
Evaluation of Two Methods (Inside-Out/Outside-In) Inferior Articular Process Resection for Uniportal Full Endoscopic Posterolateral Transforaminal Lumbar Interbody Fusion: Technical Note

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Indication, Inclusion and Exclusion Criteria
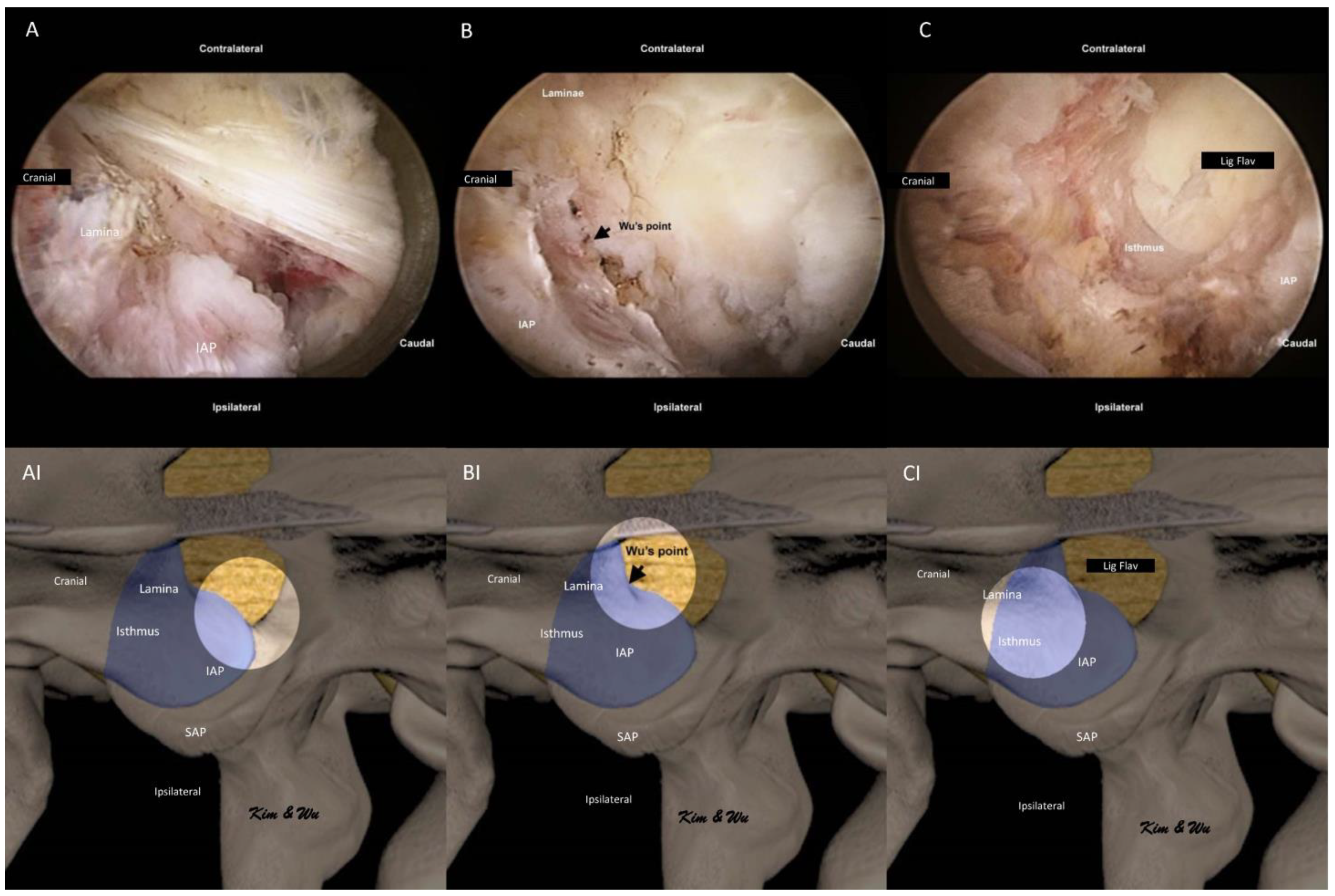
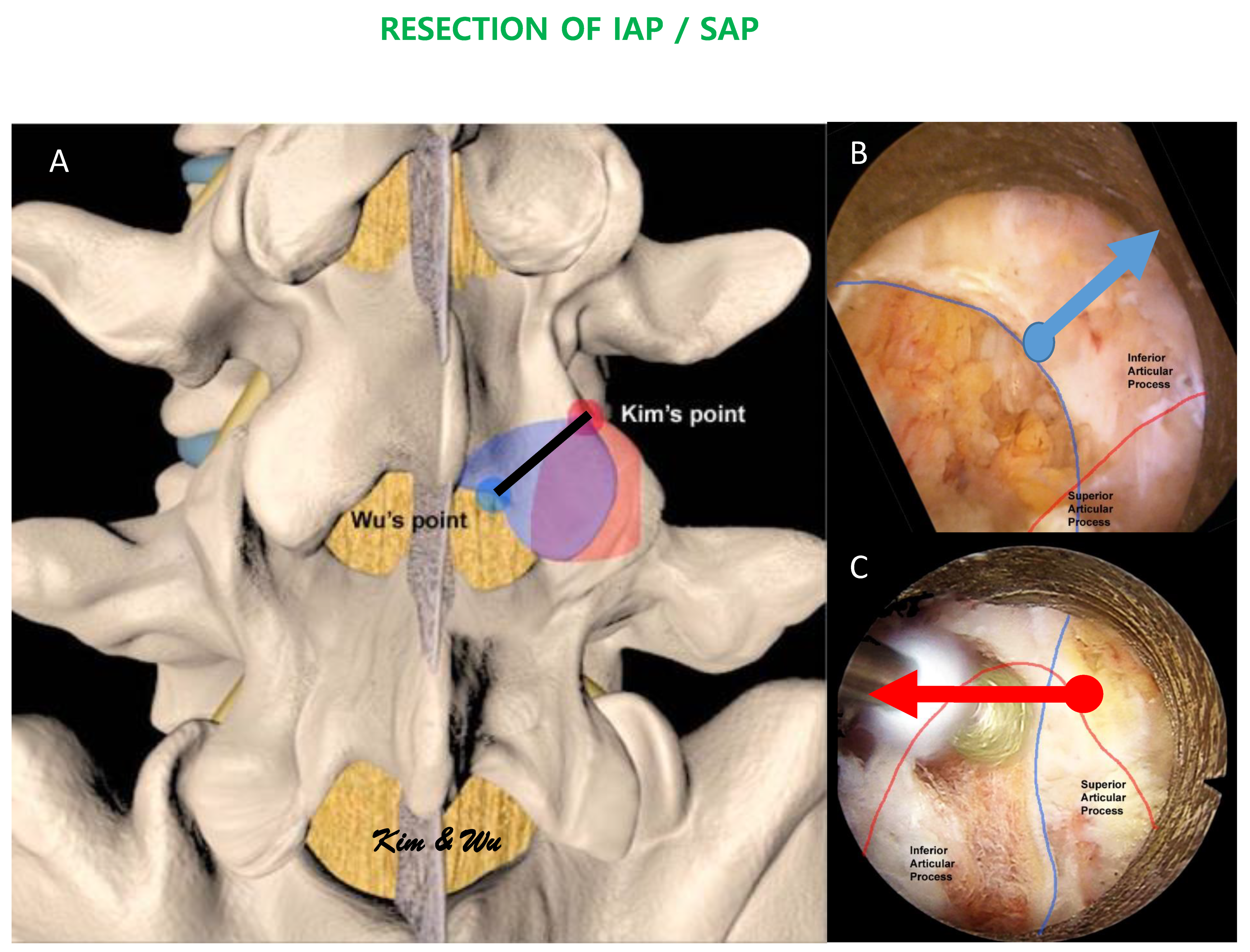
2.2. Endoscopic Surgical Anatomy of Inferior Articular Process in Endoscopic Fusion
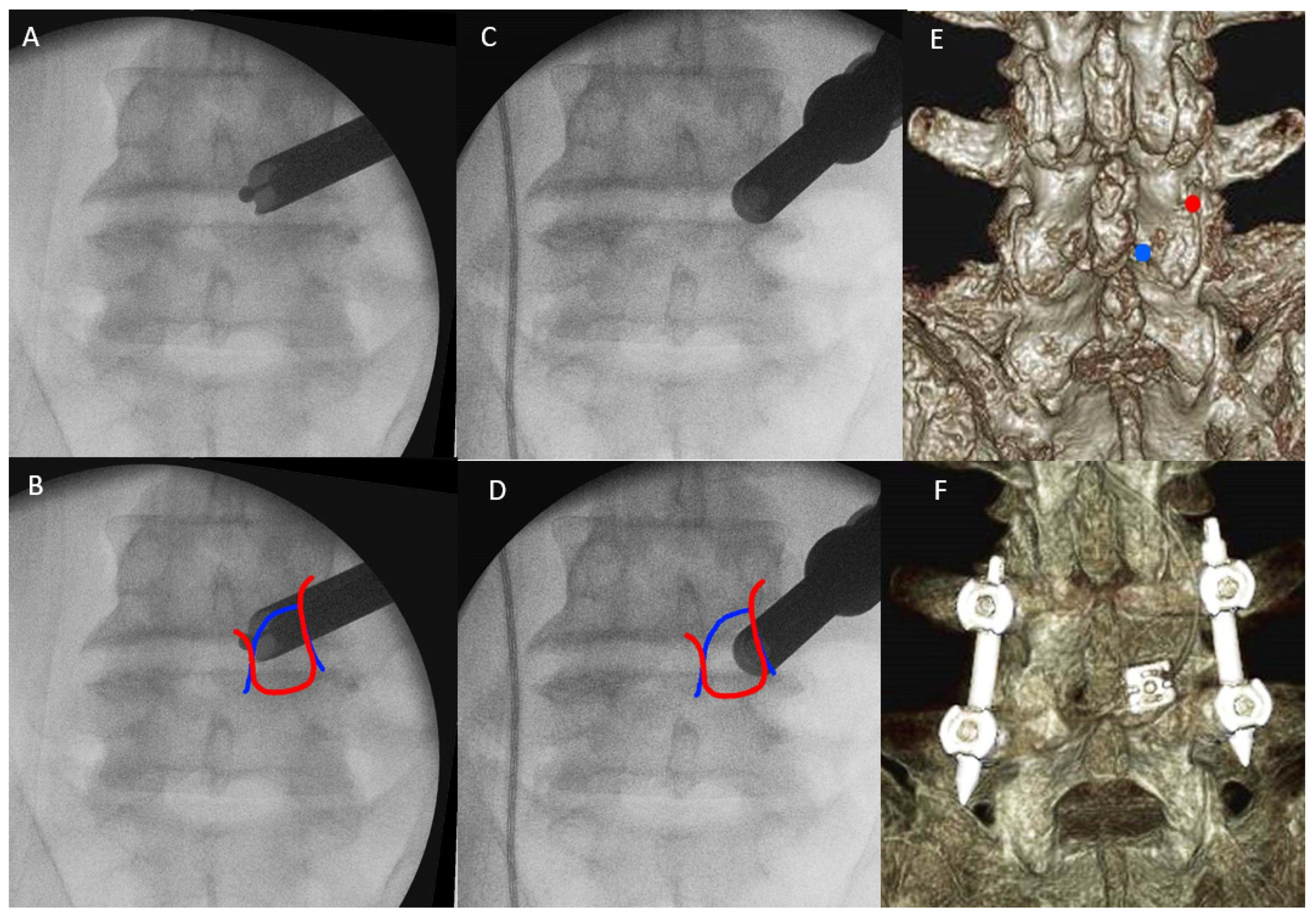
2.3. Surgical Technique of ETLIF
2.4. Surgical Procedure for ETLIF (I) and ETLIF (O)
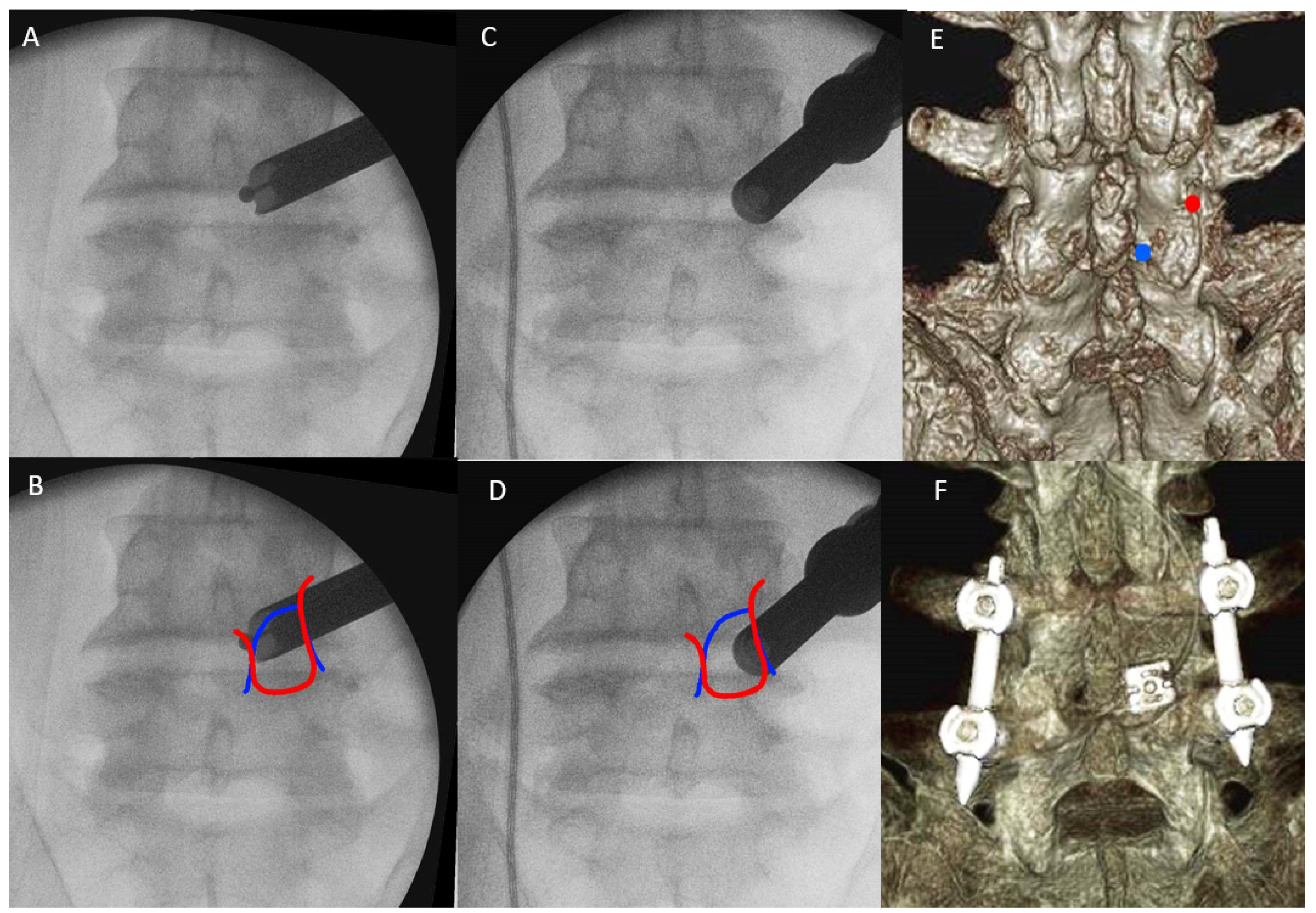
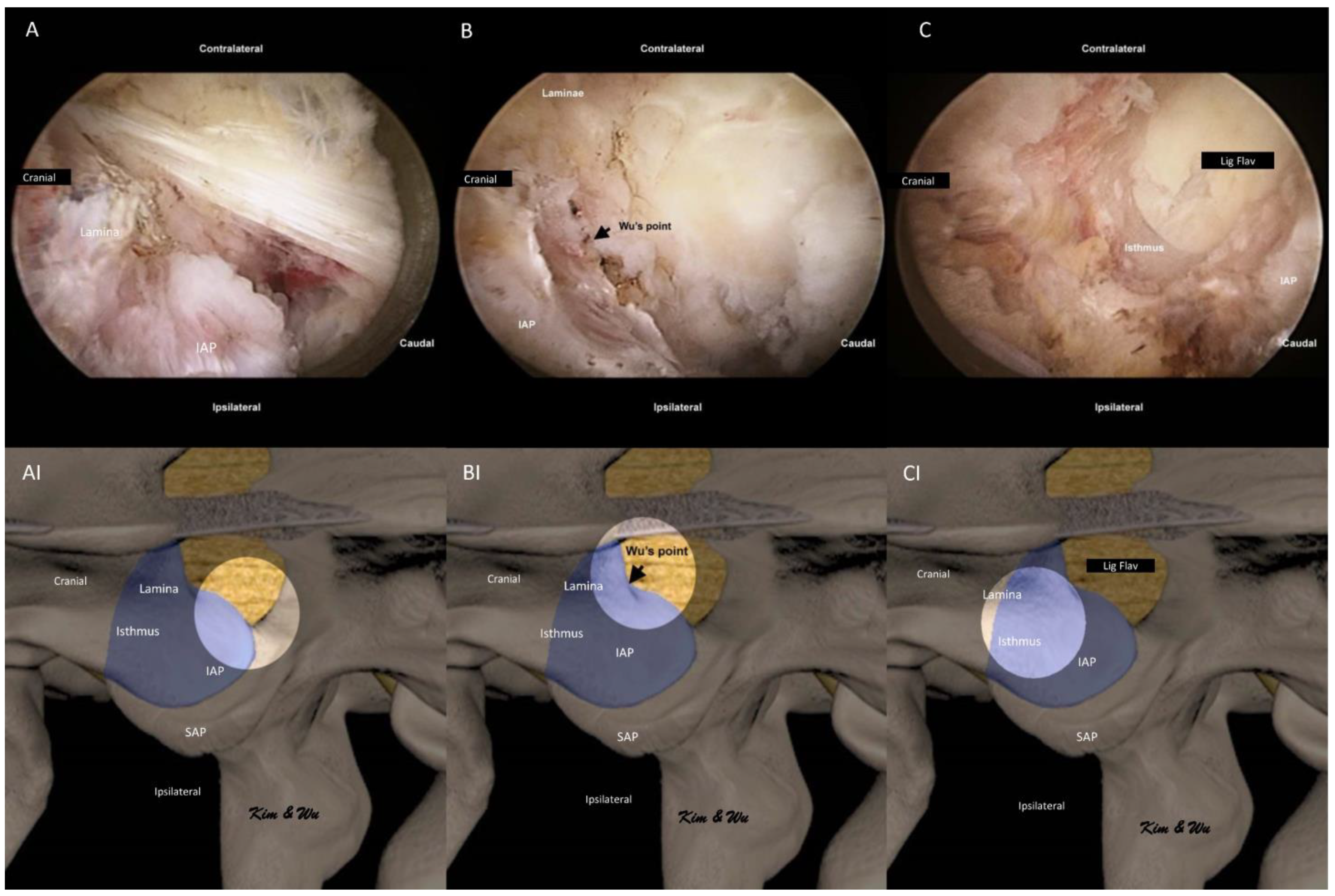
2.4.1. Docking of Endoscope on Isthmus
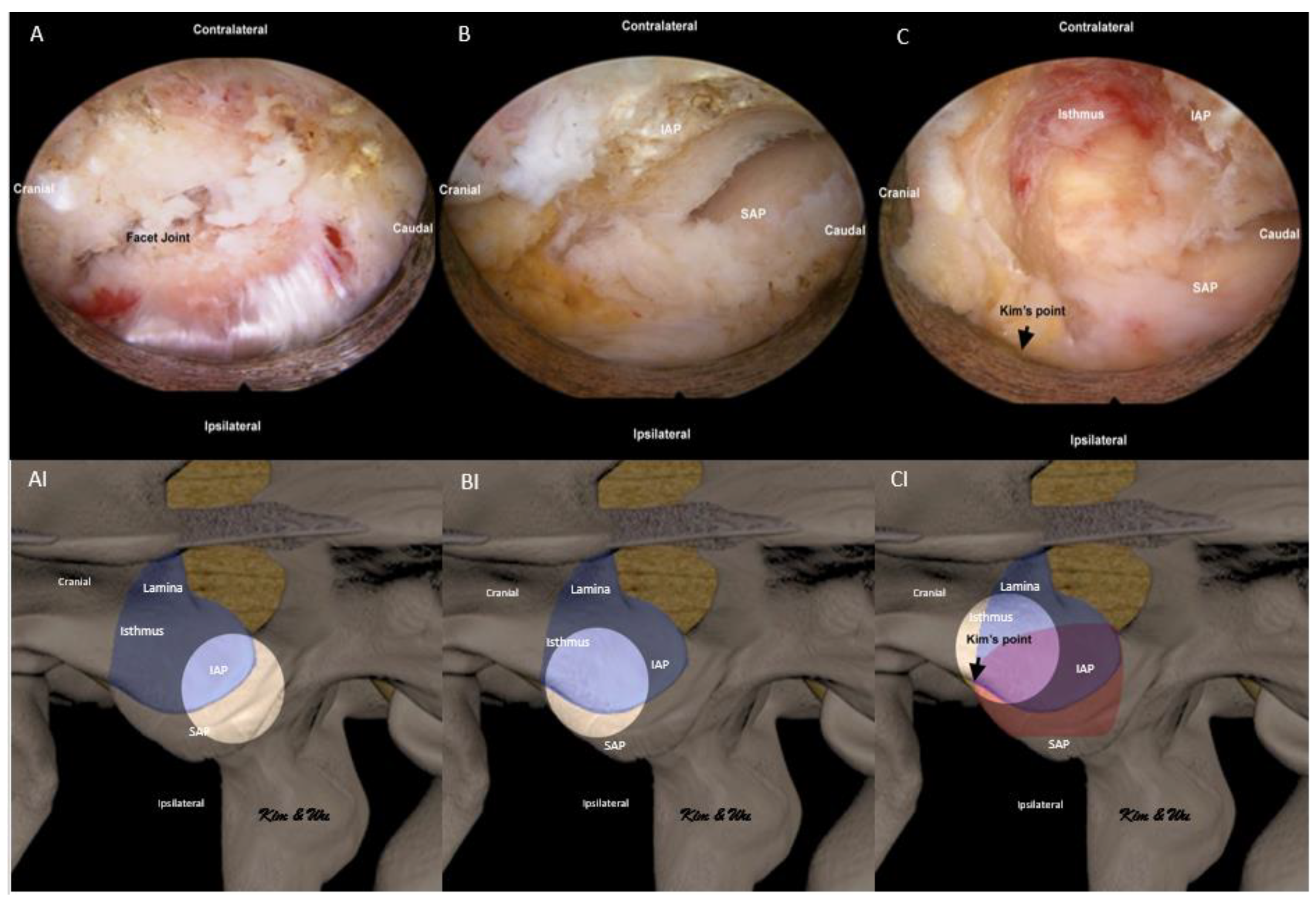
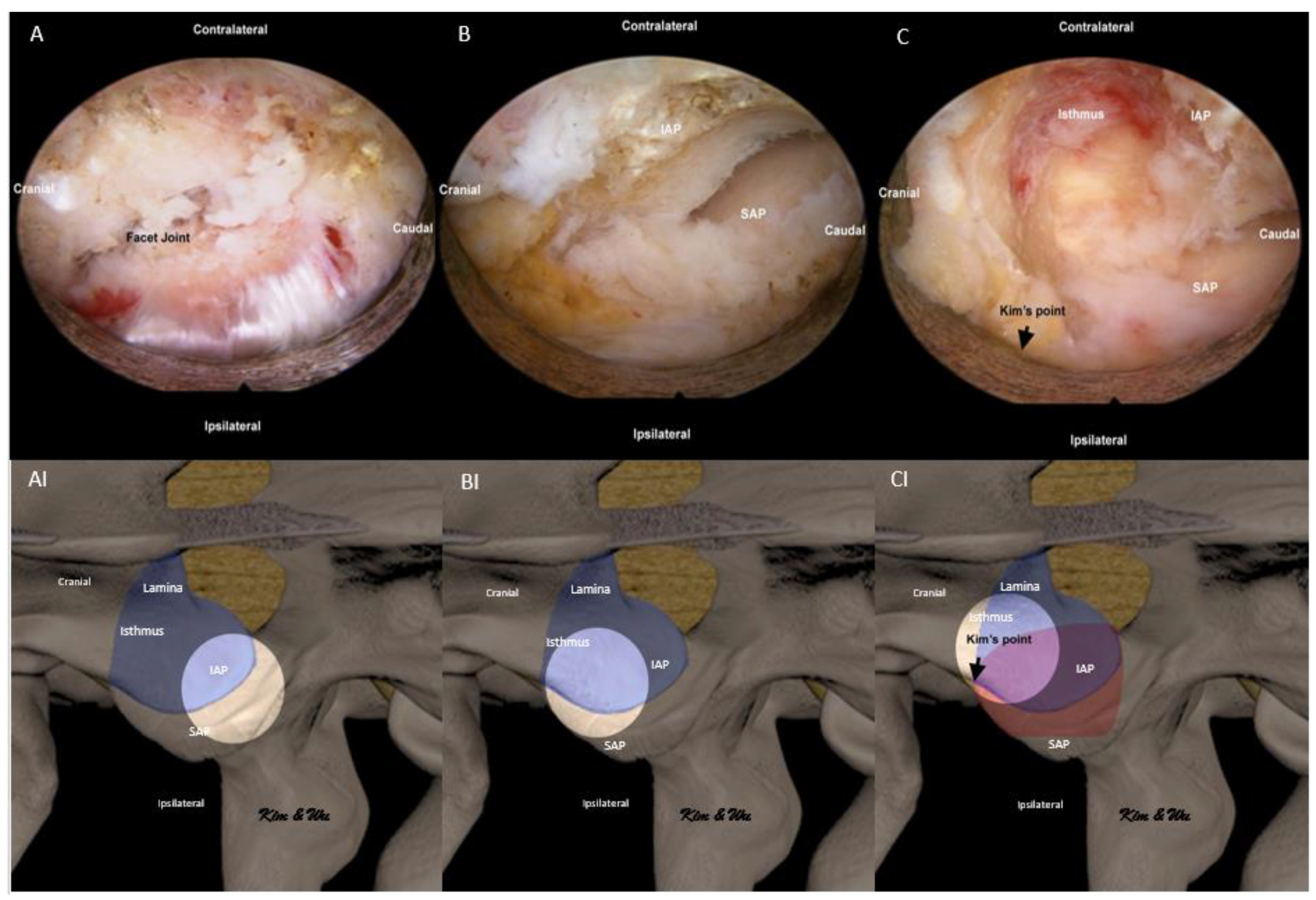
2.4.2. Handling of Inferior Articular Process: ETLIF (I) versus ETLIF (O)
2.4.3. Superior Articular Facet Resection and Flavectomy
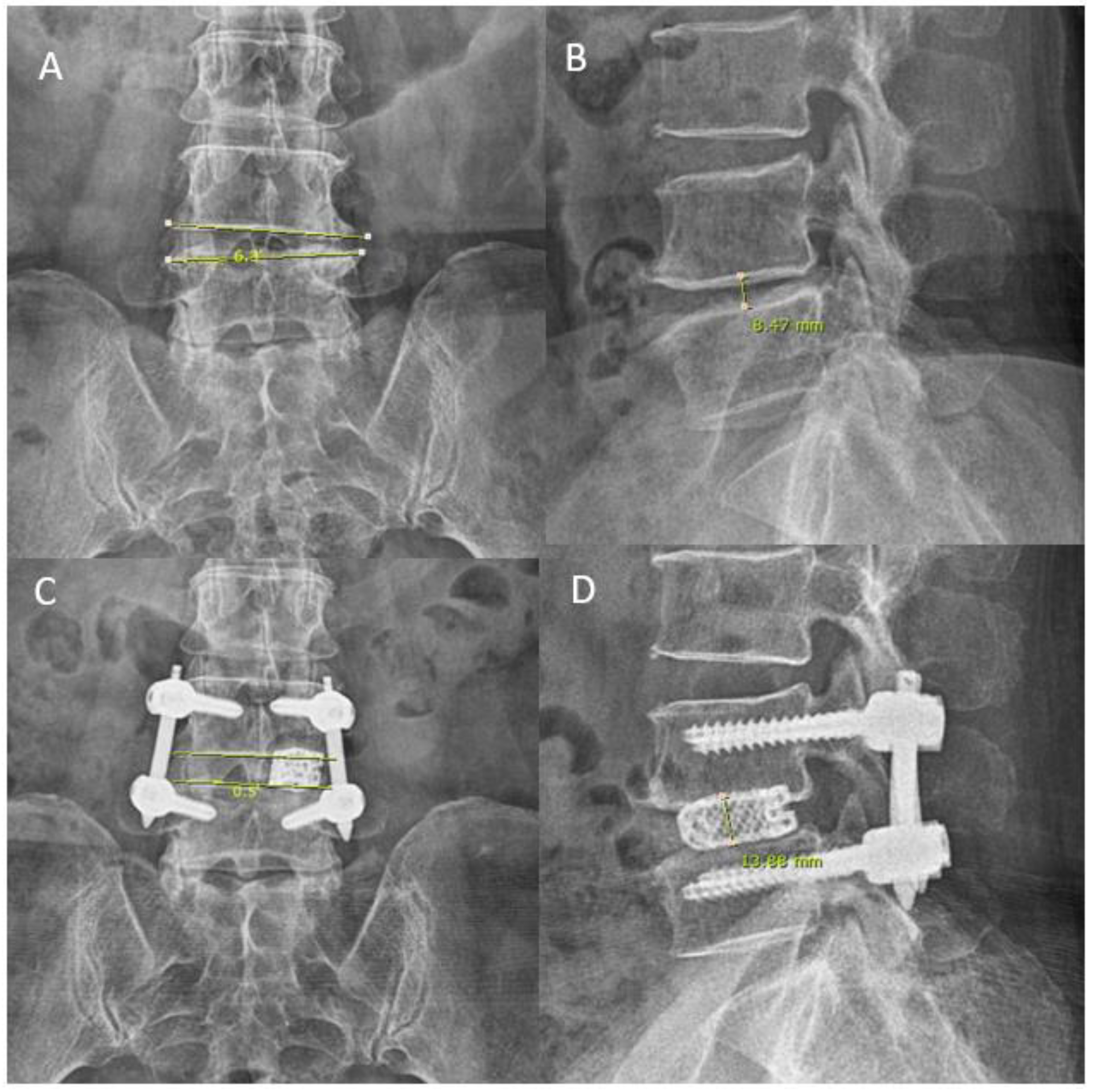
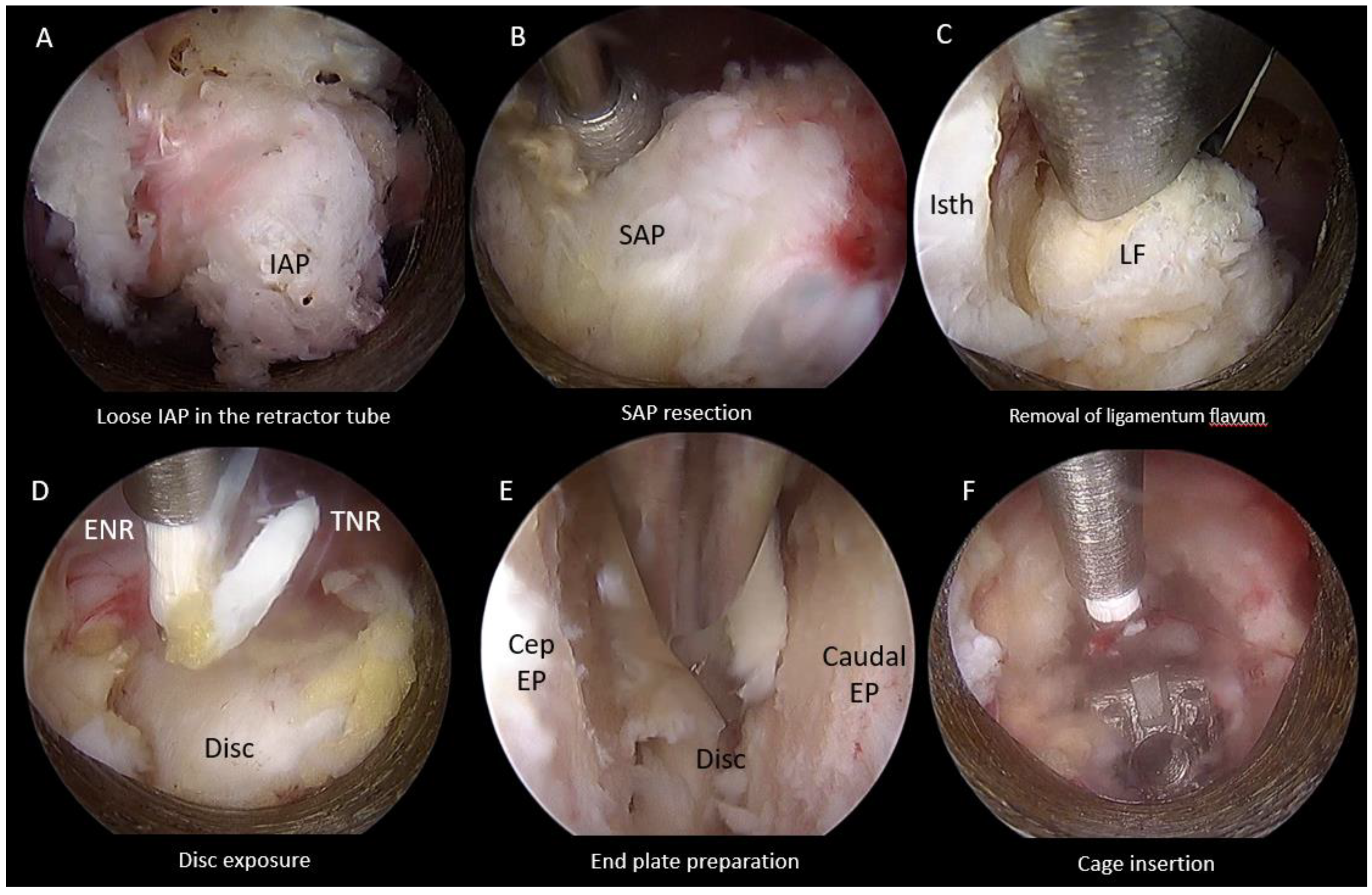
2.4.4. End Plate Preparation and Cage Insertion
2.5. Collection of Operative, Clinical and Radiological Data
2.6. Statistical Analysis
3. Results
3.1. Baseline Demographics
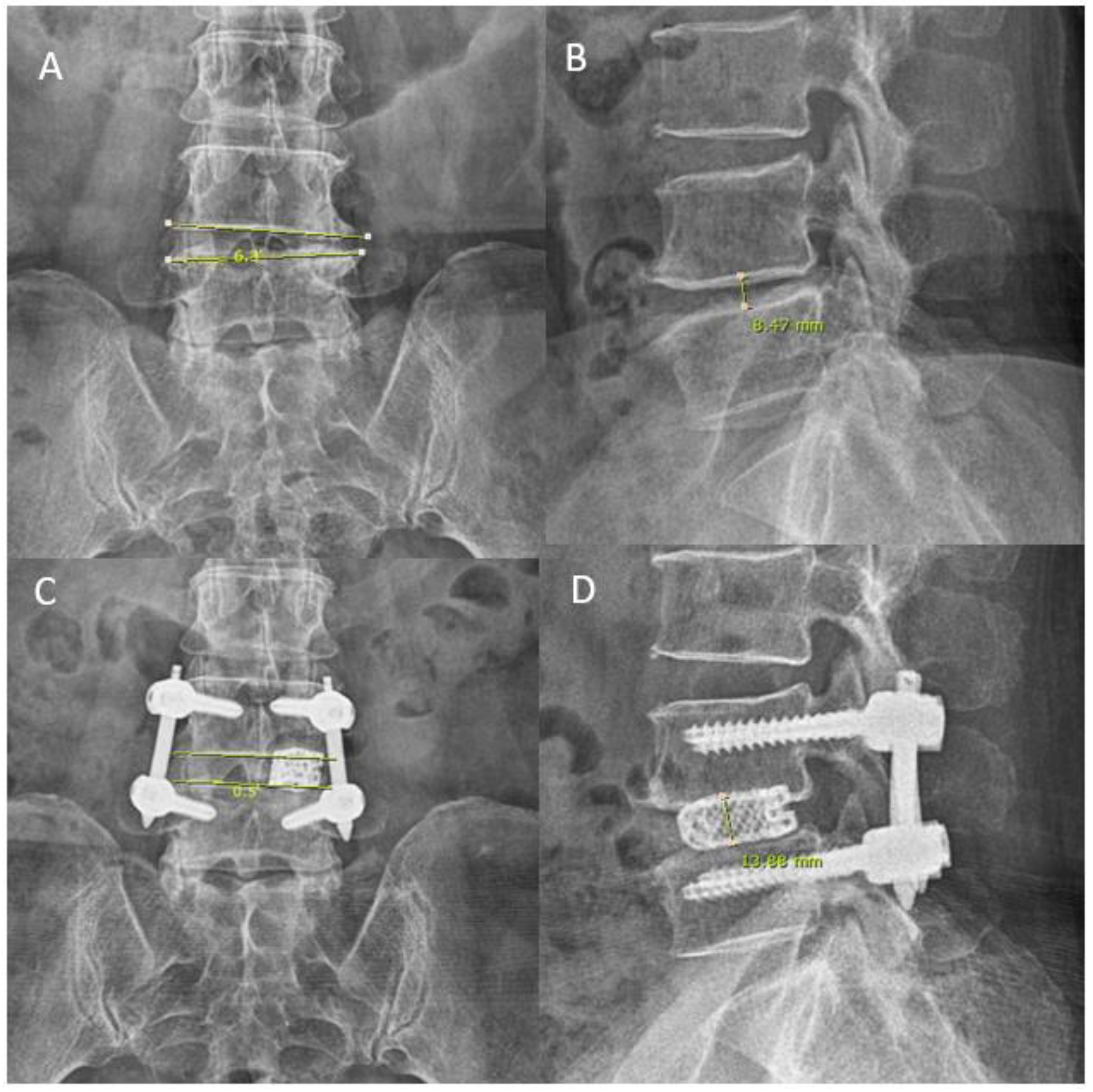
3.2. Intraoperative Timing and Radiological Parameters
3.3. Clinical Outcomes
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kim, M.; Kim, H.S.; Oh, S.W.; Adsul, N.M.; Singh, R.; Kashlan, O.N.; Noh, J.H.; Jang, I.T.; Oh, S.H. Evolution of Spinal Endoscopic Surgery. Neurospine 2019, 16, 6–14. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.S.; Wu, P.H.; Jang, I.-T. Development of Endoscopic Spine Surgery for Healthy Life: To Provide Spine Care for Better, for Worse, for Richer, for Poorer, in Sickness and in Health. Neurospine 2020, 17, S3–S8. [Google Scholar] [CrossRef]
- Wu, P.H.; Kim, H.S.; Jang, I.-T. How I do it? Uniportal full endoscopic contralateral approach for lumbar foraminal stenosis with double crush syndrome. Acta Neurochir. 2019, 162, 305–310. [Google Scholar] [CrossRef] [Green Version]
- Sebastian, R.; Martin, K.; Harry, M.; Georgios, G. Use of newly developed instruments and endoscopes: Full-endoscopic resection of lumbar disc herniations via the interlaminar and lateral transforaminal approach. J. Neurosurg. Spine SPI 2007, 6, 521–530. [Google Scholar]
- Drazin, D.; Ugiliweneza, B.; Al-Khouja, L.; Yang, D.; Johnson, P.; Kim, T.; Boakye, M. Treatment of Recurrent Disc Herniation: A Systematic Review. Cureus 2016, 8, e622. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.S.; Adsul, N.; Kapoor, A.; Choi, S.H.; Kim, J.H.; Kim, K.J.; Bang, J.S.; Yang, K.H.; Han, S.; Lim, J.H.; et al. A Mobile Outside-in Technique of Transforaminal Lumbar Endoscopy for Lumbar Disc Herniations. J. Vis. Exp. 2018, 138, 57999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruetten, S.; Komp, M.; Merk, H.; Godolias, G. Surgical treatment for lumbar lateral recess stenosis with the full-endoscopic interlaminar approach versus conventional microsurgical technique: A prospective, randomized, controlled study. J. Neurosurg. Spine 2009, 10, 476–485. [Google Scholar] [CrossRef] [Green Version]
- Morgenstern, R.; Morgenstern, C.; Jane, R.; Lee, S.H. Usefulness of an expandable interbody spacer for the treatment of foraminal stenosis in extremely collapsed disks: Preliminary clinical experience with endoscopic posterolateral transforaminal approach. J. Spinal Disord. Tech. 2011, 24, 485–491. [Google Scholar] [CrossRef]
- Kolcun, J.P.G.; Brusko, G.D.; Basil, G.W.; Epstein, R.; Wang, M.Y. Endoscopic transforaminal lumbar interbody fusion without general anesthesia: Operative and clinical outcomes in 100 consecutive patients with a minimum 1-year follow-up. Neurosurg. Focus 2019, 46, E14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.Y.; Grossman, J. Endoscopic minimally invasive transforaminal interbody fusion without general anesthesia: Initial clinical experience with 1-year follow-up. Neurosurg. Focus 2016, 40, E13. [Google Scholar] [CrossRef] [PubMed]
- Wagner, R.; Haefner, M. Uniportal Endoscopic Lumbar Interbody Fusion. Neurospine 2020, 17, S120–S128. [Google Scholar] [CrossRef]
- Heo, D.H.; Son, S.K.; Eum, J.H.; Park, C.K. Fully endoscopic lumbar interbody fusion using a percutaneous unilateral biportal endoscopic technique: Technical note and preliminary clinical results. BioMed Res. Int. 2017, 43, E8. [Google Scholar] [CrossRef]
- Ahn, Y.; Youn, M.S.; Heo, D.H. Endoscopic transforaminal lumbar interbody fusion: A comprehensive review. Expert Rev. Med. Devices 2019, 16, 373–380. [Google Scholar] [CrossRef]
- Faldini, C.; Borghi, R.; Chehrassan, M.; Perna, F.; Pilla, F.; Traina, F. Transforaminal lumbar interbody fusion. Eur. Spine J. 2017, 26, 429–430. [Google Scholar] [CrossRef] [PubMed]
- Heo, D.H.; Hong, Y.H.; Lee, D.C.; Chung, H.J.; Park, C.K. Technique of Biportal Endoscopic Transforaminal Lumbar Interbody Fusion. Neurospine 2020, 17, S129–S137. [Google Scholar] [CrossRef]
- Heo, D.H.; Lee, D.C.; Kim, H.S.; Park, C.K.; Chung, H. Clinical Results and Complications of Endoscopic Lumbar Interbody Fusion for Lumbar Degenerative Disease: A Meta-Analysis. World Neurosurg. 2020, 145, 396–404. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Wu, P.H.; Jang, I.-T. Technical note on Uniportal full endoscopic posterolateral approach transforaminal lumbar interbody fusion with reduction for grade 2 spondylolisthesis. Interdiscip. Neurosurg. 2020, 21, 100712. [Google Scholar] [CrossRef]
- Wu, P.H.; Kim, H.S.; Lee, Y.J.; Kim, D.H.; Lee, J.H.; Jeon, J.B.; Raorane, H.D.; Jang, I.-T. Uniportal Full Endoscopic Posterolateral Transforaminal Lumbar Interbody Fusion with Endoscopic Disc Drilling Preparation Technique for Symptomatic Foraminal Stenosis Secondary to Severe Collapsed Disc Space: A Clinical and Computer Tomographic Study with Technical Note. Brain Sci. 2020, 10, 373. [Google Scholar] [CrossRef]
- Kim, H.S.; Wu, P.H.; Lee, Y.J.; Kim, D.H.; Jang, I.T. Technical Considerations of Uniportal Endoscopic Posterolateral Lumbar Interbody Fusion: A Review of Its Early Clinical Results in Application in Adult Degenerative Scoliosis. World Neurosurg. 2020, 145, 682–692. [Google Scholar] [CrossRef]
- Wu, P.H.; Kim, H.S.; Jang, I.-T. Uniportal Endoscopic Lateral to Medial Direction Transforaminal Lumbar Interbody Fusion: A Case Report and Technical Guide for Navigating Through Landmarks in Left Lumbar 4/5 Post Laminotomy Revision Lumbar Fusion Surgery. J. Minim. Invasive Spine Surg. Tech. 2021, 6, 66–73. [Google Scholar] [CrossRef]
- Rauschning, W. Normal and Pathologic Anatomy of the Lumbar Root Canals. Spine 1987, 12, 1008–1019. [Google Scholar] [CrossRef]
- Wu, P.H.; Kim, H.S.; Jang, I.-T. A Narrative Review of Development of Full-Endoscopic Lumbar Spine Surgery. Neurospine 2020, 17, S20–S33. [Google Scholar] [CrossRef] [PubMed]
- McGrath, L.B.; White-Dzuro, G.A.; Hofstetter, C.P. Comparison of clinical outcomes following minimally invasive or lumbar endoscopic unilateral laminotomy for bilateral decompression. J. Neurosurg. Spine 2019, 30, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-W.; Yoon, K.-J.; Ha, S.-S. Comparative Analysis between Three Different Lumbar Decompression Techniques (Microscopic, Tubular, and Endoscopic) in Lumbar Canal and Lateral Recess Stenosis: Preliminary Report. BioMed Res. Int. 2019, 2019, 6078469. [Google Scholar] [CrossRef] [Green Version]
- Lin, G.-X.; Kotheeranurak, V.; Mahatthanatrakul, A.; Ruetten, S.; Yeung, A.; Lee, S.-H.; Ahn, Y.; Kim, H.-S.; Hofstetter, C.; Lee, J.H.; et al. Worldwide research productivity in the field of full-endoscopic spine surgery: A bibliometric study. Eur. Spine J. 2020, 29, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Morimoto, M.; Sairyo, K. Full-Endoscopic Trans-Kambin’s Triangle Lumbar Interbody Fusion (Fullendo-KLIF). In Transforaminal Full-Endoscopic Lumbar Surgery Under the Local Anesthesia: State of the Art; Sairyo, K., Ed.; Springer: Singapore, 2021; pp. 87–95. [Google Scholar]
- Morgenstern, C.; Yue, J.J.; Morgenstern, R. Full Percutaneous Transforaminal Lumbar Interbody Fusion Using the Facet-sparing, Trans-Kambin Approach. Clin. Spine Surg. 2020, 33, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Raorane, H.D.; Hung, W.P.; Heo, D.H.; Sharma, S.B.; Jang, I.T. Incidental Durotomy during Endoscopic Stenotic Lumbar Decompression (ESLD): Incidence, classification and proposed management strategies. World Neurosurg. 2020, 139, e13–e22. [Google Scholar] [CrossRef]
- Zhou, C.; Zhang, G.; Panchal, R.R.; Ren, X.; Xiang, H.; Xuexiao, M.; Chen, X.; Tongtong, G.; Hong, W.; Dixson, A.D. Unique Complications of Percutaneous Endoscopic Lumbar Discectomy and Percutaneous Endoscopic Interlaminar Discectomy. Pain Physician 2018, 21, E105–E112. [Google Scholar]
- Fan, G.; Han, R.; Gu, X.; Zhang, H.; Guan, X.; Fan, Y.; Wang, T.; He, S. Navigation improves the learning curve of transforamimal percutaneous endoscopic lumbar discectomy. Int. Orthop. 2017, 41, 323–332. [Google Scholar] [CrossRef]
- Palmer, S.; Turner, R.; Palmer, R. Bilateral decompression of lumbar spinal stenosis involving a unilateral approach with microscope and tubular retractor system. J. Neurosurg. 2002, 97, 213–217. [Google Scholar] [CrossRef]
- Rahman, M.; Summers, L.E.; Richter, B.; Mimran, R.I.; Jacob, R.P. Comparison of Techniques for Decompressive Lumbar Laminectomy: The Minimally Invasive versus the “Classic” Open Approach. Min-Minim. Invasive Neurosurg. 2008, 51, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Overdevest, G.; Vleggeert-Lankamp, C.; Jacobs, W.; Thome, C.; Gunzburg, R.; Peul, W. Effectiveness of posterior decompression techniques compared with conventional laminectomy for lumbar stenosis. Eur. Spine J. 2015, 24, 2244–2263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phan, K.; Mobbs, R.J. Minimally Invasive Versus Open Laminectomy for Lumbar Stenosis: A Systematic Review and Meta-Analysis. Spine 2016, 41, E91–E100. [Google Scholar] [CrossRef] [PubMed]
- Phan, K.; Xu, J.; Schultz, K.; Alvi, M.A.; Lu, V.M.; Kerezoudis, P.; Maloney, P.R.; Murphy, M.E.; Mobbs, R.J.; Bydon, M. Full-endoscopic versus micro-endoscopic and open discectomy: A systematic review and meta-analysis of outcomes and complications. Clin. Neurol. Neurosurg. 2017, 154, 1–12. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ETLIF (I) | ETLIF (O) | p Value | |
|---|---|---|---|
| Number of patients | 48 | 38 | N.A |
| Age (mean ± SD in years) | 65.02 ± 9.69 | 68.39 ± 11.41 | 0.142 |
| F/U Period (mean ± SD in months) | 14.73 ± 5.33 | 11.58 ± 3.81 | 0.003 |
| Operation Time For Inferior Articular Process Resection (mean ± SD in minutes) | 49.83 ± 23.97 | 36.55 ± 10.37 | 0.002 |
| Total Operation Time (mean ± SD min) | 102.56 ± 36.53 | 87.45 ± 20.14 | 0.025 |
| Disc Height Pre-operatively (mean ± SD mm) | 7.29 ± 3.07 | 7.63 ± 3.25 | 0.615 |
| Disc Height Post-operatively (mean ± SD mm) | 12.25 ± 2.74 | 13.12 ± 1.88 | 0.097 |
| Coronal Wedging Pre-operatively (mean ± SD°) | 5.54 ± 3.75 | 6.09 ± 5.67 | 0.591 |
| Coronal Wedging Post-operatively (mean ± SD°) | 3.78 ± 2.73 | 2.85 ± 1.72 | 0.071 |
| Preoperative VAS (mean ± SD) | 7.65 ± 1.25 | 7.58 ± 1.31 | 0.809 |
| Postoperative VAS at 1 week (mean ± SD) | 3.44 ± 0.85 | 3.26 ± 0.64 | 0.297 |
| Postoperative VAS at 3 months (mean ± SD) | 2.33 ± 0.88 | 2.39 ± 0.82 | 0.742 |
| Postoperative VAS at final follow up (mean ± SD) | 1.83 ± 0.86 | 2.16 ± 0.86 | 0.085 |
| Preoperative ODI (mean ± SD) | 74.38 ± 8.72 | 73.21 ± 10.62 | 0.578 |
| Postoperative ODI at 1 week (mean ± SD) | 33.50 ± 6.52 | 32.63 ± 5.44 | 0.587 |
| Postoperative ODI at 3 months (mean ± SD) | 26.25 ± 4.72 | 27.16 ± 5.31 | 0.659 |
| Postoperative ODI at final follow up (mean ± SD) | 23.81 ± 4.85 | 25.05 ± 5.52 | 0.404 |
| Percentage MacNab Good To Excellent (%) | 97.9 | 97.4 | 0.271 |
| ETLIF (I) | Mean | Std. Deviation | p Value |
|---|---|---|---|
| VAS improvement at 1 weeks | 4.21 | 1.49 | p < 0.001 |
| VAS improvement at 3 months | 5.31 | 1.68 | p < 0.001 |
| VAS improvement at final follow up | 5.81 | 1.61 | p < 0.001 |
| ODI improvement at 1 weeks | 40.88 | 11.23 | p < 0.001 |
| ODI improvement at 3 months | 48.13 | 10.86 | p < 0.001 |
| ODI improvement at final follow up | 50.56 | 10.63 | p < 0.001 |
| Disc Height Increment (mm) | 5.00 | 2.87 | p < 0.001 |
| Coronal Wedge Angle Improvement (°) | 1.76 | 1.63 | p < 0.001 |
| ETLIF (O) | Mean | Std. Deviation | p Value |
|---|---|---|---|
| VAS improvement at 1 weeks | 4.32 | 1.32 | p < 0.001 |
| VAS improvement at 3 months | 5.18 | 1.47 | p < 0.001 |
| VAS improvement at final follow up | 5.42 | 1.48 | p < 0.001 |
| ODI improvement at 1 weeks | 40.58 | 10.17 | p < 0.001 |
| ODI improvement at 3 months | 46.05 | 10.80 | p < 0.001 |
| ODI improvement at final follow up | 48.16 | 11.71 | p < 0.001 |
| Disc Height Increment (mm) | 5.49 | 2.33 | p < 0.001 |
| Coronal Wedging Improvement (°) | 2.87 | 2.25 | p < 0.001 |
| Group Charateristics | ETLIF (I) Mean ± SD | ETLIF (O) Mean ± SD | p Value |
|---|---|---|---|
| Improvement of VAS at 1 week | 4.21 ± 1.49 | 4.32 ± 1.32 | 0.727 |
| Improvement of VAS at 3 months | 1.10 ± 0.83 | 0.87 ± 0.67 | 0.158 |
| Improvement of VAS at final FU | 0.50 ± 0.74 | 0.24 ± 0.59 | 0.078 |
| Improvement of ODI at 1 week | 40.88 ± 11.23 | 40.58 ± 10.16 | 0.900 |
| Improvement of ODI at 3 months | 7.25 ± 4.68 | 5.47 ± 4.05 | 0.067 |
| Improvement of ODI at final FU | 2.44 ± 3.48 | 2.11 ± 3.54 | 0.663 |
| Change In Disc Height(Postop-Preop) (mean ± SD mm) | 5.00 ± 2.87 | 5.49 ± 2.33 | 0.394 |
| Change In Cornoal Wedging Angle(Postop-Preop) (mean ± SD°) | 1.76 ± 1.63 | 3.24 ± 2.92 | 0.072 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.-S.; Wu, P.-H.; An, J.-W.; Lee, Y.-J.; Lee, J.-H.; Kim, M.-H.; Lee, I.; Park, J.-S.; Lee, J.-H.; Park, J.-H.; et al. Evaluation of Two Methods (Inside-Out/Outside-In) Inferior Articular Process Resection for Uniportal Full Endoscopic Posterolateral Transforaminal Lumbar Interbody Fusion: Technical Note. Brain Sci. 2021, 11, 1169. https://doi.org/10.3390/brainsci11091169
Kim H-S, Wu P-H, An J-W, Lee Y-J, Lee J-H, Kim M-H, Lee I, Park J-S, Lee J-H, Park J-H, et al. Evaluation of Two Methods (Inside-Out/Outside-In) Inferior Articular Process Resection for Uniportal Full Endoscopic Posterolateral Transforaminal Lumbar Interbody Fusion: Technical Note. Brain Sciences. 2021; 11(9):1169. https://doi.org/10.3390/brainsci11091169
Chicago/Turabian StyleKim, Hyeun-Sung, Pang-Hung Wu, Jin-Woo An, Yeon-Jin Lee, Jun-Hyung Lee, Myeong-Hun Kim, Inkyung Lee, Jong-Sung Park, Jun-Hyung Lee, Jun-Hwan Park, and et al. 2021. "Evaluation of Two Methods (Inside-Out/Outside-In) Inferior Articular Process Resection for Uniportal Full Endoscopic Posterolateral Transforaminal Lumbar Interbody Fusion: Technical Note" Brain Sciences 11, no. 9: 1169. https://doi.org/10.3390/brainsci11091169
APA StyleKim, H.-S., Wu, P.-H., An, J.-W., Lee, Y.-J., Lee, J.-H., Kim, M.-H., Lee, I., Park, J.-S., Lee, J.-H., Park, J.-H., & Jang, I.-T. (2021). Evaluation of Two Methods (Inside-Out/Outside-In) Inferior Articular Process Resection for Uniportal Full Endoscopic Posterolateral Transforaminal Lumbar Interbody Fusion: Technical Note. Brain Sciences, 11(9), 1169. https://doi.org/10.3390/brainsci11091169