

Childhood Trauma and Dissociation Correlates in Alcohol Use Disorder: A Cross-Sectional Study in a Sample of 587 French Subjects Hospitalized in a Rehabilitation Center
 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Setting and Participants
2.2. Measures
2.2.1. Sociodemographic Data
2.2.2. Childhood Trauma
2.2.3. Dissociative Experiences
2.2.4. Alcohol Use Disorder
2.2.5. Depressive Symptoms
2.2.6. Anxiety Symptoms
2.2.7. Posttraumatic Symptoms
2.3. Statistical Analyses
2.4. Ethics
3. Results
Characteristics of the Participants
Clinical Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults: The Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef]
- Chapman, D.P.; Whitfield, C.L.; Felitti, V.J.; Dube, S.R.; Edwards, V.J.; Anda, R.F. Adverse Childhood Experiences and the Risk of Depressive Disorders in Adulthood. J. Affect. Disord. 2004, 82, 217–225. [Google Scholar] [CrossRef]
- Mandelli, L.; Petrelli, C.; Serretti, A. The Role of Specific Early Trauma in Adult Depression: A Meta-Analysis of Published Literature. Childhood Trauma and Adult Depression. Eur. Psychiatry 2015, 30, 665–680. [Google Scholar] [CrossRef]
- Gibb, B.E.; Chelminski, I.; Zimmerman, M. Childhood Emotional, Physical, and Sexual Abuse, and Diagnoses of Depressive and Anxiety Disorders in Adult Psychiatric Outpatients. Depress. Anxiety 2007, 24, 256–263. [Google Scholar] [CrossRef]
- Kendler, K.S.; Bulik, C.M.; Silberg, J.; Hettema, J.M.; Myers, J.; Prescott, C.A. Childhood Sexual Abuse and Adult Psychiatric and Substance Use Disorders in Women: An Epidemiological and Cotwin Control Analysis. Arch. Gen. Psychiatry 2000, 57, 953–959. [Google Scholar] [CrossRef]
- Taillieu, T.L.; Brownridge, D.A.; Sareen, J.; Afifi, T.O. Childhood Emotional Maltreatment and Mental Disorders: Results from a Nationally Representative Adult Sample from the United States. Child Abus. Negl. 2016, 59, 1–12. [Google Scholar] [CrossRef]
- Vonderlin, R.; Kleindienst, N.; Alpers, G.W.; Bohus, M.; Lyssenko, L.; Schmahl, C. Dissociation in Victims of Childhood Abuse or Neglect: A Meta-Analytic Review. Psychol. Med. 2018, 48, 2467–2476. [Google Scholar] [CrossRef]
- Konkolÿ Thege, B.; Horwood, L.; Slater, L.; Tan, M.C.; Hodgins, D.C.; Wild, T.C. Relationship between Interpersonal Trauma Exposure and Addictive Behaviors: A Systematic Review. BMC Psychiatry 2017, 17, 164. [Google Scholar] [CrossRef]
- Anda, R.F.; Whitfield, C.L.; Felitti, V.J.; Chapman, D.; Edwards, V.J.; Dube, S.R.; Williamson, D.F. Adverse Childhood Experiences, Alcoholic Parents, and Later Risk of Alcoholism and Depression. Psychiatr. Serv. 2002, 53, 1001–1009. [Google Scholar] [CrossRef]
- Lee, R.D.; Chen, J. Adverse Childhood Experiences, Mental Health, and Excessive Alcohol Use: Examination of Race/Ethnicity and Sex Differences. Child Abus. Negl. 2017, 69, 40–48. [Google Scholar] [CrossRef]
- Rehan, W.; Antfolk, J.; Johansson, A.; Jern, P.; Santtila, P. Experiences of Severe Childhood Maltreatment, Depression, Anxiety and Alcohol Abuse among Adults in Finland. PLoS ONE 2017, 12, e0177252. [Google Scholar] [CrossRef]
- Lotzin, A.; Haupt, L.; von Schönfels, J.; Wingenfeld, K.; Schäfer, I. Profiles of Childhood Trauma in Patients with Alcohol Dependence and Their Associations with Addiction-Related Problems. Alcohol. Clin. Exp. Res. 2016, 40, 543–552. [Google Scholar] [CrossRef]
- Grundmann, J.; Lincoln, T.M.; Lüdecke, D.; Bong, S.; Schulte, B.; Verthein, U.; Schäfer, I. Traumatic Experiences, Revictimization and Posttraumatic Stress Disorder in German Inpatients Treated for Alcohol Dependence. Subst. Use Misuse 2018, 53, 677–685. [Google Scholar] [CrossRef]
- Anne Lown, E.; Nayak, M.B.; Korcha, R.A.; Greenfield, T.K. Child Physical and Sexual Abuse: A Comprehensive Look at Alcohol Consumption Patterns, Consequences, and Dependence from the National Alcohol Survey. Alcohol. Clin. Exp. Res. 2011, 35, 317–325. [Google Scholar] [CrossRef]
- Widom, C.S.; White, H.R.; Czaja, S.J.; Marmorstein, N.R. Long-Term Effects of Child Abuse and Neglect on Alcohol Use and Excessive Drinking in Middle Adulthood. J. Stud. Alcohol Drugs 2007, 68, 317–326. [Google Scholar] [CrossRef]
- Evren, C.; Sar, V.; Dalbudak, E.; Oncu, F.; Cakmak, D. Social Anxiety and Dissociation among Male Patients with Alcohol Dependency. Psychiatry Res. 2009, 165, 273–280. [Google Scholar] [CrossRef]
- Grayson, C.E.; Nolen-Hoeksema, S. Motives to Drink as Mediators between Childhood Sexual Assault and Alcohol Problems in Adult Women. J. Trauma. Stress 2005, 18, 137–145. [Google Scholar] [CrossRef]
- Mezquita, L.; Ibáñez, M.I.; Moya, J.; Villa, H.; Ortet, G. A Longitudinal Examination of Different Etiological Pathways to Alcohol Use and Misuse. Alcohol. Clin. Exp. Res. 2014, 38, 1770–1779. [Google Scholar] [CrossRef]
- Ertl, V.; Saile, R.; Neuner, F.; Catani, C. Drinking to Ease the Burden: A Cross-Sectional Study on Trauma, Alcohol Abuse and Psychopathology in a Post-Conflict Context. BMC Psychiatry 2016, 16, 202. [Google Scholar] [CrossRef]
- Evren, C.; Sar, V.; Karadag, F.; Tamar Gurol, D.; Karagoz, M. Dissociative Disorders among Alcohol-Dependent Inpatients. Psychiatry Res. 2007, 152, 233–241. [Google Scholar] [CrossRef]
- Schäfer, I.; Langeland, W.; Hissbach, J.; Luedecke, C.; Ohlmeier, M.D.; Chodzinski, C.; Kemper, U.; Keiper, P.; Wedekind, D.; Havemann-Reinecke, U. Childhood Trauma and Dissociation in Patients with Alcohol Dependence, Drug Dependence, or Both—A Multi-Center Study. Drug Alcohol Depend. 2010, 109, 84–89. [Google Scholar] [CrossRef]
- Schäfer, I.; Reininghaus, U.; Langeland, W.; Voss, A.; Zieger, N.; Haasen, C.; Karow, A. Dissociative Symptoms in Alcohol-Dependent Patients: Associations with Childhood Trauma and Substance Abuse Characteristics. Compr. Psychiatry 2007, 48, 539–545. [Google Scholar] [CrossRef]
- Klanecky, A.K.; McChargue, D.E.; Tuliao, A.P. Proposed Pathways to Problematic Drinking via Post-Traumatic Stress Disorder Symptoms, Emotion Dysregulation, and Dissociative Tendencies Following Child/Adolescent Sexual Abuse. J. Addict. Dis. 2016, 35, 180–193. [Google Scholar] [CrossRef]
- Roesler, T.A.; Dafler, C.E. Chemical Dissociation in Adults Sexually Victimized as Children: Alcohol and Drug Use in Adult Survivors. J. Subst. Abus. Treat. 1993, 10, 537–543. [Google Scholar] [CrossRef]
- Somer, E.; Altus, L.; Ginzburg, K. Dissociative Psychopathology among Opioid Use Disorder Patients: Exploring the “Chemical Dissociation” Hypothesis. Compr. Psychiatry 2010, 51, 419–425. [Google Scholar] [CrossRef]
- Hingray, C.; Cohn, A.; Martini, H.; Donné, C.; El-Hage, W.; Schwan, R.; Paille, F. Impact of Trauma on Addiction and Psychopathology Profile in Alcohol-Dependent Women. Eur. J. Trauma Dissociation 2018, 2, 101–107. [Google Scholar] [CrossRef]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 10th ed.; WHO: Geneva, Switzerland, 2016; Available online: https://icd.who.int/browse10/2016/en (accessed on 16 March 2021).
- Bernstein, D.P.; Stein, J.A.; Newcomb, M.D.; Walker, E.; Pogge, D.; Ahluvalia, T.; Stokes, J.; Handelsman, L.; Medrano, M.; Desmond, D.; et al. Development and Validation of a Brief Screening Version of the Childhood Trauma Questionnaire. Child Abus. Negl. 2003, 27, 169–190. [Google Scholar] [CrossRef]
- Paquette, D.; Laporte, L.; Bigras, M.; Zoccolillo, M. Validation de la version française du CTQ et prévalence de l’histoire de maltraitance. St. Ment. Au Québec 2004, 29, 201–220. [Google Scholar] [CrossRef]
- Carlson, E.B.; Putnam, F.W.; Ross, C.A.; Torem, M.; Coons, P.; Dill, D.L.; Loewenstein, R.J.; Braun, B.G. Validity of the Dissociative Experiences Scale in Screening for Multiple Personality Disorder: A Multicenter Study. Am. J. Psychiatry 1993, 150, 1030–1036. [Google Scholar]
- Darves-Bornoz, J.-M.; Degiovanni, A.; Gaillard, P. Validation of a French Version of the Dissociative Experiences Scale in a Rape-Victim Population. Can. J. Psychiatry 1999, 44, 271–275. [Google Scholar] [CrossRef]
- Waller, N.; Putnam, F.W.; Carlson, E.B. Types of Dissociation and Dissociative Types: A Taxometric Analysis of Dissociative Experiences. Psychol. Methods 1996, 1, 300–321. [Google Scholar] [CrossRef]
- Waller, N.G.; Ross, C.A. The Prevalence and Biometric Structure of Pathological Dissociation in the General Population: Taxometric and Behavior Genetic Findings. J. Abnorm. Psychol. 1997, 106, 499–510. [Google Scholar] [CrossRef]
- World Health Organization. AUDIT: The Alcohol Use Disorders Identification Test: Guidelines for Use in Primary Health Care (WHO/MSD/MSB/01.6a). 2001. Available online: https://www.who.int/publications/i/item/WHO-MSD-MSB-01.6a (accessed on 16 March 2021).
- Gache, P.; Michaud, P.; Landry, U.; Accietto, C.; Arfaoui, S.; Wenger, O.; Daeppen, J.-B. The Alcohol Use Disorders Identification Test (AUDIT) as a Screening Tool for Excessive Drinking in Primary Care: Reliability and Validity of a French Version. Alcohol. Clin. Exp. Res. 2005, 29, 2001–2007. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Ball, R.; Ranieri, W. Comparison of Beck Depression Inventories -IA and -II in Psychiatric Outpatients. J. Pers. Assess. 1996, 67, 588–597. [Google Scholar] [CrossRef]
- Collet, L.; Cottraux, J. The Shortened Beck Depression Inventory (13 Items). Study of the Concurrent Validity with the Hamilton Scale and Widlöcher’s Retardation Scale. L’Encéphale 1986, 12, 77–79. [Google Scholar]
- Spielberger, C.; Gorsuch, R.; Lushene, R.; Vagg, P.; Jacobs, G. Manual for the State-Trait Anxiety Inventory (Form Y1–Y2); Consulting Psychologists Press: Palo Alto, CA, USA, 1983; Volume 4. [Google Scholar]
- Gauthier, J.; Bouchard, S. A French-Canadian Adaptation of the Revised Version of Spielberger’s State-Trait Anxiety Inventory. Can. J. Behav. Sci./Rev. Can. Sci. Comport. 1993, 25, 559–578. [Google Scholar] [CrossRef]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef]
- Ashbaugh, A.R.; Houle-Johnson, S.; Herbert, C.; El-Hage, W.; Brunet, A. Psychometric Validation of the English and French Versions of the Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5). PLoS ONE 2016, 11, e0161645. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing. 2021. Available online: https://cran.r-project.org/manuals.html (accessed on 16 March 2021).
- Kassambara, A. (Ed.) HCPC: Hierarchical Clustering on Principal Components. In Practical Guide to Principal Component Methods in R; CreateSpace Independent Publishing Platform: Scotts Valley, CA, USA, 2017; pp. 142–152. [Google Scholar]
- Josse, J.; Husson, F. MissMDA: A Package for Handling Missing Values in Multivariate Data Analysis. J. Stat. Softw. 2016, 70, 1–31. [Google Scholar] [CrossRef]
- Lê, S.; Josse, J.; Husson, F. FactoMineR: An R Package for Multivariate Analysis. J. Stat. Softw. 2008, 25, 1–18. [Google Scholar] [CrossRef]
- Merrick, M.T.; Ports, K.A.; Ford, D.C.; Afifi, T.O.; Gershoff, E.T.; Grogan-Kaylor, A. Unpacking the Impact of Adverse Childhood Experiences on Adult Mental Health. Child Abus. Negl. 2017, 69, 10–19. [Google Scholar] [CrossRef]
- Ostergaard, M.; Seitz, R.; Jatzkowski, L.; Speidel, S.; Höcker, W.; Odenwald, M. Changes of Self-Reported PTSD and Depression Symptoms During Alcohol Detoxification Treatment. J. Dual Diagn. 2019, 15, 123–129. [Google Scholar] [CrossRef]
- Petit, G.; Luminet, O.; Cordovil de Sousa Uva, M.; Monhonval, P.; Leclercq, S.; Spilliaert, Q.; Zammit, F.; Maurage, P.; de Timary, P. Gender Differences in Affects and Craving in Alcohol-Dependence: A Study During Alcohol Detoxification. Alcohol. Clin. Exp. Res. 2017, 41, 421–431. [Google Scholar] [CrossRef]
- Crum, R.M.; La Flair, L.; Storr, C.L.; Green, K.M.; Stuart, E.A.; Alvanzo, A.A.H.; Lazareck, S.; Bolton, J.M.; Robinson, J.; Sareen, J.; et al. Reports of Drinking to Self-Medicate Anxiety Symptoms: Longitudinal Assessment for Subgroups of Individuals with Alcohol Dependence. Depress. Anxiety 2013, 30, 174–183. [Google Scholar] [CrossRef]
- Crum, R.M.; Mojtabai, R.; Lazareck, S.; Bolton, J.M.; Robinson, J.; Sareen, J.; Green, K.M.; Stuart, E.A.; La Flair, L.; Alvanzo, A.A.H.; et al. A Prospective Assessment of Reports of Drinking to Self-Medicate Mood Symptoms with the Incidence and Persistence of Alcohol Dependence. JAMA Psychiatry 2013, 70, 718–726. [Google Scholar] [CrossRef]
- Karadag, F.; Sar, V.; Tamar-Gurol, D.; Evren, C.; Karagoz, M.; Erkiran, M. Dissociative Disorders among Inpatients with Drug or Alcohol Dependency. J. Clin. Psychiatry 2005, 66, 1247–1253. [Google Scholar] [CrossRef]
- Driessen, M.; Meier, S.; Hill, A.; Wetterling, T.; Lange, W.; Junghanns, K. The Course of Anxiety, Depression and Drinking Behaviours after Completed Detoxification in Alcoholics with and without Comorbid Anxiety and Depressive Disorders. Alcohol Alcohol. 2001, 36, 249–255. [Google Scholar] [CrossRef]
- Boschloo, L.; Vogelzangs, N.; van den Brink, W.; Smit, J.H.; Beekman, A.T.F.; Penninx, B.W.J.H. Predictors of the 2-Year Recurrence and Persistence of Alcohol Dependence. Addiction 2012, 107, 1639–1640. [Google Scholar] [CrossRef]
- Baldwin, J.R.; Reuben, A.; Newbury, J.B.; Danese, A. Agreement Between Prospective and Retrospective Measures of Childhood Maltreatment: A Systematic Review and Meta-Analysis. JAMA Psychiatry 2019, 76, 584–593. [Google Scholar] [CrossRef]
- Fein, G.; Landman, B. Treated and Treatment-Naive Alcoholics Come from Different Populations. Alcohol 2005, 36, 139–146. [Google Scholar] [CrossRef]
- Roberts, N.P.; Roberts, P.A.; Jones, N.; Bisson, J.I. Psychological Therapies for Post-traumatic Stress Disorder and Comorbid Substance Use Disorder. Cochrane Database Syst. Rev. 2016, 4, 1–100. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | LALD (n = 160) | HALD (n = 372) | HAHD (n = 36) | Total |
|---|---|---|---|---|
| Mean (SD)/n (%) | Mean (SD)/n (%) | Mean (SD)/n (%) | Mean (SD)/n (%) | |
| Gender (women) | 29 (18.13%) | 52 (13.98%) | 6 (16.67%) | 87 (15.31%) |
| Age | 45.8 (9.35) | 44.1 (8.87%) | 42.9 (7.83) | 44.51 (8.97) |
| Marital status | ||||
| Single | 45 (28.13%) | 121 (33.24%) | 14 (40.00%) | 180 (31.69%) |
| In a relationship | 65 (40.63%) | 123 (33.79%) | 14 (40.00%) | 202 (35.56%) |
| Widowed, divorced, separated | 50 (31.25%) | 120 (32.98%) | 7 (20.00%) | 177 (31.16%) |
| Highest diploma | ||||
| Certificate of general education | 18 (11.76%) | 63 (18.42%) | 8 (24.24%) | 89 (15.67%) |
| Certificate of technical education | 48 (31.37%) | 114 (33.33%) | 14 (42.42%) | 176 (30.99%) |
| High school diploma | 56 (36.60%) | 90 (26.32%) | 7 (21.21%) | 153 (26.94%) |
| Undergraduate | 15 (9.80%) | 39 (11.40%) | 3 (9.09%) | 57 (10.04%) |
| Postgraduate | 16 (10.46%) | 36 (10.53%) | 1 (3.03%) | 53 (9.33%) |
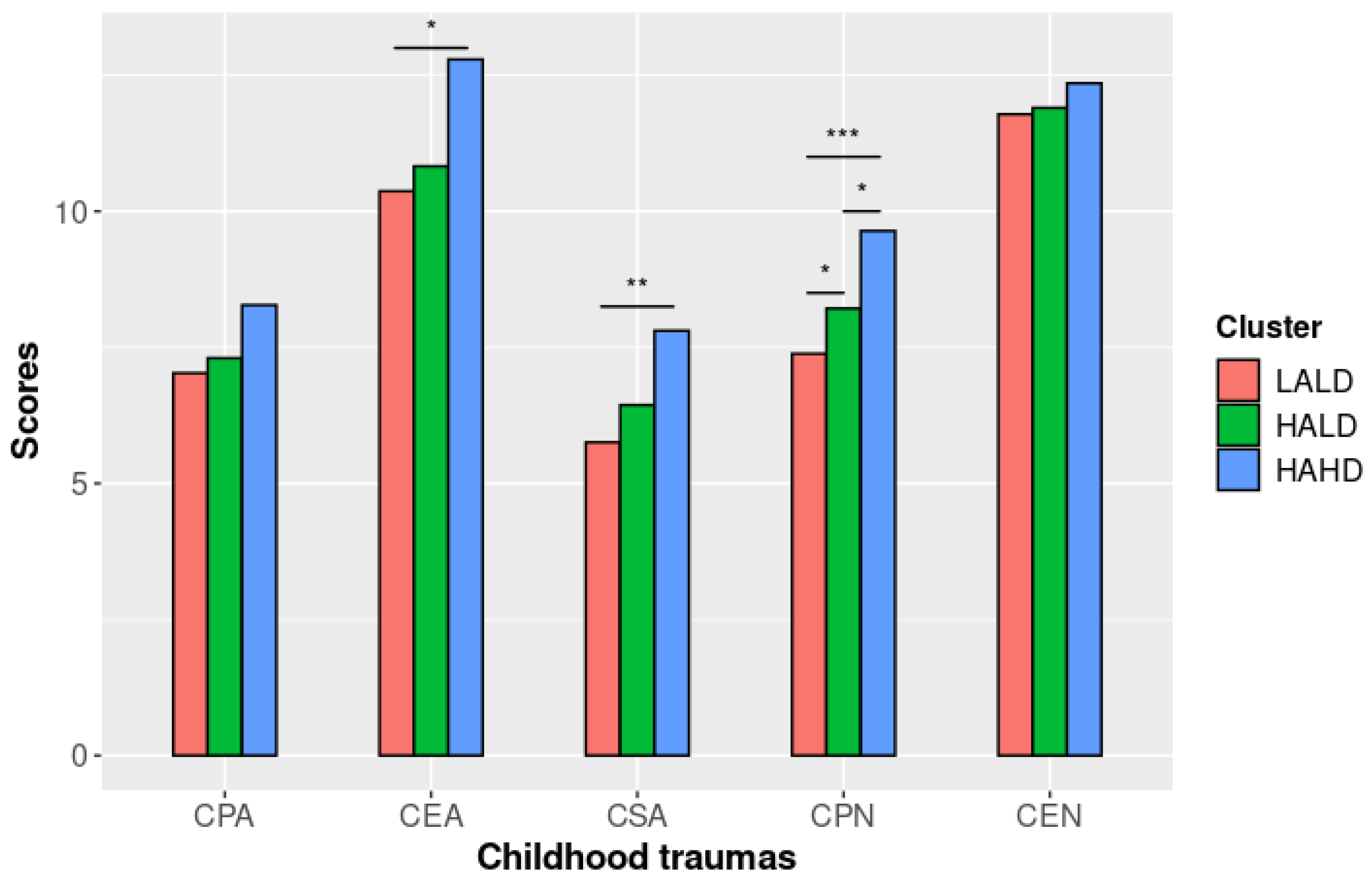
| Childhood trauma | ||||
| Childhood physical abuse (CPA) | 7.03 (3.33) | 7.30 (3.70) | 8.28 (5.38) | 7.28 (3.77) |
| Childhood emotional abuse (CEA) | 10.4 (4.81) | 10.8 (5.40) | 12.8 (6.11) | 10.79 (5.35) |
| Childhood sexual abuse (CSA) | 5.75 (2.32) | 6.44 (3.51) | 7.81 (4.60) | 6.32 (3.37) |
| Childhood physical neglect (CPN) | 7.38 (2.89) | 8.21 (3.26) | 9.64 (3.83) | 8.08 (3.26) |
| Childhood emotional neglect (CEN) | 11.8 (4.92) | 11.9 (5.14) | 12.4 (4.54) | 11.88 (5.07) |
| Clinical variables | ||||
| AUDIT score | 9.22 (6.75) | 28.9 (4.49) | 26.6 (9.49) | 23.22 (10.43) |
| DES-taxon belonging | 0 | 0 | 36 (100%) | 36 (6.34%) |
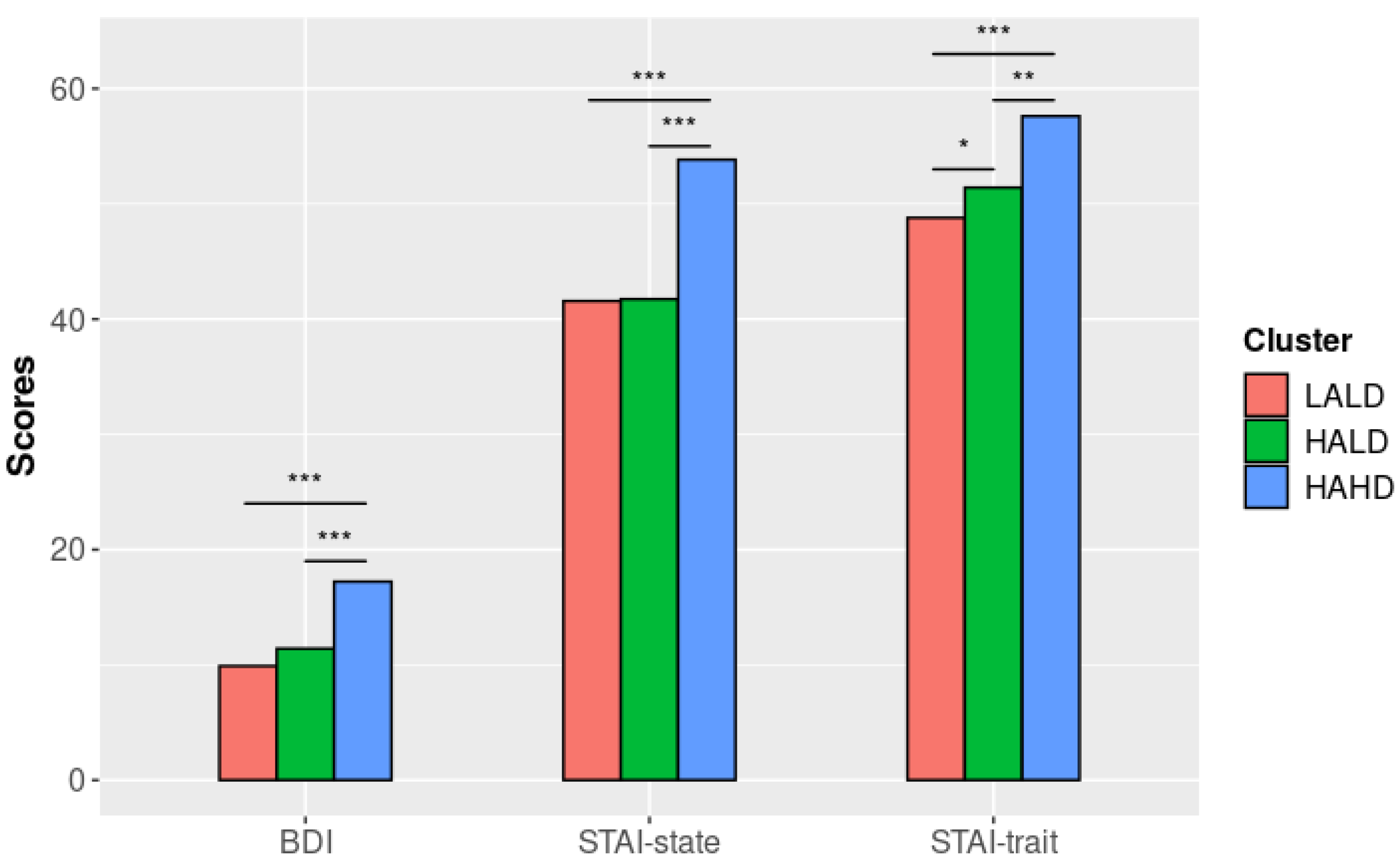
| BDI score | 9.89 (7.44) | 11.4 (7.22) | 17.2 (7.02) | 11.39 (7.46) |
| STAI-state | 41.6 (15.2) | 41.7 (14.1) | 53.8 (13.6) | 42.49 (14.66) |
| STAI-trait | 48.8 (11.4) | 51.4 (10.6) | 57.6 (11.5) | 51.08 (11.11) |
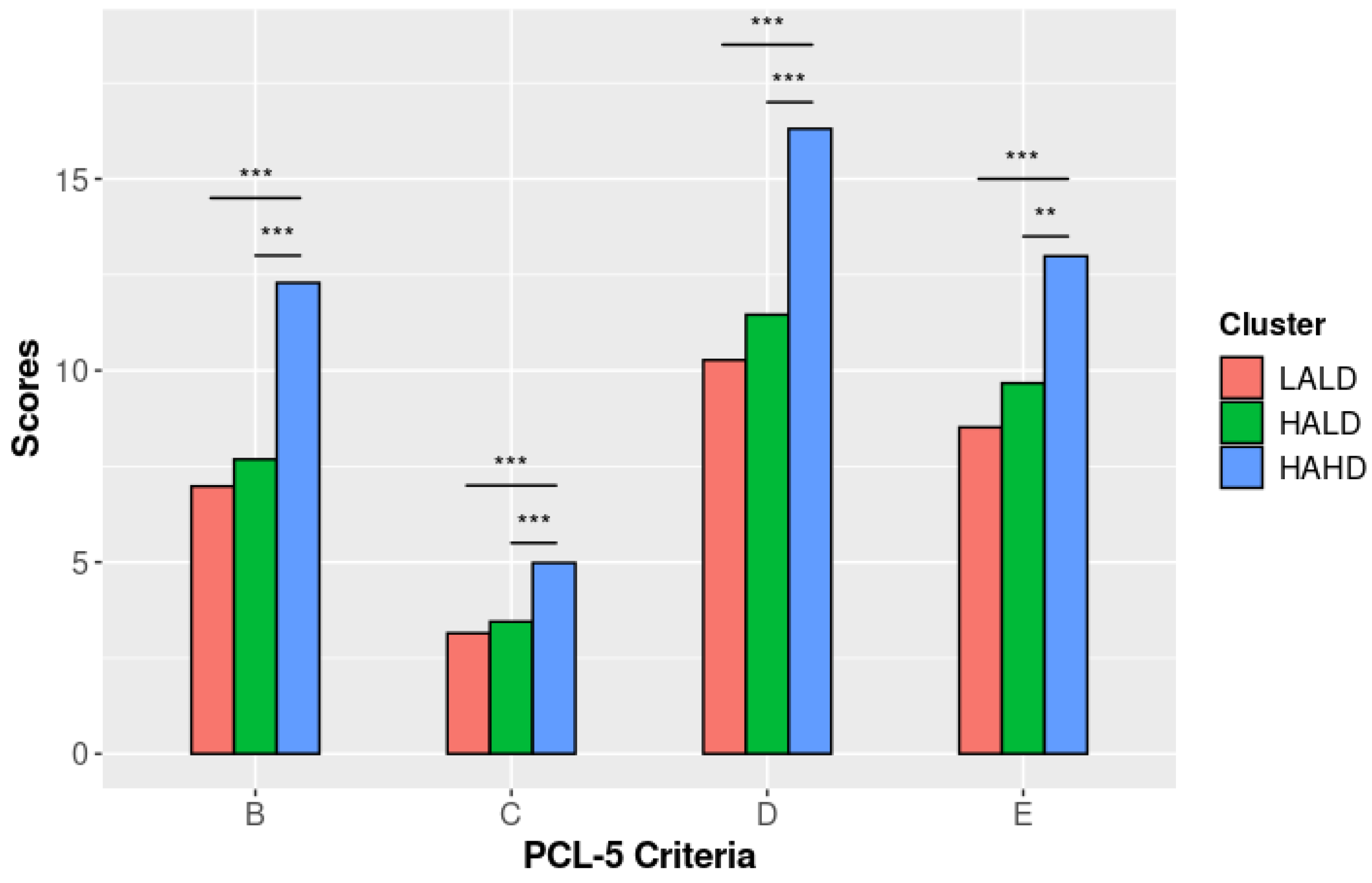
| PCL-5 Criterion B | 6.98 (5.57) | 7.68 (5.28) | 12.3 (4.81) | 7.82 (5.56) |
| PCL-5 Criterion C | 3.15 (2.56) | 3.45 (2.30) | 4.98 (2.01) | 3.48 (2.44) |
| PCL-5 Criterion D | 10.3 (7.40) | 11.5 (6.28) | 16.3 (5.06) | 11.49 (6.77) |
| PCL-5 Criterion E | 8.52 (5.97) | 9.67 (5.39) | 13.0 (5.30) | 9.60 (5.73) |
| Variables | Total Effect | LALD versus HAHD | HALD versus HAHD | LALD versus HALD |
|---|---|---|---|---|
| F (df)p-Value | Est. (SE)p-Value | Est. (SE)p-Value | Est. (SE)p-Value | |
| Childhood trauma | ||||
| Physical abuse a,b,d | 1.09 (2, 562) 0.34 | - | - | - |
| Emotional abuse a,b,c | 3.03 (2, 562) <0.05 | −2.26 (0.92) 0.04 | 1.79 (0.87) 0.09 | 0.47 (0.47) 0.57 |
| Sexual abuse a,b,c,d | 5.75 (2, 561) 0.003 | −1.86 (0.58) 0.004 | −1.21 (0.55) 0.07 | −0.65 (0.30) 0.07 |
| Physical neglect b,c | 8.50 (2, 563) <0.001 | −2.26 (0.59) <0.001 | −1.44 (0.55) 0.03 | −0.82 (0.30) 0.02 |
| Emotional neglect a,b,c,d | 0.12 (2, 561) 0.89 | - | - | - |
| Clinical variables | ||||
| AUDIT score a,b,c,d | 674.67 (2, 561) <0.001 | −17.32 (1.04) <0.001 | 2.19 (0.98) 0.07 | −19.51 (0.53) <0.001 |
| BDI score b,c,d | 15.70 (2, 562) <0.001 | −7.29 (1.30) <0.001 | −5.83 (1.23) <0.001 | −1.45 (0.67) 0.07 |
| STAI-state a,b,c | 12.16 (2, 562) <0.001 | −11.67 (2.57) <0.001 | −11.88 (2.43) <0.001 | −0.21 (1.32) 0.99 |
| STAI-trait a,b,c,d | 11.26 (2, 561) <0.001 | −9.08 (1.97) <0.001 | −6.34 (1.86) 0.002 | −2.74 (1.02) 0.02 |
| PCL-5 Criterion B a,b | 14.34 (2, 563) <0.001 | −5.13 (0.96) <0.001 | −4.43 (0.91) <0.001 | −0.70 (0.49) 0.32 |
| PCL-5 Criterion C b,d | 10.36 (2, 563) <0.001 | −1.94 (0.43) <0.001 | −1.55 (0.40) <0.001 | −0.39 (0.22) 0.16 |
| PCL-5 Criterion D a,b,c | 12.29 (2, 562) <0.001 | −5.84 (1.18) <0.001 | −4.69 (1.11) <0.001 | −1.14 (0.61) 0.14 |
| PCL-5 Criterion E a,b,c | 9.04 (2, 562) <0.001 | −4.16 (0.99) <0.001 | −3.11 (0.93) 0.003 | −1.05 (0.51) 0.10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baudin, G.; Barrault, S.; El Ayoubi, H.; Kazour, F.; Ballon, N.; Maugé, D.; Hingray, C.; Brunault, P.; El-Hage, W. Childhood Trauma and Dissociation Correlates in Alcohol Use Disorder: A Cross-Sectional Study in a Sample of 587 French Subjects Hospitalized in a Rehabilitation Center. Brain Sci. 2022, 12, 1483. https://doi.org/10.3390/brainsci12111483
Baudin G, Barrault S, El Ayoubi H, Kazour F, Ballon N, Maugé D, Hingray C, Brunault P, El-Hage W. Childhood Trauma and Dissociation Correlates in Alcohol Use Disorder: A Cross-Sectional Study in a Sample of 587 French Subjects Hospitalized in a Rehabilitation Center. Brain Sciences. 2022; 12(11):1483. https://doi.org/10.3390/brainsci12111483
Chicago/Turabian StyleBaudin, Grégoire, Servane Barrault, Hussein El Ayoubi, François Kazour, Nicolas Ballon, Damien Maugé, Coraline Hingray, Paul Brunault, and Wissam El-Hage. 2022. "Childhood Trauma and Dissociation Correlates in Alcohol Use Disorder: A Cross-Sectional Study in a Sample of 587 French Subjects Hospitalized in a Rehabilitation Center" Brain Sciences 12, no. 11: 1483. https://doi.org/10.3390/brainsci12111483
APA StyleBaudin, G., Barrault, S., El Ayoubi, H., Kazour, F., Ballon, N., Maugé, D., Hingray, C., Brunault, P., & El-Hage, W. (2022). Childhood Trauma and Dissociation Correlates in Alcohol Use Disorder: A Cross-Sectional Study in a Sample of 587 French Subjects Hospitalized in a Rehabilitation Center. Brain Sciences, 12(11), 1483. https://doi.org/10.3390/brainsci12111483