
Sexual Dysfunctions in Parkinson’s Disease and Their Influence on Partnership—Data of the PRISM Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. PRISM Study Design
2.2. Study Population
2.3. Study Assessment
2.4. Evaluation
- Question 83: Non-motor Symptoms Questionnaire (answering options dichotomously ‘yes’ or ‘no’)
- ○
- statement 18: Feeling less interested in sex or more interested in sex
- ○
- statement 19: Finding it difficult to have sex when you try
- Question 84: Questionnaire for Impulsive-Compulsive Disorder in Parkinson’s Disease (answering options dichotomously ‘yes’ or ‘no’)
- ○
- statement 2: Sex (compulsive urges)
- Question 86: Medical Outcomes Study Sexual Functioning Scale (answering options scaled from ‘not a problem’ to ’very much a problem’)
- ○
- statement 1: Lack of sexual interest
- ○
- statement 2: Unable to relax and enjoy sex
- ○
- statement 3: Difficult in becoming sexually aroused
- ○
- statement 4: Men only: Difficulty obtaining or keeping an erection
- ○
- statement 5: Women only: Difficulty in having an orgasm
- Question 97: Has your relationship with the person with Parkinson’s suffered because of their illness? This is in general, taking into consideration all aspects of your relationship (answering options scaled from ‘not at all’ to ’extremely’).
- Question 100: Has your sexual relationship with the person with Parkinson’s suffered because of their illness? (answering options dichotomously ‘yes’ or ‘no’).
2.5. Statistical Analysis
3. Results
3.1. Demographics of Sexual Dysfunctions in General
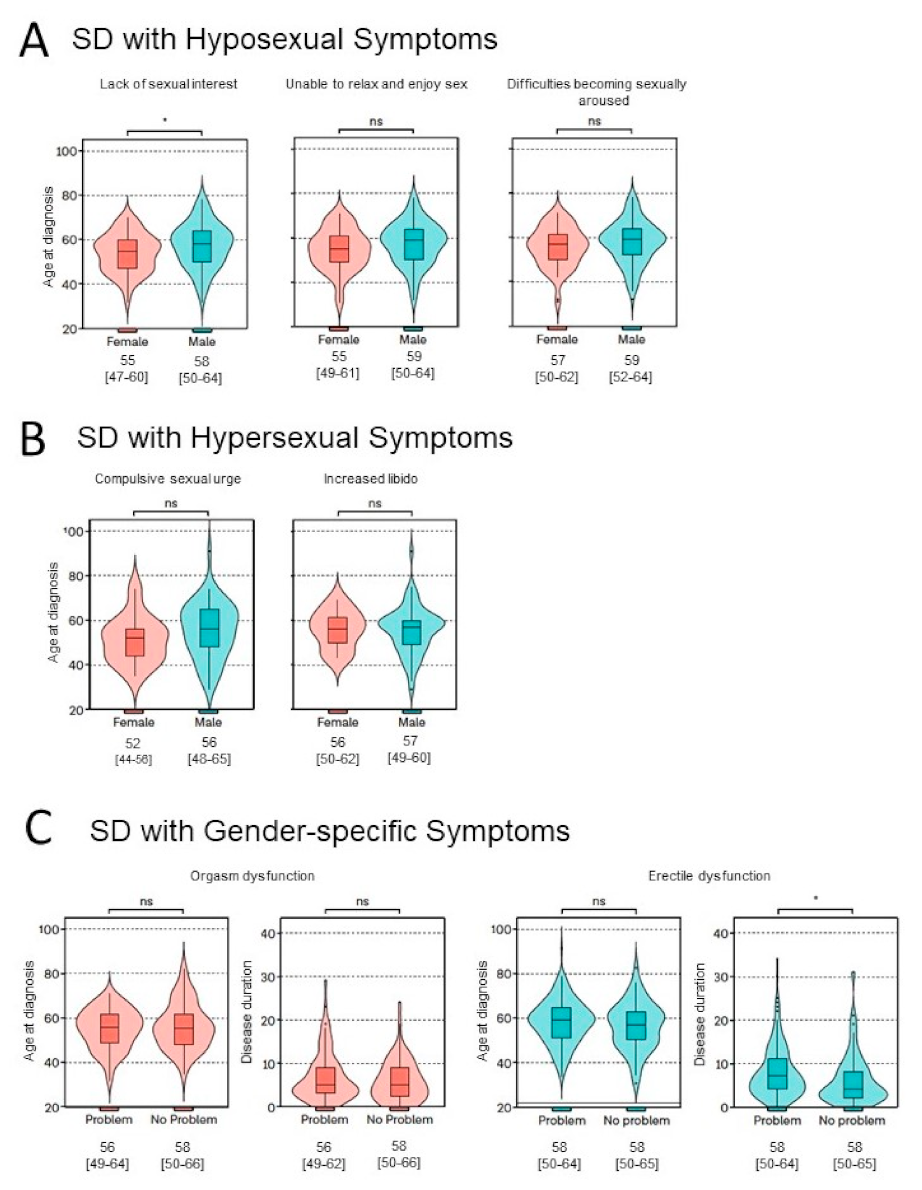
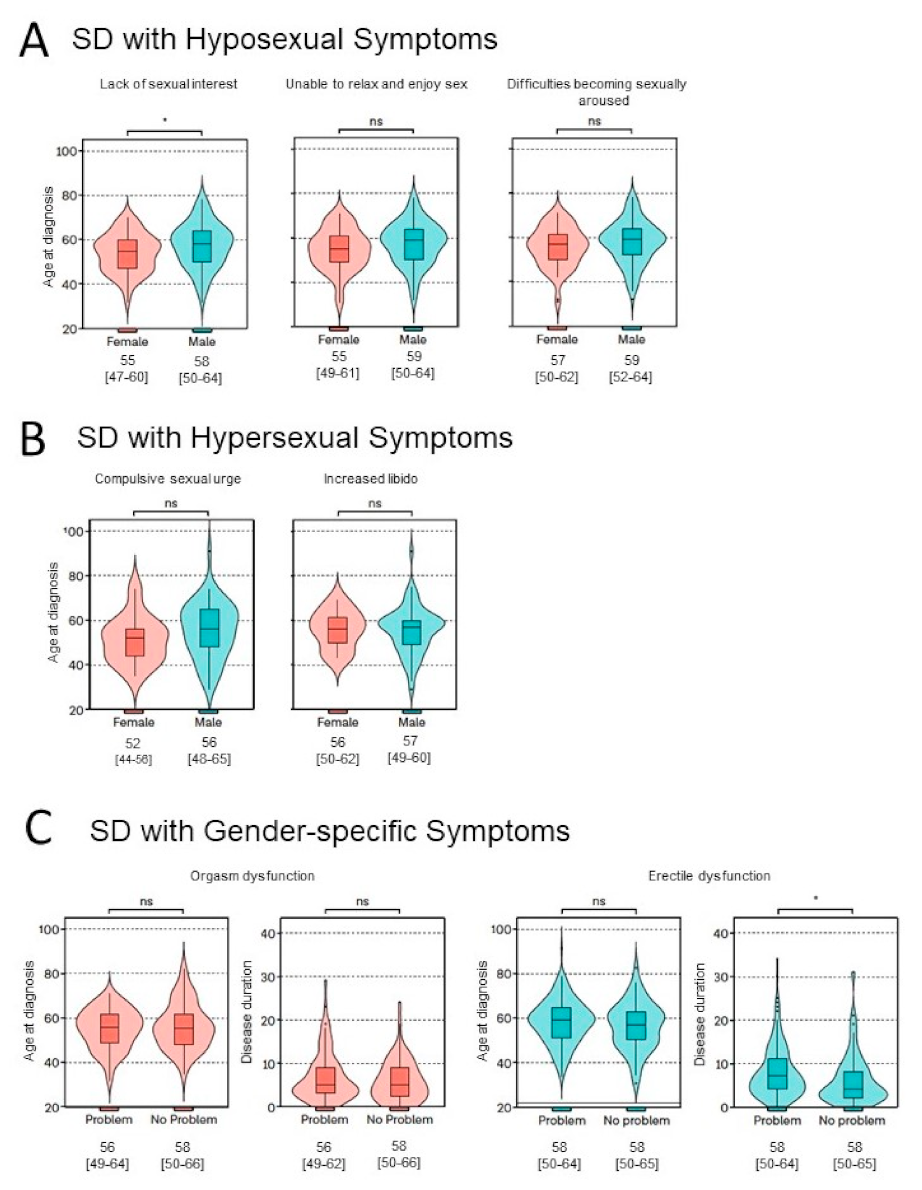
3.2. Sexual Dysfunctions in Detail
3.3. Influence of Sexual Dysfunctions on Partnership
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Responders | Total (n) | Female (n) | Male (n) |
|---|---|---|---|
| Question 83 | |||
| Statement 18: Feeling less interested in sex or more interested in sex | 602 | 283 | 311 |
| Statement 19: Finding it difficult to have sex when you try | 600 | 281 | 311 |
| Question 84 Compulsive sexual urges | 601 | 283 | 310 |
| Question 86 | |||
| Statement 1: Lack of sexual interest | 394 | 169 | 220 |
| Statement 2: Unable to relax and enjoy sex | 389 | 166 | 218 |
| Statement 3: Difficult in becoming sexually aroused | 388 | 165 | 218 |
| Statement 4: Men only: Difficulty obtaining or keeping an erection | 389 | 169 | 218 |
| Statement 5: Difficulty in having an orgasm | 390 | 165 | 220 |
| Total | Female | Male | Significance | ||
|---|---|---|---|---|---|
| Erectile Dysfunction | |||||
| N | 152 | 152 | |||
| % responders | 69.7% | 69.7% | |||
| % men with SD | 57.6% | 57.6% | |||
| Age at diagnosis (years) | N | 148 | 148 | ||
| Median [IQR] | 58 (23–26,28,55–64) | 58 (23–26,28,55–64) | |||
| Disease duration (years) | N | 147 | 147 | ||
| Median [IQR] | 7 (4–11) | 7 (4–11) | |||
| Orgasm dysfunction | |||||
| N | 84 | 84 | |||
| % responders | 50.9% | 50.9% | |||
| % women with SD | 46.8% | 46.8% | |||
| Age at diagnosis (years) | N | 77 | 77 | ||
| Median [IQR] | 56 (23–28,55–62) | 56 (23–28,55–62) | |||
| Disease duration (years) | N | 77 | 77 | ||
| Median [IQR] | 5 (3–9) | 5 (3–9) | |||
| Difficulties in becoming sexually aroused | |||||
| N | 185 | 71 | 111 | ns | |
| % responders | 47.7% | 43.0% | 50.9% | ||
| % total with SD | 43.2% | 39.4% | 42.0% | ||
| Age at diagnosis (years) | N | 174 | 63 | 109 | |
| Median [IQR] | 58 (23–26,28,55–63) | 57 (23–26,28,55–62) | 59 (24–26,55–64) | ns | |
| Disease duration (years) | N | 174 | 63 | 109 | |
| Median [IQR] | 5 (3–9) | 5 (3–8) | 6 (4–11) | ns | |
| Unable to relax and enjoy sex | |||||
| N | 177 | 68 | 106 | ns | |
| % responders | 45.5% | 41.0% | 48.6% | ||
| % total with SD | 41.4% | 37.8% | 40.2% | ||
| Age at diagnosis (years) | N | 164 | 60 | 102 | |
| Median [IQR] | 57 (23–26,28,55–63) | 55 (23–28,55–61) | 59 (23–26,28,55–64) | ns | |
| Disease duration (years) | N | 164 | 60 | 102 | |
| Median [IQR] | 5 (3–10) | 5 (3–9) | 6 (4–11) | ns | |
| Lack of sexual interest | |||||
| N | 174 | 81 | 91 | Χ2 < 0.05 * | |
| % responders | 44.2% | 48.0% | 41.4% | ||
| % total with SD | 40.65% | 45.0% | 34.5% | ||
| Age at diagnosis (years) | N | 163 | 73 | 89 | |
| Median [IQR] | 57 (23–28,55–62) | 55 (23–30,55–60) | 58 (23–26,28,55–64) | p < 0.05 * | |
| Disease duration (years) | N | 163 | 73 | 89 | |
| Median [IQR] | 5 (3–10) | 5 (3–9) | 6 (3–12) | ns | |
| Increased libido | |||||
| N | 74 | 19 | 55 | Χ2 < 0.0001 * | |
| % responders | 18.9% | 11.2% | 25.0% | ||
| % total with SD | 17.3% | 4.4% | 12.9% | ||
| Age at diagnosis (years) | N | 73 | 19 | 54 | |
| Median [IQR] | 57 (23–28,55–61) | 56 (23–26,28,55–62) | 57 (23–28,55–60) | ns | |
| Disease duration (years) | N | 71 | 19 | 52 | |
| Median [IQR] | 7 (4–10) | 4 (3–10) | 7 (4–11) | ns | |
| Compulsive sexual urges | |||||
| N | 68 | 13 | 55 | Χ2 < 0.0001 * | |
| % responders | 11.3% | 6.7% | 17.7% | ||
| % total with SD | 15.9% | 3.0% | 12.9% | ||
| Age at diagnosis (years) | N | 65 | 12 | 53 | |
| Median [IQR] | 55 (23–30,54–64) | 52 (23–30,52–56) | 56 (23–28,30,55–65) | ns | |
| Disease duration (years) | N | 63 | 12 | 51 | |
| Median [IQR] | 9 (4–13) | 7 (3–9) | 9 (5–13) | ns | |
References
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef] [PubMed]
- Elbaz, A.; Carcaillon, L.; Kab, S.; Moisan, F. Epidemiology of Parkinson’s disease. Rev. Neurol. 2016, 172, 14–26. [Google Scholar] [CrossRef] [PubMed]
- Pringsheim, T.; Jette, N.; Frolkis, A.; Steeves, T.D.L. The prevalence of Parkinson’s disease: A systematic review and meta-analysis. Mov. Disord. 2014, 29, 1583–1590. [Google Scholar] [CrossRef] [PubMed]
- Dorsey, E.R.; Sherer, T.; Okun, M.S.; Bloemd, B.R. The emerging evidence of the Parkinson pandemic. J. Parkinsons Dis. 2018, 8, S3–S8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfeiffer, R.F. Non-motor symptoms in Parkinson’s disease. Park. Relat. Disord. 2015, 22, S119–S122. [Google Scholar] [CrossRef]
- Chaudhuri, K.R.; Odin, P. The challenge of non-motor symptoms in Parkinson’s disease. In Progress in Brain Research; Elsevier B.V.: Amsterdam, The Netherlands, 2010; pp. 325–341. [Google Scholar]
- Khedr, E.M.; El Fetoh, N.A.; Khalifa, H.; Ahmed, M.A.; El Beh, K.M.A. Prevalence of non motor features in a cohort of Parkinson’s disease patients. Clin. Neurol. Neurosurg. 2013, 115, 673–677. [Google Scholar] [CrossRef]
- Barone, P.; Erro, R.; Picillo, M. Quality of Life and Nonmotor Symptoms in Parkinson’s Disease. Int. Rev. Neurobiol. 2017, 133, 499–516. [Google Scholar] [CrossRef]
- Weerkamp, N.J.; Tissingh, G.; Poels, P.J.; Zuidema, S.U.; Munneke, M.; Koopmans, R.T.; Bloem, B.R. Nonmotor Symptoms in Nursing Home Residents with Parkinson’s Disease: Prevalence and Effect on Quality of Life. J. Am. Geriatr. Soc. 2013, 61, 1714–1721. [Google Scholar] [CrossRef]
- Santa Rosa Malcher, C.M.; da Silva Gonçalves Oliveira, K.R.; Fernandes Caldato, M.C.; Dos Santos Lobato, B.L.; da Silva Pedroso, J.; de Tubino Scanavino, M. Sexual Disorders and Quality of Life in Parkinson’s Disease. Sex. Med. 2021, 9, 100280. [Google Scholar] [CrossRef]
- Laumann, E.O.; Paik, A.; Rosen, R.C. Sexual Dysfunction in the United States. JAMA 1999, 281, 537. [Google Scholar] [CrossRef] [Green Version]
- Bronner, G.; Royter, V.; Korczyn, A.D.; Giladi, N. Sexual Dysfunction in Parkinson’s Disease. J. Sex Marital Ther. 2004, 30, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Varanda, S.; da Silva, J.R.; Costa, A.S.; de Carvalho, C.A.; Alves, J.N.; Rodrigues, M.; Carneiro, G. Sexual dysfunction in women with Parkinson’s disease. Mov. Disord. 2016, 31, 1685–1693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meco, G.; Rubino, A.; Caravona, N.; Valente, M. Sexual dysfunction in Parkinson’s disease. Parkinsonism Relat. Disord. 2008, 14, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Bronner, G.; Vodušek, D.B. Management of sexual dysfunction in Parkinson’s disease. Ther. Adv. Neurol. Disord. 2011, 4, 375–383. [Google Scholar] [CrossRef] [Green Version]
- Bronner, G.; Aharon-Peretz, J.; Hassin-Baer, S. Sexuality in patients with Parkinson’s disease, Alzheimer’s disease, and other dementias. In Handbook of Clinical Neurology; Elsevier B.V.: Amsterdam, The Netherlands, 2015; pp. 297–323. [Google Scholar]
- Buhmann, C.; Dogac, S.; Vettorazzi, E.; Hidding, U.; Gerloff, C.; Jürgens, T.P. The impact of Parkinson disease on patients’ sexuality and relationship. J. Neural Transm. 2016, 124, 983–996. [Google Scholar] [CrossRef]
- Wielinski, C.L.; Varpness, S.C.; Erickson-Davis, C.; Paraschos, A.J.; Parashos, S.A. Sexual and Relationship Satisfaction among Persons with Young-Onset Parkinson’s Disease. J. Sex. Med. 2010, 7, 1438–1444. [Google Scholar] [CrossRef]
- Tolosa, E.; Ebersbach, G.; Ferreira, J.J.; Rascol, O.; Antonini, A.; Foltynie, T.; Gibson, R.; Magalhaes, D.; Rocha, J.F.; Lees, A. The Parkinson’s Real-World Impact Assessment (PRISM) Study: A European Survey of the Burden of Parkinson’s Disease in Patients and their Carers. J. Park. Dis. 2021, 11, 1309–1323. [Google Scholar] [CrossRef]
- Chaudhuri, K.R.; Martinez-Martin, P.; Schapira, A.H.; Stocchi, F.; Sethi, K.; Odin, P.; Brown, R.G.; Koller, W.; Barone, P.; Macphee, G.; et al. International multicenter pilot study of the first comprehensive self-completed nonmotor symptoms questionnaire for Parkinson’s disease: The NMSQuest study. Mov. Disord. 2006, 21, 916–923. [Google Scholar] [CrossRef]
- Weintraub, D.; Hoops, S.; Shea, J.A.; Lyons, K.E.; Pahwa, R.; Driver-Dunckley, E.D.; Adler, C.H.; Potenza, M.N.; Miyasaki, J.; Siderowf, A.D.; et al. Validation of the questionnaire for impulsive-compulsive disorders in Parkinson’s disease. Mov. Disord. 2009, 24, 1461–1467. [Google Scholar] [CrossRef] [Green Version]
- Sherbourne, C.D.; Stewart, A.L.; Ware, J.E. Social functioning: Sexual problems measures. In Measuring Functioning and Well-Being: The Medical Outcomes Study Approach; Stewart, A.L., Ware, J.E., Eds.; Duke University Press: Durham, NC, USA, 1992; pp. 194–204. [Google Scholar]
- Bhattacharyya, K.B.; Rosa-Grilo, M. Sexual Dysfunctions in Parkinson’s Disease: An Underrated Problem in a Much Discussed Disorder. Int Rev Neurobiol. 2017, 134, 859–876. [Google Scholar] [CrossRef]
- Raciti, L.; De Cola, M.C.; Ortelli, P.; Corallo, F.; Buono, V.L.; Morini, E.; Quattrini, F.; Filoni, S.; Calabrò, R.S. Sexual Dysfunction in Parkinson Disease: A Multicenter Italian Cross-sectional Study on a Still Overlooked Problem. J. Sex. Med. 2020, 17, 1914–1925. [Google Scholar] [CrossRef] [PubMed]
- Chaudhuri, K.R.; Schapira, A.H. Non-motor symptoms of Parkinson’s disease: Dopaminergic pathophysiology and treatment. Lancet Neurol. 2009, 8, 464–474. [Google Scholar] [CrossRef]
- Sakakibara, R.; Shinotoh, H.; Uchiyama, T.; Sakuma, M.; Kashiwado, M.; Yoshiyama, M.; Hattori, T. Questionnaire-based assessment of pelvic organ dysfunction in Parkinson’s disease. Auton. Neurosci. 2001, 92, 76–85. [Google Scholar] [CrossRef]
- Briken, P.; Matthiesen, S.; Pietras, L.; Wiessner, C.; Klein, V.; Reed, G.M.; Dekker, A. Prävalenzschätzungen sexueller Dysfunktionen anhand der neuen ICD-11-Leitlinien. Dtsch. Arztebl. Int. 2020, 117, 653–658. [Google Scholar] [CrossRef]
- McCabe, M.P.; Sharlip, I.D.; Lewis, R.; Atalla, E.; Balon, R.; Fisher, A.D.; Laumann, E.; Lee, S.W.; Segraves, R.T. Incidence and Prevalence of Sexual Dysfunction in Women and Men: A Consensus Statement from the Fourth International Consultation on Sexual Medicine 2015. J. Sex. Med. 2016, 13, 144–152. [Google Scholar] [CrossRef]
- Vela-Desojo, L.; Urso, D.; Kurtis-Urra, M.; García-Ruiz, P.J.; Pérez-Fernández, E.; Lopez-Valdes, E.; Posada-Rodriguez, I.; Ybot-Gorrin, I.; Lopez-Manzanares, L.; Mata, M.; et al. Sexual Dysfunction in Early-Onset Parkinson’s Disease: A Cross-Sectional, Multicenter Study. J. Park. Dis. 2020, 10, 1621–1629. [Google Scholar] [CrossRef]
- Kovács, M.; Makkos, A.; Aschermann, Z.; Janszky, J.; Komoly, S.; Weintraut, R.; Karádi, K.; Kovacs, N. Impact of Sex on the Nonmotor Symptoms and the Health-Related Quality of Life in Parkinson’s Disease. Park. Dis. 2016, 2016, 1–12. [Google Scholar] [CrossRef]
- Martinez-Martin, P.; Schapira, A.H.; Stocchi, F.; Sethi, K.; Odin, P.; Macphee, G.; Brown, R.; Naidu, Y.; Clayton, L.; Abe, K.; et al. Prevalence of nonmotor symptoms in Parkinson’s disease in an international setting; Study using nonmotor symptoms questionnaire in 545 patients. Mov. Disord. 2007, 22, 1623–1629. [Google Scholar] [CrossRef]
- Kotagal, V.; Albin, R.L.; Müller, M.L.T.M.; Koeppe, R.A.; Frey, K.A.; Bohnen, N.I. Gender differences in cholinergic and dopaminergic deficits in Parkinson disease. J. Neural Transm. 2013, 120, 1421–1424. [Google Scholar] [CrossRef] [Green Version]
- Wong, K.K.; Müller, M.L.; Kuwabara, H.; Studenski, S.A.; Bohnen, N.I. Gender differences in nigrostriatal dopaminergic innervation are present at young-to-middle but not at older age in normal adults. J. Clin. Neurosci. 2012, 19, 183–184. [Google Scholar] [CrossRef]
- Jurado-Coronel, J.C.; Cabezas, R.; Ávila Rodríguez, M.F.; Echeverria, V.; García-Segura, L.M.; Barreto, G.E. Sex differences in Parkinson’s disease: Features on clinical symptoms, treatment outcome, sexual hormones and genetics. Front. Neuroendocrinol. 2018, 50, 18–30. [Google Scholar] [CrossRef]
- Smith, K.M.; Dahodwala, N. Sex differences in Parkinson’s disease and other movement disorders. Exp. Neurol. 2014, 259, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Gillies, G.E.; Pienaar, I.S.; Vohra, S.; Qamhawi, Z. Sex differences in Parkinson’s disease. Front. Neuroendocrinol. 2014, 35, 370–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantuti-Castelvetri, I.; Keller-McGandy, C.; Bouzou, B.; Asteris, G.; Clark, T.; Frosch, M.P.; Standaert, D. Effects of gender on nigral gene expression and parkinson disease. Neurobiol. Dis. 2007, 26, 606–614. [Google Scholar] [CrossRef] [Green Version]
- Weiduschat, N.; Kaufmann, P.; Mao, X.; Engelstad, K.M.; Hinton, V.; DiMauro, S.; De Vivo, D.; Shungu, D. Cerebral metabolic abnormalities in A3243G mitochondrial DNA mutation carriers. Neurology 2014, 82, 798–805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papatsoris, A.G.; Deliveliotis, C.; Singer, C.; Papapetropoulos, S. Erectile dysfunction in Parkinson’s disease. Urology 2006, 67, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Laumann, E.O.; Glasser, D.B.; Neves, R.C.S.; Moreira, E.D. A population-based survey of sexual activity, sexual problems and associated help-seeking behavior patterns in mature adults in the United States of America. Int. J. Impot. Res. 2009, 21, 171–178. [Google Scholar] [CrossRef] [Green Version]
- McKinlay, J. The worldwide prevalence and epidemiology of erectile dysfunction. Int. J. Impot. Res. 2020, 12, S6–S11. [Google Scholar] [CrossRef] [Green Version]
- Shamloul, R.; Ghanem, H. Erectile dysfunction. Lancet 2013, 381, 153–165. [Google Scholar] [CrossRef]
- Weintraub, D.; Claassen, D.O. Impulse Control and Related Disorders in Parkinson’s Disease. Int. Rev. Neurobiol. 2017, 133, 679–717. [Google Scholar]
- Berger, C.; Mehrhoff, F.W.; Beier, K.M.; Meinck, H.M. Sexuelle delinquenz und morbus Parkinson. Nervenarzt 2003, 74, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Codling, D.; Shaw, P.; David, A.S. Hypersexuality in Parkinson’s Disease: Systematic Review and Report of 7 New Cases. Mov. Disord. Clin. Pract. 2015, 2, 116–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shalash, A.; Hamid, E.; Elrassas, H.; Abushouk, A.I.; Salem, H.H. Sexual dysfunction in male patients with Parkinson’s disease: Related factors and impact on quality of life. Neurol. Sci. 2020, 41, 2201–2206. [Google Scholar] [CrossRef] [PubMed]
- Weintraub, D.; David, A.S.; Evans, A.H.; Grant, J.E.; Stacy, M. Clinical spectrum of impulse control disorders in Parkinson’s disease. Mov. Disord. 2015, 30, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Weintraub, D. Impulse control disorders in Parkinson’s disease: Prevalence and possible risk factors. Parkinsonism Relat. Disord. 2009, 15, S110–S113. [Google Scholar] [CrossRef]
- Baumann-Vogel, H.; Valko, P.O.; Eisele, G.; Baumann, C.R. Impulse control disorders in Parkinson’s disease: Don’t set your mind at rest by self-assessments. Eur. J. Neurol. 2015, 22, 603–609. [Google Scholar] [CrossRef] [Green Version]
- Felce, D.; Perry, J. Quality of life: Its definition and measurement. Res. Dev. Disabil. 1995, 16, 51–74. [Google Scholar] [CrossRef]
- Chaudhuri, K.R.; Prieto-Jurcynska, C.; Naidu, Y.; Mitra, T.; Frades-Payo, B.; Tluk, S.; Ruessmann, A.; Odin, P.; Macphee, G.; Stocchi, F.; et al. The nondeclaration of nonmotor symptoms of Parkinson’s disease to health care professionals: An international study using the nonmotor symptoms questionnaire. Mov. Disord. 2010, 25, 704–709. [Google Scholar] [CrossRef]
- Shulman, L.M.; Taback, R.L.; Rabinstein, A.A.; Weiner, W.J. Non-recognition of depression and other non-motor symptoms in Parkinson’s disease. Parkinsonism Relat. Disord. 2002, 8, 193–197. [Google Scholar] [CrossRef]
- Chaudhuri, K.R.; Odin, P.; Antonini, A.; Martinez-Martin, P. Parkinson’s disease: The non-motor issues. Parkinsonism Relat. Disord. 2011, 17, 717–723. [Google Scholar] [CrossRef]
- Marxreiter, F.; Buttler, U.; Gassner, H.; Gandor, F.; Gladow, T.; Eskofier, B.; Winkler, J.; Ebersbach, G.; Klucken, J. The Use of Digital Technology and Media in German Parkinson’s Disease Patients. J. Park. Dis. 2020, 10, 717–727. [Google Scholar] [CrossRef] [PubMed]
| Total | Female | Male | Significance | ||
|---|---|---|---|---|---|
| All patients | |||||
| N | 861 | 418 | 433 | ||
| % | 100.0% | 48.5% | 50.3% | ||
| Age at diagnosis (years) | N | 827 | 402 | 418 | |
| Median [IQR] | 58 (49–65) | 57 (49–66) | 58 (51–65) | ns | |
| Disease duration (years) | N | 813 | 397 | 410 | |
| Median [IQR] | 6 (3–11) | 6 (3–10) | 6 (3–12) | p < 0.05 * | |
| Patients answering at least one question concerning sexuality | |||||
| N | 602 | 284 | 311 | ||
| % total | 69.9% | 67.9% | 71.8% | ||
| Age at diagnosis (years) | N | 580 | 272 | 303 | |
| Median [IQR] | 58 (50–65) | 58 (50–66) | 59 (51–65) | ns | |
| Disease duration (years) | N | 572 | 269 | 298 | |
| Median [IQR] | 6 (3–10) | 5 (3-10) | 6 (3–12) | p < 0.05 * | |
| Patients reporting any kind of sexual dysfunction | |||||
| N | 449 | 180 | 263 | p < 0.001 * | |
| % total | 52.1% | 43.1% | 60.7% | ||
| Age at diagnosis (years) | N | 428 | 169 | 256 | |
| Median [IQR] | 58 (49–64) | 56 (49–63) | 59 (50–65) | ns | |
| Disease duration (years) | N | 422 | 167 | 252 | |
| Median [IQR] | 6 (3–11) | 5 (3–10) | 7 (4–12) | ns | |
| Patients denying any kind of sexual dysfunction in NMSQuest and QUIP | |||||
| N | 201 | 130 | 67 | ns | |
| % total | 23.3% | 31.1% | 15.5% | ||
| Age at diagnosis (years) | N | 197 | 128 | 66 | |
| Median [IQR] | 60 (52–67) | 60 (54–67) | 59 (49–65) | ns | |
| Disease duration (years) | N | 195 | 127 | 65 | |
| Median [IQR] | 5 (3–9) | 5 (3–8) | 5 (2–10) | ns | |
| Patients denying any kind of sexual dysfunction in NMSQuest, QUIP and MOS-SFS | |||||
| N | 58 | 34 | 24 | ns | |
| % total | 6.7% | 8.1% | 5.5% | ||
| Age at diagnosis (years) | N | 58 | 34 | 24 | |
| Median [IQR] | 57 (51–67) | 58 (54–68) | 56 (47–63) | ns | |
| Disease duration (years) | N | 58 | 34 | 24 | |
| Median [IQR] | 4 (2–8) | 4 (2–7) | 4 (2–8) | ns | |
| Erectile Dysfunction | |||||||
|---|---|---|---|---|---|---|---|
| Does the Relationship Suffer? | Does the Sexual Relationship Suffer? | ||||||
| Severity | Not at all | Slightly | Moderately | Very Much | Extremely | No | Yes |
| Very much a problem (n) | 6 | 7 | 13 | 5 | 6 | 7 | 28 |
| Somewhat of a problem (n) | 6 | 3 | 5 | 1 | 0 | 4 | 9 |
| Little of a problem (n) | 7 | 3 | 2 | 0 | 0 | 7 | 5 |
| No problem (n) | 5 | 3 | 5 | 2 | 0 | 8 | 4 |
| Χ2 = 0.1916 | Χ2 < 0.01 * | ||||||
| Orgasm dysfunction | |||||||
| Very much a problem (n) | 1 | 0 | 3 | 0 | 0 | 2 | 2 |
| Somewhat of a problem (n) | 3 | 0 | 5 | 2 | 0 | 3 | 7 |
| Little of a problem (n) | 4 | 6 | 3 | 0 | 0 | 8 | 5 |
| No problem (n) | 11 | 4 | 4 | 2 | 0 | 14 | 3 |
| Χ2 = 0.0579 | Χ2 = 0.0569 | ||||||
| Difficulties in becoming sexually aroused | |||||||
| Very much a problem (n) | 4 | 5 | 8 | 3 | 3 | 3 | 19 |
| Somewhat of a problem (n) | 3 | 6 | 5 | 2 | 0 | 3 | 11 |
| Little of a problem (n) | 14 | 8 | 7 | 1 | 1 | 17 | 13 |
| No problem (n) | 22 | 9 | 18 | 5 | 2 | 31 | 18 |
| Χ2 = 0.2752 | Χ2 < 0.001 * | ||||||
| Unable to relax and enjoy sex | |||||||
| Very much a problem (n) | 2 | 3 | 8 | 1 | 2 | 1 | 14 |
| Somewhat of a problem (n) | 4 | 7 | 8 | 5 | 4 | 10 | 16 |
| Little of a problem (n) | 8 | 7 | 5 | 0 | 0 | 8 | 10 |
| No problem (n) | 29 | 9 | 18 | 4 | 0 | 35 | 18 |
| Χ2 < 0.01 * | Χ2 < 0.001 * | ||||||
| Lack of sexual interest | |||||||
| Very much a problem (n) | 1 | 2 | 6 | 5 | 3 | 1 | 15 |
| Somewhat of a problem (n) | 3 | 4 | 9 | 3 | 2 | 6 | 12 |
| Little of a problem (n) | 9 | 10 | 9 | 0 | 1 | 14 | 14 |
| No problem (n) | 29 | 11 | 17 | 6 | 1 | 34 | 22 |
| Χ2 < 0.01 * | Χ2 < 0.01 * | ||||||
| Increased libido | |||||||
| Yes (n) | 13 | 7 | 11 | 3 | 1 | 13 | 17 |
| No (n) | 29 | 20 | 30 | 11 | 6 | 42 | 46 |
| Χ2 = 0.8869 | Χ2 = 0.8378 | ||||||
| Compulsive sexual urges | |||||||
| Yes (n) | 5 | 7 | 13 | 4 | 3 | 9 | 19 |
| No (n) | 63 | 46 | 47 | 33 | 8 | 57 | 79 |
| Χ2 = 0.1169 | Χ2 = 0.4543 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kinateder, T.; Marinho, D.; Gruber, D.; Hatzler, L.; Ebersbach, G.; Gandor, F. Sexual Dysfunctions in Parkinson’s Disease and Their Influence on Partnership—Data of the PRISM Study. Brain Sci. 2022, 12, 159. https://doi.org/10.3390/brainsci12020159
Kinateder T, Marinho D, Gruber D, Hatzler L, Ebersbach G, Gandor F. Sexual Dysfunctions in Parkinson’s Disease and Their Influence on Partnership—Data of the PRISM Study. Brain Sciences. 2022; 12(2):159. https://doi.org/10.3390/brainsci12020159
Chicago/Turabian StyleKinateder, Thomas, Daniela Marinho, Doreen Gruber, Laura Hatzler, Georg Ebersbach, and Florin Gandor. 2022. "Sexual Dysfunctions in Parkinson’s Disease and Their Influence on Partnership—Data of the PRISM Study" Brain Sciences 12, no. 2: 159. https://doi.org/10.3390/brainsci12020159
APA StyleKinateder, T., Marinho, D., Gruber, D., Hatzler, L., Ebersbach, G., & Gandor, F. (2022). Sexual Dysfunctions in Parkinson’s Disease and Their Influence on Partnership—Data of the PRISM Study. Brain Sciences, 12(2), 159. https://doi.org/10.3390/brainsci12020159