
Effects of Smartphone-Based Compensatory Cognitive Training and Physical Activity on Cognition, Depression, and Self-Esteem in Women with Subjective Cognitive Decline


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
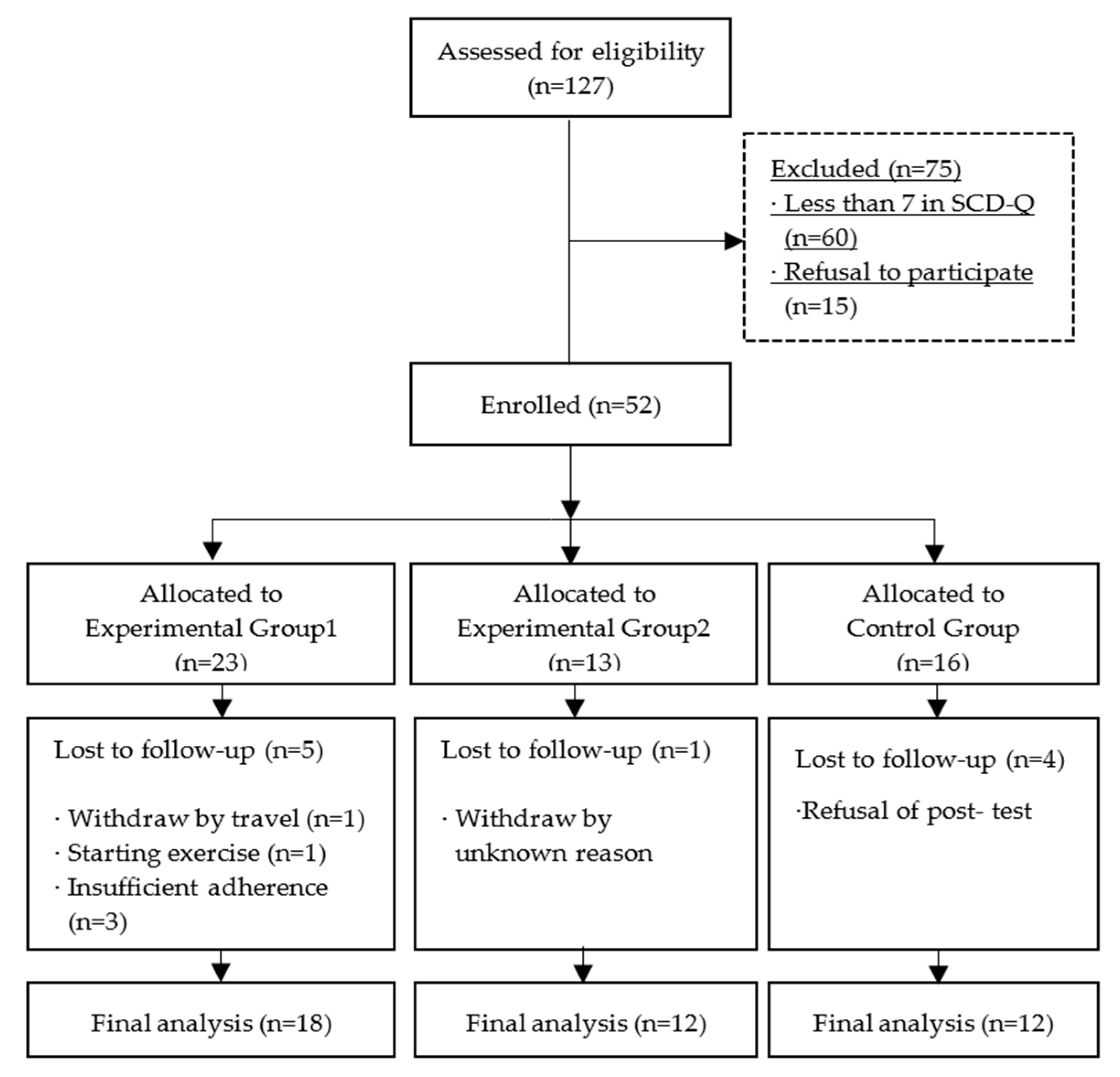
2.2. Participants
2.3. Interventions
2.3.1. Calendar Training
2.3.2. Walking Exercise
2.4. Data Collection and Outcome measures
2.4.1. Cognitive Function
2.4.2. Depressive Symptoms
2.4.3. Self-Esteem
2.4.4. Adherence
- 2 points if an appointment, to-do item, or journaling was completed more than 2 days per week;
- 2 points if there was a record of the appointment;
- 2 points if there was at least one recorded to-do item;
- 4 points if there was a record in the journaling area.
2.5. Data Analysis
3. Results
3.1. Participant Characteristics
3.2. Cognitive Function, Depressive Symptoms, and Self-Esteem among Groups at Baseline
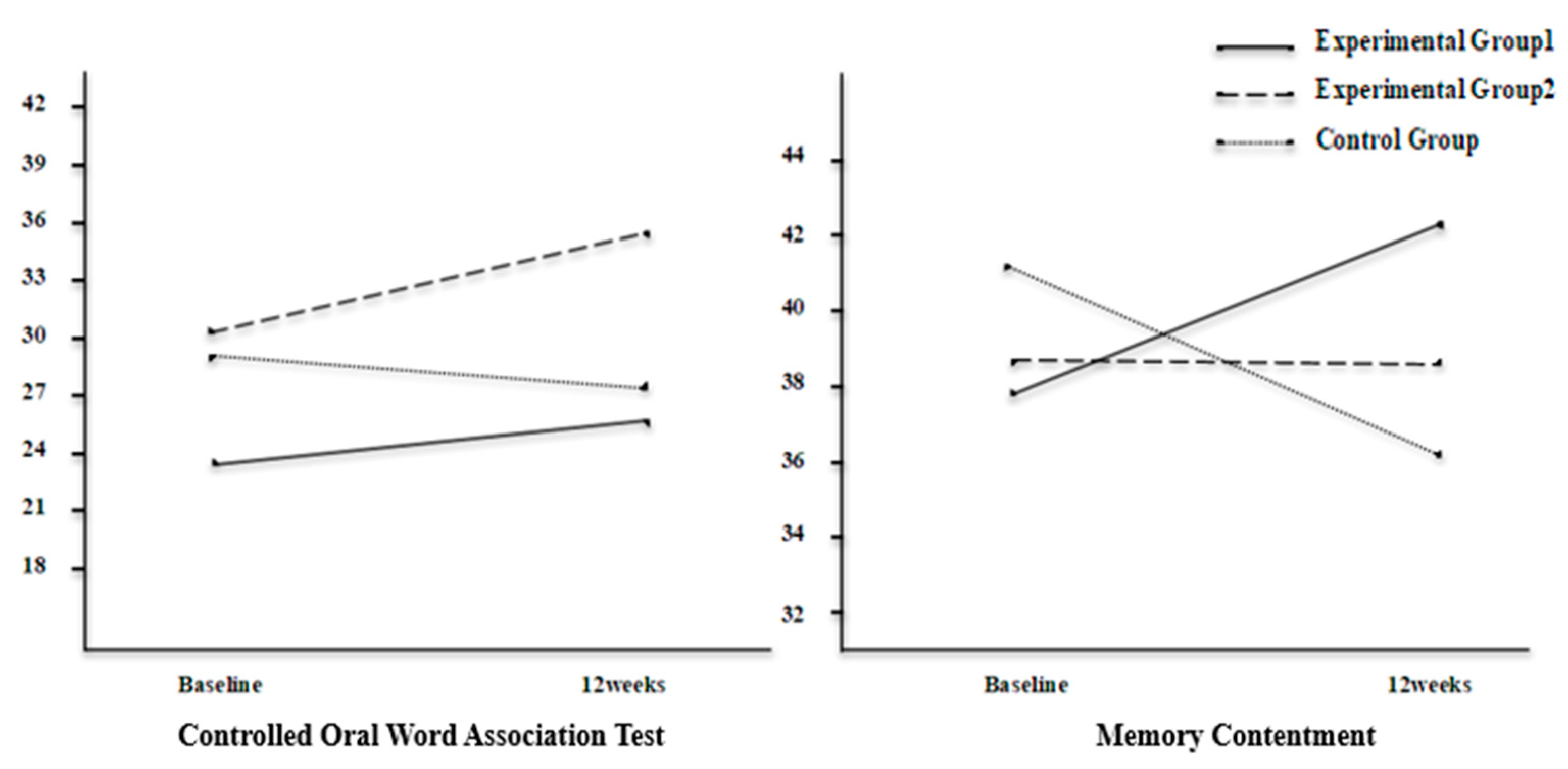
3.3. Effects of Intervention on Cognitive Function, Depressive Symptoms, and Self-Esteem
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jessen, F.; Amariglio, R.E.; Buckley, R.F.; van der Flier, W.M.; Han, Y.; Molinuevo, J.L.; Rabin, L.; Rentz, D.M.; Rodriguez-Gomez, O.; Saykin, A.J.; et al. The characterisation of subjective cognitive decline. Lancet. Neurol. 2020, 19, 271–278. [Google Scholar] [CrossRef]
- Rabin, L.A.; Smart, C.M.; Amariglio, R.E. Subjective cognitive decline in preclinical alzheimer’s disease. Annu. Rev. Clin. Psychol. 2017, 13, 369–396. [Google Scholar] [CrossRef]
- Hsieh, T.J.; Chang, H.Y.; Wu, I.C.; Chen, C.C.; Tsai, H.J.; Chiu, Y.F.; Chuang, S.C.; Hsiung, C.A.; Hsu, C.C. Independent association between subjective cognitive decline and frailty in the elderly. PLoS ONE 2018, 13, e0201351. [Google Scholar] [CrossRef] [Green Version]
- Jessen, F.; Amariglio, R.E.; van Boxtel, M.; Breteler, M.; Ceccaldi, M.; Chetelat, G.; Dubos, B.; Dufouil, C.; Ellis, K.A.; van der Flier, W.M.; et al. A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer’s disease. Alzheimers Dement. 2014, 10, 844–852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez-Blazqueza, M.A.; A’vila-Villanueva, M.; Maestu´, F.; Medina, M. Specific features of subjective cognitive decline predict faster conversion to mild cognitive impairment. J. Alzheimers Dis. 2016, 52, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.A.; Bouldin, E.D.; McGuire, L.C. Subjective cognitive decline among adults aged ≥45 Years-United States, 2015–2016. Morb. Mortal Wkly Rep. 2018, 67, 753–757. [Google Scholar] [CrossRef]
- Hao, L.; Wang, X.; Zhang, L.; Xing, Y.; Guo, Q.; Hu, X.; Mu, B.; Chen, Y.; Chen, G.; Cao, J.; et al. Prevalence, risk factors, and complaints screening tool exploration of subjective cognitive decline in a large cohort of the Chinese population. J. Alzheimers Dis. 2017, 60, 371–388. [Google Scholar] [CrossRef] [PubMed]
- Niu, H.; Álvarez-Álvarez, I.; Guillén-Grima, F.; Aguinaga-Ontoso, I. Prevalence and incidence of Alzheimer’s disease in Europe: A meta-analysis. Neurologia 2017, 32, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Armeni, E.; Apostolakis, M.; Christidi, F.; Rizos, D.; Kaparos, G.; Panoulis, K.; Augoulea, A.; Alexandrou, A.; Karopoulou, E.; Zalonis, I.; et al. Endogenous sex hormones and memory performance in middle-aged Greek women with subjective memory complaints. Neurol. Sci. 2018, 39, 259–266. [Google Scholar] [CrossRef]
- Russell, J.K.; Jones, C.K.; Newhouse, P.A. The role of estrogen in brain and cognitive aging. Neurotherapeutics 2019, 16, 649–665. [Google Scholar] [CrossRef]
- Augoulea, A.; Moros, M.; Lykeridou, A.; Kaparos, G.; Lyberi, R.; Panoulis, K. Psychosomatic and vasomotor symptom changes during transition to menopause. Menopause Rev. 2019, 18, 110–115. [Google Scholar] [CrossRef]
- Donovan, N.J.; Locascio, J.J.; Marshall, G.A.; Gatchel, J.; Hanseeuw, B.J.; Rentz, D.M.; Johnson, K.A.; Sperling, R.A. Harvard Aging Brain Study. Longitudinal association of amyloid beta and anxious-depressive symptoms in cognitively normal older adults. Am. J. Psychiatry 2018, 175, 530–537. [Google Scholar] [CrossRef] [PubMed]
- Gatchel, J.R.; Rabin, J.S.; Buckley, R.F.; Locascio, J.J.; Quiroz, Y.T.; Yang, H.S.; Vannini, P.; Amariglio, R.E.; Rentz, D.M.; Properzi, M.; et al. Longitudinal association of depression symptoms with cognition and cortical amyloid among community-dwelling older adults. JAMA Netw. Open 2019, 2, e198964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slot, R.E.R.; Verfaillie, S.C.J.; Overbeek, J.M.; Timmers, T.; Wesselman, L.M.P.; Teunissen, C.E.; Dols, A.; Bouwman, F.H.; Prins, N.D.; Barkhof, F.; et al. Subjective Cognitive Impairment Cohort (SCIENCe): Study design and first results. Alzheimers Res. Ther. 2018, 10, 76. [Google Scholar] [CrossRef]
- Zlatar, Z.Z.; Muniz, M.; Galasko, D.; Salmon, D.P. Subjective cognitive decline correlates with depression symptoms and not with concurrent objective cognition in a clinic-based sample of older adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2018, 73, 1198–1202. [Google Scholar] [CrossRef]
- Santos, S.B.; Rocha, G.P.; Fernandez, L.L.; De Padua, A.C.; Reppold, C.T. Association of lower spiritual well-being, social support, self-esteem, subjective well-being, optimism and hope scores with mild cognitive impairment and mild dementia. Front. Psychol. 2018, 9, 371. [Google Scholar] [CrossRef] [PubMed]
- Smart, C.M.; Karr, J.E.; Areshenkoff, C.N.; Rabin, L.A.; Hudon, C.; Gates, N.; Ali, J.I.; Arenaza-Urquijo, E.M.; Buckley, R.F.; Chetelat, G.; et al. Non-pharmacologic interventions for older adults with subjective cognitive decline: Systematic review, meta-Analysis, and preliminary recommendations. Neuropsychol. Rev. 2017, 27, 245–257. [Google Scholar] [CrossRef]
- Huckans, M.; Hutson, L.; Twamley, E.; Jak, A.; Storzbach, D. Efficacy of cognitive rehabilitation therapies for mild cognitive impairment (MCI) in older adults: Working toward a theoretical model and evidence-based interventions. Neuropsychol. Rev. 2013, 23, 63–80. [Google Scholar] [CrossRef] [PubMed]
- Chandler, M.J.; Locke, D.; Duncan, N.L.; Hanna, S.M.; Cuc, A.V.; Fields, J.A.; Hoffman Snyder, C.R.; Lunde, A.M.; Smith, G.E. Computer versus compensatory calendar training in individuals with mild cognitive impairment: Functional impact in a pilot study. Brain Sci. 2017, 7, 112. [Google Scholar] [CrossRef] [Green Version]
- Falck, R.S.; Davis, J.C.; Best, J.R.; Crockett, R.A.; Liu-Ambrose, T. Impact of exercise training on physical and cognitive function among older adults: A systematic review and meta-analysis. Neurobiol. Aging 2019, 79, 119–130. [Google Scholar] [CrossRef]
- Thomas, B.P.; Tarumi, T.; Sheng, M.; Tseng, B.; Womack, K.B.; Cullum, C.M.; Rypma, B.; Zhang, R.; Lu, H. Brain perfusion change in patients with mild cognitive impairment after 12 months of aerobic exercise training. J. Alzheimers Dis. 2020, 75, 617–631. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, P.D.; Frith, E. A brief primer on the mediational role of BDNF in the exercise-memory link. Clin. Physiol. Funct. Imaging 2019, 39, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Dinoff, A.; Herrmann, N.; Swardfager, W.; Lanctot, K. The effect of acute exercise on blood concentrations of brain-derived neurotrophic factor in healthy adults: A meta-analysis. Eur. J. Neurosci. 2017, 46, 1635–1646. [Google Scholar] [CrossRef]
- Erickson, K.I.; Voss, M.W.; Prakash, R.S.; Basak, C.; Szabo, A.; Chaddock, L.; Kim, J.S.; Heo, S.; Alves, H.; White, S.M.; et al. Exercise training increases size of hippocampus and improves memory. Proc. Natl. Acad. Sci. USA 2011, 108, 3017–3022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gokal, K.; Munir, F.; Ahmed, S.; Kancherla, K.; Wallis, D. Does walking protect against decline in cognitive functioning among breast cancer patients undergoing chemotherapy? results from a small randomised controlled trial. PLoS ONE 2018, 13. [Google Scholar] [CrossRef]
- Kim, O.; Pang, Y.; Kim, J.H. The effectiveness of virtual reality for people with mild cognitive impairment or dementia: A meta-analysis. BMC Psychiatry 2019, 19, 219. [Google Scholar] [CrossRef] [Green Version]
- Wesselman, L.M.; Hooghiemstra, A.M.; Schoonmade, L.J.; de Wit, M.C.; van der Flier, W.M.; Sikkes, S.A. Web-based multidomain lifestyle programs for brain health: Comprehensive overview and meta-analysis. JMIR Ment. Health 2019, 6, e12104. [Google Scholar] [CrossRef] [Green Version]
- Oh, S.J.; Seo, S.; Lee, J.H.; Song, M.J.; Shin, M.S. Effects of smartphone-based memory training for older adults with subjective memory complaints: A randomized controlled trial. Aging Ment. Health 2018, 22, 526–534. [Google Scholar] [CrossRef] [PubMed]
- Shellington, E.M.; Felfeli, T.; Shigematsu, R.; Gill, D.P.; Petrella, R.J. HealtheBrain: An innovative smartphone application to improve cognitive function in older adults. mHealth 2017, 3, 17. [Google Scholar] [CrossRef] [Green Version]
- Korinek, E.V.; Phatak, S.S.; Martin, C.A.; Freigoun, M.T.; Rivera, D.E.; Adams, M.A.; Klasnja, P.; Buman, M.P.; Hekler, E.B. Adaptive step goals and rewards: A longitudinal growth model of daily steps for a smartphone-based walking intervention. J. Behav. Med. 2018, 41, 74–86. [Google Scholar] [CrossRef] [PubMed]
- Gal, R.; May, A.M.; van Overmeeren, E.J.; Simons, M.; Monninkhof, E.M. The effect of physical activity interventions compris ing wearables and smartphone applications on physical activity: A systematic review and meta-analysis. Sports Med. Open 2018, 4, 42. [Google Scholar] [CrossRef]
- Glynn, L.G.; Hayes, P.S.; Casey, M.; Glynn, F.; Alvarez-Iglesias, A.; Newell, J.; OLaighin, G.; Heaney, D.; O’Donnell, M.; Murphy, A.W. Effectiveness of a smartphone application to promote physical activity in primary care: The SMART MOVE randomised controlled trial. Br. J. Gen. Pract. 2014, 64, e384–e391. [Google Scholar] [CrossRef]
- Korea Information Society Development Institute. KISDI STAT Report. Available online: https://www.kisdi.re.kr/kisdi/common/premium?file=1%7C14503 (accessed on 3 May 2019).
- Folstein, M.F.; Folstein, S.E. Korean Version of the Mini-Mental State Examination, 2nd ed.; PAR Inc.: Lutz, FL, USA, 2010. [Google Scholar]
- Rami, L.; Mollica, M.A.; García-Sanchez, C.; Saldaña, J.; Sanchez, B.; Sala, I.; Valls-Pedret, C.; Castellví, M.; Olives, J.; Molinuevo, J.L. The Subjective Cognitive Decline Questionnaire (SCD-Q): A validation study. J. Alzheimer’s Dis. 2014, 41, 453–466. [Google Scholar] [CrossRef] [PubMed]
- Greenaway, M.C.; Duncan, N.L.; Smith, G.E. The memory support system for mild cognitive impairment: Randomized trial of a cognitive rehabilitation intervention. Int. J. Geriatr. Psychiatry 2013, 28, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Tudor-Locke, C.; Craig, C.L.; Aoyagi, Y.; Bell, R.C.; Croteau, K.A.; De Bourdeaudhuij, I.; Ewald, B.; Gardner, A.W.; Hatano, Y.; Lutes, L.D.; et al. How many steps/day are enough? For older adults and special populations. Int. J. Behav. Nutr. Phys. Act 2011, 8, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, H.; Lee, H. The effects of reinforced walking exercise on dyspnea-fatigue symptoms, daily activities, walking ability, and health related quality of life in heart failure patients. Korean J. Adult Nurs. 2016, 28, 266–278. [Google Scholar] [CrossRef]
- Kang, Y.W.; Jang, S.M.; Na, D.L. Seoul Neuropsychological Screening Battery Core; Human Brain Research & Consulting Seoul: Seoul, Korea, 2018. [Google Scholar]
- Troyer, A.K.; Rich, J.B. Psychometric properties of a new metamemory questionnaire for older adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2002, 57, 19–27. [Google Scholar] [CrossRef] [Green Version]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Jung, I.K.; Kwak, D.I.; Shin, D.K.; Lee, M.S.; Lee, H.S.; Kim, J.Y. A reliability and validity study of geriatric depression scale. J. Korean Neuropsychiatr. Assoc. 1997, 36, 103–111. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 3rd ed.; Harper Collins: New York, NY, USA, 1996. [Google Scholar]
- Kim, Y.K.; Ghim, H.L. The effects of a cognitive enhancement program for elderly. Korean J. Dev. Psychol. 2015, 28, 87–105. [Google Scholar]
- Northey, J.M.; Cherbuin, N.; Pumpa, K.L.; Smee, D.J.; Rattray, B. Exercise interventions for cognitive function in adults older than 50: A systematic review with meta-analysis. Br. J. Sports Med. 2018, 52, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Ngandu, T.; Lehtisalo, J.; Solomon, A.; Levälahti, E.; Ahtiluoto, S.; Antikainen, R.; Bäckman, L.; Hänninen, T.; Jula, A.; Laatikainen, T.; et al. A 2year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): A randomised controlled trial. Lancet 2015, 385, 2255–2263. [Google Scholar] [CrossRef]
- Gokal, K.; Wallis, D.; Ahmed, S.; Boiangiu, I.; Kancherla, K.; Munir, F. Effects of a self-managed home-based walking interven tion on psychosocial health outcomes for breast cancer patients receiving chemotherapy: A randomised controlled trial. Support Care Cancer 2016, 24, 1139–1166. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Experimental Group 1 (n = 18) | Experimental Group 2 (n = 12) | Control Group (n = 12) | χ2/F | p | ||
|---|---|---|---|---|---|---|
| n (%) or M ± SD | ||||||
| Age (years) | 60.89 ± 6.62 | 59.42 ± 5.16 | 59.33 ± 6.54 | 0.305 | 0.739 | |
| Education years | 12.94 ± 3.06 | 13.58 ± 2.94 | 13.33 ± 2.96 | 0.172 | 0.843 | |
| Marital status | single | 3 (16.7) | 0 | 0 | 8.458 | 0.089 |
| married | 10 (55.6) | 12 (100.0) | 10 (83.3) | |||
| divorced/ widowed | 5 (27.7) | 0 | 2 (16.7) | |||
| Cohabiting family | spouse | 3 (16.7) | 4 (33.3) | 3 (25.0) | 9.553 | 0.237 |
| children | 3 (16.7) | 0 | 1 (8.3) | |||
| spouse & children | 7 (38.9) | 8 (66.7) | 6 (50.0) | |||
| living alone | 5 (27.7) | 0 | 2 (16.7) | |||
| Occupation | Yes | 14 (77.8) | 7 (58.3) | 6 (50.0) | 2.716 | 0.284 |
| No | 4 (22.2) | 5 (41.7) | 6 (50.0) | |||
| Hobbies (reading, puzzles, etc.) | Yes | 8 (44.4) | 8 (66.7) | 7 (58.3) | 1.512 | 0.539 |
| No | 10 (55.6) | 4 (33.3) | 5 (41.7) | |||
| Experimental Group1 (n = 18) | Experimental Group2 (n = 12) | Control Group (n = 12) | F | p | ||
|---|---|---|---|---|---|---|
| M ± SD | ||||||
| Attention | DST-F | 6.56 ± 1.20 | 7.67 ± 1.07 | 6.75 ± 1.60 | 2.812 | 0.072 |
| DST-B | 4.11 ± 0.96 | 5.75 ± 4.60 | 4.58 ± 1.83 | 4.925 | 0.019 * | |
| Memory | Immediate Recall | 23.11 ± 3.76 | 24.00 ± 5.26 | 23.25 ± 5.36 | 0.138 | 0.871 |
| Delayed Recall | 8.56 ± 1.85 | 8.17 ± 2.25 | 8.83 ± 2.76 | 0.266 | 0.768 | |
| Executive function | K-CWST-60 | 50.22 ± 8.04 | 56.42 ± 7.22 | 56.00 ± 10.42 | 2.515 | 0.094 |
| COWAT | 23.50 ± 7.20 | 30.75 ± 7.70 | 29.50 ± 9.56 | 3.541 | 0.039 * | |
| Memory contentment | 37.83 ± 7.45 | 38.75 ± 11.33 | 41.25 ± 7.98 | 0.547 | 0.583 | |
| Depressive symptoms | 10.50 ± 4.93 | 13.50 ± 6.68 | 10.33 ± 5.07 | 1.328 | 0.277 | |
| Self-esteem | 33.44 ± 5.48 | 35.42 ± 5.45 | 33.83 ± 3.74 | 0.578 | 0.566 | |
| Experimental Group 1 (n = 18) | Experimental Group 2 (n = 12) | Control Group (n = 12) | F (Time) | F (Group) | F (Time * Group) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | |||||
| Attention | DST-F | 6.56 ± 1.20 | 6.72 ± 1.27 | 7.67 ± 1.07 | 7.58 ± 1.44 | 6.75 ± 1.60 | 7.42 ± 1.38 | 1.298 | 2.773 | 0.906 |
| DST-B | 4.11 ± 0.96 | 4.72 ± 1.60 | 5.75 ± 4.60 | 6.25 ± 1.14 | 4.58 ± 1.83 | 5.17 ± 1.34 | 3.400 | 8.464 ** | 0.012 | |
| Memory | Immediate Recall | 23.11 ± 3.76 | 26.94 ± 3.40 | 24.00 ± 5.26 | 28.75 ± 4.81 | 23.25 ± 5.36 | 26.67 ± 3.92 | 36.858 *** | 0.557 | 0.322 |
| Delayed Recall | 8.56 ± 1.85 | 9.67 ± 1.50 | 8.17 ± 2.25 | 10.33 ± 2.19 | 8.83 ± 2.76 | 10.42 ± 1.83 | 24.632 *** | 0.314 | 0.932 | |
| Executive function | K-CWST-60 | 50.22 ± 8.04 | 56.89 ± 11.12 | 56.42 ± 7.22 | 65.08 ± 13.62 | 56.00 ± 10.42 | 57.75 ± 9.86 | 18.824 *** | 2.174 | 2.214 |
| COWAT | 23.50 ± 7.20 | 26.17 ± 7.23 | 30.75 ± 7.70 | 36.17 ± 5.00 | 29.50 ± 9.56 | 27.67 ± 6.87 | 5.296 * | 5.854 ** | 4.869 * | |
| Memory contentment | 37.83 ± 7.45 | 42.33 ± 8.56 | 38.75 ± 11.33 | 38.67 ± 10.53 | 41.25 ± 7.98 | 36.25 ± 9.89 | .022 | 0.140 | 4.789 * | |
| Depressive symptoms | 10.50 ± 4.93 | 7.89 ± 5.17 | 13.50 ± 6.68 | 12.17 ± 7.27 | 10.33 ± 5.07 | 11.58 ± 5.57 | 1.192 | 1.849 | 1.969 | |
| Self-esteem | 33.44 ± 5.48 | 35.28 ± 5.63 | 35.42 ± 5.45 | 34.58 ± 4.60 | 33.83 ± 3.74 | 34.33 ± 4.89 | 0.545 | 0.126 | 1.393 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pang, Y.; Kim, O. Effects of Smartphone-Based Compensatory Cognitive Training and Physical Activity on Cognition, Depression, and Self-Esteem in Women with Subjective Cognitive Decline. Brain Sci. 2021, 11, 1029. https://doi.org/10.3390/brainsci11081029
Pang Y, Kim O. Effects of Smartphone-Based Compensatory Cognitive Training and Physical Activity on Cognition, Depression, and Self-Esteem in Women with Subjective Cognitive Decline. Brain Sciences. 2021; 11(8):1029. https://doi.org/10.3390/brainsci11081029
Chicago/Turabian StylePang, Yanghee, and Oksoo Kim. 2021. "Effects of Smartphone-Based Compensatory Cognitive Training and Physical Activity on Cognition, Depression, and Self-Esteem in Women with Subjective Cognitive Decline" Brain Sciences 11, no. 8: 1029. https://doi.org/10.3390/brainsci11081029
APA StylePang, Y., & Kim, O. (2021). Effects of Smartphone-Based Compensatory Cognitive Training and Physical Activity on Cognition, Depression, and Self-Esteem in Women with Subjective Cognitive Decline. Brain Sciences, 11(8), 1029. https://doi.org/10.3390/brainsci11081029