
EMG-Triggered Pedaling Training on Muscle Activation, Gait, and Motor Function for Stroke Patients

Abstract
:1. Introduction
2. Materials and Methods
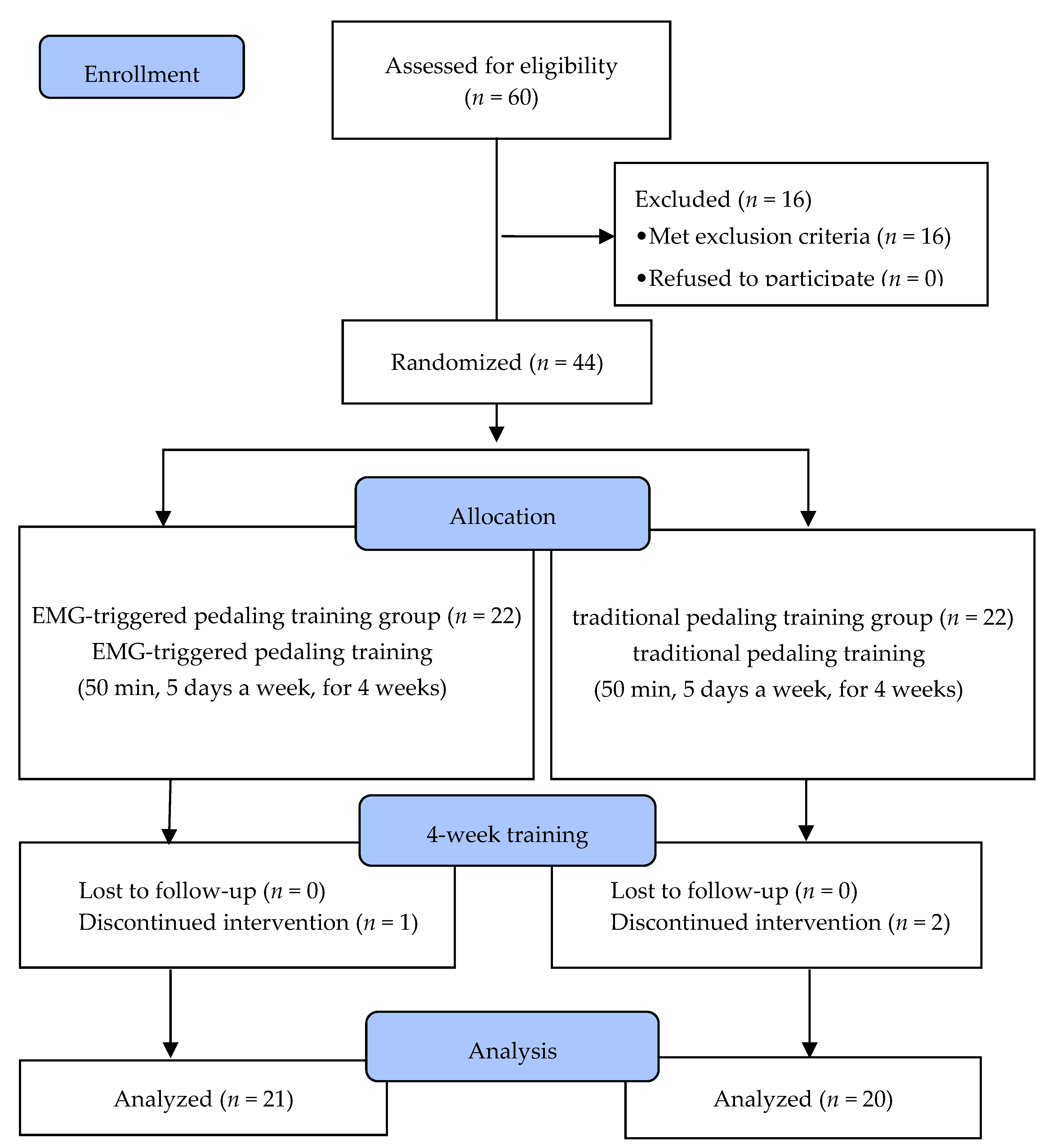
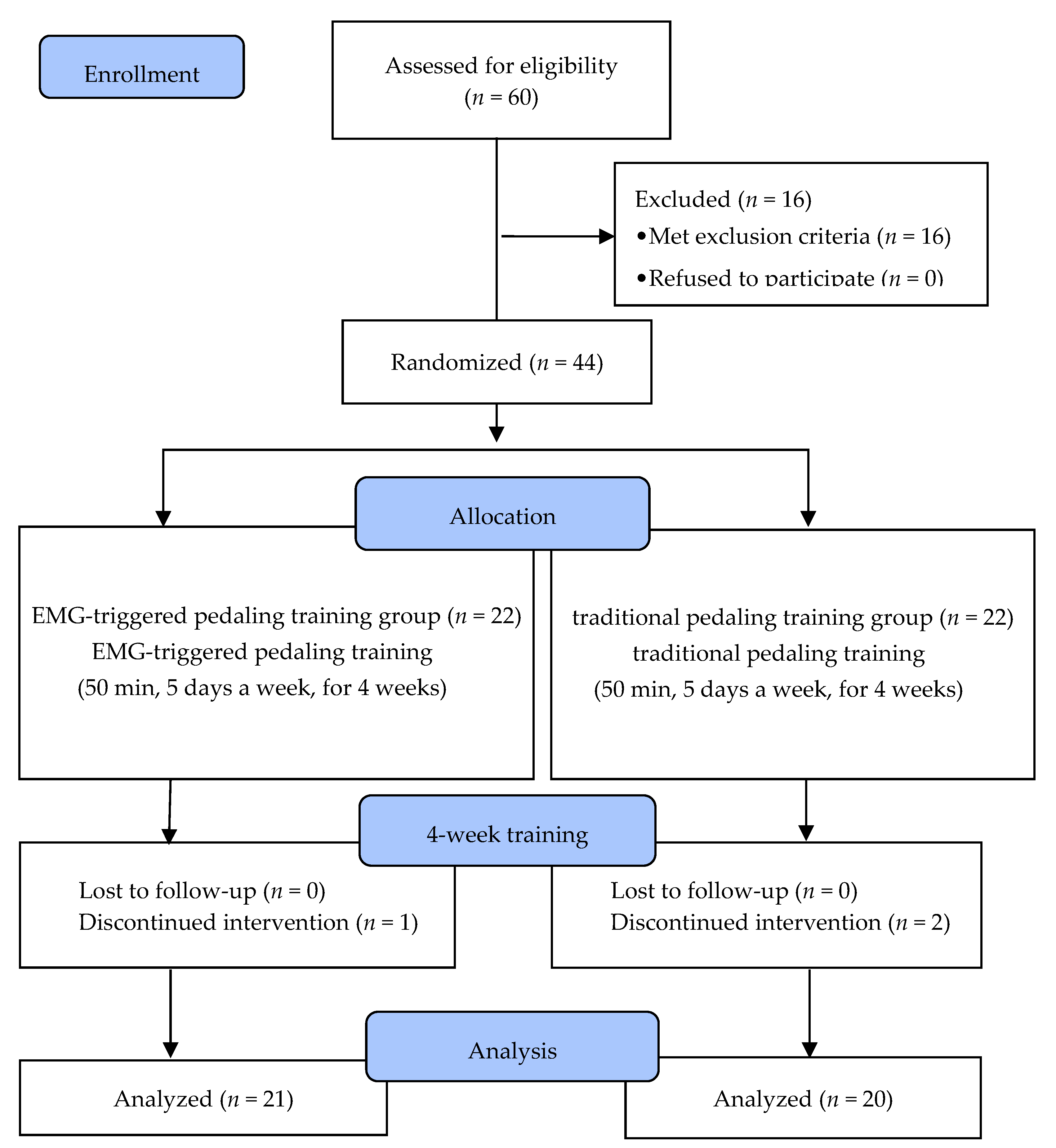
2.1. Subjects
2.2. Experimental Procedure
2.3. Experimental Method
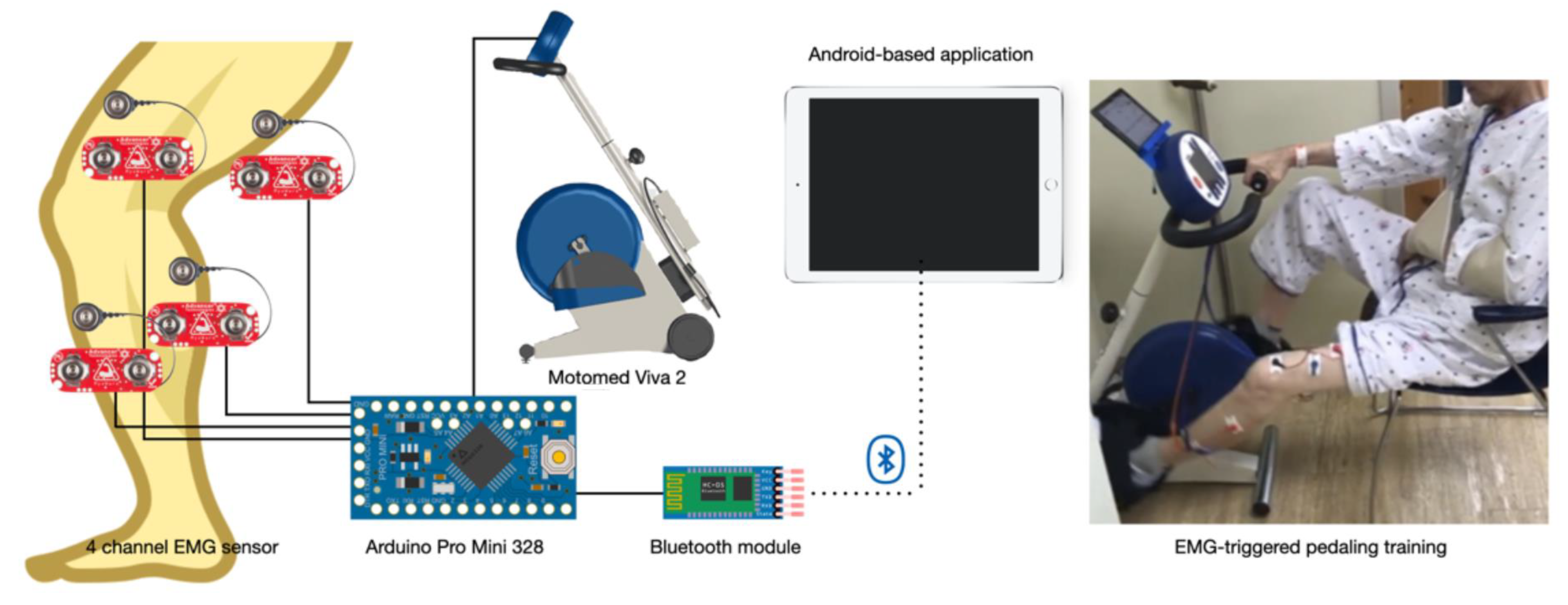
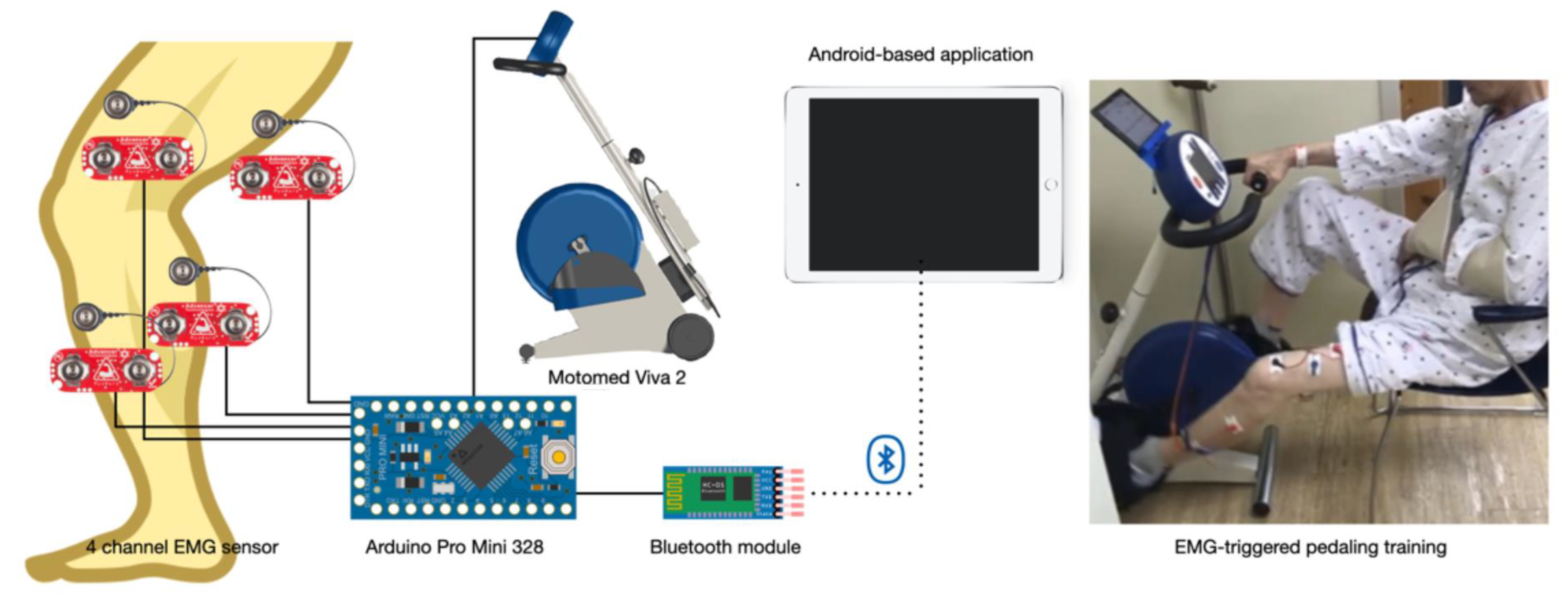
2.3.1. EMG-Triggered Device
2.3.2. EMG-Triggered Pedaling Training
2.4. Outcome Measurements
2.4.1. Muscle Activation
2.4.2. Gait Ability
2.4.3. Lower Extremity Motor Function
2.5. Data Analysis
3. Results
3.1. General Characteristics of the Subjects
3.2. Changes of in Muscle Activation
3.3. Changes of Gait Ability
3.4. Changes of Lower Extremity Motor Function
4. Discussion
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bejot, Y.; Bailly, H.; Durier, J.; Giroud, M. Epidemiology of stroke in europe and trends for the 21st century. Presse Med. 2016, 45, e391–e398. [Google Scholar] [CrossRef]
- Taylor-Piliae, R.E.; Hepworth, J.T.; Coull, B.M. Predictors of depressive symptoms among community-dwelling stroke survivors. J. Cardiovasc. Nurs. 2013, 28, 460–467. [Google Scholar] [CrossRef]
- Tyedin, K.; Cumming, T.B.; Bernhardt, J. Quality of life: An important outcome measure in a trial of very early mobilisation after stroke. Disabil. Rehabil. 2010, 32, 875–884. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W.; Andrews, A.W. Rehabilitation goals of patients with hemiplegia. Int. J. Rehabil. Res. 1988, 11, 181–183. [Google Scholar] [CrossRef]
- Wonsetler, E.C.; Bowden, M.G. A systematic review of mechanisms of gait speed change post-stroke. Part 1: Spatiotemporal parameters and asymmetry ratios. Top. Stroke Rehabil. 2017, 24, 435–446. [Google Scholar] [CrossRef] [PubMed]
- Patterson, K.K.; Gage, W.H.; Brooks, D.; Black, S.E.; McIlroy, W.E. Evaluation of gait symmetry after stroke: A comparison of current methods and recommendations for standardization. Gait Posture 2010, 31, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Francisco, G.E.; Zhou, P. Post-stroke hemiplegic gait: New perspective and insights. Front. Physiol. 2018, 9, 1021. [Google Scholar] [CrossRef] [Green Version]
- Patterson, K.K.; Parafianowicz, I.; Danells, C.J.; Closson, V.; Verrier, M.C.; Staines, W.R.; Black, S.E.; McIlroy, W.E. Gait asymmetry in community-ambulating stroke survivors. Arch. Phys. Med. Rehabil. 2008, 89, 304–310. [Google Scholar] [CrossRef]
- Rodriguez, G.M.; Aruin, A.S. The effect of shoe wedges and lifts on symmetry of stance and weight bearing in hemiparetic individuals. Arch. Phys. Med. Rehabil. 2002, 83, 478–482. [Google Scholar] [CrossRef]
- Ambrosini, E.; Ferrante, S.; Ferrigno, G.; Molteni, F.; Pedrocchi, A. Cycling induced by electrical stimulation improves muscle activation and symmetry during pedaling in hemiparetic patients. IEEE Trans. Neural Syst. Rehabil. Eng. 2012, 20, 320–330. [Google Scholar] [CrossRef]
- Langan, J.; van Donkelaar, P. The influence of hand dominance on the response to a constraint-induced therapy program following stroke. Neurorehabilit. Neural Repair 2008, 22, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Hamzei, F.; Krüger, H.; Peters, M.; Ketels, G.; Blessin, J.; Ringer, T.; Liepert, J.; Taub, E. Shaping-induced movement therapy for lower extremity (simt)—A pilot study. Neurol. Und Rehabil. 2012, 18, 236–241. [Google Scholar]
- Taub, E.; Uswatte, G.; Elbert, T. New treatments in neurorehabilitation founded on basic research. Nat. Rev. Neurosci. 2002, 3, 228–236. [Google Scholar] [CrossRef] [Green Version]
- dos Anjos, S.; Morris, D.; Taub, E. Constraint-induced movement therapy for lower extremity function: Describing the le-cimt protocol. Phys. Ther. 2020, 100, 698–707. [Google Scholar] [CrossRef] [PubMed]
- Numata, K.; Murayama, T.; Takasugi, J.; Oga, M. Effect of modified constraint-induced movement therapy on lower extremity hemiplegia due to a higher-motor area lesion. Brain Inj. 2008, 22, 898–904. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, T.S.; da Silva, T.C.C.; Costa, M.F.P.; Cavalcanti, F.; Lindquist, A.R.R. Effects of constraint-induced movement therapy for lower limbs on measurements of functional mobility and postural balance in subjects with stroke: A randomized controlled trial. Top. Stroke Rehabil. 2017, 24, 555–561. [Google Scholar]
- Kallio, K.; Nilsson-Wikmar, L.; Thorsén, A.-M. Modified constraint-induced therapy for the lower extremity in elderly persons with chronic stroke: Single-subject experimental design study. Top. Stroke Rehabil. 2014, 21, 111–119. [Google Scholar] [CrossRef]
- Billinger, S.A.; Arena, R.; Bernhardt, J.; Eng, J.J.; Franklin, B.A.; Johnson, C.M.; MacKay-Lyons, M.; Macko, R.F.; Mead, G.E.; Roth, E.J.; et al. Physical activity and exercise recommendations for stroke survivors. Stroke 2014, 45, 2532–2553. [Google Scholar] [CrossRef] [Green Version]
- Mazzocchio, R.; Meunier, S.; Ferrante, S.; Molteni, F.; Cohen, L.G. Cycling, a tool for locomotor recovery after motor lesions? NeuroRehabilitation 2008, 23, 67–80. [Google Scholar] [CrossRef]
- Yang, H.-C.; Lee, C.-L.; Lin, R.; Hsu, M.-J.; Chen, C.-H.; Lin, J.-H.; Lo, S.K. Effect of biofeedback cycling training on functional recovery and walking ability of lower extremity in patients with stroke. Kaohsiung J. Med. Sci. 2014, 30, 35–42. [Google Scholar] [CrossRef] [Green Version]
- Janssen, T.W.; Beltman, J.M.; Elich, P.; Koppe, P.A.; Konijnenbelt, H.; de Haan, A.; Gerrits, K.H. Effects of electric stimulation−assisted cycling training in people with chronic stroke. Arch. Phys. Med. Rehabil. 2008, 89, 463–469. [Google Scholar] [CrossRef]
- Barbosa, D.; Santos, C.P.; Martins, M. The application of cycling and cycling combined with feedback in the rehabilitation of stroke patients: A review. J. Stroke Cerebrovasc. Dis. 2015, 24, 253–273. [Google Scholar] [CrossRef] [PubMed]
- Perry, J.; Burnfield, J.M. Gait Analysis: Normal and Pathological Function, 2nd ed.; Slack incorporated: Thorofare, NJ, USA, 2010. [Google Scholar]
- Bae, S.; Kim, K.Y. Dual-afferent sensory input training for voluntary movement after stroke: A pilot randomized controlled study. NeuroRehabilitation 2017, 40, 293–300. [Google Scholar] [CrossRef]
- Mitsutake, T.; Sakamoto, M.; Horikawa, E. The effects of electromyography-triggered neuromuscular electrical stimulation plus tilt sensor functional electrical stimulation training on gait performance in patients with subacute stroke: A randomized controlled pilot trial. Int. J. Rehabil. Res. 2019, 42, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Shariat, A.; Najafabadi, M.G.; Ansari, N.N.; Cleland, J.A.; Singh, M.A.F.; Memari, A.H.; Honarpishe, R.; Hakakzadeh, A.; Ghaffari, M.S.; Naghdi, S. The effects of cycling with and without functional electrical stimulation on lower limb dysfunction in patient’s post-stroke: A systematic review with meta-analysis. NeuroRehabilitation 2019, 44, 389–412. [Google Scholar] [CrossRef] [PubMed]
- Ambrosini, E.; Parati, M.; Ferriero, G.; Pedrocchi, A.; Ferrante, S. Does cycling induced by functional electrical stimulation enhance motor recovery in the subacute phase after stroke? A systematic review and meta-analysis. Clin. Rehabil. 2020, 34, 1341–1354. [Google Scholar] [CrossRef]
- McDonough, A.L.; Batavia, M.; Chen, F.C.; Kwon, S.; Ziai, J. The validity and reliability of the gaitrite system’s measurements: A preliminary evaluation. Arch. Phys. Med. Rehabil. 2001, 82, 419–425. [Google Scholar] [CrossRef] [Green Version]
- van Uden, C.J.; Besser, M.P. Test-retest reliability of temporal and spatial gait characteristics measured with an instrumented walkway system (gaitrite). BMC Musculoskelet Disord. 2004, 5, 13. [Google Scholar] [CrossRef]
- Duncan, P.W.; Propst, M.; Nelson, S.G. Reliability of the fugl-meyer assessment of sensorimotor recovery following cerebrovascular accident. Phys. Ther. 1983, 63, 1606–1610. [Google Scholar] [CrossRef]
- Raasch, C.C.; Zajac, F.E. Locomotor strategy for pedaling: Muscle groups and biomechanical functions. J. Neurophysiol. 1999, 82, 515–525. [Google Scholar] [CrossRef] [PubMed]
- Kautz, S.A.; Duncan, P.W.; Perera, S.; Neptune, R.R.; Studenski, S.A. Coordination of hemiparetic locomotion after stroke rehabilitation. Neurorehabil. Neural Repair 2005, 19, 250–258. [Google Scholar] [CrossRef]
- Bolton, D.A.; Cauraugh, J.H.; Hausenblas, H.A. Electromyogram-triggered neuromuscular stimulation and stroke motor recovery of arm/hand functions: A meta-analysis. J. Neurol. Sci. 2004, 223, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Mukaino, M.; Ohtsuka, K.; Otaka, Y.; Tanikawa, H.; Matsuda, F.; Tsuchiyama, K.; Yamada, J.; Saitoh, E. Gait characteristics of post-stroke hemiparetic patients with different walking speeds. Int. J. Rehabil. Res. 2020, 43, 69–75. [Google Scholar] [CrossRef]
- Shen, C.; Liu, F.; Yao, L.; Li, Z.; Qiu, L.; Fang, S. Effects of motomed movement therapy on the mobility and activities of daily living of stroke patients with hemiplegia: A systematic review and meta-analysis. Clin. Rehabil. 2018, 32, 1569–1580. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.; Kim, Y.; Cha, Y.; In, T.-S.; Hur, Y.-G.; Chung, Y. Effects of gait training with a cane and an augmented pressure sensor for enhancement of weight bearing over the affected lower limb in patients with stroke: A randomized controlled pilot study. Clin. Rehabil. 2014, 29, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Cramp, M.C.; Greenwood, R.J.; Gill, M.; Rothwell, J.C.; Scott, O.M. Low intensity strength training for ambulatory stroke patients. Disabil. Rehabil. 2006, 28, 883–889. [Google Scholar] [CrossRef] [PubMed]
- Karthiga, R. The Effect of Visual Feedback Assisted Bicycle Ergometry in Improving Functional Activities of Lower Extremity among Post Stroke Patients-Quasi Experimental Study. 2020, Volume 14, p. 2148. Available online: www.ijpot.com (accessed on 27 December 2021).
- Choi, H.-S.; Shin, W.-S.; Bang, D.-H.; Choi, S.-J. Effects of game-based constraint-induced movement therapy on balance in patients with stroke: A single-blind randomized controlled trial. Am. J. Phys. Med. Rehabil. 2017, 96, 184–190. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| EMG-PTG (n = 21) | TPTG (n = 20) | χ2/t | p | |
|---|---|---|---|---|
| Age (year) | 62.71 ± 6.91 | 64.80 ± 9.59 | 0.802 | 0.428 |
| Height (cm) | 162.62 ± 7.85 | 161.70 ± 9.33 | 0.342 | 0.734 |
| Weight (kg) | 59.10 ± 8.17 | 59.93 ± 8.53 | 0.319 | 0.752 |
| Body mass index (point) | 22.30 ± 2.27 | 22.85 ± 1.93 | 0.828 | 0.413 |
| Duration of stroke (month) | 13.71 ± 5.97 | 16.70 ± 5.83 | 1.619 | 0.113 |
| MMSE | 25.86 ± 1.31 | 25.50 ± 1.05 | 0.958 | 0.344 |
| MBI | 53.10 ± 10.00 | 56.01 ± 10.05 | 0.929 | 0.359 |
| Gender (male/female) | 10/11 | 10/10 | 0.023 | 0.879 |
| Paretic side (right/left) | 10/11 | 14/6 | 2.114 | 0.146 |
| Stroke type (infarction/hemorrhage) | 14/7 | 12/8 | 0.196 | 0.658 |
| EMG-PTG (n = 21) | TPTG (n = 20) | Significance of Change Scores t(p) | Effect Size | MDC (MDC%) | ||
|---|---|---|---|---|---|---|
| Muscle activation of affected side | ||||||
| Rectus femoris muscle (μV) | Pre | 7.58 ± 4.26 | 7.08 ± 4.02 | |||
| Post | 10.19 ± 4.60 | 7.88 ± 4.68 | ||||
| Change Score | 2.61 ± 1.35 * | 0.80 ± 2.03 | 3.364(0.002) | 1.05 | 0.82(31.35) | |
| Biceps femoris muscle (μV) | Pre | 12.00 ± 5.09 | 12.13 ± 4.91 | |||
| Post | 13.73 ± 5.22 | 12.84 ± 5.75 | ||||
| Change Score | 1.73 ± 0.74 * | 0.70 ± 2.00 | 2.192(0.034) | 0.68 | 0.45(25.84) | |
| Tibialis anterior muscle (μV) | Pre | 11.16 ± 9.18 | 13.83 ± 10.12 | |||
| Post | 11.90 ± 9.63 | 14.71 ± 9.47 | ||||
| Change Score | 0.73 ± 1.82 | 0.87 ± 2.13 | 0.224(0.824) | |||
| Gastrocnemius muscle (μV) | Pre | 14.05 ± 12.65 | 12.79 ± 11.76 | |||
| Post | 15.84 ± 12.73 | 13.45 ± 11.80 | ||||
| Change Score | 1.79 ± 1.27 * | 0.67 ± 1.84 | 2.278(0.028) | 0.71 | 0.77(42.85) | |
| Muscle activation of unaffected side | ||||||
| Rectus femoris muscle (μV) | Pre | 12.48 ± 5.18 | 12.76 ± 6.27 | |||
| Post | 12.79 ± 4.93 | 12.90 ± 5.38 | ||||
| Change Score | 0.19 ± 1.64 | 0.14 ± 1.90 | 0.056(0.932) | |||
| Biceps femoris muscle (μV) | Pre | 23.57 ± 15.82 | 20.73 ± 15.75 | |||
| Post | 24.08 ± 15.71 | 21.36 ± 15.82 | ||||
| Change Score | 0.51 ± 1.98 | 0.62 ± 2.17 | 0.175(0.862) | |||
| Tibialis anterior muscle (μV) | Pre | 18.19 ± 9.91 | 18.95 ± 9.05 | |||
| Post | 18.60 ± 10.12 | 19.54 ± 9.38 | ||||
| Change Score | 0.40 ± 1.75 | 0.59 ± 1.99 | 0.320(0.751) | |||
| Gastrocnemius muscle (μV) | Pre | 15.25 ± 5.22 | 14.29 ± 5.12 | |||
| Post | 15.59 ± 5.60 | 14.84 ± 5.02 | ||||
| Change Score | 0.34 ± 1.62 | 0.55 ± 2.17 | 0.363(0.718) | |||
| Symmetry ratio | ||||||
| Rectus femoris muscle | Pre | 1.97 ± 0.89 | 2.12 ± 1.01 | |||
| Post | 1.40 ± 0.64 | 2.04 ± 1.10 | ||||
| Change Score | −0.57 ± 0.52 * | −0.08 ± 0.80 | 2.343(0.024) | 0.73 | 0.32(55.33) | |
| Biceps femoris muscle | Pre | 2.00 ± 1.06 | 1.67 ± 0.94 | |||
| Post | 1.76 ± 0.91 | 1.69 ± 1.00 | ||||
| Change Score | −0.24 ± 0.26 * | 0.03 ± 0.21 | 3.630(0.001) | 1.13 | 0.16(65.38) | |
| Tibialis anterior muscle | Pre | 2.13 ± 1.18 | 1.77 ± 0.87 | |||
| Post | 2.12 ± 1.39 | 1.67 ± 0.75 | ||||
| Change Score | −0.01 ± 0.57 | −0.10 ± 0.35 | 0.605(0.549) | |||
| Gastrocnemius muscle | Pre | 1.71 ± 1.10 | 1.66 ± 1.10 | |||
| Post | 1.42 ± 0.88 | 1.78 ± 1.39 | ||||
| Change Score | −0.29 ± 0.30 * | 0.12 ± 0.52 | 3.073(0.004) | 0.96 | 0.18(62.46) | |
| EMG-PTG (n = 21) | TPTG (n = 20) | Significance of Change Scores t(p) | Effect Size | MDC(MDC%) | ||
|---|---|---|---|---|---|---|
| Temporal gait parameter | ||||||
| Velocity (cm/s) | Pre | 32.40 ± 16.41 | 33.71 ± 15.23 | |||
| Post | 39.66 ± 18.83 | 36.35 ± 16.75 | ||||
| Change Score | 7.26 ± 4.29 * | 2.64 ± 2.91 * | 4.018(0.000) | 1.26 | 2.56(35.71) | |
| Cadence (step/min) | Pre | 56.75 ± 14.36 | 57.73 ± 13.92 | |||
| Post | 63.94 ± 18.80 | 61.22 ± 17.52 | ||||
| Change Score | 7.18 ± 6.58 * | 3.49 ± 5.55 * | 1.936(0.060) | |||
| Stride time (s) | Pre | 2.34 ± 1.05 | 2.30 ± 1.07 | |||
| Post | 2.15 ± 1.11 | 2.22 ± 1.11 | ||||
| Change Score | −0.19 ± 0.22* | −0.08 ± 0.14 * | 2.005(0.052) | |||
| Affected side step time (s) | Pre | 1.32 ± 0.54 | 1.32 ± 0.54 | |||
| Post | 1.17 ± 0.55 | 1.29 ± 0.55 | ||||
| Change Score | −0.15 ± 0.13 * | −0.03 ± 0.11 | 3.128(0.003) | 0.98 | 0.08(52.11) | |
| Unaffected side step time (s) | Pre | 1.02 ± 0.52 | 0.98 ± 0.54 | |||
| Post | 0.98 ± 0.56 | 0.94 ± 0.59 | ||||
| Change Score | −0.04 ± 0.12 | −0.04 ± 0.10 | 0.184(0.855) | |||
| Affected side Single-limb support time (s) | Pre | 0.41 ± 0.14 | 0.42 ± 0.14 | |||
| Post | 0.44 ± 0.14 | 0.41 ± 0.15 | ||||
| Change Score | 0.03 ± 0.05 * | −0.01 ± 0.07 | 2.568(0.014) | 0.80 | 0.03(88.80) | |
| Unaffected side Single-limb support time (s) | Pre | 0.54 ± 0.13 | 0.58 ± 0.14 | |||
| Post | 0.54 ± 0.14 | 0.58 ± 0.16 | ||||
| Change Score | 0.00 ± 0.04 | 0.01 ± 0.07 | 0.112(0.912) | |||
| Double-limb support (%) | Pre | 55.82 ± 14.82 | 53.04 ± 13.73 | |||
| Post | 49.11 ± 16.27 | 51.63 ± 12.84 | ||||
| Change Score | −6.71 ± 3.32 * | −1.42 ± 2.98 * | 5.359(0.000) | 1.67 | 2.01(29.93) | |
| Spatial gait parameter | ||||||
| Stride length (cm) | Pre | 66.12 ± 22.79 | 68.43 ± 21.17 | |||
| Post | 72.10 ± 20.61 | 69.47 ± 19.12 | ||||
| Change Score | 5.98 ± 5.53 * | 1.04 ± 3.66 | 3.354(0.002) | 1.05 | 3.34(55.88) | |
| Affected side Step length (cm) | Pre | 35.52 ± 13.51 | 36.45 ± 12.79 | |||
| Post | 38.37 ± 12.24 | 36.26 ± 10.90 | ||||
| Change Score | 2.86 ± 2.76 * | −0.19 ± 3.88 | 2.913(0.006) | 0.91 | 1.67(58.38) | |
| Unaffected side Step length (cm) | Pre | 30.60 ± 9.57 | 31.97 ± 8.70 | |||
| Post | 33.73 ± 8.90 | 33.21 ± 8.70 | ||||
| Change Score | 3.12 ± 3.50 * | 1.24 ± 2.08* | 2.084(0.044) | 0.65 | 2.12(67.84) | |
| Symmetry of gait | ||||||
| Gait symmetry on step length (score) | Pre | 0.20 ± 0.09 | 0.18 ± 0.10 | |||
| Post | 0.16 ± 0.12 | 0.18 ± 0.17 | ||||
| Change Score | −0.04 ± 0.08 * | 0.00 ± 0.17 | 0.963(0.341) | |||
| Gait symmetry on step time (score) | Pre | 0.34 ± 0.18 | 0.41 ± 0.27 | |||
| Post | 0.24 ± 0.12 | 0.50 ± 0.45 | ||||
| Change Score | −0.10 ± 0.16 * | 0.09 ± 0.25 | 2.971(0.005) | 0.93 | 0.10(91.13) | |
| EMG-PTG (n = 21) | TPTG (n = 20) | Significance of Change Scores t(p) | Effect Size | MDC (MDC%) | ||
|---|---|---|---|---|---|---|
| FMA-LE (score) | Pre | 15.90 ± 4.71 | 15.08 ± 4.13 | |||
| Post | 19.62 ± 5.12 | 15.84 ± 3.17 | ||||
| Change Score | 3.72 ± 1.53 * | 0.76 ± 3.17 * | 6.419(0.000) | 2.01 | 0.93(24.92) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K. EMG-Triggered Pedaling Training on Muscle Activation, Gait, and Motor Function for Stroke Patients. Brain Sci. 2022, 12, 76. https://doi.org/10.3390/brainsci12010076
Lee K. EMG-Triggered Pedaling Training on Muscle Activation, Gait, and Motor Function for Stroke Patients. Brain Sciences. 2022; 12(1):76. https://doi.org/10.3390/brainsci12010076
Chicago/Turabian StyleLee, Kyeongjin. 2022. "EMG-Triggered Pedaling Training on Muscle Activation, Gait, and Motor Function for Stroke Patients" Brain Sciences 12, no. 1: 76. https://doi.org/10.3390/brainsci12010076
APA StyleLee, K. (2022). EMG-Triggered Pedaling Training on Muscle Activation, Gait, and Motor Function for Stroke Patients. Brain Sciences, 12(1), 76. https://doi.org/10.3390/brainsci12010076