
Effects of Aquatic Exercise and Land-Based Exercise on Cardiorespiratory Fitness, Motor Function, Balance, and Functional Independence in Stroke Patients—A Meta-Analysis of Randomized Controlled Trials


Abstract
1. Introduction
2. Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Quality Assessment
2.4. Data Extraction
2.5. Statistical Analysis
3. Results
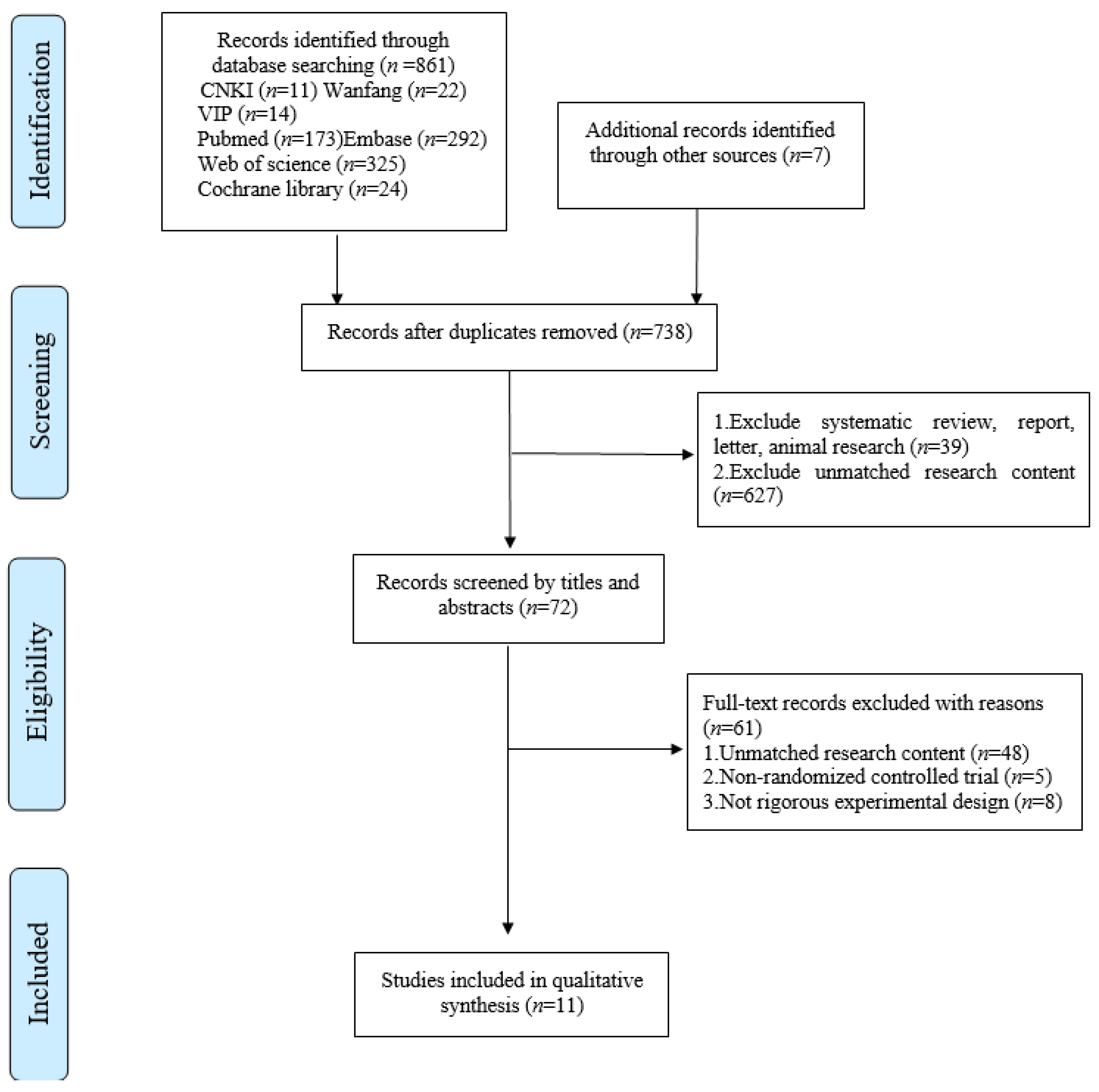
3.1. Study Selection
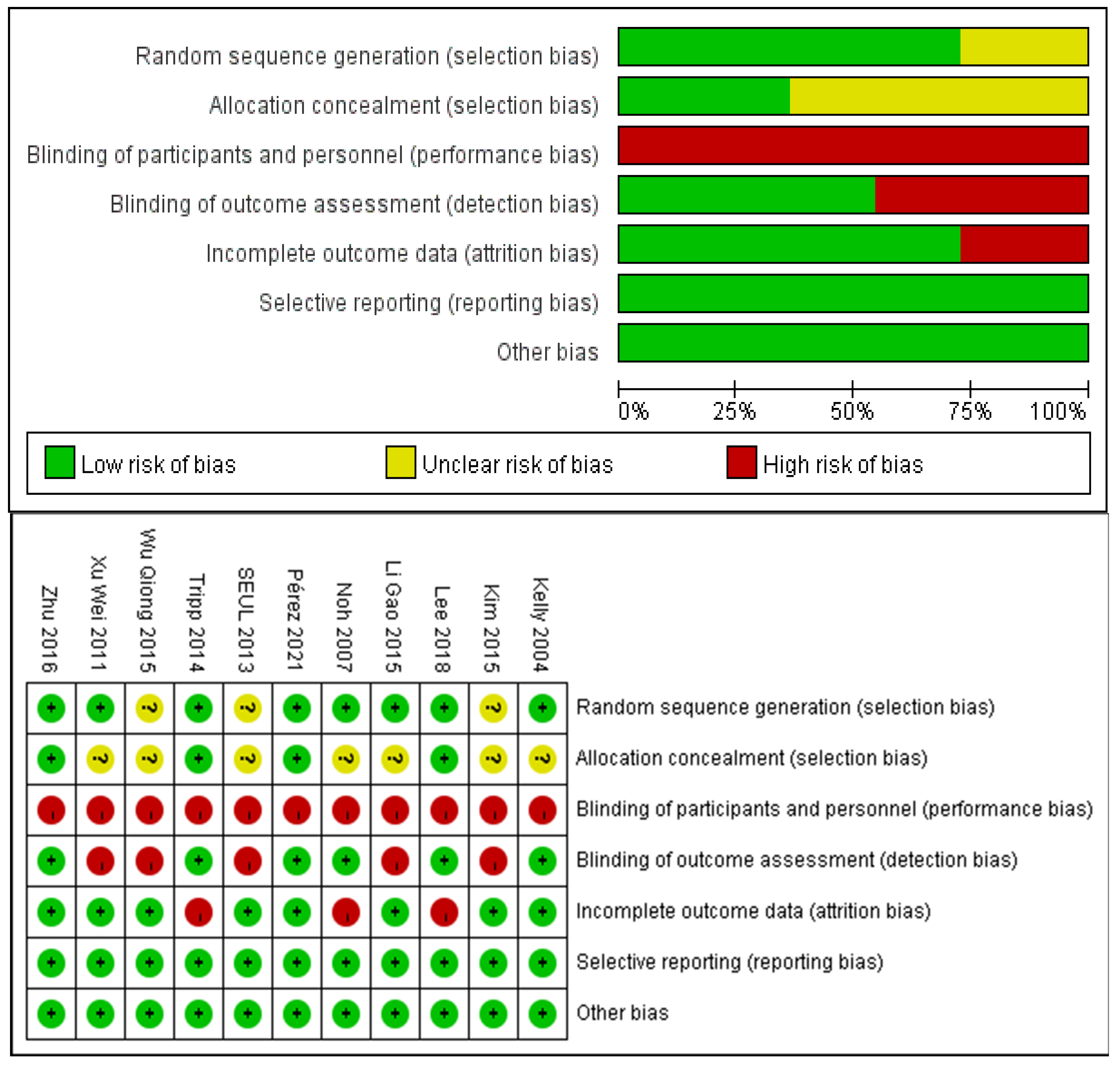
3.2. Risk of Bias Assessment
3.3. Study Characteristics
4. Meta-Analysis
4.1. Berg Balance Scale (BBS)
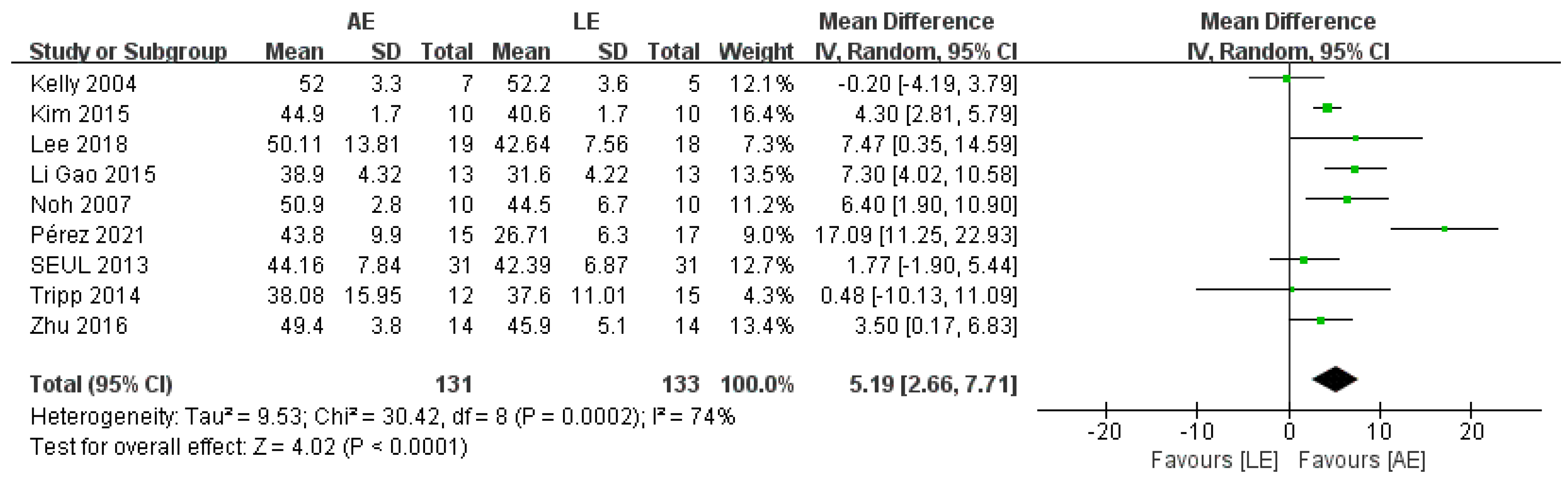
4.2. Fugl–Meyer Assessment (FMA)
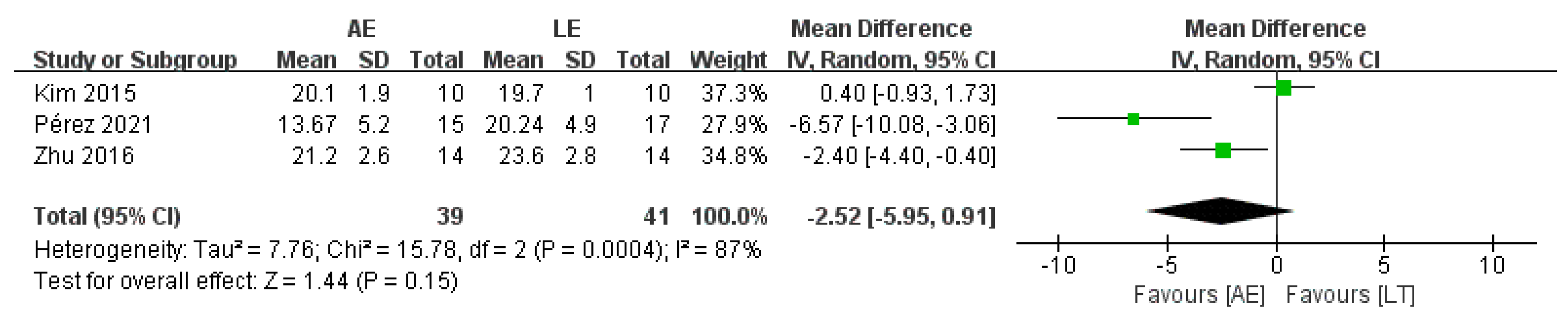
4.3. Timed Up and Go Test (TUGT)
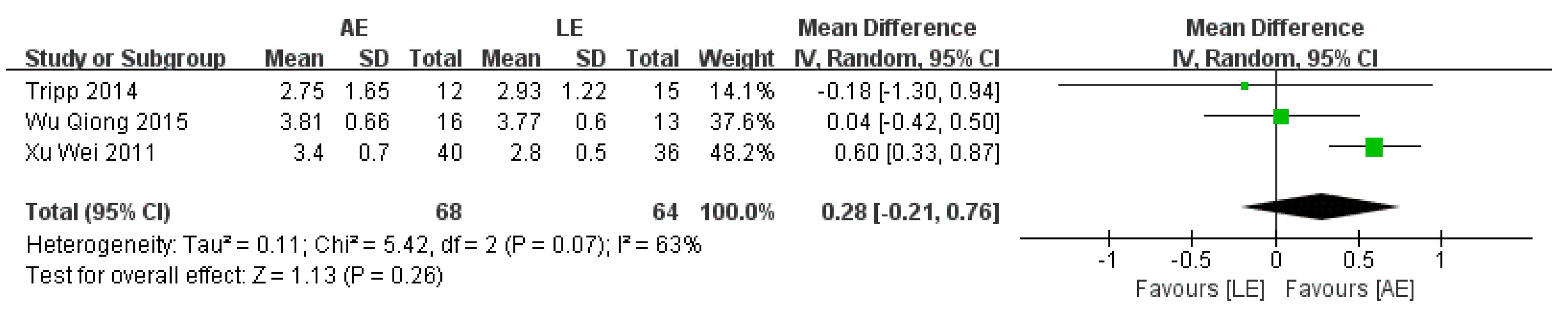
4.4. Functional Ambulation Category Scale (FAC)
4.5. Peak Oxygen Uptake (VO2peak)
4.6. Functional Independence Measure (FIM)
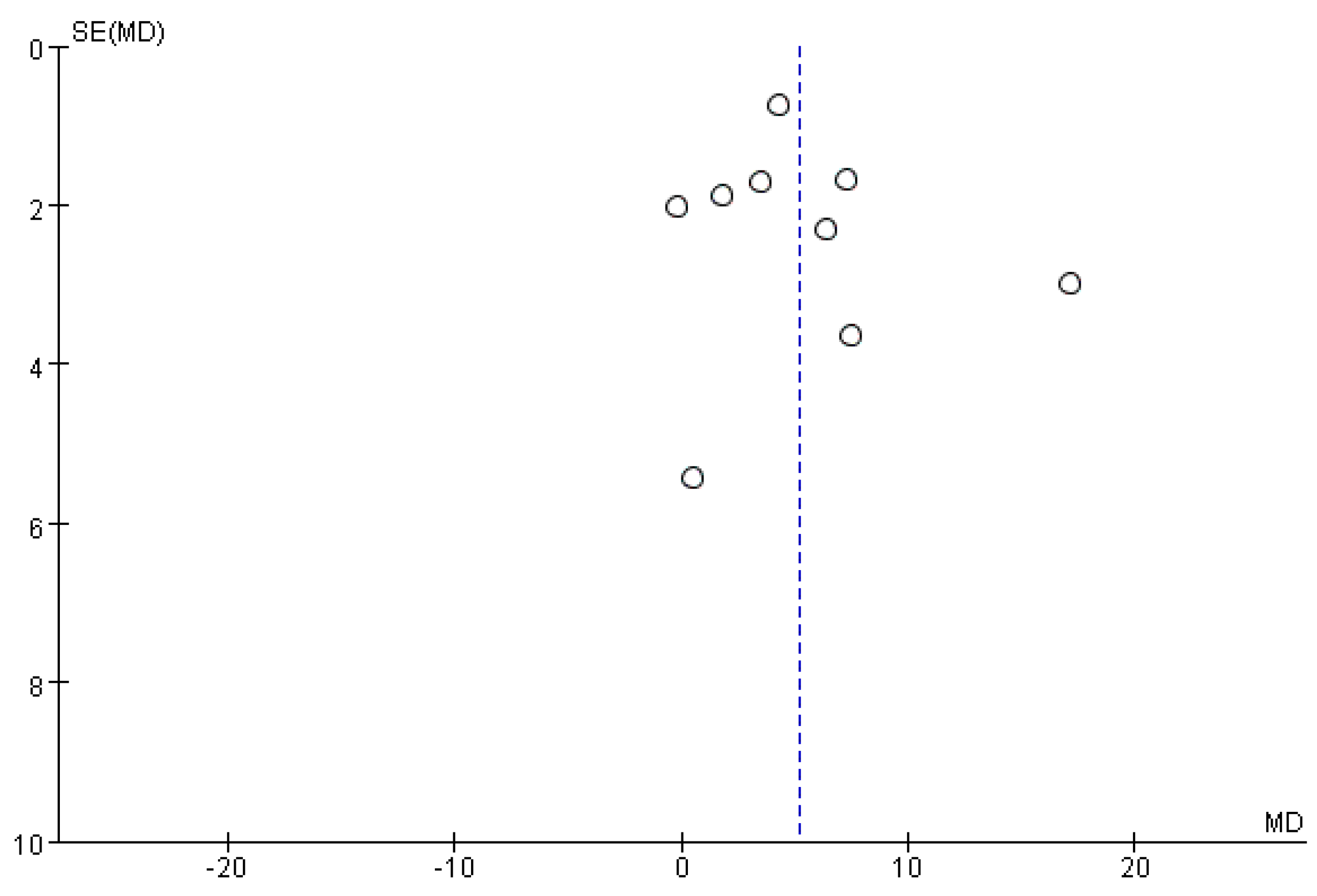
4.7. Publication Bias
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De La Cruz, S.P. Influence of an Aquatic Therapy Program on Perceived Pain, Stress, and Quality of Life in Chronic Stroke Patients: A Randomized Trial. Int. J. Environ. Res. Public Health 2020, 17, 4796. [Google Scholar] [CrossRef] [PubMed]
- Donkor, E.S. Stroke in the 21st Century: A Snapshot of the Burden, Epidemiology, and Quality of Life. Stroke Res. Treat. 2018, 2018, 3238165. [Google Scholar] [CrossRef] [PubMed]
- Han, P.; Zhang, W.; Kang, L.; Ma, Y.; Fu, L.; Jia, L.; Yu, H.; Chen, X.; Hou, L.; Wang, L.; et al. Clinical Evidence of Exercise Benefits for Stroke. Adv. Exp. Med. Biol. 2017, 1000, 131–151. [Google Scholar] [CrossRef]
- Lincoln, N.; Flannaghan, T. Cognitive Behavioral Psychotherapy for Depression Following Stroke. Stroke 2003, 34, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.; Rathore, C.; Kate, M.; Joy, J.; Zachariah, G.; Vincent, P.C.; Varma, R.P.; Radhakrishnan, K. The comparative efficacy of theta burst stimulation or functional electrical stimulation when combined with physical therapy after stroke: A randomized controlled trial. Clin. Rehabil. 2019, 33, 693–703. [Google Scholar] [CrossRef]
- Han, S.K.; Kim, M.C.; An, C.S. Comparison of Effects of a Proprioceptive Exercise Program in Water and on Land the Balance of Chronic Stroke Patients. J. Phys. Ther. Sci. 2013, 25, 1219–1222. [Google Scholar] [CrossRef][Green Version]
- Zhu, Z.; Cui, L.; Yin, M.; Yu, Y.; Zhou, X.; Wang, H.; Yan, H. Hydrotherapy vs. conventional land-based exercise for improving walking and balance after stroke: A randomized controlled trial. Clin. Rehabil. 2015, 30, 587–593. [Google Scholar] [CrossRef]
- Noh, D.K.; Lim, J.-Y.; Shin, H.-I.; Paik, N.-J. The effect of aquatic therapy on postural balance and muscle strength in stroke survivors—A randomized controlled pilot trial. Clin. Rehabil. 2008, 22, 966–976. [Google Scholar] [CrossRef]
- Lee, J.; Stone, A.J. Combined Aerobic and Resistance Training for Cardiorespiratory Fitness, Muscle Strength, and Walking Capacity after Stroke: A Systematic Review and Meta-Analysis. J. Stroke Cerebrovasc. Dis. 2019, 29, 104498. [Google Scholar] [CrossRef]
- Kim, H.; Lee, H.; Seo, K. The Effects of Dual-Motor Task Training on the Gait Ability of Chronic Stroke Patients. J. Phys. Ther. Sci. 2013, 25, 317–320. [Google Scholar] [CrossRef]
- Saleh, M.S.M.; Rehab, N.I.; Aly, S.M.A. Effect of aquatic versus land motor dual task training on balance and gait of patients with chronic stroke: A randomized controlled trial. NeuroRehabilitation 2019, 44, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Tripp, F.; Krakow, K. Effects of an aquatic therapy approach (Halliwick-Therapy) on functional mobility in subacute stroke patients: A randomized controlled trial. Clin. Rehabil. 2014, 28, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Tamin, T.Z.; Loekito, N. Aquatic versus land-based exercise for cardiorespiratory endurance and quality of life in obese patients with knee osteoarthritis: A randomized controlled trial. Med. J. Indones. 2018, 27, 284–292. [Google Scholar] [CrossRef]
- De La Cruz, S.P. Comparison of Aquatic Therapy vs. Dry Land Therapy to Improve Mobility of Chronic Stroke Patients. Int. J. Environ. Res. Public Health 2020, 17, 4728. [Google Scholar] [CrossRef]
- Kim, E.-K.; Lee, D.-K.; Kim, Y.-M. Effects of aquatic PNF lower extremity patterns on balance and ADL of stroke patients. J. Phys. Ther. Sci. 2015, 27, 213–215. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Im, S.H.; Kim, B.R.; Han, E.Y. The Effects of a Motorized Aquatic Treadmill Exercise Program on Muscle Strength, Cardiorespiratory Fitness, and Clinical Function in Subacute Stroke Patients. Am. J. Phys. Med. Rehabil. 2018, 97, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Nayak, P.; Mahmood, A.; Natarajan, M.; Hombali, A.; Prashanth, C.; Solomon, J.M. Effect of aquatic therapy on balance and gait in stroke survivors: A systematic review and meta-analysis. Complement. Ther. Clin. Pr. 2020, 39, 101110. [Google Scholar] [CrossRef]
- Giuriati, S.; Servadio, A.; Temperoni, G.; Curcio, A.; Valente, D.; Galeoto, G. The effect of aquatic physical therapy in patients with stroke: A systematic review and meta-analysis. Top. Stroke Rehabil. 2021, 28, 19–32. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. Cochrane Collab. 2011, 2, 126–130. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Chu, K.S.; Eng, J.J.; Dawson, A.S.; Harris, J.E.; Ozkaplan, A.; Gylfadóttir, S. Water-based exercise for cardiovascular fitness in people with chronic stroke: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2004, 85, 870–874. [Google Scholar] [CrossRef]
- Xu, W.; Fan, J.T.; Zhang, L.Y.; Yang, X.; Wang, Y.Z. Effects of water sports training and weight-loss walking training on walking ability of stroke patients with hemiplegia. Chin. J. Phys. Med. Rehabil. 2011, 33, 469–470. [Google Scholar] [CrossRef]
- Wu, Q.; Cong, F.; Song, G. Comparison of Effects between Underwater and Body Weight Support Treadmill Training on Walking and Balance in Hemiplegics after Stroke. Chin. J. Rehabil. Theory Pract. 2015, 21, 207–211. [Google Scholar] [CrossRef]
- Li, G. Effect of muscle strength training combined with water walking training on lower limb function recovery of stroke patients with hemiplegia. Chin. J. Phys. Med. Rehabil. 2015, 37, 942–944. [Google Scholar] [CrossRef]
- De La Cruz, S.P. Comparison between Three Therapeutic Options for the Treatment of Balance and Gait in Stroke: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 426. [Google Scholar] [CrossRef] [PubMed]
- Pin-Barre, C.; Laurin, J. Physical Exercise as a Diagnostic, Rehabilitation, and Preventive Tool: Influence on Neuroplasticity and Motor Recovery after Stroke. Neural Plast. 2015, 2015, 608581. [Google Scholar] [CrossRef] [PubMed]
- Ijmker, T.; Houdijk, H.; Lamoth, C.; Jarbandhan, A.V.; Rijntjes, D.; Beek, P.J.; van der Woude, L. Effect of Balance Support on the Energy Cost of Walking After Stroke. Arch. Phys. Med. Rehabil. 2013, 94, 2255–2261. [Google Scholar] [CrossRef]
- Berg, K.O.; Maki, B.E.; Williams, J.I.; Holliday, P.J.; Wood-Dauphinee, S.L. Clinical and laboratory measures of postural balance in an elderly population. Arch. Phys. Med. Rehabil. 1992, 73, 1073–1080. [Google Scholar]
- Andersson, A.G.; Kamwendo, K.; Seiger, Å.; Appelros, P. How to identify potential fallers in a stroke unit: Validity indexes of four test methods. J. Rehabil. Med. 2006, 38, 186–191. [Google Scholar] [CrossRef]
- Kollen, B.; Van De Port, I.; Lindeman, E.; Twisk, J.; Kwakkel, G. Predicting Improvement in Gait After Stroke. Stroke 2005, 36, 2676–2680. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Chaoqin, D. The Effect of Water Intensive Walking Training on the Recovery of Walking Ability of Hemiplegia Patients with Stroke. Chin. J. Rehabil. Med. 2014, 29, 76–78. [Google Scholar] [CrossRef]
- Wang, J.; Huang, B.; Yang, Z. Effect of treadmill training in water on walking ability of stroke patients. Chin. J. Rehabil. Med. 2015, 30, 692–695. [Google Scholar] [CrossRef]
- Roth, E.J. Heart disease in patients with stroke: Incidence, impact, and implications for rehabilitation part 1: Classification and prevalence. Arch. Phys. Med. Rehabil. 1993, 74, 752–760. [Google Scholar] [CrossRef]
- Opasich, C.; Pinna, G.D.; Bobbio, M.; Sisti, M.; Demichelis, B.; Febo, O.; Forni, G.; Riccardi, R.; Riccardi, P.; Capomolla, S.; et al. Peak exercise oxygen consumption in chronic heart failure: Toward efficient use in the individual patient. J. Am. Coll. Cardiol. 1998, 31, 766–775. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The TiMed “Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| #1 | Search “Stroke”[Mesh] |
|---|---|
| #2 | Search (((((((((((((Strokes [Title/Abstract]) OR (Cerebrovascular Accident [Title/Abstract])) OR (CVA (Cerebrovascular Accident) [Title/Abstract])) OR (Cerebrovascular Apoplexy [Title/Abstract])) OR (Vascular Accident, Brain [Title/Abstract])) OR (Brain Vascular Accident [Title/Abstract])) OR (Cerebrovascular Stroke [Title/Abstract])) OR (Stroke, Cerebrovascular [Title/Abstract])) OR (Cerebral Stroke [Title/Abstract])) OR (Stroke, Cerebral [Title/Abstract])) OR (Stroke, Acute [Title/Abstract])) OR (Acute Stroke [Title/Abstract])) OR (Cerebrovascular Accident, Acute [Title/Abstract])) OR (Acute Cerebrovascular Accident [Title/Abstract]) |
| #3 | Search #1 OR #2 |
| #4 | Search ((aquatic [Title/Abstract]) OR (aquatic therapy [Title/Abstract])) OR (aquatic exercise [Title/Abstract]) |
| #5 | Search #3 AND #4 |
| Study | Country | Characteristics of Patients | Intervention | Outcomes | Quality Assessment | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sample size (AE/LE) | Gender (M/F) | Age (Years) (MEAN ± SD) | Duration | Water Temperature | Depth | Exercise Program (AE/LE) | |||||
| Kelly, 2004 [22] | Canada | 12 (7/5) | AE: 7 (6/1) LE: 5 (5/0) | AE: 61.9 ± 9.4 LE: 63.4 ± 8.4 | 8 weeks 3/wks 60 min | 26–28 °C | chest- level | Aerobic training: ① 10 min land-based stretching ② 5 min warm-up in the water ③ 30 min moderate to high aerobic activities ④ 5 min cool down ⑤ 10 min stretching inthe water | Strength training: ① 5 min warm-up ② 42 min upper-extremity strengthening ③ 5 min cool-down | ①⑤ | 5 |
| Noh, 2007 [8] | Korea | 25 (13/12) | AE: 13 (7/6) LE: 12 (4/8) | AE:61.9 ± 10.1 LE:66 ± 11.4 | 8 weeks 3/weeks 60 min | 34 °C | 115 cm | Halliwick and Ai Chi training: ① 10 min warm-up ② 20 min Halliwick method ③ 20 min rounding and balancing according to the Ai Chi method ④ 10 min cool-down | Strength and balance training: ① 10 min warm-up ② 40 min lower extremity strengthening, upper-extremity strengthening and gait training ③ 10 min cool-down | ① | 4 |
| Xu Wei, 2011 [23] | China | 76 (40/36) | AE: 40 (23/17) LE:36 (20/16) | AE: 51.3 ± 8.2 LE: 49.3 ± 7.4 | 4 weeks 6/weeks 30 min | / | 130–140 cm | Aerobic and balance training: ① Warm-up ② Hemiplegic gymnastics ③ Water-based walking | Aerobic training: Land-based treadmill walking | ②④ | 4 |
| SEUL, 2013 [6] | Korea | 62 (31/31) | AE: 31 (15/16) LE:31 (13/18) | AE: 56.1 ± 7.3 LE: 56.6 ± 10 | 6 weeks 3/weeks 40 min | 33.5 °C | 110 cm | Strength training: ① 5 min warm-up ② 30 min main exercises (one-legged knee flexion, toe stand, one-legged stance, knee flexion of both legs, eeight shift) ③ 5 min cool-down | Strength training: ① 5 min warm-up ② 30 min main exercises (one-legged knee flexion, toe stand, one-legged stance, knee flexion of both legs, weight shift) ③ 5 min cool-down | ① | 3 |
| Tripp, 2014 [16] | Germany | 30 (14/16) | AE: 14 (9/5) LE: 16 (10/6) | AE: 64.8 ± 15 LE: 65 ± 15.1 | 2 weeks 5/weeks 45 min | / | / | Halliwick training: ① 5 min warm-up ② 5 min were for exercises in water familiarization and mental adaption ③ 15 min for exercising rotational control ④ 15 min locomotion under various disturbances and in changing water depths ⑤ 5 min cool-down | No standard intervention programs: An individual mix of different treatment concepts, task-specific exercising of various tasks in the area of mobility and possibly treadmill training | ①④ | 5 |
| Kim, 2015 [15] | Korea | 20 (10/10) | AE: 10 (5/5) LE: 10 (5/5) | AE: 69.1 ± 3.2 LE: 68 ± 3.1 | 6 weeks 5/weeks 30 min | 31–33 °C | 110 cm | Proprioceptive training: Proprioceptive neuromuscular facilitation lower extremity patterns in water | Proprioceptive training: Proprioceptive neuromuscular facilitation lower extremity patterns on the ground | ①③⑥ | 3 |
| Wu Qiong, 2015 [24] | China | 29 (16/13) | AE: 16 (10/6) LE: 13 (9/4) | AE: 50.94 ± 11.06 LE: 51.38 ± 10.62 | 4 weeks 6/weeks 20 min | 37 °C | xiphoid level | Aerobic training: Underwater treadmill training | Aerobic training: Land-based treadmill training | ④ | 3 |
| Li Gao, 2015 [25] | China | 26 (13/13) | AE: 13 (8/5) LE: 13 (8/5) | AE: 54.6 ± 5.58 LE: 55.4 ± 5.62 | 9 weeks 5/weeks 45 min | 37 °C | 120- 150 cm | Strength and aerobic training: Underwater walking and strengthening exercises | Strength and aerobic training: Land-based walking and strengthening exercises | ①②⑥ | 4 |
| Zhu, Z 2016 [7] | China | 28 (14/14) | AE: 14 (12/2) LE: 14 (10/4) | AE: 56.6 ± 6.9 LE: 57.1 ± 8.6 | 4 weeks 5/weeks 45 min | 34–36 °C | 140 cm | Strength and aerobic training: ① 5 min warm-up ② 30 min strengthening exercises and treadmill exercises ③ 10 min cool-down | Strength and aerobic training: ① 5 min warm-up ② 30 min strengthening exercises and treadmill exercises ③ 10 min cool-down | ①③ | 6 |
| Lee, S. Y, 2018 [16] | Korea | 37 (19/18) | AE: 19 (9/10) LE: 18 (10/8) | AE: 57.58 ± 13.98 LE: 63.67 ± 11.37 | 4 weeks 5/weeks 30 min | 30–33 °C | popliteal level | Aerobic training: ① 5 min warm-up ② 20 min water-based running ③ 5 min cool-down | Aerobic training: 30 min land-based aerobic exercise | ①②⑤ | 5 |
| Pérez, 2021 [26] | Spain | 32 (15/17) | AE: 15 (7/8) LE: 17 (8/9) | AE: 63.8 ± 13.6 LE: 62.7 ± 13.4 | 12 weeks 2/weeks 45 min | 30 °C | 110 cm | Aerobic training: ① 10 min warm-up ② 30 min Ai Chi program ③ 5 min cool-down | Strength and aerobic training: ① 10 min warm-up ② 30–40 min strength training and aerobic exercises ③ 5 min cool-down | ①③ | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, D.; Chen, P. Effects of Aquatic Exercise and Land-Based Exercise on Cardiorespiratory Fitness, Motor Function, Balance, and Functional Independence in Stroke Patients—A Meta-Analysis of Randomized Controlled Trials. Brain Sci. 2021, 11, 1097. https://doi.org/10.3390/brainsci11081097
Li D, Chen P. Effects of Aquatic Exercise and Land-Based Exercise on Cardiorespiratory Fitness, Motor Function, Balance, and Functional Independence in Stroke Patients—A Meta-Analysis of Randomized Controlled Trials. Brain Sciences. 2021; 11(8):1097. https://doi.org/10.3390/brainsci11081097
Chicago/Turabian StyleLi, Daxin, and Ping Chen. 2021. "Effects of Aquatic Exercise and Land-Based Exercise on Cardiorespiratory Fitness, Motor Function, Balance, and Functional Independence in Stroke Patients—A Meta-Analysis of Randomized Controlled Trials" Brain Sciences 11, no. 8: 1097. https://doi.org/10.3390/brainsci11081097
APA StyleLi, D., & Chen, P. (2021). Effects of Aquatic Exercise and Land-Based Exercise on Cardiorespiratory Fitness, Motor Function, Balance, and Functional Independence in Stroke Patients—A Meta-Analysis of Randomized Controlled Trials. Brain Sciences, 11(8), 1097. https://doi.org/10.3390/brainsci11081097