
Should Echolalia Be Considered a Phonic Stereotypy? A Narrative Review



{kind=link}
Abstract
:1. Introduction
- Stereotyped or repetitive motor movements, use of objects or speech;
- Insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior;
- Highly restricted, fixated interests with abnormal intensity or focus;
- Hyper- or hypo-reactivity to sensory input or unusual interest in sensory elements.
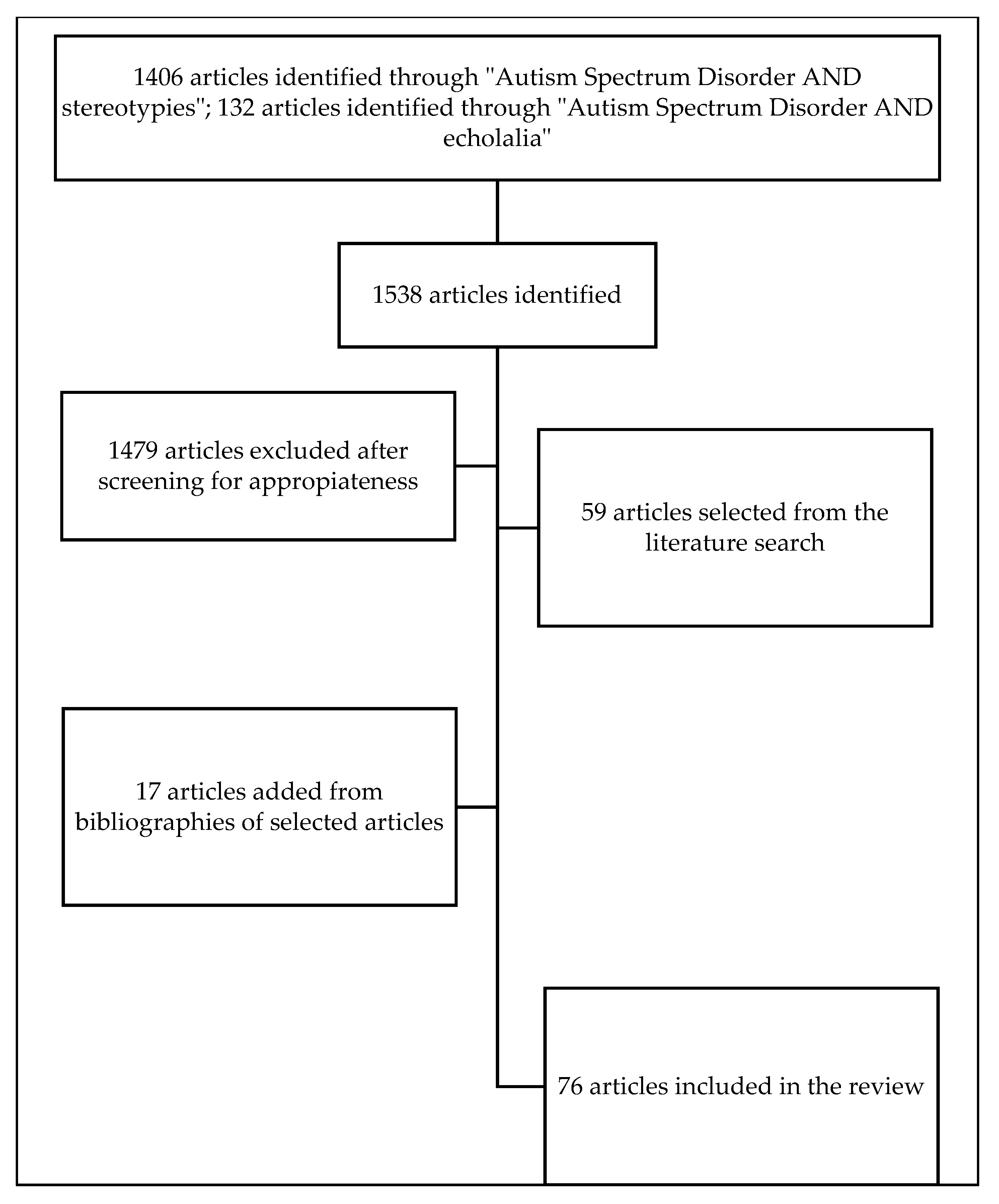
2. Methods
3. Results
3.1. RRBs and Stereotypies
3.2. Phonic Stereotypies
- Simple: any straightforward and distinct sound whose utterance requires little effort;
- Complex: any sound that mimics physiological functions such as hyperventilation, nonsensical word repetitions, or any other sound that is notably complex in nature. Classification of PS based on the quality of phonation:
- Vocal: communicative vocalizations, syllables, echolalia [37];
- Non-vocal: guttural emissions and non-communicative vocalizations such as throat clearing, grunting, buzzing, whistling, laughing, and coughing [38].
3.3. Language Development in Children with ASD
3.4. Echolalia and Echoic Behaviour
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Simonoff, E.; Pickles, A.; Charman, T.; Chandler, S.; Loucas, T.; Baird, G. Psychiatric Disorders in Children With Autism Spectrum Disorders: Prevalence, Comorbidity, and Associated Factors in a Population-Derived Sample. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 921–929. [Google Scholar] [CrossRef] [Green Version]
- Taurines, R.; Schwenck, C.; Westerwald, E.; Sachse, M.; Siniatchkin, M.; Freitag, C. ADHD and autism: Differential diagnosis or overlapping traits? A selective review. ADHD Atten. Deficit Hyperact. Disord. 2012, 4, 115–139. [Google Scholar] [CrossRef]
- Pruccoli, J.; Solari, A.; Terenzi, L.; Malaspina, E.; Angotti, M.; Pignataro, V.; Gualandi, P.; Sacrato, L.; Cordelli, D.M.; Franzoni, E.; et al. Autism spectrum disorder and anorexia nervosa: An Italian prospective study. Ital. J. Pediatr. 2021, 47, 1–6. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, (DSM-V); American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- D’Cruz, A.-M.; Ragozzino, M.; Mosconi, M.W.; Shrestha, S.; Cook, E.H.; Sweeney, J.A. Reduced behavioral flexibility in autism spectrum disorders. Neuropsychology 2013, 27, 152–160. [Google Scholar] [CrossRef] [Green Version]
- Parmeggiani, A.; Corinaldesi, A.; Posar, A. Early features of autism spectrum disorder: A cross-sectional study. Ital. J. Pediatr. 2019, 45, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Berkson, G. Repetitive stereotyped behaviors. Am. J. Ment. Defic. 1983, 88, 239–246. [Google Scholar] [PubMed]
- Lanzarini, E.; Pruccoli, J.; Grimandi, I.; Spadoni, C.; Angotti, M.; Pignataro, V.; Sacrato, L.; Franzoni, E.; Parmeggiani, A. Phonic and Motor Stereotypies in Autism Spectrum Disorder: Video Analysis and Neurological Characterization. Brain Sci. 2021, 11, 431. [Google Scholar] [CrossRef] [PubMed]
- Burrow, J.P.; Spurling, B.C.; Marwaha, R. Catatonia; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Mendez, M.F.; Perryman, K.M. Neuropsychiatric features of frontotemporal dementia: Evaluation of consensus criteria and review. J. Neuropsychiatry Clin. Neurosci. 2002, 14, 424–429. [Google Scholar] [CrossRef]
- Natasha Marrus, M.D.; Lacey Hall, M.S. Intellectual Disability and Language Disorder. Child Adolesc. Psychiatr. Clin. N. Am. 2017, 26, 539–554. [Google Scholar] [CrossRef] [PubMed]
- Turner, M. Annotation: Repetitive Behaviour in Autism: A Review of Psychological Research. J. Child Psychol. Psychiatry 1999, 40, 839–849. [Google Scholar] [CrossRef]
- Birdwhistell, R.L.; Hutt, S.J.; Hutt, C. Direct Observation and Measurement of Behavior. Springfield, Ill: Charles C Thomas, 1970. Pp. 224 + xii. $14.95. Am. J. Clin. Hypn. 1972, 14, 263–264. [Google Scholar]
- Lewis, F.M.; Murdoch, B.E.; Woodyatt, G.C. Communicative Competence and Metalinguistic Ability: Performance by Children and Adults with Autism Spectrum Disorder. J. Autism Dev. Disord. 2007, 37, 1525–1538. [Google Scholar] [CrossRef]
- Cheung, C.; Chua, S.; Cheung, V.; Khong, P.; Tai, K.; Wong, T.; Ho, T.; McAlonan, G. White matter fractional anisotrophy differences and correlates of diagnostic symptoms in autism. J. Child Psychol. Psychiatry 2009, 50, 1102–1112. [Google Scholar] [CrossRef] [PubMed]
- Weng, S.-J.; Wiggins, J.L.; Peltier, S.J.; Carrasco, M.; Risi, S.; Lord, C.; Monk, C.S. Alterations of resting state functional connectivity in the default network in adolescents with autism spectrum disorders. Brain Res. 2010, 1313, 202–214. [Google Scholar] [CrossRef] [Green Version]
- Uddin, L.Q.; Esupekar, K.; Emenon, V. Reconceptualizing functional brain connectivity in autism from a developmental perspective. Front. Hum. Neurosci. 2013, 7, 458. [Google Scholar] [CrossRef] [Green Version]
- Lovaas, O.I. Behavioral treatment and normal educational and intellectual functioning in young autistic children. J. Consult. Clin. Psychol. 1987, 55, 3–9. [Google Scholar] [CrossRef]
- Kennedy, G.S.C.H.; Souza, G. Functional Analysis and Treatment of Eye Poking. J. Appl. Behav. Anal. 1995, 28, 27–37. [Google Scholar] [CrossRef]
- Rapp, J.T.; Miltenberger, R.G.; Galensky, T.L.; Ellingson, S.A.; Long, E.S. A Functional Analysis of Hair Pulling. J. Appl. Behav. Anal. 1999, 32, 329–337. [Google Scholar] [CrossRef] [Green Version]
- Iwata, B.A. On the distinction between positive and negative reinforcement. Behav. Anal. 2006, 29, 121–123. [Google Scholar] [CrossRef]
- Rincover, A. Sensory Extinction: A procedure for eliminating self-stimulatory behavior in developmentally disabled children. J. Abnorm. Child Psychol. 1978, 6, 299–310. [Google Scholar] [CrossRef]
- Sprague, J.; Holland, K.; Thomas, K. The effect of noncontingent sensory reinforcement, contingent sensory reinforcement, and response interruption on stereotypical and self-injurious behavior. Res. Dev. Disabil. 1997, 18, 61–77. [Google Scholar] [CrossRef]
- Piazza, C.C.; Adelinis, J.D.; Hanley, G.P.; Goh, H.-L.; Delia, M.D. An Evaluation of The Effects of Matched Stimuli on Behaviors Maintained by Automatic Reinforcement. J. Appl. Behav. Anal. 2000, 33, 13–27. [Google Scholar] [CrossRef]
- Tang, J.-C.; Patterson, T.G.; Kennedy, C.H. Identifying specific sensory modalities maintaining the stereotypy of students with multiple profound disabilities. Res. Dev. Disabil. 2003, 24, 433–451. [Google Scholar] [CrossRef] [PubMed]
- Higbee, T.S.; Chang, S.-M.; Endicott, K. Noncontingent access to preferred sensory stimuli as a treatment for automatically reinforced stereotypy. Behav. Interv. 2005, 20, 177–184. [Google Scholar] [CrossRef]
- Fetta, A.; Carati, E.; Moneti, L.; Pignataro, V.; Angotti, M.; Bardasi, M.; Cordelli, D.; Franzoni, E.; Parmeggiani, A. Relationship between Sensory Alterations and Repetitive Behaviours in Children with Autism Spectrum Disorders: A Parents’ Questionnaire Based Study. Brain Sci. 2021, 11, 484. [Google Scholar] [CrossRef]
- Tröster, H.; Brambring, M.; Beelmann, A. The age dependence of stereotyped behaviours in blind infants and preschoolers. Child Care Heal. Dev. 1991, 17, 137–157. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, C.H.; Meyer, K.A.; Knowles, T.; Shukla, S. Analyzing the multiple functions of stereotypical behavior for students with autism: Implications for assessment and treatment. J. Appl. Behav. Anal. 2000, 33, 559–571. [Google Scholar] [CrossRef] [Green Version]
- Durand, V.M.; Carr, E.G. Social Influences on “Self-Stimulatory” Behavior: Analysis and Treatment Application. J. Appl. Behav. Anal. 1987, 20, 119–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koegel, R.L.; Covert, A. The relationship of self-stimulation to learning in autistic children1. J. Appl. Behav. Anal. 1972, 5, 381–387. [Google Scholar] [CrossRef] [Green Version]
- Lovaas, O.; Litrownik, A.; Mann, R. Response latencies to auditory stimuli in autistic children engaged in self-stimulatory behavior. Behav. Res. Ther. 1971, 9, 39–49. [Google Scholar] [CrossRef]
- Sherer, M.R.; Schreibman, L. Individual Behavioral Profiles and Predictors of Treatment Effectiveness for Children With Autism. J. Consult. Clin. Psychol. 2005, 73, 525–538. [Google Scholar] [CrossRef] [Green Version]
- Shore, L.M.; Randel, A.E.; Chung, B.G.; Dean, M.A.; Ehrhart, K.H.; Singh, G. Inclusion and Diversity in Work Groups: A Review and Model for Future Research. J. Manag. 2010, 37, 1262–1289. [Google Scholar] [CrossRef] [Green Version]
- Van Santen, J.P.H.; Sproat, R.W.; Hill, A.P. Quantifying Repetitive Speech in Autism Spectrum Disorders and Language Impairment. Autism Res. 2013, 6, 372–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yankowitz, L.D.; Schultz, R.T.; Parish-Morris, J. Pre- and Paralinguistic Vocal Production in ASD: Birth Through School Age. Curr. Psychiatry Rep. 2019, 21, 126. [Google Scholar] [CrossRef] [PubMed]
- Healy, O.; Lydon, S.; Brady, T.; Rispoli, M.; Holloway, J.; Neely, L.; Grey, I. The Use of Differential Reinforcement of Other Behaviours to Establish Inhibitory Stimulus Control for the Management of Vocal Stereotypy in Children with Autism. Dev. Neurorehabilit. 2018, 22, 192–202. [Google Scholar] [CrossRef]
- Min, C.-H.; Fetzner, J. Vocal Stereotypy Detection: An Initial Step to Understanding Emotions of Children with Autism Spectrum Disorder. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. (EMBC) 2018, 2018, 3306–3309. [Google Scholar]
- Singer, H.S. Motor Stereotypies. Semin. Pediatr. Neurol. 2009, 16, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Herlihy, L.; Knoch, K.; Vibert, B.; Fein, D. Parents’ first concerns about toddlers with autism spectrum disorder: Effect of sibling status. Autism 2013, 19, 20–28. [Google Scholar] [CrossRef] [Green Version]
- Lang, S.; Bartl-Pokorny, K.D.; Pokorny, F.B.; Garrido, D.; Mani, N.; Fox-Boyer, A.V.; Zhang, D.; Marschik, P.B. Canonical Babbling: A Marker for Earlier Identification of Late Detected Developmental Disorders? Curr. Dev. Disord. Rep. 2019, 6, 111–118. [Google Scholar] [CrossRef] [Green Version]
- Eilers, R.E.; Oller, D.K.; Levine, S.; Basinger, D.; Lynch, M.P.; Urbano, R. The role of prematurity and socioeconomic status in the onset of canonical babbling in infants. Infant Behav. Dev. 1993, 16, 297–315. [Google Scholar] [CrossRef]
- Oller, D.K.; Eilers, R.E.; Basinger, D.; Steffens, M.L.; Urbano, R. Extreme poverty and the development of precursors to the speech capacity. First Lang. 1995, 15, 167–187. [Google Scholar] [CrossRef]
- Patten, E.; Belardi, K.; Baranek, G.; Watson, L.R.; Labban, J.D.; Oller, D.K. Vocal Patterns in Infants with Autism Spectrum Disorder: Canonical Babbling Status and Vocalization Frequency. J. Autism Dev. Disord. 2014, 44, 2413–2428. [Google Scholar] [CrossRef] [Green Version]
- Watt, N.; Wetherby, A.; Shumway, S. Prelinguistic Predictors of Language Outcome at 3 Years of Age. J. Speech Lang. Hear. Res. 2006, 49, 1224–1237. [Google Scholar] [CrossRef]
- Marschik, P.B.; Einspieler, C.; Sigafoos, J. Contributing to the early detection of Rett syndrome: The potential role of auditory Gestalt perception. Res. Dev. Disabil. 2012, 33, 461–466. [Google Scholar] [CrossRef] [Green Version]
- Paul, R.; Fuerst, Y.; Ramsay, G.; Chawarska, K.; Klin, A. Out of the mouths of babes: Vocal production in infant siblings of children with ASD. J. Child Psychol. Psychiatry 2010, 52, 588–598. [Google Scholar] [CrossRef] [Green Version]
- Warlaumont, A.S.; Richards, J.A.; Gilkerson, J.; Oller, D.K. A Social Feedback Loop for Speech Development and Its Reduction in Autism. Psychol. Sci. 2014, 25, 1314–1324. [Google Scholar] [CrossRef] [Green Version]
- Swanson, M.R.; Shen, M.D.; Wolff, J.J.; Boyd, B.; Clements, M.; Rehg, J.; Elison, J.T.; Paterson, S.; Parish-Morris, J.; Chappell, J.C.; et al. Naturalistic Language Recordings Reveal “Hypervocal” Infants at High Familial Risk for Autism. Child Dev. 2018, 89, e60–e73. [Google Scholar] [CrossRef] [Green Version]
- Warren, S.F.; Gilkerson, J.; Richards, J.A.; Oller, D.K.; Xu, D.; Yapanel, U.; Gray, S. What Automated Vocal Analysis Reveals About the Vocal Production and Language Learning Environment of Young Children with Autism. J. Autism Dev. Disord. 2009, 40, 555–569. [Google Scholar] [CrossRef]
- English, M.S.; Tenenbaum, E.J.; Levine, T.P.; Lester, B.M.; Sheinkopf, S.J. Perception of Cry Characteristics in 1-Month-Old Infants Later Diagnosed with Autism Spectrum Disorder. J. Autism Dev. Disord. 2018, 49, 834–844. [Google Scholar] [CrossRef]
- Furlow, F. Human Neonatal Cry Quality as an honest signal of fitness. Evol. Hum. Behav. 1997, 18, 175–193. [Google Scholar] [CrossRef]
- Esposito, G.; Venuti, P. Developmental changes in the fundamental frequency (f0) of infants’ cries: A study of children with Autism Spectrum Disorder. Early Child Dev. Care 2010, 180, 1093–1102. [Google Scholar] [CrossRef]
- Bornstein, M.; Costlow, K.; Truzzi, A.; Esposito, G. Categorizing the cries of infants with ASD versus typically developing infants: A study of adult accuracy and reaction time. Res. Autism Spectr. Disord. 2016, 31, 66–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Riper, C. Speech Correction; Prentice Hall: Hoboken, NJ, USA, 1963. [Google Scholar]
- Nakanishi, Y.; Owada, K. Echoic utterances of children between the ages of one and three years. J. Verbal Learn. Verbal Behav. 1973, 12, 658–665. [Google Scholar] [CrossRef]
- Fay, W.H. On the basis of autistic echolalia. J. Commun. Disord. 1969, 2, 38–47. [Google Scholar] [CrossRef]
- Haworth, M.R.; Menolascino, F.J. Some Aspects of Psychotic Behavior in Young Children. Arch. Gen. Psychiatry 1968, 18, 355–359. [Google Scholar] [CrossRef] [PubMed]
- Esch, J.W.; Mahoney, A.M.; Kestner, K.M.; LaLonde, K.B.; Esch, B.E. Echoic and Self-Echoic Responses in Children. Anal. Verbal Behav. 2013, 29, 117–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fay, W.H.; Butler, B.V. Echolalia, IQ, and the Developmental Dichotomy of Speech and Language Systems. J. Speech Hear. Res. 1968, 11, 365–371. [Google Scholar] [CrossRef]
- Fay, W.H.; Butler, B.V. Echo-Reaction as an Approach to Semantic Resolution. J. Speech Hear. Res. 1971, 14, 645–651. [Google Scholar] [CrossRef]
- Philips, G.M.; Dyer, C. Late Onset Echolalia in Autism and Allied Disorders. Int. J. Lang. Commun. Disord. 1977, 12, 47–59. [Google Scholar] [CrossRef]
- Charlop, M.H. The effects of echolalia on acquisition and generalization of receptive labeling in autistic children. J. Appl. Behav. Anal. 1983, 16, 111–126. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, M.T. Comunicative Functions of Echolalia in Children with Autism: Assessment and Treatment; University of California: San Diego, CA, USA, 2002. [Google Scholar]
- Prizant, B.M. Language Acquisition and Communicative Behavior in Autism. J. Speech Hear. Disord. 1983, 48, 296–307. [Google Scholar] [CrossRef] [PubMed]
- Prizant, B.M.; Duchan, J.F. The Functions of Immediate Echolalia in Autistic Children. J. Speech Hear. Disord. 1981, 46, 241–249. [Google Scholar] [CrossRef]
- McEvoy, R.E.; Loveland, K.A.; Landry, S.H. The functions of immediate echolalia in autistic children: A developmental perspective. J. Autism Dev. Disord. 1988, 18, 657–668. [Google Scholar] [CrossRef]
- Charlop, M.H. Setting effects on the occurrence of autistic children’s immediate echolalia. J. Autism Dev. Disord. 1986, 16, 473–483. [Google Scholar] [CrossRef]
- Resnick, S.M. A Review of the Literature and an Experimental Analysis of Echolalia; University of California at Los Angeles: Los Angeles, CA, USA, 1973. [Google Scholar]
- Curcio, F.; Paccia, J. Conversations with autistic children: Contingent relationships between features of adult input and children’s response adequacy. J. Autism Dev. Disord. 1987, 17, 81–93. [Google Scholar] [CrossRef]
- Rydell, P.J.; Mirenda, P. The effects of two levels of linguistic constraint on echolalia and generative language production in children with autism. J. Autism Dev. Disord. 1991, 21, 131–157. [Google Scholar] [CrossRef]
- Violette, J.; Swisher, L. Echolalic Responses by a Child With Autism to Four Experimental Conditions of Sociolinguistic Input. J. Speech, Lang. Hear. Res. 1992, 35, 139–147. [Google Scholar] [CrossRef]
- Matson, J.L.; Dempsey, T.; Fodstad, J.C. Stereotypies and repetitive/restrictive behaviours in infants with autism and pervasive developmental disorder. Dev. Neurorehabilit. 2009, 12, 122–127. [Google Scholar] [CrossRef]
- Ghanizadeh, A. Clinical Approach to Motor Stereotypies in Autistic Children. Iran. J. Pediatr. 2010, 20, 149–159. [Google Scholar] [PubMed]
- Sterponi, L.; De Kirby, K.; Shankey, J. Rethinking language in autism. Autism 2014, 19, 517–526. [Google Scholar] [CrossRef]
- Saad, A.G.D.F.; Goldfeld, M. A ecolalia no desenvolvimento da linguagem de pessoas autistas: Uma revisão bibliográfica. Pró-Fono Rev. de Atualização Científica 2009, 21, 255–260. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pruccoli, J.; Spadoni, C.; Orsenigo, A.; Parmeggiani, A. Should Echolalia Be Considered a Phonic Stereotypy? A Narrative Review. Brain Sci. 2021, 11, 862. https://doi.org/10.3390/brainsci11070862
Pruccoli J, Spadoni C, Orsenigo A, Parmeggiani A. Should Echolalia Be Considered a Phonic Stereotypy? A Narrative Review. Brain Sciences. 2021; 11(7):862. https://doi.org/10.3390/brainsci11070862
Chicago/Turabian StylePruccoli, Jacopo, Chiara Spadoni, Alex Orsenigo, and Antonia Parmeggiani. 2021. "Should Echolalia Be Considered a Phonic Stereotypy? A Narrative Review" Brain Sciences 11, no. 7: 862. https://doi.org/10.3390/brainsci11070862
APA StylePruccoli, J., Spadoni, C., Orsenigo, A., & Parmeggiani, A. (2021). Should Echolalia Be Considered a Phonic Stereotypy? A Narrative Review. Brain Sciences, 11(7), 862. https://doi.org/10.3390/brainsci11070862