and static balance. | Pure tone audiogram: bilateral profound SNHL Otoacoustic emissions: bilaterally absent Acoustic reflexes: bilaterally absent Vestibular testing–video head impulse test: bilateral low gain in both horizontal and vertical canals, more so on the right, with prominent covert catch-up saccades on horizontal canal testing on the right Summary: bilateral, largely symmetric, audiovestibular dysfunction. | Contrast-enhanced MRI IAMs and brain: bilateral cochlear enhancement and enhancement of the vestibule, lateral semicircular canal and cochlear nerve on the left. Pre-contrast T1 shortening suggestive of Cogan’s syndrome but differentials include inflammatory conditions (sarcoid, connective tissue disease, Behçet’s disease), infection and CSF-borne spread of neoplastic disease. CT temporal bones: nil significant findings |
| Examination | Blood Tests | Imaging | Other | |
|---|---|---|---|---|
| Rheumatological | No rash. | Chest X-ray: normal | ||
| No lymphadenopathy | ||||
| No synovitis. | ||||
| Neurological | Nerve conduction studies: normal | |||
| Lumbar puncture and CSF analysis: normal | ||||
| other | Heart sounds normal. | |||
| Chest clear. | FBC, U&Es, LFTs, bone profile, glucose, CRP: normal | Whole body FDG PET *: | US-guided axillary | |
| Abdomen soft and non-tender | lymph node | |||
| biopsy: normal | ||||
| No palpable organomegaly | Widespread Lymphadenopathy. Repeat imaging showed mildly avid symmetrical axillary, pelvic-inguino- femoral lymph nodes. Reactive appearance, rather than pathological. | |||
| Urine analysis: | ||||
| normal | ||||
| USS abdomen: Lymphadenopathy within the abdomen and pelvis is comparable to the PET scan |
| Clinical Examination | Audiovestibular Testing | Imaging |
|---|---|---|
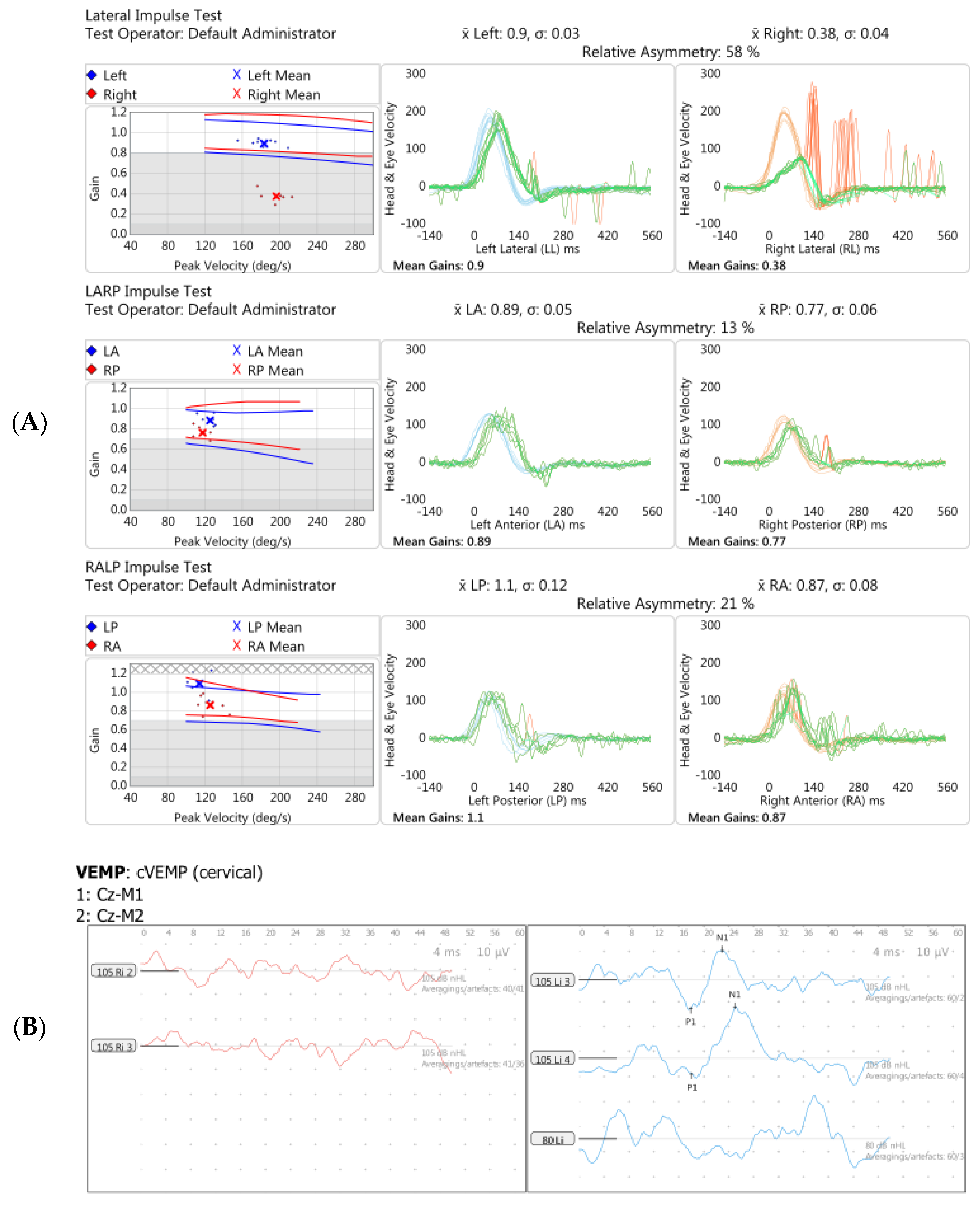
| Gaze testing: normal Right-sided catch-up saccades in the horizontal plane on head thrust testing. Positive Romberg test Ataxic gait Positional (Dix-Hallpike) testing: normal Remaining neurological examination: normal Summary: Right-sided vestibular impairment, evidence of impaired dynamic and static balance. | Pure tone audiogram (serial):
Audiovestibular testing:
Summary: Left-sided, then right-sided high frequency hearing loss. Bilateral vestibulopathy, worse on the right. | MRI IAMs and head, with and without Gadolinium contrast: normal |
| Blood Tests | |
|---|---|
| Rheumatological | Cardiolipin IgG: (weakly positive). |
| Lupus anticoagulant: normal | |
| ANA, ANCA, ENA, C3, C4: normal | |
| ESR, CRP: normal | |
| ACE: normal | |
| collagen type 2 antibodies: negative | |
| HLA-B27 antibodies: positive | |
| anti-phospholipid antibodies: negative | |
| Other | |
| FBC: mild lymphopenia | |
| ESR, U&Es, LFTs: normal | |
| Hepatitis B serology–previous immunisation | |
| Hepatitis C serology: negative. | |
| Thyroid function: normal | |
| Thyroid autoantibodies: raised (458 U/mL). | |
| VZV IgM negative, VZV IgG positive, HSV 1&2 IgG and IgM: negative. |
| Case 1 | Case 2 | Case 3 | |
|---|---|---|---|
| Gender | Male | Male | Female |
| Ethnicity | White British | Black Ghanaian | White British |
| Age at presentation | 28 | 17 | 46 |
| Occupation | Carpenter | Student | Medical doctor |
| Pre-existing medical conditions | Ulcerative colitis, migraine | Prior episode of uveitis age 4 | Allergic rhinitis/atopy |
| Hearing loss | Asymmetric, fluctuant SNHL | Insidious right SNHL, then sudden onset bilateral profound hearing loss | Asymmetric, fluctuant, high-frequency SNHL |
| Vestibulopathy | Subjective: episodic vertigo, later imbalance Objective: bilateral vestibulopathy | Subjective: sudden onset imbalance Objective: bilateral vestibulopathy | Subjective: sudden onset imbalance Objective: bilateral vestibulopathy |
| Diagnosis | Secondary AIED (in context of ulcerative colitis) | Cogan syndrome | Possible primary AIED |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendis, S.; Longley, N.; Morley, S.; Korres, G.; Kaski, D. Autoimmune Vestibulopathy—A Case Series. Brain Sci. 2022, 12, 306. https://doi.org/10.3390/brainsci12030306
Mendis S, Longley N, Morley S, Korres G, Kaski D. Autoimmune Vestibulopathy—A Case Series. Brain Sciences. 2022; 12(3):306. https://doi.org/10.3390/brainsci12030306
Chicago/Turabian StyleMendis, Surangi, Nicola Longley, Simon Morley, George Korres, and Diego Kaski. 2022. "Autoimmune Vestibulopathy—A Case Series" Brain Sciences 12, no. 3: 306. https://doi.org/10.3390/brainsci12030306
APA StyleMendis, S., Longley, N., Morley, S., Korres, G., & Kaski, D. (2022). Autoimmune Vestibulopathy—A Case Series. Brain Sciences, 12(3), 306. https://doi.org/10.3390/brainsci12030306