
Motor Imagery of Walking in People Living with and without Multiple Sclerosis: A Cross-Sectional Comparison of Mental Chronometry



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Study Participants
2.3. Procedures
2.4. Statistical Analysis
3. Results
3.1. Study Participants
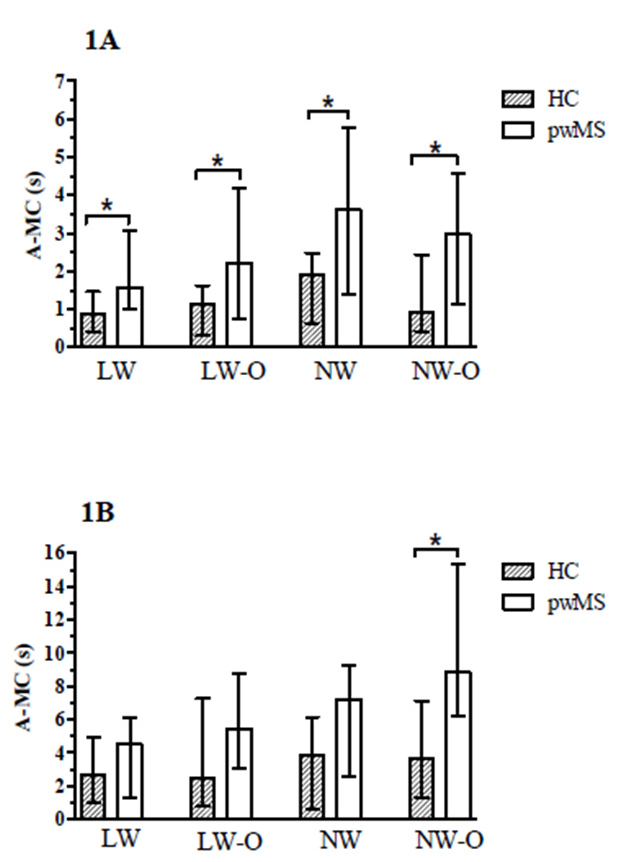
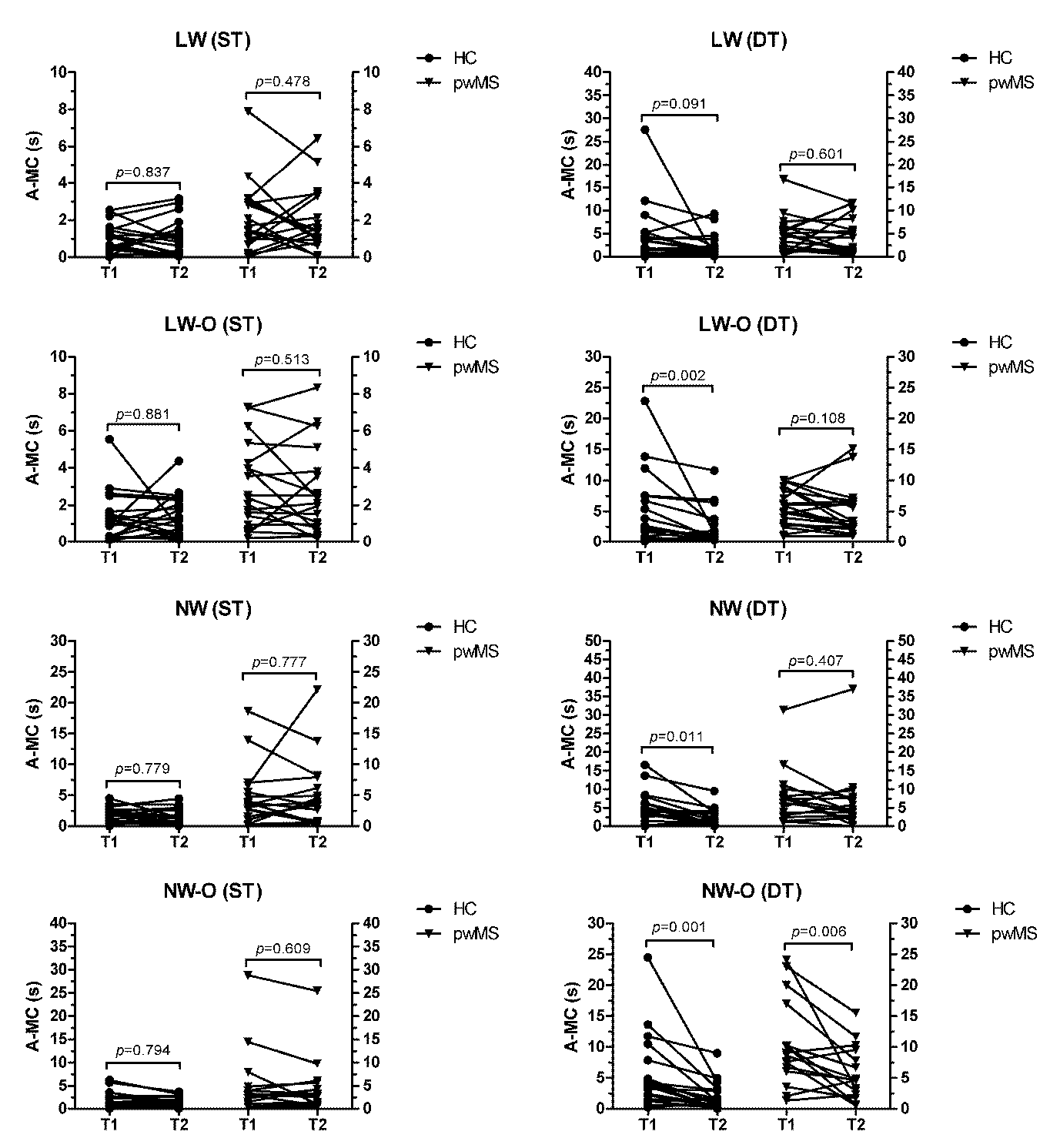
3.2. Mental Chronometry
3.3. Correlation Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Savaki, H.E.; Raos, V. Action perception and motor imagery: Mental practice of action. Prog. Neurobiol. 2019, 175, 107–125. [Google Scholar] [CrossRef]
- Krüger, B.; Hettwer, M.; Zabicki, A.; de Haas, B.; Munzert, J.; Zentgraf, K. Practice modality of motor sequences impacts the neural signature of motor imagery. Sci. Rep. 2020, 10, 19176. [Google Scholar] [CrossRef]
- Hardwick, R.M.; Caspers, S.; Eickhoff, S.B.; Swinnen, S.P. Neural correlates of action: Comparing meta-analyses of imagery, observation, and execution. Neurosci. Biobehav. Rev. 2018, 94, 31–44. [Google Scholar] [CrossRef] [PubMed]
- Ryckewaert, G.; Luyat, M.; Rambour, M.; Tard, C.; Noël, M.; Defebvre, L.; Delval, A. Self-perceived and actual ability in the functional reach test in patients with Parkinson’s disease. Neurosci. Lett. 2015, 589, 181–184. [Google Scholar] [CrossRef] [PubMed]
- Greiner, J.; Schoenfeld, M.A.; Liepert, J. Assessment of mental chronometry (MC) in healthy subjects. Arch. Gerontol. Geriatr. 2014, 58, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.E.; Guillot, A.; Di Rienzo, F.; Cumming, J. Comparing self-report and mental chronometry measures of motor imagery ability. Eur. J. Sport Sci. 2015, 15, 703–711. [Google Scholar] [CrossRef] [PubMed]
- Saimpont, A.; Malouin, F.; Tousignant, B.; Jackson, P.L. Motor imagery and aging. J. Mot. Behav. 2013, 45, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Lafargue, G.; Noël, M.; Luyat, M. In the elderly, failure to update internal models leads to over-optimistic predictions about upcoming actions. PLoS ONE 2013, 8, e51218. [Google Scholar] [CrossRef]
- Wallin, M.T.; Culpepper, W.J.; Campbell, J.D.; Nelson, L.M.; Langer-Gould, A.; Marrie, R.A.; Cutter, G.R.; Kaye, W.E.; Wagner, L.; Tremlett, H.; et al. The prevalence of MS in the United States: A population-based estimate using health claims data. Neurology 2019, 92, e1029–e1040. [Google Scholar] [CrossRef] [Green Version]
- Ghasemi, N.; Razavi, S.; Nikzad, E. Multiple Sclerosis: Pathogenesis, Symptoms, Diagnoses and Cell-Based Therapy. Cell J. 2017, 19, 1–10. [Google Scholar] [PubMed]
- Tacchino, A.; Bove, M.; Pedullà, L.; Battaglia, M.A.; Papaxanthis, C.; Brichetto, G. Imagined actions in multiple sclerosis patients: Evidence of decline in motor cognitive prediction. Exp. Brain Res. 2013, 229, 561–570. [Google Scholar] [CrossRef] [PubMed]
- Podda, J.; Pedullà, L.; Monti Bragadin, M.; Piccardo, E.; Battaglia, M.A.; Brichetto, G.; Bove, M.; Tacchino, A. Spatial constraints and cognitive fatigue affect motor imagery of walking in people with multiple sclerosis. Sci. Rep. 2020, 10, 21938. [Google Scholar] [CrossRef] [PubMed]
- Heremans, E.; D’hooge, A.M.; De Bondt, S.; Helsen, W.; Feys, P. The relation between cognitive and motor dysfunction and motor imagery ability in patients with multiple sclerosis. Mult. Scler. 2012, 18, 1303–1309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanson, M.; Concialdi, M. Motor imagery in multiple sclerosis: Exploring applications in therapeutic treatment. J. Neurophysiol. 2019, 121, 347–349. [Google Scholar] [CrossRef] [Green Version]
- Seebacher, B.; Kuisma, R.; Glynn, A.; Berger, T. Exploring cued and non-cued motor imagery interventions in people with multiple sclerosis: A randomised feasibility trial and reliability study. Arch. Physiother. 2018, 8, 6. [Google Scholar] [CrossRef] [Green Version]
- Cameron, M.H.; Nilsagard, Y. Balance, gait, and falls in multiple sclerosis. Handb. Clin. Neurol. 2018, 159, 237–250. [Google Scholar]
- Bentvelzen, A.C.; Crawford, J.D.; Theobald, A.; Maston, K.; Slavin, M.J.; Reppermund, S.; Kang, K.; Numbers, K.; Brodaty, H.; Sachdev, P.; et al. Validation and Normative Data for the Modified Telephone Interview for Cognitive Status: The Sydney Memory and Ageing Study. J. Am. Geriatr. Soc. 2019, 67, 2108–2115. [Google Scholar] [CrossRef]
- Wong-Yu, I.S.; Mak, M.K. Multi-dimensional balance training programme improves balance and gait performance in people with Parkinson’s disease: A pragmatic randomized controlled trial with 12-month follow-up. Parkinsonism Relat. Disord. 2015, 21, 615–621. [Google Scholar] [CrossRef]
- Springer, S.; Giladi, N.; Peretz, C.; Yogev, G.; Simon, E.S.; Hausdorff, J.M. Dual-tasking effects on gait variability: The role of aging, falls, and executive function. Mov. Disord. 2006, 21, 950–957. [Google Scholar] [CrossRef]
- Gunn, H.; Creanor, S.; Haas, B.; Marsden, J.; Freeman, J. Risk factors for falls in multiple sclerosis: An observational study. Mult. Scler. 2013, 19, 1913–1922. [Google Scholar] [CrossRef]
- Nakano, H.; Murata, S.; Shiraiwa, K.; Nonaka, K. Increased Time Difference between Imagined and Physical Walking in Older Adults at a High Risk of Falling. Brain Sci. 2020, 10, 332. [Google Scholar] [CrossRef]
- Singh, D.K.; Pillai, S.G.; Tan, S.T.; Tai, C.C.; Shahar, S. Association between physiological falls risk and physical performance tests among community-dwelling older adults. Clin. Interv. Aging. 2015, 10, 1319–1326. [Google Scholar] [CrossRef] [Green Version]
- Lord, S.R.; Delbaere, K.; Gandevia, S.C. Use of a physiological profile to document motor impairment in ageing and in clinical groups. J. Physiol. 2016, 594, 4513–4523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powell, L.E.; Myers, A.M. The Activities-specific Balance Confidence (ABC) Scale. J. Gerontol. A Biol. Sci. Med. Sci. 1995, 50, M28–M34. [Google Scholar] [CrossRef] [PubMed]
- Nilsagård, Y.; Carling, A.; Forsberg, A. Activities-specific balance confidence in people with multiple sclerosis. Mult. Scler. Int. 2012, 2012, 613925. [Google Scholar] [CrossRef] [Green Version]
- Hoang, P.D.; Baysan, M.; Gunn, H.; Cameron, M.; Freeman, J.; Nitz, J.; Low Choy, N.L.; Lord, S.R. Fall risk in people with MS: A Physiological Profile Assessment study. Mult. Scler. J. Exp. Transl. Clin. 2016, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunn, H.; Cameron, M.; Hoang, P.; Lord, S.; Shaw, S.; Freeman, J. Relationship Between Physiological and Perceived Fall Risk in People With Multiple Sclerosis: Implications for Assessment and Management. Arch. Phys. Med. Rehabil. 2018, 99, 2022–2029. [Google Scholar] [CrossRef] [PubMed]
- Leone, C.; Patti, F.; Feys, P. Measuring the cost of cognitive-motor dual tasking during walking in multiple sclerosis. Mult. Scler. J. 2015, 21, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Sacheli, L.M.; Zapparoli, L.; De Santis, C.; Preti, M.; Pelosi, C.; Ursino, N.; Zerbi, A.; Banfi, G.; Paulesu, E. Mental steps: Differential activation of internal pacemakers in motor imagery and in mental imitation of gait. Hum. Brain Mapp. 2017, 38, 5195–5216. [Google Scholar] [CrossRef] [Green Version]
- Strik, M.; Chard, D.T.; Dekker, I.; Meijer, K.A.; Eijlers, A.J.; Pardini, M.; Uitdehaag, B.M.; Kolbe, S.C.; Geurts, J.J.; Schoonheim, M.M. Increased functional sensorimotor network efficiency relates to disability in multiple sclerosis. Mult. Scler. 2020. [Google Scholar] [CrossRef]
- Allali, G.; Blumen, H.M.; Devanne, H.; Pirondini, E.; Delval, A.; Van De Ville, D. Brain imaging of locomotion in neurological conditions. Neurophysiol. Clin. 2018, 48, 337–359. [Google Scholar] [CrossRef]
- Kouvatsou, Z.; Masoura, E.; Kiosseoglou, G.; Kimiskidis, V.K. Working memory profiles of patients with multiple sclerosis: Where does the impairment lie? J. Clin. Exp. Neuropsychol. 2019, 41, 832–844. [Google Scholar] [CrossRef]
- Costers, L.; Van Schependom, J.; Laton, J.; Baijot, J.; Sjøgård, M.; Wens, V.; De Tiège, X.; Goldman, S.; D’Haeseleer, M.; D’hooghe, M.B.; et al. The role of hippocampal theta oscillations in working memory impairment in multiple sclerosis. Hum. Brain Mapp. 2021, 42, 1376–1390. [Google Scholar] [CrossRef]
- Nakano, H.; Murata, S.; Shiraiwa, K.; Iwase, H.; Kodama, T. Temporal characteristics of imagined and actual walking in frail older adults. Aging Clin. Exp. Res. 2018, 30, 1453–1457. [Google Scholar] [CrossRef] [PubMed]
- Beauchet, O.; Launay, C.P.; Sejdić, E.; Allali, G.; Annweiler, C. Motor imagery of gait: A new way to detect mild cognitive impairment? J. Neuroeng. Rehabil. 2014, 11, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yogev-Seligmann, G.; Hausdorff, J.M.; Giladi, N. Do we always prioritize balance when walking? Towards an integrated model of task prioritization. Mov. Disord. 2012, 27, 765–770. [Google Scholar]
- Nilsagård, Y.; Westerdahl, E.; Wittrin, A.; Gunnarsson, M. Walking Distance as a Predictor of Falls in People With Multiple Sclerosis. Physiother. Res. Int. 2016, 21, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Seebacher, B.; Kuisma, R.; Glynn, A.; Berger, T. The effect of rhythmic-cued motor imagery on walking, fatigue and quality of life in people with multiple sclerosis: A randomised controlled trial. Mult. Scler. 2017, 23, 286–296. [Google Scholar] [CrossRef] [PubMed]
- Gil-Bermejo-Bernardez-Zerpa, A.; Moral-Munoz, J.A.; Lucena-Anton, D.; Luque-Moreno, C. Effectiveness of Motor Imagery on Motor Recovery in Patients with Multiple Sclerosis: Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 498. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | All Participants (40) | HC (20) | pwMS (20) | p-Value |
|---|---|---|---|---|
| Age (years) | 57.6 ± 7.8 | 58.1 ± 7 | 57.1 ± 8.6 | 0.690 |
| Gender (% F) | 57.5 | 60 | 55 | 0.749 |
| SREDSS (score) | - | - | 3.8 (3.3) | N.A. |
| MS duration (years) | - | - | 17 ± 8.3 | N.A. |
| PPA (score) | 1.1 ± 1.3 | 0.2 ± 0.8 | 2 ± 1.2 | <0.001 |
| ABC scale (score) | 82.8 ± 17.7 | 92.1 ± 7.2 | 73.5 ± 20.2 | 0.002 |
| LW | LW-O | NW | NW-O | |||||
|---|---|---|---|---|---|---|---|---|
| HC | pwMS | HC | pwMS | HC | pwMS | HC | pwMS | |
| ST | ||||||||
| T1 | −0.65 ± 1.10 | −0.68 ± 2.75 | 0.03 ± 1.90 | −0.70 ± 3.63 | 0.07 ± 2.20 | −1.53 ± 6.56 | −0.33 ± 2.38 | −2.38 ± 8.61 |
| T2 | −0.50 ± 1.30 | −0.48 ± 2.50 | −0.64 ± 1.66 | −0.90 ± 3.41 | 0.05 ± 2.12 | −2.54 ± 7.02 | −0.75 ± 1.63 | −2.90 ± 7.07 |
| DT | ||||||||
| T1 | 4.40 ± 6.25 | 4.27 ± 4.14 | 3.38 ± 6.72 | 3.55 ± 5.43 | 3.49 ± 5.41 | 5.63 ± 9.17 | 4.40 ± 6.66 | 5.06 ± 11.76 |
| T2 | 1.83 ± 2.78 | 4.34 ± 4.26 | 0.46 ± 3.65 | 3.64 ± 4.99 | 1.37 ± 2.94 | 4.22 ± 9.85 | 1.14 ± 2.73 | 0.39 ± 7.27 |
| Large-Width Walkway | Narrow-Width Walkway | ||||
|---|---|---|---|---|---|
| Condition | Group | LW | LW-O | NW | NW-O |
| ST | HC | −0.155 (↑17.9%) | +0.055 (↓4.8%) | −0.455 (↑23.8%) | +0.305 (↓32.3%) |
| ST | pwMS | −0.240 (↑15.3%) | −0.190 (↑8.6%) | +0.035 (↓1.0%) | −0.045 (↑1.5%) |
| DT | HC | −1.220 (↑46.0%) | −1.365 (↑54.9%) | −2.080 (↑53.5%) | −2.400 (↑64.9%) |
| DT | pwMS | −1.500 (↑33.1%) | −2.365 (↑43.4%) | −3.270 (↑45.5%) | −4.195 (↑47.4%) |
| Large-Width Walkway | Narrow-Width Walkway | ||||
|---|---|---|---|---|---|
| Variables | LW | LW-O | NW | NW-O | |
| HC | PPA | −0.082 | 0.144 | 0.323 | 0.001 |
| ABC | 0.124 | 0.037 | −0.249 | −0.049 | |
| SR-EDSS | n.a. | n.a. | n.a. | n.a. | |
| pwMS | PPA | 0.080 | 0.408 | 0.342 | −0.006 |
| ABC | −0.199 | −0.629 ** | −0.501 * | 0.024 | |
| SR-EDSS | 0.260 | 0.747 ** | 0.521 * | 0.180 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wajda, D.A.; Zanotto, T.; Sosnoff, J.J. Motor Imagery of Walking in People Living with and without Multiple Sclerosis: A Cross-Sectional Comparison of Mental Chronometry. Brain Sci. 2021, 11, 1131. https://doi.org/10.3390/brainsci11091131
Wajda DA, Zanotto T, Sosnoff JJ. Motor Imagery of Walking in People Living with and without Multiple Sclerosis: A Cross-Sectional Comparison of Mental Chronometry. Brain Sciences. 2021; 11(9):1131. https://doi.org/10.3390/brainsci11091131
Chicago/Turabian StyleWajda, Douglas A., Tobia Zanotto, and Jacob J. Sosnoff. 2021. "Motor Imagery of Walking in People Living with and without Multiple Sclerosis: A Cross-Sectional Comparison of Mental Chronometry" Brain Sciences 11, no. 9: 1131. https://doi.org/10.3390/brainsci11091131
APA StyleWajda, D. A., Zanotto, T., & Sosnoff, J. J. (2021). Motor Imagery of Walking in People Living with and without Multiple Sclerosis: A Cross-Sectional Comparison of Mental Chronometry. Brain Sciences, 11(9), 1131. https://doi.org/10.3390/brainsci11091131