

Burdens and Resources of Staff of a Specialized Ward for Neuropalliative Care: A Cross-Sectional Survey
 , and
, and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Sample Description
3.2. Critical Number of Deaths per Week
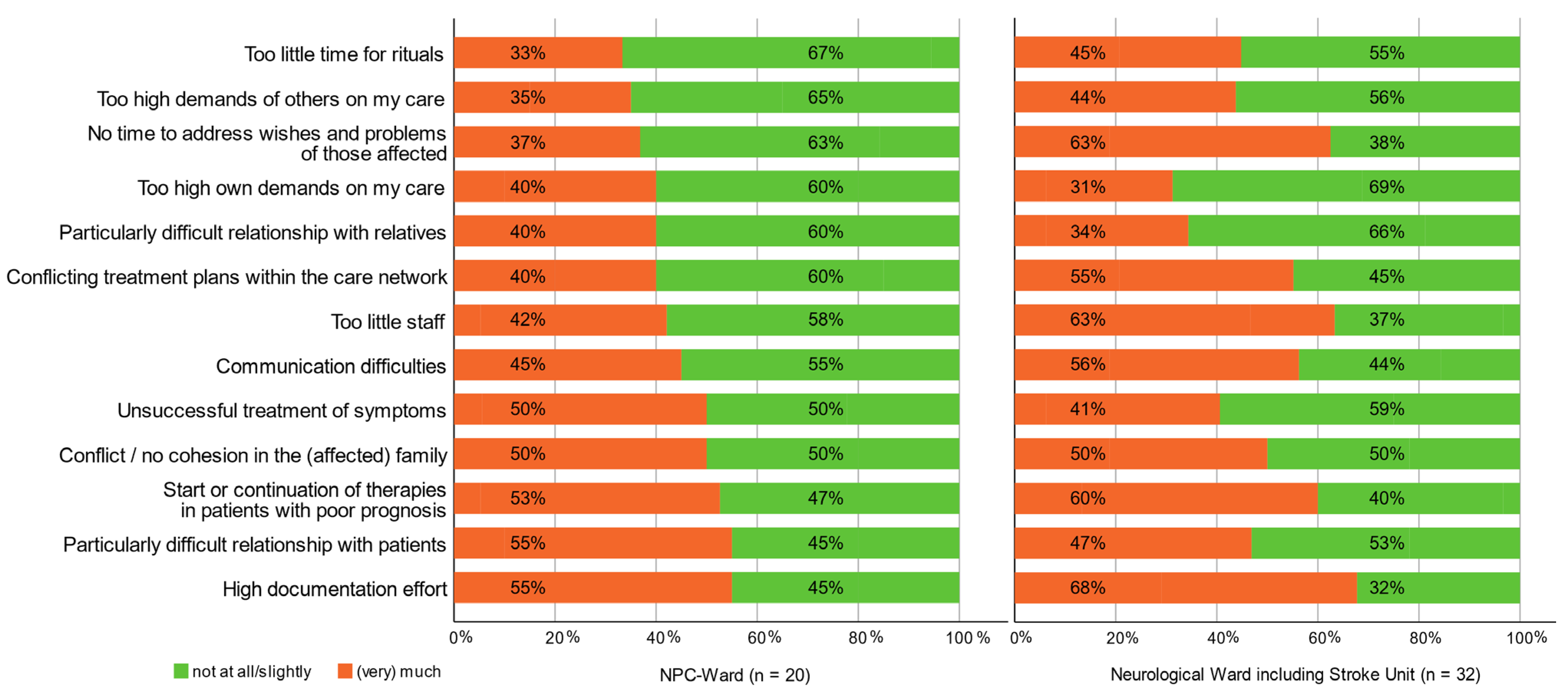
3.3. Potential Burdens
3.4. Institutional and Interpersonal Burdening Events
3.5. Stress Symptoms Shown by the Team when Confronted with Death
3.6. Personal Resources
3.7. Palliative Care Attitude, Change of Working Conditions, and Team Sustainability
3.8. Physical and Mental Distress Symptoms
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Parola, V.; Coelho, A.; Cardoso, D.; Sandgren, A.; Apostolo, J. Prevalence of burnout in health professionals working in palliative care: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2017, 15, 1905–1933. [Google Scholar] [CrossRef] [PubMed]
- Creutzfeldt, C.J.; Kluger, B.M.; Holloway, R.G.; SpringerLink. Neuropalliative Care: A Guide to Improving the Lives of Patients and Families Affected by Neurologic Disease, 1st ed.; Springer: Cham, Switzerland, 2019. [Google Scholar]
- Ablett, J.R.; Jones, R.S. Resilience and well-being in palliative care staff: A qualitative study of hospice nurses’ experience of work. Psychooncology 2007, 16, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Peters, L.; Cant, R.; Sellick, K.; O’Connor, M.; Lee, S.; Burney, S.; Karimi, L. Is work stress in palliative care nurses a cause for concern? A literature review. Int. J. Palliat. Nurs. 2012, 18, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Zanatta, F.; Maffoni, M.; Giardini, A. Resilience in palliative healthcare professionals: A systematic review. Support. Care Cancer 2020, 28, 971–978. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Sanchez, J.C.; Perez-Marmol, J.M.; Blasquez, A.; Santos-Ruiz, A.M.; Peralta-Ramirez, M.I. Association between burnout and cortisol secretion, perceived stress, and psychopathology in palliative care unit health professionals. Palliat. Support. Care 2018, 16, 286–297. [Google Scholar] [CrossRef] [PubMed]
- Kauffmann, J.; Müller, E.; Becker, G. Burdens, Resources and Expectation to Stay on the Job in Members of Specialised Outpatient Palliative Care Teams in Bavaria. Zeitschrift für Palliativmedizin 2021, 22, 47–54. [Google Scholar] [CrossRef]
- Dijxhoorn, A.Q.; Brom, L.; van der Linden, Y.M.; Leget, C.; Raijmakers, N.J. Healthcare Professionals’ Work-Related Stress in Palliative Care: A Cross-Sectional Survey. J. Pain Symptom Manag. 2021, 62, e38–e45. [Google Scholar] [CrossRef] [PubMed]
- Tertemiz, O.F.; Tuyluoglu, E. Are signs of burnout and stress in palliative care workers different from other clinic workers? Agri 2020, 32, 79–84. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, S.; Gerhart, J.I.; Grosse, J.; Abrams, I.; Levy, M.M. Posttraumatic stress symptoms in palliative care professionals seeking mindfulness training: Prevalence and vulnerability. Palliat. Med. 2016, 30, 189–192. [Google Scholar] [CrossRef] [PubMed]
- Kamal, A.H.; Bull, J.H.; Wolf, S.P.; Swetz, K.M.; Shanafelt, T.D.; Ast, K.; Kavalieratos, D.; Sinclair, C.T. Prevalence and Predictors of Burnout Among Hospice and Palliative Care Clinicians in the U.S. J. Pain Symptom Manag. 2020, 59, e6–e13. [Google Scholar] [CrossRef] [PubMed]
- Muller, M.; Pfister, D.; Markett, S.; Jaspers, B. How many patient deaths can a team cope with?: A nationwide survey of palliative care units in Germany. Schmerz 2009, 23, 600–608. [Google Scholar] [CrossRef] [PubMed]
- Ateş, G.; Jaspers, B.; Kern, M. Belastungs- und Schutzfaktoren in Teams der Hospiz- und Palliativversorgung in Nordrhein-Westfalen–eine Pilotstudie. 2020. Available online: https://alpha-nrw.de/neuerscheinung-pilotstudie-belastungs-und-schutzfaktoren-in-teams-der-hospiz-und-palliativversorgung/ (accessed on 8 November 2022).
- Rokusek, C.; Chandan, N. Palliative Care—An Ideal Environment for Interprofessional Education and Practice. Austin Palliat. Care 2016, 1, 1006. [Google Scholar]
- Barstow, J. Stress variance in hospice nursing. Nurs. Outlook 1980, 28, 751–754. [Google Scholar] [PubMed]
- Wahrendorf, M.; Sembajwe, G.; Zins, M.; Berkman, L.; Goldberg, M.; Siegrist, J. Long-term effects of psychosocial work stress in midlife on health functioning after labor market exit--results from the GAZEL study. J. Gerontol. B Psychol. Sci. Soc. Sci. 2012, 67, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Moores, T.S.; Castle, K.L.; Shaw, K.L.; Stockton, M.R.; Bennett, M.I. ‘Memorable patient deaths’: Reactions of hospital doctors and their need for support. Med. Educ. 2007, 41, 942–946. [Google Scholar] [CrossRef] [PubMed]
- Edmonds, K.P.; Yeung, H.N.; Onderdonk, C.; Mitchell, W.; Thornberry, K. Clinical supervision in the palliative care team setting: A concrete approach to team wellness. J. Palliat. Med. 2015, 18, 274–277. [Google Scholar] [CrossRef] [PubMed]
- Barham, D.; de Beer, W.; Clark, H. The role of professional supervision for palliative care doctors in New Zealand: A quantitative survey of attitudes and experiences. N. Z. Med. J. 2019, 132, 10–20. [Google Scholar] [PubMed]
- Diener, E.; Pressman, S.D.; Hunter, J.; Delgadillo-Chase, D. If, Why, and When Subjective Well-Being Influences Health, and Future Needed Research. Appl. Psychol. Health Well Being 2017, 9, 133–167. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| NPC Ward | Neuro Ward | Mann–Whitney U-Test | |
|---|---|---|---|
| Response rate | 87% (n = 20) | 78% (n = 32) | n.s. |
| Mean work experience with SD | 17.7 years (±14.5) | 11.1 years (±10.3) | n.s. |
| Experience in palliative care | 4.7 years (±9.6) | 0.9 years (±2.2) | p = 0.019 * |
| Overtime per week | 4.2 h (±3.9) | 6.3 h (±8.7) | n.s. |
| Fisher’s exact test | |||
| Living situation | Alone: 35% (n = 7) | Alone: 34% (n = 11) | n.s. |
| Together: 65% (n = 13) | Together: 66% (n = 21) | ||
| Working time | Full-time: 75% (n = 15) | Full-time: 91% (n = 29) | n.s. |
| Part-time: 25% (n = 5) | Part-time: 9% (n = 3) | ||
| Care dependent relatives | 20% (n = 4) | 31% (n = 10) | n.s. |
| Profession | Nursing staff 75% (n = 15) | Nursing staff 78% (n = 25) | n.s. |
| Physicians 25% (n = 5) | Physicians 22% (n = 7) |
| NPC Ward | Neuro Ward | Fisher’s Exact Test | |||||
|---|---|---|---|---|---|---|---|
| Never/ Rarely | Sometimes | Often/ Always | Never/ Rarely | Sometimes | Often/ Always | ||
| Sense of purpose | 0% | 20% | 80% | 6% | 0% | 94% | n.s. |
| Job satisfaction | 5% | 35% | 60% | 9% | 34% | 57% | n.s. |
| Excessive responsibility | 70% | 15% | 15% | 35% | 44% | 22% | p = 0.05 |
| Wish for more responsibilities | 40% | 50% | 10% | 35% | 41% | 25% | n.s. |
| Unmanageable workload | 50% | 20% | 30% | 47% | 13% | 40% | n.s. |
| Interprofessional work meets expectations | 10% | 30% | 60% | 13% | 50% | 37% | n.s. |
| Failing to partake in educational opportunities due to lack of resources | 60% | 25% | 15% | 44% | 22% | 34% | n.s. |
| NPC Ward | Neuro Ward | Fisher’s Exact Test | |||
|---|---|---|---|---|---|
| Not at All/Less Important | (Very) Important | Not at All/Less Important | (Very) Important | ||
| Supervision | 50% | 50% | 44% | 56% | n.s. |
| Rituals | 35% | 65% | 56% | 44% | n.s. |
| The team | 0% | 100% | 16% | 84% | n.s. |
| Family | 15% | 85% | 19% | 81% | n.s. |
| Private life | 10% | 90% | 22% | 78% | n.s. |
| Sports | 45% | 55% | 31% | 69% | n.s. |
| Distraction | 35% | 65% | 37% | 63% | n.s. |
| Humor | 15% | 85% | 12% | 88% | n.s. |
| Worldview/Faith | 50% | 50% | 53% | 47% | n.s. |
| Empathy of others | 45% | 55% | 47% | 53% | n.s. |
| Experiencing nature/walks/hikes | 25% | 75% | 37% | 63% | n.s. |
| Meeting friends | 20% | 80% | 19% | 81% | n.s. |
| Offers for self-care | 55% | 45% | 47% | 53% | n.s. |
| Team activities, e.g., excursions, gatherings, team sports | 55% | 45% | 47% | 53% | n.s. |
| NPC Ward | Neuro Ward | Fisher’s Exact Test | |
|---|---|---|---|
| (A) Changes in palliative care attitude | |||
| Changed | 25% (n = 5) | 22% (n = 7) | n.s. |
| Unchanged | 55% (n = 11) | 66% (n = 21) | |
| Indecisive | 20% (n = 4) | 13% (n = 4) | |
| (B) Expected team sustainability | |||
| Few weeks | 0% (n = 0) | 3% (n = 1) | |
| Few months | 15% (n = 3) | 25% (n = 8) | n.s. |
| Few years | 35% (n = 7) | 44% (n = 14) | |
| Many years | 50% (n = 10) | 28% (n = 9) | |
| (C) Changes in working conditions since employment | |||
| (Strongly) improved | 45% (n = 9) | 19% (n = 6) | p = 0.033 * |
| Unchanged | 40% (n = 8) | 56% (n = 18) | |
| (Strongly) worsened | 15% (n = 3) | 25% (n = 8) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herwest, S.; Kuhlmann, S.L.; Willert, A.-C.; Ploner, C.J.; Kowski, A.B. Burdens and Resources of Staff of a Specialized Ward for Neuropalliative Care: A Cross-Sectional Survey. Brain Sci. 2022, 12, 1697. https://doi.org/10.3390/brainsci12121697
Herwest S, Kuhlmann SL, Willert A-C, Ploner CJ, Kowski AB. Burdens and Resources of Staff of a Specialized Ward for Neuropalliative Care: A Cross-Sectional Survey. Brain Sciences. 2022; 12(12):1697. https://doi.org/10.3390/brainsci12121697
Chicago/Turabian StyleHerwest, Sarah, Stella Linnea Kuhlmann, Anna-Christin Willert, Christoph Johannes Ploner, and Alexander Bernhard Kowski. 2022. "Burdens and Resources of Staff of a Specialized Ward for Neuropalliative Care: A Cross-Sectional Survey" Brain Sciences 12, no. 12: 1697. https://doi.org/10.3390/brainsci12121697
APA StyleHerwest, S., Kuhlmann, S. L., Willert, A.-C., Ploner, C. J., & Kowski, A. B. (2022). Burdens and Resources of Staff of a Specialized Ward for Neuropalliative Care: A Cross-Sectional Survey. Brain Sciences, 12(12), 1697. https://doi.org/10.3390/brainsci12121697