


Is the Zero-P Spacer Suitable for 3-Level Anterior Cervical Discectomy and Fusion Surgery in Terms of Sagittal Alignment Reconstruction: A Comparison Study with Traditional Plate and Cage System
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bakhsheshian, J.; Mehta, V.A.; Liu, J.C. Current Diagnosis and Management of Cervical Spondylotic Myelopathy. Glob. Spine J. 2017, 7, 572–586. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Kuo, C.H.; Cheng, C.M.; Wu, J.C. Recent advances in the management of cervical spondylotic myelopathy: Bibliometric analysis and surgical perspectives. J. Neurosurg. Spine 2019, 31, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.W.; Robinson, R.A. The treatment of certain cervical-spine disorders by anterior removal of the intervertebral disc and interbody fusion. J. Bone Jt. Surg. Am. 1958, 40-A, 607–624. [Google Scholar] [CrossRef]
- Cloward, R.B. The anterior approach for removal of ruptured cervical disks. J. Neurosurg. 1958, 15, 602–617. [Google Scholar] [CrossRef] [PubMed]
- Fountas, K.N.; Kapsalaki, E.Z.; Nikolakakos, L.G.; Smisson, H.F.; Johnston, K.W.; Grigorian, A.A.; Lee, G.P.; Robinson, J.S., Jr. Anterior cervical discectomy and fusion associated complications. Spine 2007, 32, 2310–2317. [Google Scholar] [CrossRef] [PubMed]
- Oliver, J.D.; Goncalves, S.; Kerezoudis, P.; Alvi, M.A.; Freedman, B.A.; Nassr, A.; Bydon, M. Comparison of Outcomes for Anterior Cervical Discectomy and Fusion With and Without Anterior Plate Fixation: A Systematic Review and Meta-Analysis. Spine 2018, 43, E413–E422. [Google Scholar] [CrossRef]
- Kaiser, M.G.; Haid, R.W., Jr.; Subach, B.R.; Barnes, B.; Rodts, G.E., Jr. Anterior cervical plating enhances arthrodesis after discectomy and fusion with cortical allograft. Neurosurgery 2002, 50, 229–236, Discussion 236–238. [Google Scholar] [CrossRef]
- Song, K.J.; Taghavi, C.E.; Lee, K.B.; Song, J.H.; Eun, J.P. The efficacy of plate construct augmentation versus cage alone in anterior cervical fusion. Spine 2009, 34, 2886–2892. [Google Scholar] [CrossRef]
- Fraser, J.F.; Hartl, R. Anterior approaches to fusion of the cervical spine: A metaanalysis of fusion rates. J. Neurosurg. Spine 2007, 6, 298–303. [Google Scholar] [CrossRef]
- Niu, C.C.; Liao, J.C.; Chen, W.J.; Chen, L.H. Outcomes of interbody fusion cages used in 1 and 2-levels anterior cervical discectomy and fusion: Titanium cages versus polyetheretherketone (PEEK) cages. J. Spinal Disord. Tech. 2010, 23, 310–316. [Google Scholar] [CrossRef]
- Barbagallo, G.M.; Romano, D.; Certo, F.; Milone, P.; Albanese, V. Zero-P: A new zero-profile cage-plate device for single and multilevel ACDF. A single institution series with four years maximum follow-up and review of the literature on zero-profile devices. Eur. Spine J. 2013, 22 (Suppl. S6), S868–S878. [Google Scholar] [CrossRef] [PubMed]
- Xiao, S.; Liang, Z.; Wei, W.; Ning, J. Zero-profile anchored cage reduces risk of postoperative dysphagia compared with cage with plate fixation after anterior cervical discectomy and fusion. Eur. Spine J. 2017, 26, 975–984. [Google Scholar] [CrossRef] [PubMed]
- Hofstetter, C.P.; Kesavabhotla, K.; Boockvar, J.A. Zero-profile Anchored Spacer Reduces Rate of Dysphagia Compared with ACDF with Anterior Plating. J. Spinal Disord. Tech. 2015, 28, E284–E290. [Google Scholar] [CrossRef] [PubMed]
- Scholz, M.; Schleicher, P.; Pabst, S.; Kandziora, F. A zero-profile anchored spacer in multilevel cervical anterior interbody fusion: Biomechanical comparison to established fixation techniques. Spine 2015, 40, E375–E380. [Google Scholar] [CrossRef]
- Li, Y.; Hao, D.; He, B.; Wang, X.; Yan, L. The Efficiency of Zero-profile Implant in Anterior Cervical Discectomy Fusion: A Prospective Controlled Long-term Follow-up Study. J. Spinal Disord. Tech. 2015, 28, 398–403. [Google Scholar] [CrossRef]
- Chen, Y.; Chen, H.; Cao, P.; Yuan, W. Anterior cervical interbody fusion with the Zero-P spacer: Mid-term results of two-level fusion. Eur. Spine J. 2015, 24, 1666–1672. [Google Scholar] [CrossRef]
- Wang, C.; Zhang, Y.; Yuan, W. Early Clinical Outcomes and Radiographic Features After Treatment of Cervical Degenerative Disk Disease With the New Zero-Profile Implant: A 1-Year Follow-up Retrospective Study. Clin. Spine Surg. 2016, 29, E73–E79. [Google Scholar] [CrossRef]
- Wang, Z.; Jiang, W.; Li, X.; Wang, H.; Shi, J.; Chen, J.; Meng, B.; Yang, H. The application of zero-profile anchored spacer in anterior cervical discectomy and fusion. Eur. Spine J. 2015, 24, 148–154. [Google Scholar] [CrossRef]
- Yun, D.J.; Lee, S.J.; Park, S.J.; Oh, H.S.; Lee, Y.J.; Oh, H.M.; Lee, S.H. Use of a Zero-Profile Device for Contiguous 2-Level Anterior Cervical Diskectomy and Fusion: Comparison with Cage with Plate Construct. World Neurosurg. 2017, 97, 189–198. [Google Scholar] [CrossRef]
- Lee, Y.S.; Kim, Y.B.; Park, S.W. Does a zero-profile anchored cage offer additional stabilization as anterior cervical plate? Spine 2015, 40, E563–E570. [Google Scholar] [CrossRef]
- Albanese, V.; Certo, F.; Visocchi, M.; Barbagallo, G.M.V. Multilevel Anterior Cervical Diskectomy and Fusion with Zero-Profile Devices: Analysis of Safety and Feasibility, with Focus on Sagittal Alignment and Impact on Clinical Outcome: Single-Institution Experience and Review of Literature. World Neurosurg. 2017, 106, 724–735. [Google Scholar] [CrossRef] [PubMed]
- Vanek, P.; Bradac, O.; Delacy, P.; Lacman, J.; Benes, V. Anterior interbody fusion of the cervical spine with Zero-P spacer: Prospective comparative study-clinical and radiological results at a minimum 2 years after surgery. Spine 2013, 38, E792–E797. [Google Scholar] [CrossRef] [PubMed]
- Tong, M.J.; Xiang, G.H.; He, Z.L.; Chen, D.H.; Tang, Q.; Xu, H.Z.; Tian, N.F. Zero-Profile Spacer Versus Cage-Plate Construct in Anterior Cervical Diskectomy and Fusion for Multilevel Cervical Spondylotic Myelopathy: Systematic Review and Meta-Analysis. World Neurosurg. 2017, 104, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Miao, J.; Shen, Y.; Kuang, Y.; Yang, L.; Wang, X.; Chen, Y.; Chen, D. Early follow-up outcomes of a new zero-profile implant used in anterior cervical discectomy and fusion. J. Spinal Disord. Tech. 2013, 26, E193–E197. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Feng, H.; Lan, Z.; Lai, J.; Sun, Z.; Wang, Y.; Wang, J.; Ren, Z.; Huang, F.; Xu, F. A Randomized Trial Comparing Clinical Outcomes Between Zero-Profile and Traditional Multilevel Anterior Cervical Discectomy and Fusion Surgery for Cervical Myelopathy. Spine 2018, 43, E259–E266. [Google Scholar] [CrossRef]
- Duan, Y.; Yang, Y.; Wang, Y.; Liu, H.; Hong, Y.; Gong, Q.; Song, Y. Comparison of anterior cervical discectomy and fusion with the zero-profile device versus plate and cage in treating cervical degenerative disc disease: A meta-analysis. J. Clin. Neurosci. 2016, 33, 11–18. [Google Scholar] [CrossRef]
- Chen, Y.; Chen, H.; Wu, X.; Wang, X.; Lin, W.; Yuan, W. Comparative analysis of clinical outcomes between zero-profile implant and cages with plate fixation in treating multilevel cervical spondilotic myelopathy: A three-year follow-up. Clin. Neurol. Neurosurg. 2016, 144, 72–76. [Google Scholar] [CrossRef]
- Chen, Y.; Liu, Y.; Chen, H.; Cao, P.; Yuan, W. Comparison of Curvature Between the Zero-P Spacer and Traditional Cage and Plate After 3-Level Anterior Cervical Discectomy and Fusion: Mid-term Results. Clin. Spine Surg. 2017, 30, E1111–E1116. [Google Scholar] [CrossRef]
- Sun, B.; Shi, C.; Wu, H.; Xu, Z.; Lin, W.; Shen, X.; Wu, X.D.; Zhang, Y.; Yuan, W. Application of Zero-profile Spacer in the Treatment of Three-level Cervical Spondylotic Myelopathy: 5-year Follow-up Results. Spine 2020, 45, 504–511. [Google Scholar] [CrossRef]
- Xiao, B.; Wu, B.; Rong, T.; Cui, W.; Sang, D.; Liu, B. Clinical impact of 3-level anterior cervical decompression and fusion (ACDF) on the occipito-atlantoaxial complex: A retrospective study of patients who received a zero-profile anchored spacer versus cage-plate construct. Eur. Spine J. 2021, 30, 3656–3665. [Google Scholar] [CrossRef]
- Rhee, J.M.; Chapman, J.R.; Norvell, D.C.; Smith, J.; Sherry, N.A.; Riew, K.D. Radiological Determination of Postoperative Cervical Fusion: A Systematic Review. Spine 2015, 40, 974–991. [Google Scholar] [CrossRef] [PubMed]
- Robertson, J.T.; Papadopoulos, S.M.; Traynelis, V.C. Assessment of adjacent-segment disease in patients treated with cervical fusion or arthroplasty: A prospective 2-year study. J. Neurosurg. Spine 2005, 3, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Pitzen, T.R.; Chrobok, J.; Stulik, J.; Ruffing, S.; Drumm, J.; Sova, L.; Kucera, R.; Vyskocil, T.; Steudel, W.I. Implant complications, fusion, loss of lordosis, and outcome after anterior cervical plating with dynamic or rigid plates: Two-year results of a multi-centric, randomized, controlled study. Spine 2009, 34, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Azimi, P.; Yazdanian, T.; Benzel, E.C.; Hai, Y.; Montazeri, A. Sagittal balance of the cervical spine: A systematic review and meta-analysis. Eur. Spine J. 2021, 30, 1411–1439. [Google Scholar] [CrossRef] [PubMed]
- Scheer, J.K.; Tang, J.A.; Smith, J.S.; Acosta, F.L., Jr.; Protopsaltis, T.S.; Blondel, B.; Bess, S.; Shaffrey, C.I.; Deviren, V.; Lafage, V.; et al. Cervical spine alignment, sagittal deformity, and clinical implications: A review. J. Neurosurg. Spine 2013, 19, 141–159. [Google Scholar] [CrossRef]
- Riley, L.H., 3rd; Skolasky, R.L.; Albert, T.J.; Vaccaro, A.R.; Heller, J.G. Dysphagia after anterior cervical decompression and fusion: Prevalence and risk factors from a longitudinal cohort study. Spine 2005, 30, 2564–2569. [Google Scholar] [CrossRef]
- Pinder, E.M.; Sharp, D.J. Cage subsidence after anterior cervical discectomy and fusion using a cage alone or combined with anterior plate fixation. J. Orthop. Surg. 2016, 24, 97–100. [Google Scholar] [CrossRef]
- Lee, C.H.; Hyun, S.J.; Kim, M.J.; Yeom, J.S.; Kim, W.H.; Kim, K.J.; Jahng, T.A.; Kim, H.J.; Yoon, S.H. Comparative analysis of 3 different construct systems for single-level anterior cervical discectomy and fusion: Stand-alone cage, iliac graft plus plate augmentation, and cage plus plating. J. Spinal Disord. Tech. 2013, 26, 112–118. [Google Scholar] [CrossRef]
- Kwon, W.K.; Kim, P.S.; Ahn, S.Y.; Song, J.Y.; Kim, J.H.; Park, Y.K.; Kwon, T.H.; Moon, H.J. Analysis of Associating Factors With C2-7 Sagittal Vertical Axis After Two-level Anterior Cervical Fusion: Comparison Between Plate Augmentation and Stand-alone Cages. Spine 2017, 42, 318–325. [Google Scholar] [CrossRef]
- Fujibayashi, S.; Neo, M.; Nakamura, T. Stand-alone interbody cage versus anterior cervical plate for treatment of cervical disc herniation: Sequential changes in cage subsidence. J. Clin. Neurosci. 2008, 15, 1017–1022. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Symptom Severity | Liquid Food | Solid Food |
|---|---|---|
| None | None | None |
| Mild | None | Rare |
| Moderate | None or rare | Occasionally (only with specific food) |
| Severe | None or rare | Frequent (majority of solids) |
| Variables | Group ZP (Zero-P) | Group PC (Plate & Cage) | P |
|---|---|---|---|
| No. | 23 | 21 | - |
| Sex (M/F) | 13/10 | 11/10 | 0.783 |
| Age (y) | 50.3 ± 6.8 | 49.5 ± 7.7 | 0.546 |
| Operation time (min) | 112.5 ± 15.1 | 117.3 ± 18.6 | 0.117 |
| Blood loss (mL) | 82.4 ± 11.7 | 88.9 ± 14.1 | 0.169 |
| FU time (mo) | 30.1 ± 4.4 | 31.4 ± 5.1 | 0.223 |
| Fused segments | |||
| C3-C6 | 10 | 11 | 0.555 |
| C4-C7 | 13 | 10 |
| Variables | Group ZP | Group PC | P |
|---|---|---|---|
| (Zero-P) | (Plate & Cage) | ||
| JOA score | |||
| Preop | 8.8 ± 0.8 | 9.1 ± 0.9 | 0.743 |
| 3-mo Postop | 13.3 ± 1.1 | 13.1 ± 0.9 | 0.811 |
| Last FU | 14.1 ± 1.3 | 13.9 ± 1.0 | 0.636 |
| NDI score | |||
| Preop | 13.5 ± 2.6 | 13.8 ± 2.1 | 0.677 |
| 3-mo Postop | 5.5 ± 1.4 | 5.8 ± 1.1 | 0.725 |
| Last FU | 7.1 ± 2.1 | 7.7 ± 1.8 | 0.554 |
| Dysphagia | |||
| 48-h | 8/23 (34.8%) | 8/21 (38.1%) | 0.82 |
| 3-mo | 1/23 (4.3%) | 6/21 (28.6%) | 0.028 |
| 6-mo | 0/23 (0%) | 4/21 (19.0%) | 0.028 |
| Variables | Group ZP | Group PC | P |
|---|---|---|---|
| (Zero-P) | (Plate & Cage) | ||
| Fusion rate (24 mo) | 21/23(91.3%) | 20/21(95.2%) | 0.605 |
| ASD (24 mo) | 3/23(13.0%) | 3/21(14.3%) | 0.905 |
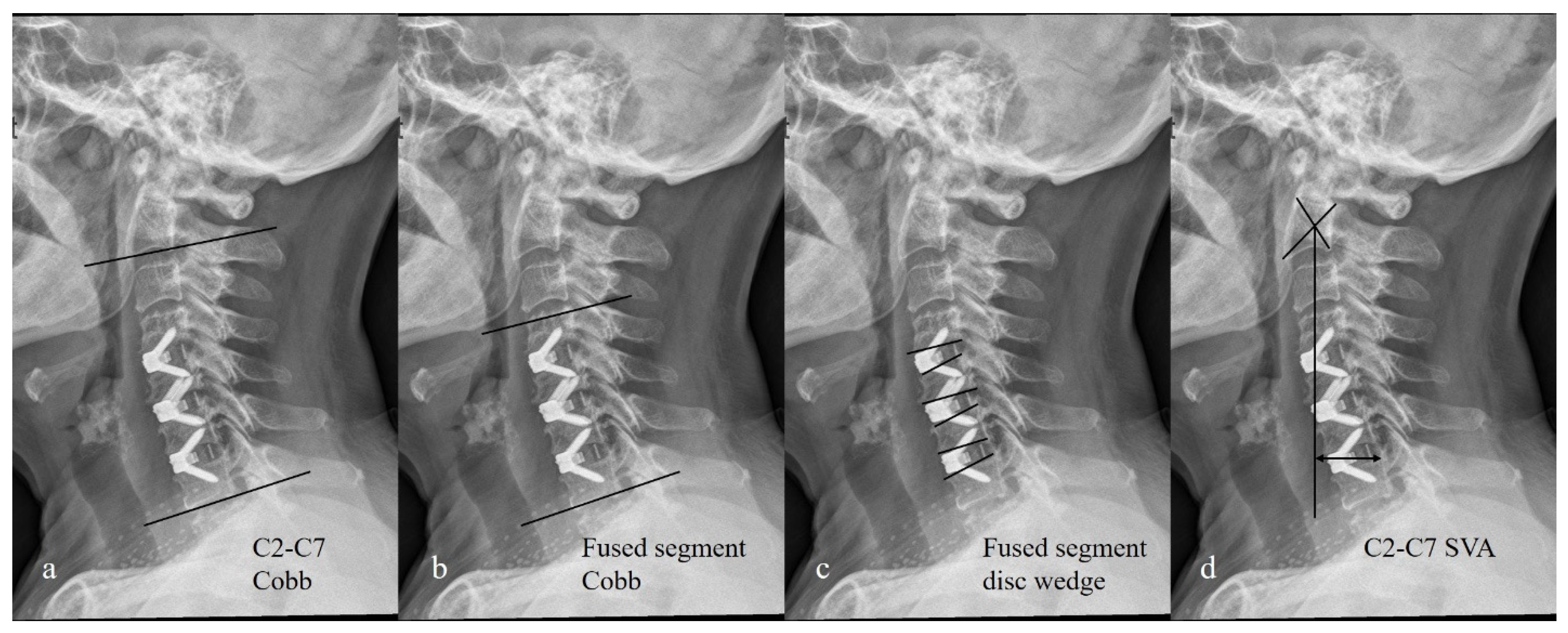
| C2-C7 Cobb (°) | |||
| Preop | 10.8 ± 8.1 | 11.1 ± 7.9 | 0.331 |
| Postop | 15.7 ± 7.4 | 24.8 ± 8.1 | 0.011 |
| Last FU | 12.5 ± 5.7 | 18.6 ± 6.9 | 0.023 |
| Fused segment Cobb (°) | |||
| Preop | 6.1 ± 6.8 | 5.9 ± 7.9 | 0.667 |
| Postop | 12.4 ± 7.1 | 19.8 ± 8.2 | 0.014 |
| Last FU | 9.5 ± 6.6 | 13.9 ± 7.4 | 0.025 |
| Fused segment disc wedge (°) | |||
| Preop | 5.8 ± 5.1 | 6.1 ± 6.9 | 0.564 |
| Postop | 11.3 ± 7.2 | 18.1 ± 7.9 | 0.012 |
| Last FU | 8.1 ± 6.8 | 13.6 ± 7.5 | 0.021 |
| C2-C7 SVA (mm) | |||
| Preop | 28.4 ± 11.3 | 30.1 ± 14.4 | 0.248 |
| Postop | 30.2 ± 14.6 | 28.2 ± 15.7 | 0.145 |
| Last FU | 31.7 ± 13.9 | 29.6 ± 16.5 | 0.233 |
| Subgroups | Variables | Group ZP | Group PC | P |
|---|---|---|---|---|
| (Zero-P) | (Plate & Cage) | |||
| Preop C2-C7 Cobb ≤ 10° | C2-C7 Cobb (°) | |||
| Preop | 4.9 ± 4.1 | 5.2 ± 4.7 | 0.516 | |
| Postop | 9.7 ± 5.8 | 17.8 ± 6.5 | 0.009 | |
| Last FU | 7.6 ± 6.6 | 15.2 ± 8.9 | 0.011 | |
| Fused segment Cobb (°) | ||||
| Preop | 3.1 ± 3.8 | 2.9 ± 3.9 | 0.712 | |
| Postop | 8.3 ± 6.5 | 14.8 ± 7.6 | 0.01 | |
| Last FU | 6.4 ± 5.7 | 13.1 ± 7.0 | 0.013 | |
| Fused segment disc wedge (°) | ||||
| Preop | 2.8 ± 3.1 | 3.0 ± 2.9 | 0.411 | |
| Postop | 7.5 ± 4.2 | 12.7 ± 4.9 | 0.015 | |
| Last FU | 5.5 ± 3.9 | 11.0 ± 5.5 | 0.008 | |
| Preop C2-C7 Cobb > 10° | C2-C7 Cobb (°) | |||
| Preop | 15.8 ± 6.2 | 16.0 ± 5.9 | 0.451 | |
| Postop | 24.7 ± 11.7 | 28.8 ± 10.3 | 0.092 | |
| Last FU | 21.1 ± 10.3 | 23.5 ± 11.6 | 0.121 | |
| Fused segment Cobb (°) | ||||
| Preop | 10.6 ± 4.1 | 11.9 ± 5.0 | 0.685 | |
| Postop | 18.8 ± 5.1 | 22.3 ± 6.2 | 0.146 | |
| Last FU | 15.9 ± 6.0 | 17.3 ± 8.8 | 0.083 | |
| Fused segment disc wedge (°) | ||||
| Preop | 8.8 ± 5.3 | 9.1 ± 6.3 | 0.541 | |
| Postop | 17.3 ± 6.1 | 20.1 ± 5.8 | 0.089 | |
| Last FU | 14.1 ± 5.8 | 15.3 ± 6.6 | 0.107 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, J.; Jin, W.; Shi, Y.; Guan, Z.; Wen, J.; Huang, Y.; Yu, B. Is the Zero-P Spacer Suitable for 3-Level Anterior Cervical Discectomy and Fusion Surgery in Terms of Sagittal Alignment Reconstruction: A Comparison Study with Traditional Plate and Cage System. Brain Sci. 2022, 12, 1583. https://doi.org/10.3390/brainsci12111583
Guo J, Jin W, Shi Y, Guan Z, Wen J, Huang Y, Yu B. Is the Zero-P Spacer Suitable for 3-Level Anterior Cervical Discectomy and Fusion Surgery in Terms of Sagittal Alignment Reconstruction: A Comparison Study with Traditional Plate and Cage System. Brain Sciences. 2022; 12(11):1583. https://doi.org/10.3390/brainsci12111583
Chicago/Turabian StyleGuo, Jing, Weiming Jin, Yan Shi, Zhiping Guan, Jian Wen, Yongcan Huang, and Binsheng Yu. 2022. "Is the Zero-P Spacer Suitable for 3-Level Anterior Cervical Discectomy and Fusion Surgery in Terms of Sagittal Alignment Reconstruction: A Comparison Study with Traditional Plate and Cage System" Brain Sciences 12, no. 11: 1583. https://doi.org/10.3390/brainsci12111583
APA StyleGuo, J., Jin, W., Shi, Y., Guan, Z., Wen, J., Huang, Y., & Yu, B. (2022). Is the Zero-P Spacer Suitable for 3-Level Anterior Cervical Discectomy and Fusion Surgery in Terms of Sagittal Alignment Reconstruction: A Comparison Study with Traditional Plate and Cage System. Brain Sciences, 12(11), 1583. https://doi.org/10.3390/brainsci12111583