
Association between Visceral Fat and Brain Structural Changes or Cognitive Function

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
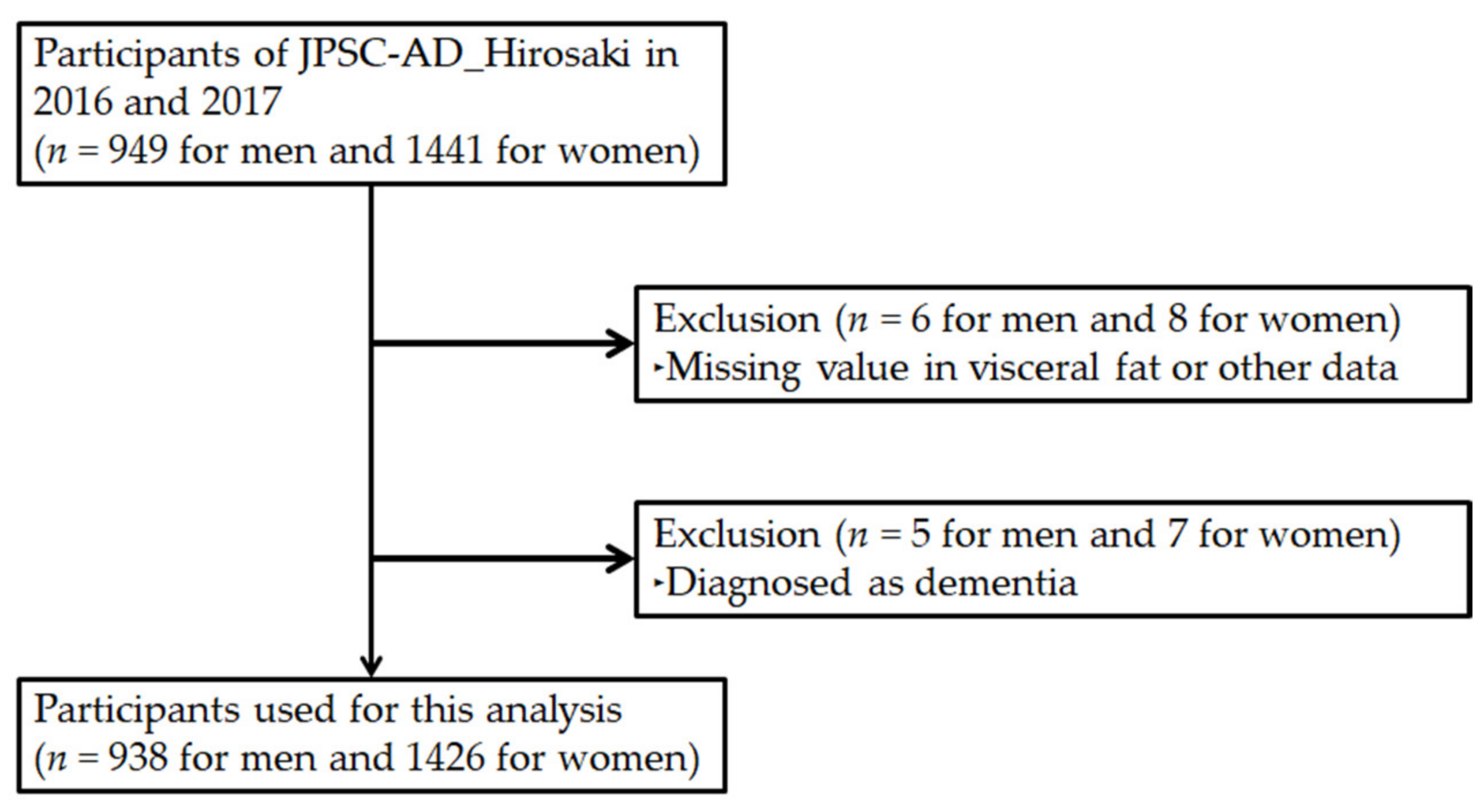
2.1. Design, Participants, and Ethics
2.2. Measurements of Cognitive Function and Brain MRI Examination
2.3. Diagnosis of Depression, Hypertension, Hyperlipidemia, and Diabetes
2.4. Measurements of Other Items
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Cohort
3.2. Association between Cognitive Function and Visceral Fat
3.3. Association between Brain Disorder and Visceral Fat
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J.; et al. Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef]
- Ritchie, K.; Artero, S.; Touchon, J. Classification criteria for mild cognitive impairment: A population-based validation study. Neurology 2001, 56, 37–42. [Google Scholar] [CrossRef]
- Bruscoli, M.; Lovestone, S. Is MCI really just early dementia? A systematic review of conversion studies. Int. Psychogeriatr. 2004, 16, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Luchsinger, J.A.; Gustafson, D.R. Adiposity and Alzheimer’s disease. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 15–21. [Google Scholar] [CrossRef]
- Cournot, M.; Marquié, J.C.; Ansiau, D.; Martinaud, C.; Fonds, H.; Ferrières, J.; Ruidavets, J.B. Relation between body mass index and cognitive function in healthy middle-aged men and women. Neurology 2006, 67, 1208–1214. [Google Scholar] [CrossRef]
- O’Brien, P.D.; Hinder, L.M.; Callaghan, B.C.; Feldman, E.L. Neurological consequences of obesity. Lancet Neurol. 2017, 16, 465–477. [Google Scholar] [CrossRef]
- Dahl, A.K.; Löppönen, M.; Isoaho, R.; Berg, S.; Kivelä, S.L. Overweight and obesity in old age are not associated with greater dementia risk. J. Am. Geriatr. Soc. 2008, 56, 2261–2266. [Google Scholar] [CrossRef]
- Fitzpatrick, A.L.; Kuller, L.H.; Lopez, O.L.; Diehr, P.; O’Meara, E.S.; Longstreth, W.T.; Luchsinger, J.A. Midlife and late-life obesity and the risk of dementia: Cardiovascular health study. Arch. Neurol. 2009, 66, 336–342. [Google Scholar] [CrossRef]
- Hughes, T.F.; Borenstein, A.R.; Schofield, E.; Wu, Y.; Larson, E.B. Association between late-life body mass index and dementia: The Kame Project. Neurology 2009, 72, 1741–1746. [Google Scholar] [CrossRef]
- Emmerzaal, T.L.; Kiliaan, A.J.; Gustafson, D.R. 2003–2013: A decade of body mass index, Alzheimer’s disease, and dementia. J. Alzheimer’s Dis. 2015, 43, 739–755. [Google Scholar] [CrossRef]
- Pedditzi, E.; Peters, R.; Beckett, N. The risk of overweight/obesity in mid-life and late life for the development of dementia: A systematic review and meta-analysis of longitudinal studies. Age Ageing 2016, 45, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Yokomichi, H.; Kondo, K.; Nagamine, Y.; Yamagata, Z.; Kondo, N. Dementia risk by combinations of metabolic diseases and body mass index: Japan Gerontological Evaluation Study Cohort Study. J. Diabetes Investig. 2020, 11, 206–215. [Google Scholar] [CrossRef]
- Gustafson, D. BMI and dementia: Feast or famine for the brain. Lancet Diabetes Endocrinol. 2015, 3, 397–398. [Google Scholar] [CrossRef]
- Fox, C.S.; Massaro, J.M.; Hoffmann, U.; Pou, K.M.; Maurovich-Horvat, P.; Liu, C.Y.; Vasan, R.S.; Murabito, J.M.; Meigs, J.B.; Cupples, L.A.; et al. Abdominal visceral and subcutaneous adipose tissue compartments: Association with metabolic risk factors in the Framingham Heart Study. Circulation 2007, 116, 39–48. [Google Scholar] [CrossRef]
- Tchernof, A.; Després, J.P. Pathophysiology of human visceral obesity: An update. Physiol. Rev. 2013, 93, 359–404. [Google Scholar] [CrossRef]
- Kuk, J.L.; Katzmarzyk, P.T.; Nichaman, M.Z.; Church, T.S.; Blair, S.N.; Ross, R. Visceral fat is an independent predictor of all-cause mortality in men. Obesity 2006, 14, 336–341. [Google Scholar] [CrossRef]
- McNeely, M.J.; Shofer, J.B.; Leonetti, D.L.; Fujimoto, W.Y.; Boyko, E.J. Associations among visceral fat, all-cause mortality, and obesity-related mortality in Japanese Americans. Diabetes Care 2012, 35, 296–298. [Google Scholar] [CrossRef][Green Version]
- Koster, A.; Murphy, R.A.; Eiriksdottir, G.; Aspelund, T.; Sigurdsson, S.; Lang, T.F.; Gudnason, V.; Launer, L.J.; Harris, T.B. Fat distribution and mortality: The AGES-Reykjavik Study. Obesity 2015, 23, 893–897. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, T.; Rask-Andersen, M.; Pan, G.; Höglund, J.; Wadelius, C.; Ek, W.E.; Johansson, Å. Contribution of genetics to visceral adiposity and its relation to cardiovascular and metabolic disease. Nat. Med. 2019, 25, 1390–1395. [Google Scholar] [CrossRef]
- Yoon, D.H.; Choi, S.H.; Yu, J.H.; Ha, J.H.; Ryu, S.H.; Park, D.H. The relationship between visceral adiposity and cognitive performance in older adults. Age Ageing 2012, 41, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Papachristou, E.; Ramsay, S.E.; Lennon, L.T.; Papacosta, O.; Iliffe, S.; Whincup, P.H.; Wannamethee, S.G. The relationships between body composition characteristics and cognitive functioning in a population-based sample of older British men. BMC Geriatr. 2015, 15, 172. [Google Scholar] [CrossRef] [PubMed]
- Spauwen, P.J.; Murphy, R.A.; Jónsson, P.V.; Sigurdsson, S.; Garcia, M.E.; Eiriksdottir, G.; van Boxtel, M.P.; Lopez, O.L.; Gudnason, V.; Harris, T.B.; et al. Associations of fat and muscle tissue with cognitive status in older adults: The AGES-Reykjavik Study. Age Ageing 2017, 46, 250–257. [Google Scholar] [CrossRef]
- Parker, K.G.; Lirette, S.T.; Deardorff, D.S.; Bielak, L.F.; Peyser, P.A.; Carr, J.J.; Terry, J.G.; Fornage, M.; Benjamin, E.J.; Turner, S.T.; et al. Relationships of clinical and computed tomography-imaged adiposity with cognition in middle-aged and older African Americans. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Chiba, I.; Lee, S.; Bae, S.; Makino, K.; Shinkai, Y.; Shimada, H. Visceral fat accumulation is associated with mild cognitive impairment in community-dwelling older Japanese women. J. Nutr. Health Aging 2020, 24, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Van Elderen, S.G.; de Roos, A.; de Craen, A.J.; Westendorp, R.G.; Blauw, G.J.; Jukema, J.W.; Bollen, E.L.; Middelkoop, H.A.; van Buchem, M.A.; van der Grond, J. Progression of brain atrophy and cognitive decline in diabetes mellitus: A 3-year follow-up. Neurology 2010, 75, 997–1002. [Google Scholar] [CrossRef] [PubMed]
- Maillard, P.; Carmichael, O.; Fletcher, E.; Reed, B.; Mungas, D.; DeCarli, C. Coevolution of white matter hyperintensities and cognition in the elderly. Neurology 2012, 79, 442–448. [Google Scholar] [CrossRef]
- Barber, R.; Scheltens, P.; Gholkar, A.; Ballard, C.; McKeith, I.; Ince, P.; Perry, R.; O’Brien, J. White matter lesions on magnetic resonance imaging in dementia with Lewy bodies, Alzheimer’s disease, vascular dementia, and normal aging. J. Neurol. Neurosurg. Psychiatry 1999, 67, 66–72. [Google Scholar] [CrossRef]
- Ninomiya, T.; Nakaji, S.; Maeda, T.; Yamada, M.; Mimura, M.; Nakashima, K.; Mori, T.; Takebayashi, M.; Ohara, T.; Hata, J.; et al. Study design and baseline characteristics of a population-based prospective cohort study of dementia in Japan: The Japan Prospective Studies Collaboration for Aging and Dementia (JPSC-AD). Environ. Health Prev. Med. 2020, 25, 64. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Tsoi, K.K.; Chan, J.Y.; Hirai, H.W.; Wong, S.Y.; Kwok, T.C. Cognitive tests to detect dementia: A systematic review and meta-analysis. JAMA Intern. Med. 2015, 175, 1450–1458. [Google Scholar] [CrossRef]
- Jack, C.R.; Bernstein, M.A.; Fox, N.C.; Thompson, P.; Alexander, G.; Harvey, D.; Borowski, B.; Britson, P.J.; Whitwell, J.L.; Ward, C.; et al. The Alzheimer’s Disease Neuroimaging Initiative (ADNI): MRI methods. J. Magn. Reson. Imaging 2008, 27, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Shinohara, Y.; Tohgi, H.; Hirai, S.; Terashi, A.; Fukuuchi, Y.; Yamaguchi, T.; Okudera, T. Effect of the Ca antagonist nilvadipine on stroke occurrence or recurrence and extension of asymptomatic cerebral infarction in hypertensive patients with or without history of stroke (PICA Study). Cerebrovasc. Dis. 2007, 24, 202–209. [Google Scholar] [CrossRef]
- Fazekas, F.; Kleinert, R.; Offenbacher, H.; Payer, F.; Schmidt, R.; Kleinert, G.; Radner, H.; Lechner, H. The morphologic correlate of incidental punctate white matter hyperintensities on MR images. AJNR Am. J. Neuroradiol. 1991, 12, 915–921. [Google Scholar] [PubMed]
- Shimamoto, K.; Ando, K.; Fujita, T.; Hasebe, N.; Higaki, J.; Horiuchi, M.; Imai, Y.; Imaizumi, T.; Ishimitsu, T.; Ito, M.; et al. The Japanese Society of Hypertension guidelines for the management of hypertension (JSH 2014). Hypertens. Res. 2014, 37, 253–390. [Google Scholar] [CrossRef] [PubMed]
- Teramoto, T.; Sasaki, J.; Ishibashi, S.; Birou, S.; Daida, H.; Dohi, S.; Egusa, G.; Hiro, T.; Hirobe, K.; Iida, M.; et al. Diagnostic criteria for dyslipidemia. J. Atheroscler. Thromb. 2013, 20, 655–660. [Google Scholar] [CrossRef]
- Araki, E.; Goto, A.; Kondo, T.; Noda, M.; Noto, H.; Origasa, H.; Osawa, H.; Taguchi, A.; Tanizawa, Y.; Tobe, K.; et al. Japanese Clinical Practice Guideline for diabetes 2019. J. Diabetes. Investig. 2020, 11, 1020–1076. [Google Scholar] [CrossRef]
- Ryo, M.; Maeda, K.; Onda, T.; Katashima, M.; Okumiya, A.; Nishida, M.; Yamaguchi, T.; Funahashi, T.; Matsuzawa, Y.; Nakamura, T.; et al. A new simple method for the measurement of visceral fat accumulation by bioelectrical impedance. Diabetes Care 2005, 28, 451–453. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare (Japan). Japan National Health and Nutrition Survey 2010. Available online: http://ghdx.healthdata.org/record/japan-national-healthand-nutrition-survey-2010 (accessed on 21 October 2019).
- Examination Committee of Criteria for ‘Obesity Disease’ in Japan; Japan Society for the Study of Obesity. New criteria for ‘obesity disease’ in Japan. Circ. J. 2002, 66, 987–992. [Google Scholar] [CrossRef] [PubMed]
- Anan, F.; Masaki, T.; Eto, T.; Iwao, T.; Shimomura, T.; Umeno, Y.; Eshima, N.; Saikawa, T.; Yoshimatsu, H. Visceral fat accumulation is a significant risk factor for white matter lesions in Japanese type 2 diabetic patients. Eur. J. Clin. Invest. 2009, 39, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Yunli, Q.; Mengqi, L.; Yunjun, Y.; Yanxuan, L. Relationship of visceral adipose tissue with dilated perivascular spaces. Front. Neurosci. 2021, 4, 1454. [Google Scholar] [CrossRef]
- Nam, K.W.; Kwon, H.; Kwon, H.M.; Park, J.H.; Jeong, H.Y.; Kim, S.H.; Jeong, S.M.; Kim, H.J.; Hwang, S.S. Abdominal fatness and cerebral white matter hyperintensity. J. Neurol. Sci. 2019, 404, 52–57. [Google Scholar] [CrossRef]
- Enzinger, C.; Fazekas, F.; Matthews, P.M.; Ropele, S.; Schmidt, H.; Smith, S.; Schmidt, R. Risk factors for progression of brain atrophy in aging: Six-year follow-up of normal subjects. Neurology 2005, 64, 1704–1711. [Google Scholar] [CrossRef]
- Lee, H.; Seo, H.S.; Kim, R.E.Y.; Lee, S.K.; Lee, Y.H.; Shin, C. Obesity and muscle may have synergic effect more than independent effects on brain volume in community-based elderly. Eur. Radiol. 2021, 31, 2956–2966. [Google Scholar] [CrossRef]
- Hirabayashi, N.; Hata, J.; Ohara, T.; Mukai, N.; Nagata, M.; Shibata, M.; Gotoh, S.; Furuta, Y.; Yamashita, F.; Yoshihara, K.; et al. Association between diabetes and hippocampal atrophy in elderly Japanese: The Hisayama Study. Diabetes Care 2016, 39, 1543–1549. [Google Scholar] [CrossRef]
- Nyberg, C.K.; Fjell, A.M.; Walhovd, K.B. Level of body fat relates to memory decline and interacts with age in its association with hippocampal and subcortical atrophy. Neurobiol. Aging 2020, 91, 112–124. [Google Scholar] [CrossRef]
- Yamashiro, K.; Tanaka, R.; Tanaka, Y.; Miyamoto, N.; Shimada, Y.; Ueno, Y.; Urabe, T.; Hattori, N. Visceral fat accumulation is associated with cerebral small vessel disease. Eur. J. Neurol. 2014, 21, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Kober, H.; Boswell, R.G. Potential psychological & neural mechanisms in binge eating disorder: Implications for treatment. Clin. Psychol. Rev. 2018, 60, 32–44. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Criteria |
|---|---|
| Atrophy | “Boundary” or “yes” |
| White matter lesions [32,33] | Beginning confluence of foci (≥3 mm) |
| PVH grade [32,33] | Smooth “halo” |
| Perivascular | Judge by basal ganglia level 1 slice (≥6) |
| Hemorrhage | “Yes” |
| Characteristics | All | Low-VFA | High-VFA | p Value a |
|---|---|---|---|---|
| Number (men/women) | 2364 (938/1426) | 1221 (260/961) | 1143 (465/678) | |
| Age (y) | 70.0 ± 4.2 | 70.0 ± 4.2 | 70.1 ± 4.2 | 0.573 |
| Height (cm) | 157.8 ± 8.4 | 155.2 ± 7.2 | 160.7 ± 8.6 | <0.001 *** |
| Metabolic risk factors | ||||
| BMI (kg/m2) | 22.8 ± 3.0 | 21.0 ± 2.1 | 24.7 ± 2.7 | <0.001 *** |
| Waist circumference (cm) | 77.8 ± 9.4 | 71.2 ± 6.0 | 84.8 ± 7.1 | <0.001 *** |
| VFA (cm2) | 86.0 ± 41.2 | 54.7 ± 18.0 | 119.5 ± 31.5 | <0.001 *** |
| Glucose (mmol/L) | 5.2 ± 1.0 | 5.0 ± 0.8 | 5.4 ± 1.1 | <0.001 *** |
| HbA1c (%) | 5.8 ± 0.6 | 5.7 ± 0.5 | 5.9 ± 0.7 | <0.001 *** |
| DBP (mmHg) | 83.2 ± 12.1 | 82.2 ± 12.1 | 84.2 ± 12.0 | <0.001 *** |
| SBP (mmHg) | 150.5 ± 21.9 | 148.4 ± 22.8 | 152.7 ± 20.5 | <0.001 *** |
| TG (mmol/L) | 1.1 ± 0.6 | 1.0 ± 0.5 | 1.3 ± 0.7 | <0.001 *** |
| HDL cholesterol (mmol/L) | 1.8 ± 0.4 | 1.9 ± 0.4 | 1.6 ± 0.4 | <0.001 *** |
| LDL cholesterol (mmol/L) | 3.3 ± 0.8 | 3.4 ± 0.8 | 3.2 ± 0.8 | <0.001 *** |
| Lifestyle habit | ||||
| Energy intake (kcal) | 1765 ± 413 | 1726 ± 367 | 1805 ± 453 | <0.001 *** |
| Smoking habit (yes, %) | 7.0 | 5.6 | 8.5 | 0.011 * |
| Sleep time (h/d) | 7.0 ± 1.2 | 7.1 ± 1.2 | 7.0 ± 1.2 | 0.439 |
| Daily exercise (yes, %) | 68.8 | 70.3 | 67.2 | 0.117 |
| Alcohol intake (yes, %) | 46.7 | 37.5 | 56.5 | <0.001 *** |
| Disease | ||||
| Depression (%) | 1.6 | 1.7 | 1.6 | 0.914 |
| Hypertension (%) | 79.6 | 72.2 | 87.1 | <0.001 *** |
| Hyperlipidemia (%) | 49.6 | 43.0 | 56.6 | <0.001 *** |
| Diabetes (%) | 17.0 | 11.7 | 22.7 | <0.001 *** |
| Characteristics | Low-VFA (n = 1224) | High-VFA (n = 1143) | p Value a |
|---|---|---|---|
| Atrophy | 19.2% | 29.2% | <0.001 *** |
| Non-atrophy | 80.8% | 70.8% | |
| White matter lesions | 6.3% | 10.7% | <0.001 *** |
| Non-white matter lesions | 93.7% | 89.3% | |
| PVH grade | 13.1% | 17.1% | 0.008 ** |
| Non-PVH grade | 86.9% | 82.9% | |
| Perivascular | 22.1% | 27.0% | 0.008 ** |
| Non-perivascular | 77.9% | 73.0% | |
| Hemorrhage | 11.5% | 15.0% | 0.016 * |
| Non-hemorrhage | 88.5% | 85.0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ozato, N.; Saitou, S.; Yamaguchi, T.; Katashima, M.; Misawa, M.; Jung, S.; Mori, K.; Kawada, H.; Katsuragi, Y.; Mikami, T.; et al. Association between Visceral Fat and Brain Structural Changes or Cognitive Function. Brain Sci. 2021, 11, 1036. https://doi.org/10.3390/brainsci11081036
Ozato N, Saitou S, Yamaguchi T, Katashima M, Misawa M, Jung S, Mori K, Kawada H, Katsuragi Y, Mikami T, et al. Association between Visceral Fat and Brain Structural Changes or Cognitive Function. Brain Sciences. 2021; 11(8):1036. https://doi.org/10.3390/brainsci11081036
Chicago/Turabian StyleOzato, Naoki, Shinnichiro Saitou, Tohru Yamaguchi, Mitsuhiro Katashima, Mina Misawa, Songee Jung, Kenta Mori, Hiromitsu Kawada, Yoshihisa Katsuragi, Tatsuya Mikami, and et al. 2021. "Association between Visceral Fat and Brain Structural Changes or Cognitive Function" Brain Sciences 11, no. 8: 1036. https://doi.org/10.3390/brainsci11081036
APA StyleOzato, N., Saitou, S., Yamaguchi, T., Katashima, M., Misawa, M., Jung, S., Mori, K., Kawada, H., Katsuragi, Y., Mikami, T., & Nakaji, S. (2021). Association between Visceral Fat and Brain Structural Changes or Cognitive Function. Brain Sciences, 11(8), 1036. https://doi.org/10.3390/brainsci11081036