
Cerebral Hemodynamics and Intracranial Compliance Impairment in Critically Ill COVID-19 Patients: A Pilot Study



 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
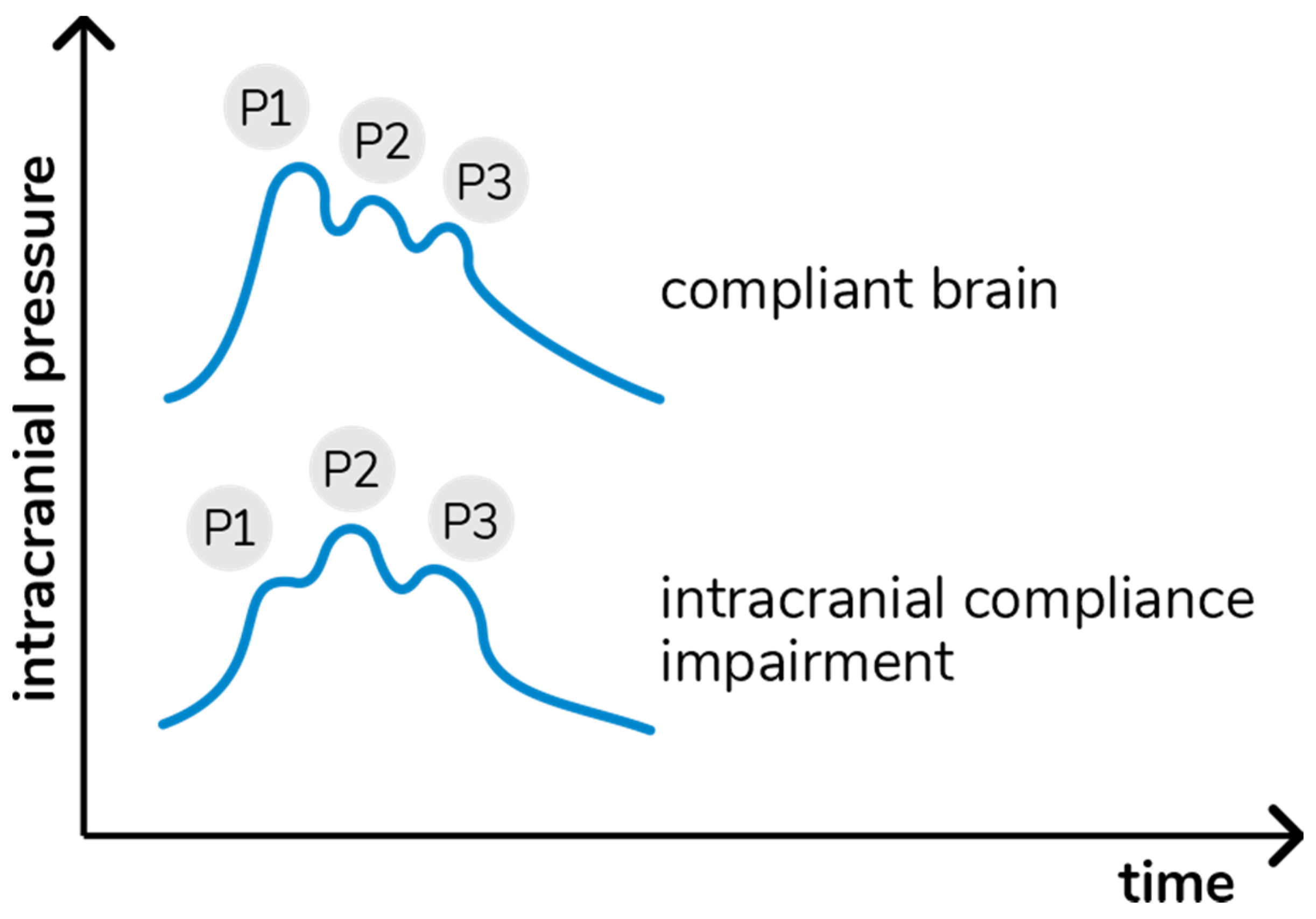
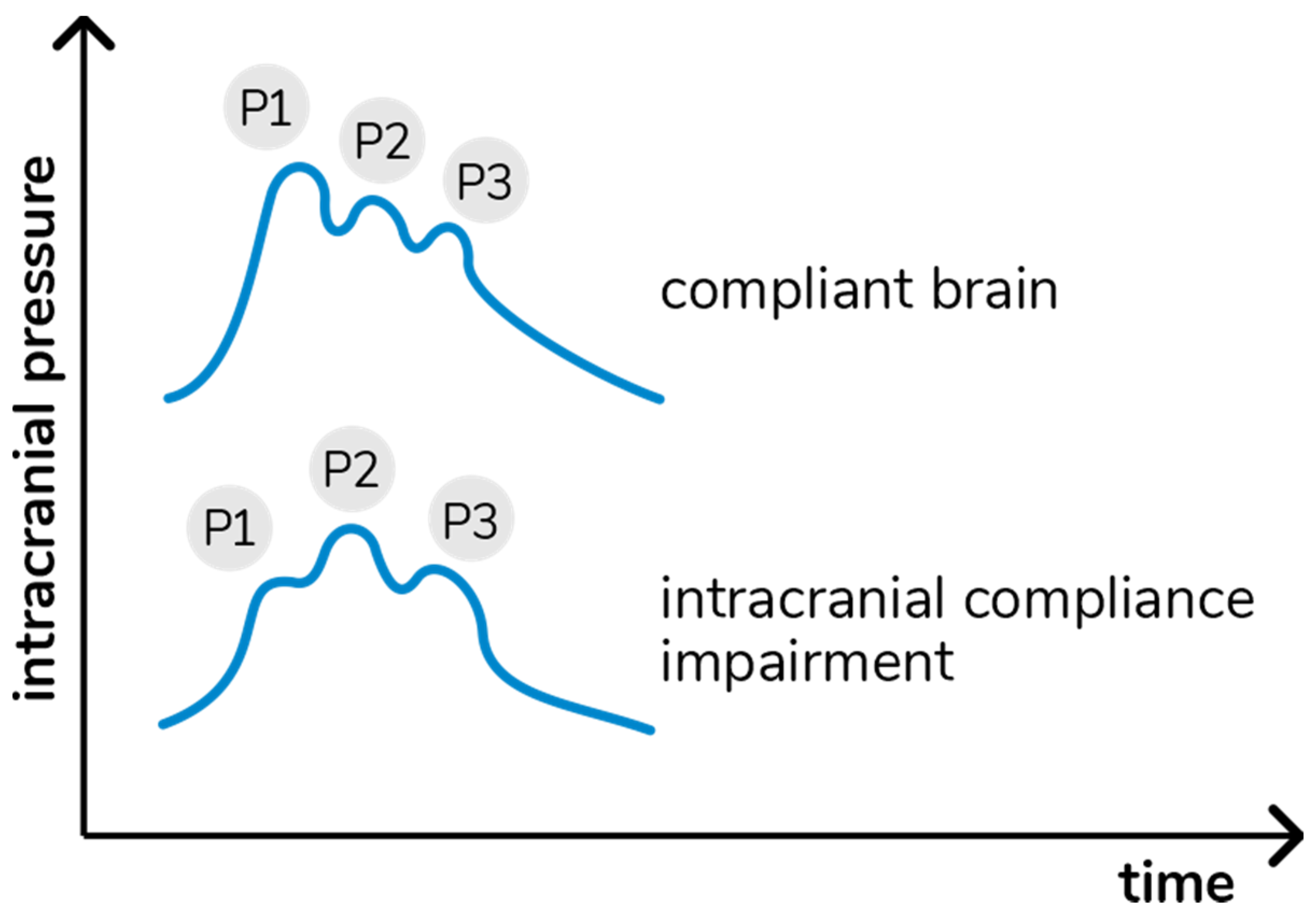
2.2. Intracranial Compliance Monitoring Technique
2.3. Cerebrovascular Hemodynamics Assessment
2.4. Outcomes
2.5. Sample Size
2.6. Statistical Analysis
3. Results
3.1. Study Population
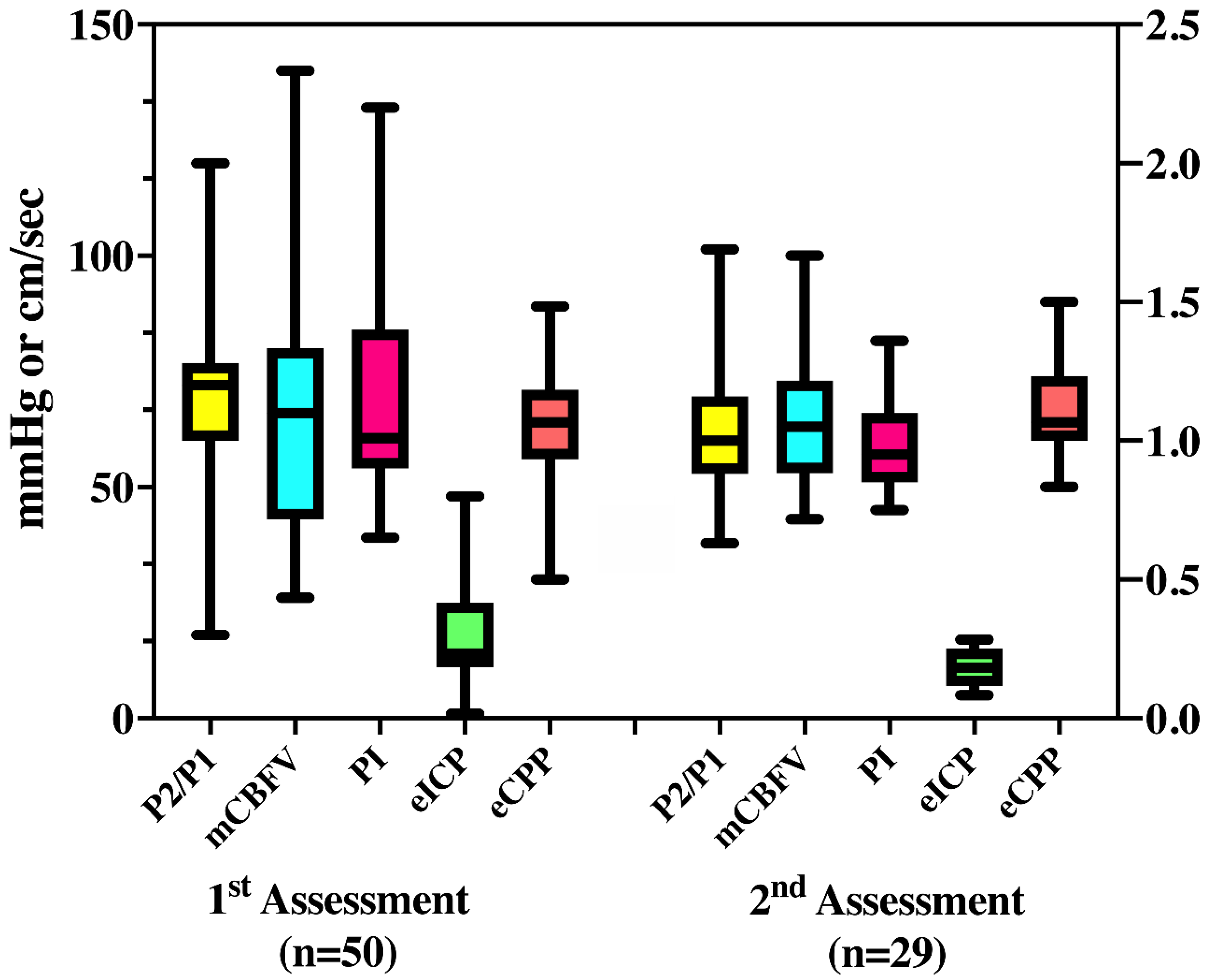
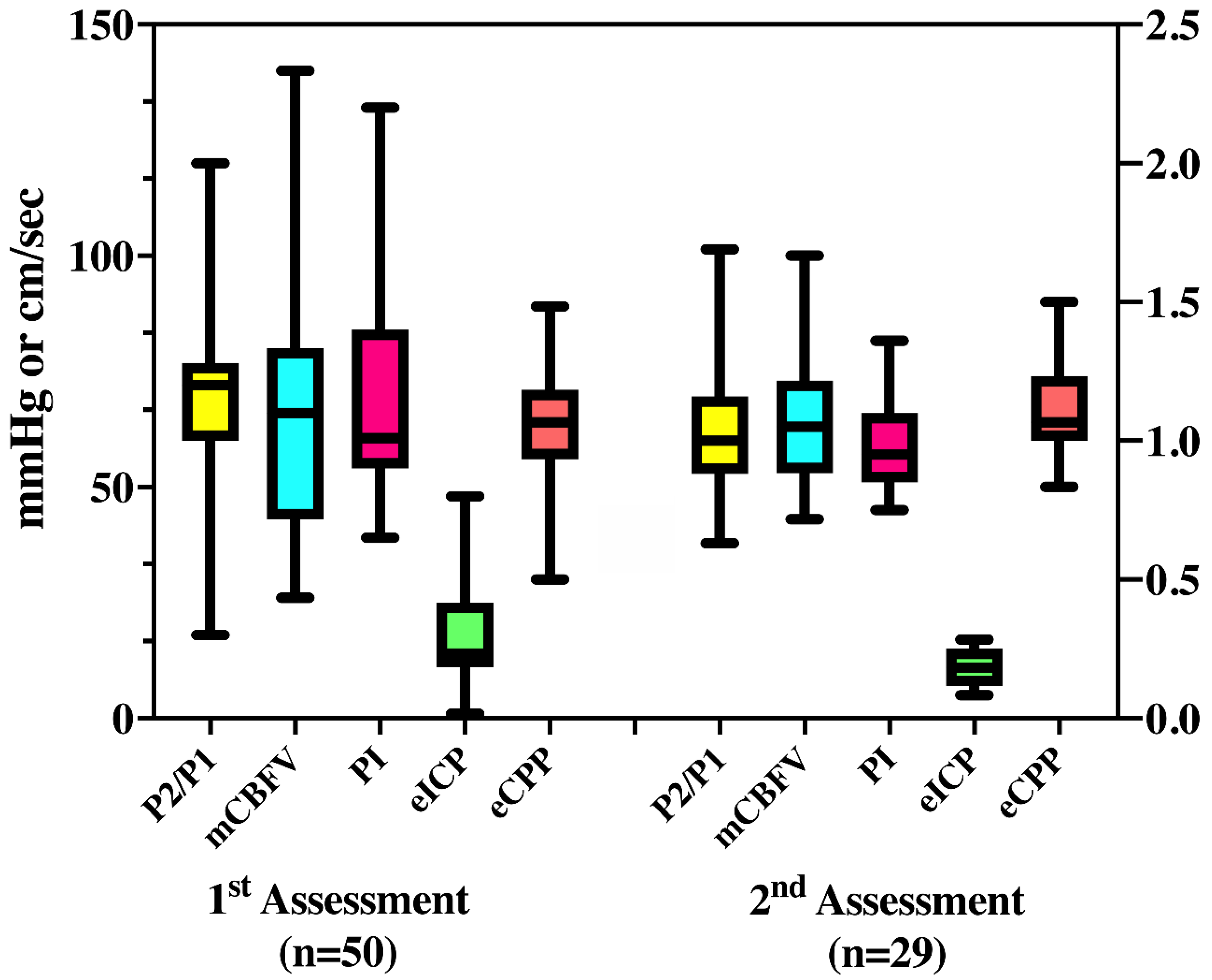
3.2. ICC and CVH Assessment
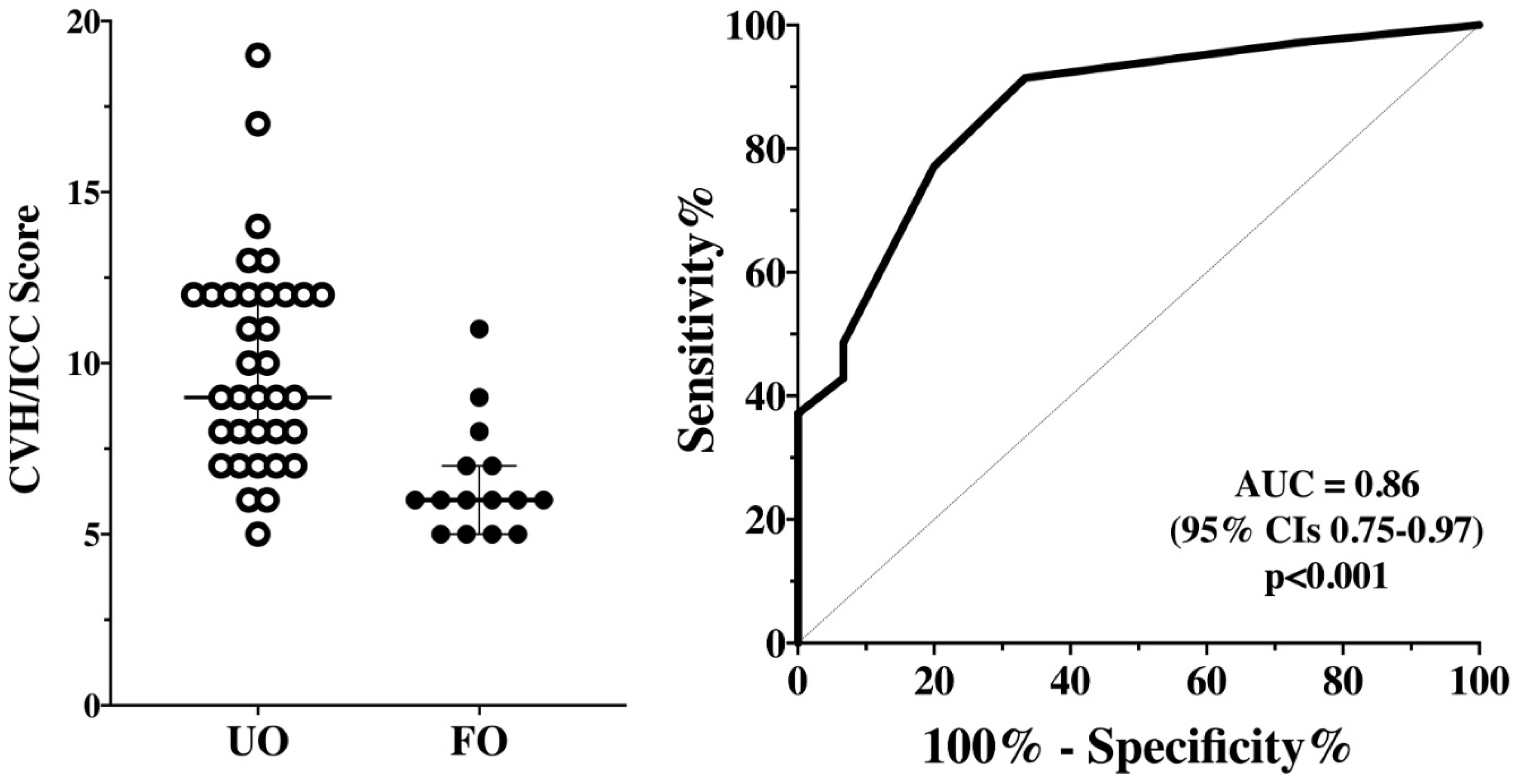
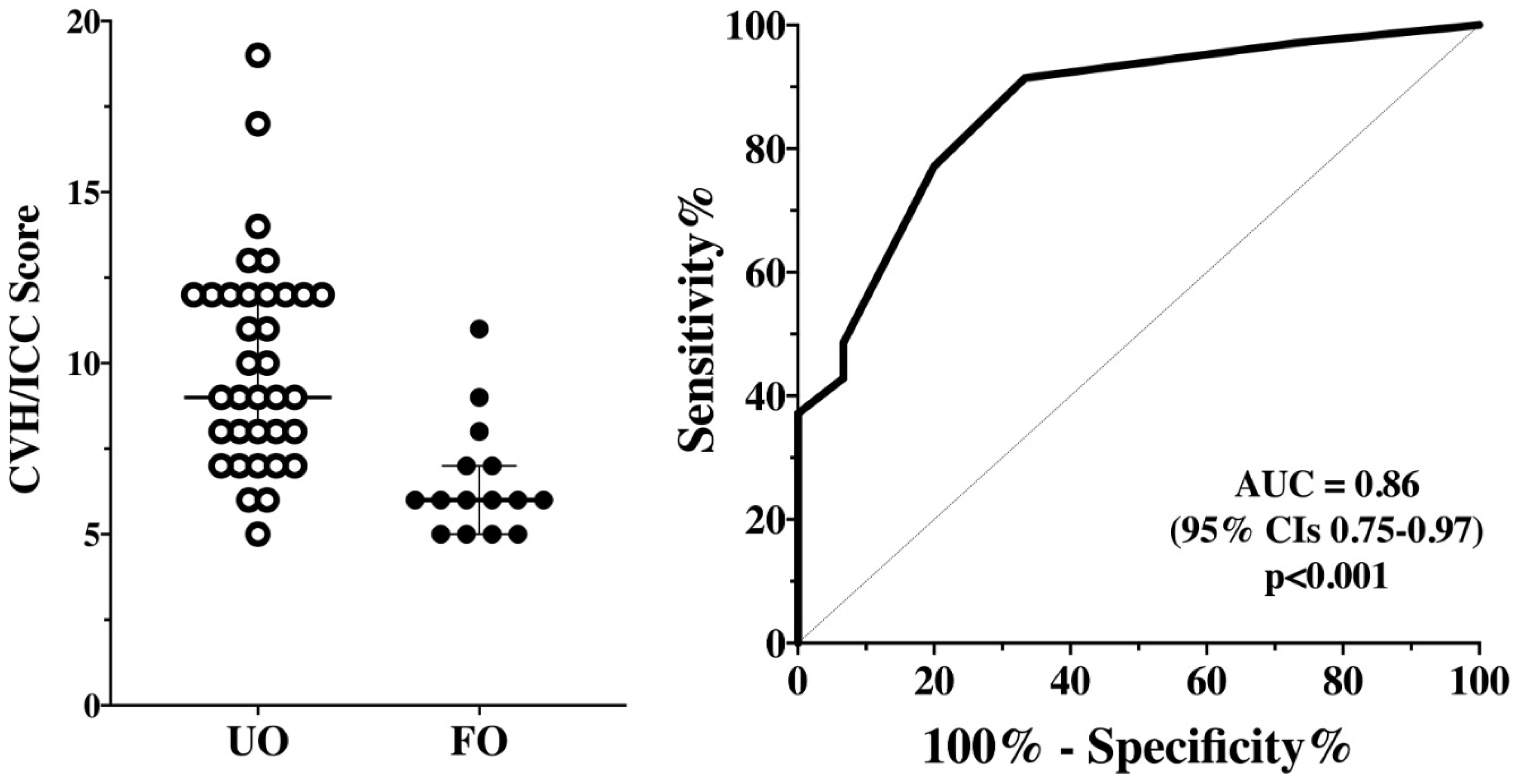
3.3. CVH/ICCI and Primary Outcome
3.4. CVH/ICCI and ICU Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, Y.C.; Bai, W.Z.; Hashikawa, T. The neuroinvasive potential of SARS-CoV2 may play a role in the respiratory failure of COVID-19 patients. J. Med. Virol. 2020, 92, 552–555. [Google Scholar] [CrossRef]
- Baig, A.M.; Khaleeq, A.; Ali, U.; Syeda, H. Evidence of the COVID-19 Virus targeting the CNS: Tissue distribution, host-virus interaction, and proposed neurotropic mechanisms. ACS Chem. Neurosci. 2020, 11, 995–998. [Google Scholar] [CrossRef] [Green Version]
- Needham, E.J.; Chou, S.H.; Coles, A.J.; Menon, D.K. Neurological implications of COVID-19 infections. Neurocrit. Care 2020, 32, 667–671. [Google Scholar] [CrossRef] [PubMed]
- Bridwell, R.; Long, B.; Gottlieb, M. Neurologic complications of COVID-19. Am. J. Emerg. Med. 2020, 38, 1549.e3–1549.e7. [Google Scholar] [CrossRef]
- Niazkar, H.R.; Zibaee, B.; Nasimi, A.; Bahri, N. The neurological manifestations of COVID-19: A review article. Neurol. Sci. 2020, 41, 1667–1671. [Google Scholar] [CrossRef] [PubMed]
- Solomon, I.H.; Normandin, E.; Bhattacharyya, S.; Mukerji, S.S.; Keller, K.; Ali, A.S.; Adams, G.; Hornick, J.L.; Padera, R.F., Jr.; Sabeti, P. Neuropathological features of Covid-19. N. Engl. J. Med. 2020, 383, 989–992. [Google Scholar] [CrossRef] [PubMed]
- Toscano, G.; Palmerini, F.; Ravaglia, S.; Ruiz, L.; Invernizzi, P.; Cuzzoni, M.G.; Franciotta, D.; Baldanti, F.; Daturi, R.; Postorino, P.; et al. Guillain-Barre syndrome associated with SARS-CoV-2. N. Engl. J. Med. 2020, 382, 2574–2576. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez-Ortiz, C.; Mendez, A.; Rodrigo-Rey, S.; San Pedro-Murillo, E.; Bermejo-Guerrero, L.; Gordo-Manas, R.; de Aragon-Gomez, F.; Benito-Leon, J. Miller Fisher syndrome and polyneuritis cranialis in COVID-19. Neurology 2020, 95, e601–e605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreau, A.; Ego, A.; Vandergheynst, F.; Taccone, F.S.; Sadeghi, N.; Montesinos, I.; Gaspard, N.; Gorham, J. Cytotoxic lesions of the corpus callosum (CLOCCs) associated with SARS-CoV-2 infection. J. Neurol. 2020, 268, 1592–1594. [Google Scholar] [CrossRef]
- Spallazzi, M.; Morelli, N.; Taga, A. COVID-19 and neurologic manifestations: A still missing link and a call for neurologists. Neurol. Sci. 2020, 41, 1997–1998. [Google Scholar] [CrossRef]
- Wu, Y.; Xu, X.; Chen, Z.; Duan, J.; Hashimoto, K.; Yang, L.; Liu, C.; Yang, C. Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain Behav. Immun. 2020, 87, 18–22. [Google Scholar] [CrossRef]
- Delanghe, J.R.; Speeckaert, M.M.; de Buyzere, M.L. The host’s angiotensin-converting enzyme polymorphism may explain epidemiological findings in COVID-19 infections. Clin. Chim. Acta 2020, 505, 192–193. [Google Scholar] [CrossRef]
- Deana, C.; Verriello, L.; Pauletto, G.; Corradi, F.; Forfori, F.; Cammarota, G.; Bignami, E.; Vetrugno, L.; Bove, T. Insights into neurological dysfunction of critically ill COVID-19 patients. Trends Anaesth. Crit. Care 2021, 36, 30–38. [Google Scholar] [CrossRef]
- Paterson, R.W.; Brown, R.L.; Benjamin, L.; Nortley, R.; Wiethoff, S.; Bharucha, T.; Jayaseelan, D.L.; Kumar, G.; Raftopoulos, R.E.; Zambreanu, L.; et al. The emerging spectrum of COVID-19 neurology: Clinical, radiological and laboratory findings. Brain 2020, 143, 3104–3120. [Google Scholar] [CrossRef]
- Rogers, J.P.; Chesney, E.; Oliver, D.; Pollak, T.A.; McGuire, P.; Fusar-Poli, P.; Zandi, M.S.; Lewis, G.; David, A.S. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: A systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 611–627. [Google Scholar] [CrossRef]
- Kochanek, P.M.; Tasker, R.C.; Carney, N.; Totten, A.M.; Adelson, P.D.; Selden, N.R.; Davis-O’Reilly, C.; Hart, E.L.; Bell, M.J.; Bratton, S.L.; et al. Guidelines for the management of pediatric severe traumatic brain injury, third edition: Update of the brain trauma foundation guidelines. Pediatr. Crit. Care Med. 2019, 20, S1–S82. [Google Scholar] [CrossRef] [Green Version]
- Frigieri, G.; Andrade, R.A.P.; Dias, C.; Spavieri, D.L., Jr.; Brunelli, R.; Cardim, D.A.; Wang, C.C.; Verzola, R.M.M.; Mascarenhas, S. Analysis of a non-invasive intracranial pressure monitoring method in patients with traumatic brain injury. Acta Neurochir. Suppl. 2018, 126, 107–110. [Google Scholar] [CrossRef]
- Vilela, G.H.; Cabella, B.; Mascarenhas, S.; Czosnyka, M.; Smielewski, P.; Dias, C.; Cardim, D.A.; Mascarenhas, Y.M.; Wang, C.C.; Andrade, R.; et al. Validation of a New Minimally Invasive Intracranial Pressure Monitoring Method by Direct Comparison with an Invasive Technique. Acta Neurochir. Suppl. 2016, 122, 97–100. [Google Scholar] [CrossRef]
- Cabella, B.; Vilela, G.H.; Mascarenhas, S.; Czosnyka, M.; Smielewski, P.; Dias, C.; Cardim, D.A.; Wang, C.C.; Mascarenhas, P.; Andrade, R.; et al. Validation of a New Noninvasive Intracranial Pressure Monitoring Method by Direct Comparison with an Invasive Technique. Acta Neurochir. Suppl. 2016, 122, 93–96. [Google Scholar] [CrossRef]
- Brasil, S.; Bor-Seng-Shu, E.; de-Lima-Oliveira, M.; Taccone, F.S.; Gattas, G.; Nunes, D.M.; de Oliveira, R.A.G.; Martins Tomazini, B.; Tierno, P.F.; Becker, R.A.; et al. Computed tomography angiography accuracy in brain death diagnosis. J. Neurosurg. 2019, 133, 1220–1228. [Google Scholar] [CrossRef]
- Ballestero, M.F.M.; Frigieri, G.; Cabella, B.C.T.; de Oliveira, S.M.; de Oliveira, R.S. Prediction of intracranial hypertension through noninvasive intracranial pressure waveform analysis in pediatric hydrocephalus. Childs Nerv. Syst. 2017, 33, 1517–1524. [Google Scholar] [CrossRef]
- Nucci, C.G.; de Bonis, P.; Mangiola, A.; Santini, P.; Sciandrone, M.; Risi, A.; Anile, C. Intracranial pressure wave morphological classification: Automated analysis and clinical validation. Acta Neurochir. 2016, 158, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Nag, D.S.; Sahu, S.; Swain, A.; Kant, S. Intracranial pressure monitoring: Gold standard and recent innovations. World J. Clin. Cases 2019, 7, 1535–1553. [Google Scholar] [CrossRef] [PubMed]
- Panerai, R.B.; Hudson, V.; Fan, L.; Mahony, P.; Yeoman, P.M.; Hope, T.; Evans, D.H. Assessment of dynamic cerebral autoregulation based on spontaneous fluctuations in arterial blood pressure and intracranial pressure. Physiol. Meas. 2002, 23, 59–72. [Google Scholar] [CrossRef]
- Franklin, S. Chapter 5—The peripheral and central nervous system. In Conn’s Translational Neuroscience; Conn, P.M., Ed.; Academic Press: San Diego, CA, USA, 2017; pp. 113–129. [Google Scholar]
- Tegeler, C.H.; Crutchfield, K.; Katsnelson, M.; Kim, J.; Tang, R.; Passmore Griffin, L.; Rundek, T.; Evans, G. Transcranial doppler velocities in a large, healthy population. J. Neuroimaging 2013, 23, 466–472. [Google Scholar] [CrossRef]
- Robba, C.; Pozzebon, S.; Moro, B.; Vincent, J.L.; Creteur, J.; Taccone, F.S. Multimodal non-invasive assessment of intracranial hypertension: An observational study. Crit. Care 2020, 24, 379. [Google Scholar] [CrossRef]
- Czosnyka, M.; Matta, B.F.; Smielewski, P.; Kirkpatrick, P.J.; Pickard, J.D. Cerebral perfusion pressure in head-injured patients: A noninvasive assessment using transcranial Doppler ultrasonography. J. Neurosurg. 1998, 88, 802–808. [Google Scholar] [CrossRef] [PubMed]
- Rasulo, F.A.; Bertuetti, R.; Robba, C.; Lusenti, F.; Cantoni, A.; Bernini, M.; Girardini, A.; Calza, S.; Piva, S.; Fagoni, N.; et al. The accuracy of transcranial Doppler in excluding intracranial hypertension following acute brain injury: A multicenter prospective pilot study. Crit. Care 2017, 21, 44. [Google Scholar] [CrossRef] [Green Version]
- Morales, D.R.; Conover, M.M.; You, S.C.; Pratt, N.; Kostka, K.; Duarte Salles, T.; Fernandez Bertolin, S.; Aragon, M.; DuVall, S.L.; Lynch, K.; et al. Renin-angiotensin system blockers and susceptibility to COVID-19: A multinational open science cohort study. medRxiv 2020. [Google Scholar] [CrossRef]
- Fisman, D.N.; Greer, A.L.; Tuite, A.R. Age is just a number: A critically important number for COVID-19 case fatality. Ann. Intern. Med. 2020, 173, 762–763. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Huang, J.; Zhu, G.; Wang, Q.; Lv, Q.; Huang, Y.; Yu, Y.; Si, X.; Yi, H.; Wang, C.; et al. Elevation of blood glucose level predicts worse outcomes in hospitalized patients with COVID-19: A retrospective cohort study. BMJ Open Diabetes Res. Care 2020, 8, e001476. [Google Scholar] [CrossRef]
- Wong, S.H.; Lui, R.N.; Sung, J.J. Covid-19 and the digestive system. J. Gastroenterol. Hepatol. 2020, 35, 744–748. [Google Scholar] [CrossRef]
- Brasil, S.; Renck, A.C.; Taccone, F.S.; Fontoura Solla, D.J.; Tomazini, B.M.; Wayhs, S.Y.; Fonseca, S.; Bassi, E.; Lucena, B.; de Carvalho Nogueira, R.; et al. Obesity and its implications on cerebral circulation and intracranial compliance in severe COVID-19. Obes. Sci. Pract. 2021. [Google Scholar] [CrossRef]
- Kieser, M.; Wassmer, G. On the use of the upper confidence limit for the variance from a pilot sample for sample size determination. Biom. J. 1996, 38, 941–949. [Google Scholar] [CrossRef]
- Kazimierska, A.; Kasprowicz, M.; Czosnyka, M.; Placek, M.M.; Baledent, O.; Smielewski, P.; Czosnyka, Z. Compliance of the cerebrospinal space: Comparison of three methods. Acta Neurochir. 2021, 163, 1979–1989. [Google Scholar] [CrossRef]
- Asgari, S.; Bergsneider, M.; Hamilton, R.; Vespa, P.; Hu, X. Consistent changes in intracranial pressure waveform morphology induced by acute hypercapnic cerebral vasodilatation. Neurocrit. Care 2011, 15, 55–62. [Google Scholar] [CrossRef] [Green Version]
- Cardim, D.; Robba, C.; Donnelly, J.; Bohdanowicz, M.; Schmidt, B.; Damian, M.; Varsos, G.V.; Liu, X.; Cabeleira, M.; Frigieri, G.; et al. Prospective study on noninvasive assessment of intracranial pressure in traumatic brain-injured patients: Comparison of four methods. J. Neurotrauma 2016, 33, 792–802. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, M.V.; Melo, M.R.; Mowry, F.E.; Lucera, G.M.; Lauar, M.R.; Frigieri, G.; Biancardi, V.C.; Menani, J.V.; Colombari, D.S.A.; Colombari, E. Intracranial pressure during the development of renovascular hypertension. Hypertension 2021, 77, 1311–1322. [Google Scholar] [CrossRef]
- Battaglini, D.; Santori, G.; Chandraptham, K.; Iannuzzi, F.; Bastianello, M.; Tarantino, F.; Ball, L.; Giacobbe, D.R.; Vena, A.; Bassetti, M.; et al. Neurological complications and noninvasive multimodal neuromonitoring in critically Ill mechanically ventilated COVID-19 patients. Front. Neurol. 2020, 11, 602114. [Google Scholar] [CrossRef]
- Ziai, W.C.; Cho, S.M.; Johansen, M.C.; Ergin, B.; Bahouth, M.N. Transcranial doppler in acute COVID-19 infection: Unexpected associations. Stroke 2021, 52, 2422–2426. [Google Scholar] [CrossRef]
- Li, Y.; Li, M.; Wang, M.; Zhou, Y.; Chang, J.; Xian, Y.; Wang, D.; Mao, L.; Jin, H.; Hu, B. Acute cerebrovascular disease following COVID-19: A single center, retrospective, observational study. Stroke Vasc. Neurol. 2020, 5, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Fotuhi, M.; Mian, A.; Meysami, S.; Raji, C.A. Neurobiology of COVID-19. J. Alzheimers Dis. 2020, 76, 3–19. [Google Scholar] [CrossRef]
- Battaglini, D.; Brunetti, I.; Anania, P.; Fiaschi, P.; Zona, G.; Ball, L.; Giacobbe, D.R.; Vena, A.; Bassetti, M.; Patroniti, N.; et al. Neurological manifestations of severe SARS-CoV-2 infection: Potential mechanisms and implications of individualized mechanical ventilation settings. Front. Neurol. 2020, 11, 845. [Google Scholar] [CrossRef] [PubMed]
- Crippa, I.A.; Subira, C.; Vincent, J.L.; Fernandez, R.F.; Hernandez, S.C.; Cavicchi, F.Z.; Creteur, J.; Taccone, F.S. Impaired cerebral autoregulation is associated with brain dysfunction in patients with sepsis. Crit. Care 2018, 22, 327. [Google Scholar] [CrossRef] [Green Version]
- Taccone, F.S.; Crippa, I.A.; Creteur, J.; Rasulo, F. Estimated cerebral perfusion pressure among post-cardiac arrest survivors. Intensive Care Med. 2018, 44, 966–967. [Google Scholar] [CrossRef] [PubMed]
- Sonkaya, A.R.; OztUrk, B.; Karada, S.O. Cerebral hemodynamic alterations in patients with Covid-19. Turk. J. Med. Sci. 2020, 51, 435–439. [Google Scholar] [CrossRef]
- Van der Kleij, L.A.; de Vis, J.B.; de Bresser, J.; Hendrikse, J.; Siero, J.C.W. Arterial CO2 pressure changes during hypercapnia are associated with changes in brain parenchymal volume. Eur. Radiol. Exp. 2020, 4, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prakash, K.; Chandran, D.S.; Khadgawat, R.; Jaryal, A.K.; Deepak, K.K. Correction for blood pressure improves correlation between cerebrovascular reactivity assessed by breath holding and 6% CO(2) breathing. J. Stroke Cerebrovasc. Dis. 2014, 23, 630–635. [Google Scholar] [CrossRef]
- Meng, L.; Gelb, A.W. Regulation of cerebral autoregulation by carbon dioxide. Anesthesiology 2015, 122, 196–205. [Google Scholar] [CrossRef] [Green Version]
- Brower, R.G.; Matthay, M.A.; Morris, A.; Schoenfeld, D.; Thompson, B.T.; Wheeler, A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. Acute Respiratory Distress Syndrome Network. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Points | P2/P1 | mCBFV | PI | eICP | eCPP | Score (Sum of Each) |
|---|---|---|---|---|---|---|
| 1 | ≤1 | 40–70 | <1.2 | <15 | 50–75 | 5 no CVH/ICCI |
| 2 | 1.01–1.19 | 71–99 | ≥1.2 | 15–20 | ≥75 | 6–7 mild CVH/ICCI |
| 3 | ≥1.2 | ≥100 | ≥1.3 | 21–25 | ≤50 | 8–9 moderate CVH/ICCI |
| 4 | ≥1.4 | <40 | ≥1.4 | >25 | <40 | ≥10 severe CVH/ICCI |
| Characteristic | Total (n = 50) | FO (n = 17) | UO (n = 33) | Survivors (n = 20) | Non-Survivors (n = 30) |
|---|---|---|---|---|---|
| Age, median (IQR)—years | 62 (44–68) | 38 (17–63) | 64 (49–68) | 49 (17–63) | 66 (51–68) * |
| Female gender—no. (%) | 22 (44) | 8 (48) | 14 (43) | 9 (43) | 13 (45) |
| SAPS 3, median (IQR) | 63 (52–75) | 55 (51–72) | 69 (57–78) | 58 (51–69) | 67 (54–78) |
| Antibiotics use—no. (%) | 36 (77) | 14 (70) | 22 (82) | 15 (71) | 21 (81) |
| Comorbidities and risk factors—no. (%) | |||||
| Hypertension | 26 (54) | 9 (52) | 17 (51) | 11 (52) | 15 (56) |
| Diabetes | 15 (31) | 6 (35) | 9 (27) | 6 (29) | 9 (33) |
| Obesity | 23 (46) | 9 (52) | 14 (42) | 9 (43) | 11 (42) |
| Current smoker | 15 (31) | 5 (29) | 10 (30) | 6 (29) | 9 (33) |
| Chronic kidney failure | 7 (15) | 2 (11) | 5 (15) | 2 (10) | 5 (19) |
| Laboratory variables | |||||
| D-dimer—ng/mL, median (IQR) | 2304 (1120–5528) | 2018 (1120–6027) | 2512 (1007–18,631) | 2038 (1166–4792) | 2449 (1007–18,631) |
| Creatinine—mg/dL, median (IQR) | 1.25 (0.66–2.71) | 1.23 (0.66–2.52) | 1.41 (0.66–4.59) | 0.98 (0.62–1.82) | 1.45 (0.69–4.59) |
| Platelets count—×109/L | 240 (150–333) | 293 (146–375) | 217 (146–310) | 257(170–375) | 226 (146–310) |
| Intravenous sedation | |||||
| Midazolam—no. (%) | 44 (88) | 12 (70) | 23 (69) | 18 (86) | 26 (90) |
| Propofol—no. (%) | 13 (26) | 6 (30) | 7 (21) | 7 (33) | 6 (21) |
| Ketamine—no. (%) | 2 (4) | 0 | 2 (6) | 0 (0) | 2 (7) |
| On the day of the first assessment | |||||
| MAP—mmHg | 79 (72–87) | 83 (75–90) | 77 (72–83) | 84 (75–90) | 78 (72–82) |
| MAP < 65 mmHg—no. (%) | 2 (4) | – | 2 (6) | – | 2 (7) |
| Vasopressor use—no. (%) | 25 (50) | 9 (50) | 16 (32) | 8 (38) | 17 (77) |
| Heart rate—mmHg | 87 (75–98) | 75 (72–81) | 87 (79–104) | 78 (72–93) | 89 (82–104) |
| Respiratory rate—rpm | 26 (22–30) | 25 (22–31) | 29 (23–32) | 26 (22–29) | 28 (22–32) |
| Oxygen saturation (SaO2)—% | 93 (90–95) | 94 (90–97) | 92 (90–95) | 93 (91–94) | 92 (90–95) |
| PaO2 < 60 mmHg—no. (%) | 3 (6) | 1 (5) | 2 (6) | 1 (5) | 2 (7) |
| PaCO2—mmHg | 41 (37–49) | 39 (36–44) | 42 (40–44) | 40 (37–44) | 42 (38–44) |
| PaCO2 > 45 mmHg)—no. (%) | 16 (32) | 4 (22) | 12 (37) | 5 (24) | 11 (38) |
| Temperature—°C | 36.1 (35.6–36.9) | 36 (35.8–37) | 36.5 (35.5–38) | 36.2 (35.5–37.0) | 36.2 (35.7–38.0) |
| Hemoglobin—g/dL | 11.1 (8.8–12.7) | 11.2 (9.9–12.9) | 10.3 (8.7–13.1) | 11.6 (10.4–12.4) | 10.2 (8.7–13.1) |
| PaO2/FiO2 –median (IQR) | 145 (127–182) | 178 (141–216) | 132 (98–151) | 167 (138–216) | 136 (98–151) * |
| Renal replacement therapy—no. (%) | 13 (32) | 5 (27) | 8 (25) | 5 (26.3) | 8 (36) |
| Abnormal mCBFv n = 26 | Abnormal PI n = 19 | Abnormal eICP n = 14 | Abnormal eCPP n = 11 | Abnormal P2/P1 n = 33 | |
|---|---|---|---|---|---|
| Abnormal mCBFV n = 26 | - | 11 (42) | 10 (38) | 7 (27) | 18 (69) |
| Abnormal PI n = 19 | 11 (58) | - | 13 (68) | 5 (26) | 14 (73) |
| Abnormal eICP n = 14 | 10 (71) | 13 (93) | - | 6 (42) | 13 (93) |
| Abnormal eCPP n = 11 | 7 (63) | 5 (45) | 6 (54) | - | 6 (54) |
| Abnormal P2/P1 n = 33 | 18 (54) | 14 (42) | 13 (39) | 6 (18) | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brasil, S.; Taccone, F.S.; Wayhs, S.Y.; Tomazini, B.M.; Annoni, F.; Fonseca, S.; Bassi, E.; Lucena, B.; Nogueira, R.D.C.; De-Lima-Oliveira, M.; et al. Cerebral Hemodynamics and Intracranial Compliance Impairment in Critically Ill COVID-19 Patients: A Pilot Study. Brain Sci. 2021, 11, 874. https://doi.org/10.3390/brainsci11070874
Brasil S, Taccone FS, Wayhs SY, Tomazini BM, Annoni F, Fonseca S, Bassi E, Lucena B, Nogueira RDC, De-Lima-Oliveira M, et al. Cerebral Hemodynamics and Intracranial Compliance Impairment in Critically Ill COVID-19 Patients: A Pilot Study. Brain Sciences. 2021; 11(7):874. https://doi.org/10.3390/brainsci11070874
Chicago/Turabian StyleBrasil, Sérgio, Fabio Silvio Taccone, Sâmia Yasin Wayhs, Bruno Martins Tomazini, Filippo Annoni, Sérgio Fonseca, Estevão Bassi, Bruno Lucena, Ricardo De Carvalho Nogueira, Marcelo De-Lima-Oliveira, and et al. 2021. "Cerebral Hemodynamics and Intracranial Compliance Impairment in Critically Ill COVID-19 Patients: A Pilot Study" Brain Sciences 11, no. 7: 874. https://doi.org/10.3390/brainsci11070874
APA StyleBrasil, S., Taccone, F. S., Wayhs, S. Y., Tomazini, B. M., Annoni, F., Fonseca, S., Bassi, E., Lucena, B., Nogueira, R. D. C., De-Lima-Oliveira, M., Bor-Seng-Shu, E., Paiva, W., Turgeon, A. F., Jacobsen Teixeira, M., & Malbouisson, L. M. S. (2021). Cerebral Hemodynamics and Intracranial Compliance Impairment in Critically Ill COVID-19 Patients: A Pilot Study. Brain Sciences, 11(7), 874. https://doi.org/10.3390/brainsci11070874