
Hippocampal Malrotation: A Genetic Developmental Anomaly Related to Epilepsy?

 ,
, 
Abstract
1. Introduction
2. Terminology
3. Normal Development of Human Hippocampus
4. Mechanisms of HIMAL Development
- Lack of infolding drive: The hippocampal infolding process is passively driven by the development of the neocortex, which pushes the hippocampus deeper into the temporal lobe forming the “Swiss roll” appearance. If there was a problem with neocortical development, the hippocampus would assume its prenatal position. This is likely the explanation for HIMAL associated with diffuse cortical malformations, for instance, periventricular heterotopia, polymicrogyria, and lissencephaly;
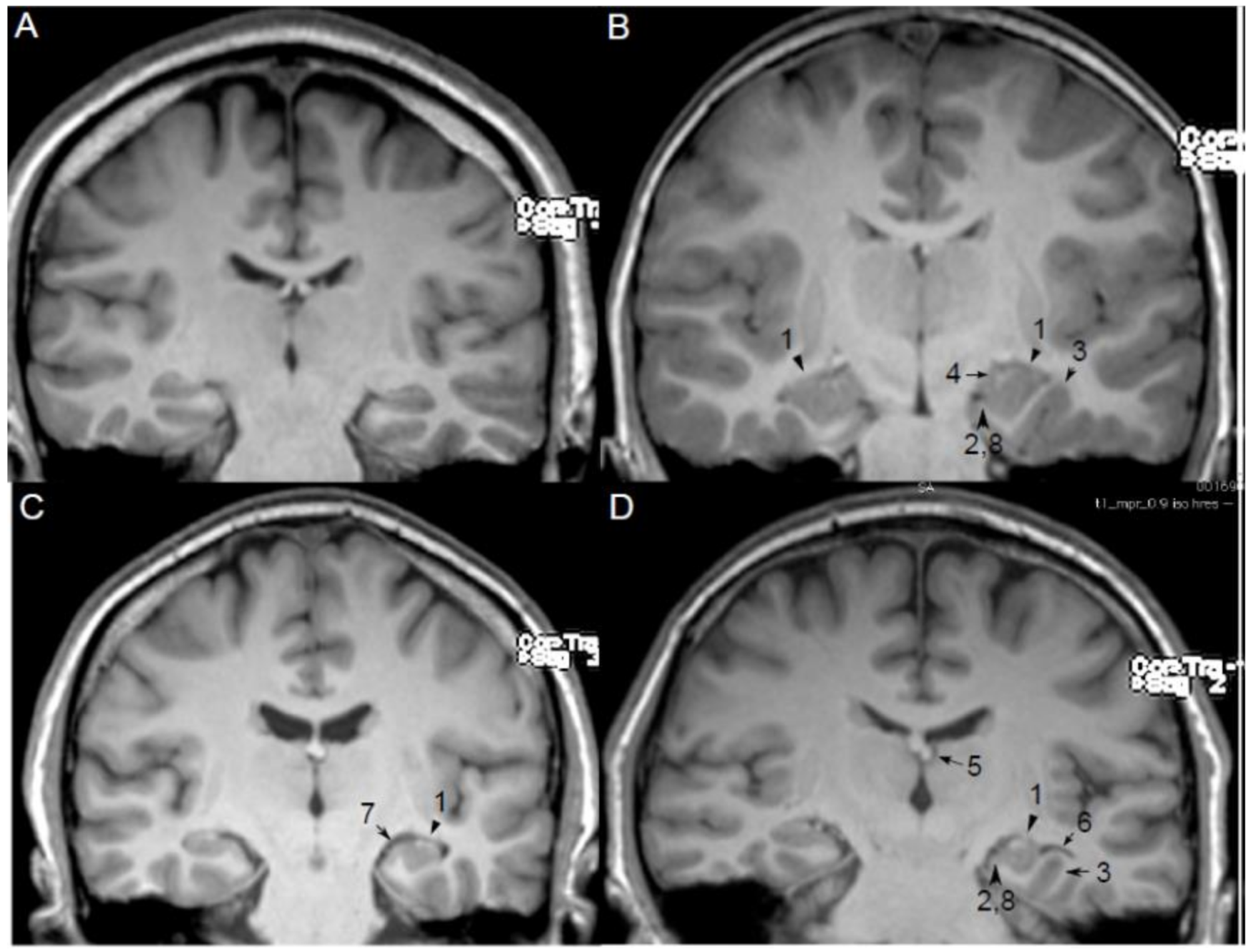
5. MRI Features and Qualitative Diagnosis of HIMAL
- Round or pyramidal shape instead of ovoid shape;
- Medial position of the hippocampus on the hippocampal sulcus;
- The collateral sulcus is excessively deep or “verticalized”;
- Fimbria located medial to the hippocampus;
- Small or displaced fornix;
- Enlarged temporal horn and empty choroid fissure;
- Thickened subiculum;
- Reduced upper horizontal portion of the parahippocampal gyrus.
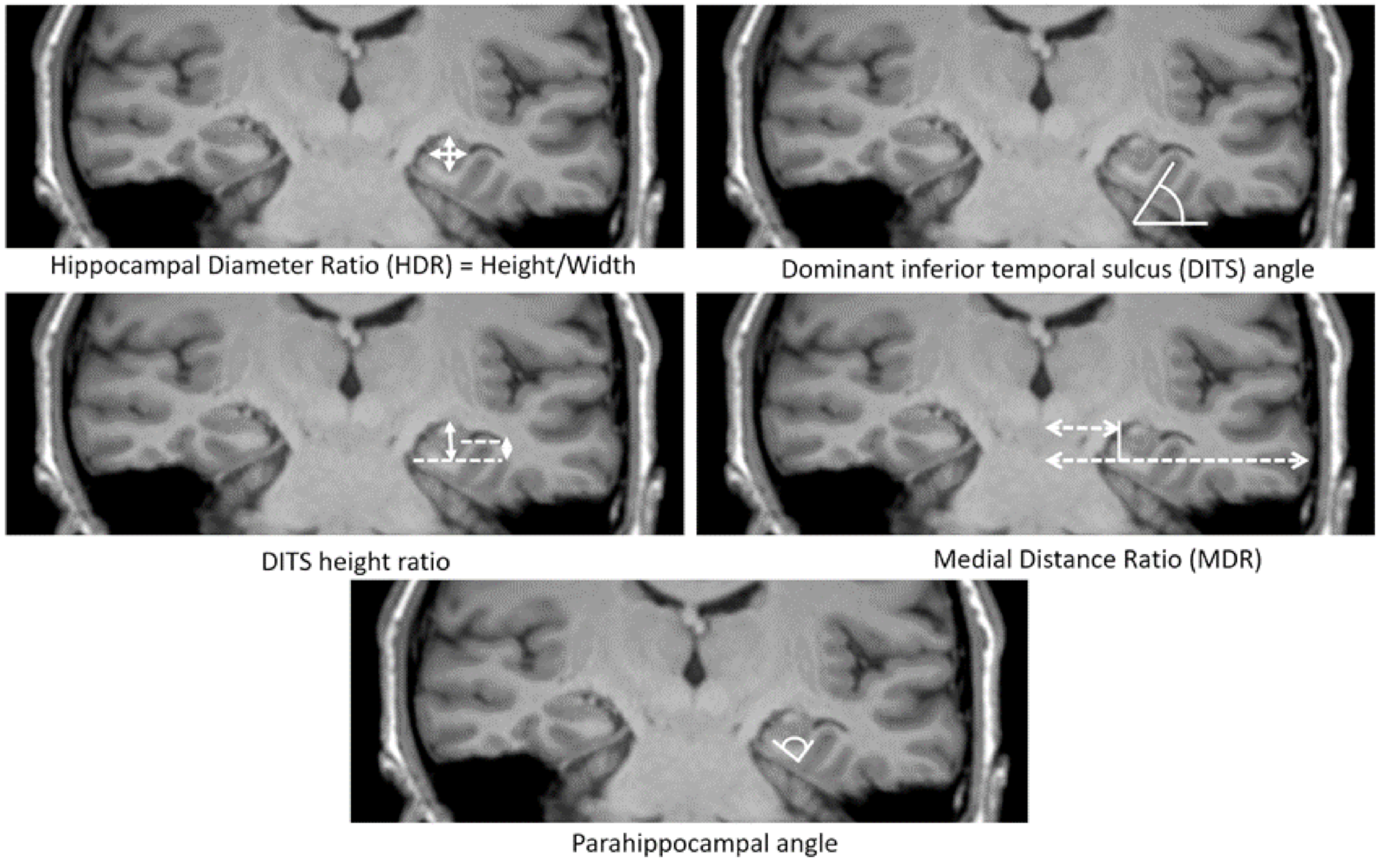
6. Measurements of HIMAL
7. Histopathology of HIMAL
8. Laterality of HIMAL
9. Epileptogenic Role of HIMAL
10. The Role of HIMAL on Pre-Surgical Decision
11. Relationship between HIMAL and HS
12. Genetics of HIMAL
13. Debates about Normal and Abnormal Hippocampus
14. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Baker, L.L.; Barkovich, A.J. The large temporal horn: MR analysis in developmental brain anomalies versus hydrocephalus. Am. J. Neuroradiol. 1992, 13, 115–122. [Google Scholar]
- Atlas, S.W.; Zimmerman, R.A.; Bilaniuk, L.T.; Rorke, L.; Hackney, D.B.; Goldberg, H.I.; Grossman, R.I. Corpus callosum and limbic system: Neuroanatomic MR evaluation of developmental anomalies. Radiology 1986, 160, 355–362. [Google Scholar] [CrossRef]
- Baulac, M.; De Grissac, N.; Hasboun, D.; Oppenheim, C.; Adam, C.; Arzimanoglou, A.; Semah, F.; Lehéricy, S.; Clémenceau, S.; Berger, B. Hippocampal developmental changes in patients with partial epilepsy: Magnetic resonance imaging and clinical aspects. Ann. Neurol. 1998, 44, 223–233. [Google Scholar] [CrossRef]
- Thom, M.; Sisodiya, S.M.; Lin, W.R.; Mitchell, T.; Free, S.L.; Stevens, J.; Scaravilli, F. Bilateral isolated hippocampal malformation in temporal lobe epilepsy. Neurology 2002, 58, 1683–1686. [Google Scholar] [CrossRef]
- Labate, A.; Sammarra, I.; Trimboli, M.; Caligiuri, M.E.; Gambardella, A. Looking for indicative magnetic resonance imaging signs of hippocampal developmental abnormalities in patients with mesial temporal lobe epilepsy and healthy controls. Epilepsia 2020, 61, 1714–1722. [Google Scholar] [CrossRef]
- Sen, A.; Thom, M.; Martinian, L.; Dawodu, S.; Sisodiya, S.M. Hippocampal malformations do not necessarily evolve into hippocampal sclerosis. Epilepsia 2005, 46, 939–943. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, G.; Effenberger, O.; Vinz, B.; Steinlein, O.; Elger, C.E.; Dohring, W.; Heinze, H.J. Hippocampal malformation as a cause of familial febrile convulsions and subsequent hippocampal sclerosis. Neurology 1998, 50, 909–917. [Google Scholar] [CrossRef] [PubMed]
- Humphrey, T. The development of the human hippocampal fissure. J. Anat. 1967, 101, 655–676. [Google Scholar]
- Kier, E.L.; Kim, J.H.; Fulbright, R.K.; Bronen, R.A. Embryology of the human fetal hippocampus: MR imaging, anatomy, and histology. Am. J. Neuroradiol. 1997, 18, 525–532. [Google Scholar] [PubMed]
- Gloor, P. Comparative Anatomy of the Temporal Lobe and of the Limbic System. In The Temporal Lobe and Limbic System; Oxford University Press Inc: New York, NY, USA, 1997; pp. 21–112. [Google Scholar]
- Bajic, D.; Moreira, N.C.; Wikström, J.; Raininko, R. Asymmetric development of the hippocampal region is common: A fetal MR imaging study. Am. J. Neuroradiol. 2011, 33, 513–518. [Google Scholar] [CrossRef]
- Utsunomiya, H.; Takano, K.; Okazaki, M.; Mitsudome, A. Development of the temporal lobe in infants and children: Analysis by MR-based volumetry. Am. J. Neuroradiol. 1999, 20, 717–723. [Google Scholar]
- Bigler, E.D.; Blatter, D.D.; Anderson, C.V.; Johnson, S.C.; Gale, S.D.; Hopkins, R.O.; Burnett, B. Hippocampal volume in normal aging and traumatic brain injury. Am. J. Neuroradiol. 1997, 18, 11–23. [Google Scholar]
- Li, Y.-J.; Ga, S.-N.; Huo, Y.; Li, S.-Y.; Gao, X.-G. Characteristics of hippocampal volumes in healthy Chinese from MRI. Neurol. Res. 2007, 29, 803–806. [Google Scholar] [CrossRef]
- Sloviter, R.S.; Kudrimoti, H.S.; Laxer, K.D.; Barbaro, N.M.; Chan, S.; Hirsch, L.J.; Goodman, R.R.; Pedley, T.A. “Tectonic” hippocampal malformations in patients with temporal lobe epilepsy. Epilepsy Res. 2004, 59, 123–153. [Google Scholar] [CrossRef]
- Lehéricy, S.; Dormont, D.; Sémah, F.; Clémenceau, S.; Granat, O.; Marsault, C.; Baulac, M. Developmental abnormalities of the medial temporal lobe in patients with temporal lobe epilepsy. Am. J. Neuroradiol. 1995, 16, 617–626. [Google Scholar] [PubMed]
- Barsi, P.; Kenéz, J.; Solymosi, D.; Kulin, Á.; Halasz, P.; Rásonyi, G.; Janszky, J.; Kalóczkai, A.; Barcs, G.; Neuwirth, M.; et al. Hippocampal malrotation with normal corpus callosum: A new entity? Neuroradiology 2000, 42, 339–345. [Google Scholar] [CrossRef]
- Bernasconi, N.; Kinay, D.; Andermann, F.; Antel, S. Analysis of shape and positioning of the hippocampal formation: An MRI study in patients with partial epilepsy and healthy controls. Brain 2005, 128, 2442–2452. [Google Scholar] [CrossRef]
- Bajic, D.; Wang, C.; Kumlien, E.; Mattsson, P.; Lundberg, S.; Eeg-Olofsson, O.; Raininko, R. Incomplete inversion of the hippocampus—A common developmental anomaly. Eur. Radiol. 2007, 18, 138–142. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.-H.; Vaughan, D.N.; Perchyonok, Y.; Fitt, G.J.; Scheffer, I.E.; Berkovic, S.F.; Jackson, G.D. Hippocampal malrotation is an anatomic variant and has no clinical significance in MRI-negative temporal lobe epilepsy. Epilepsia 2016, 57, 1719–1728. [Google Scholar] [CrossRef] [PubMed]
- Mutti, C.; Riccò, M.; Bartolini, Y.; Bernabè, G.; Trippi, I.; Melpignano, A.; Ciliento, R.; Zinno, L.; Florindo, I.; Sasso, E.; et al. Incomplete hippocampal inversion and epilepsy: A systematic review and meta-analysis. Epilepsia 2021, 62, 383–396. [Google Scholar] [CrossRef] [PubMed]
- Gamss, R.; Slasky, S.; Bello, J.A.; Miller, T.S.; Shinnar, S. Prevalence of hippocampal malrotation in a population without seizures: Fig 1. Am. J. Neuroradiol. 2009, 30, 1571–1573. [Google Scholar] [CrossRef]
- Caciagli, L.; Wandschneider, B.; Xiao, F.; Vollmar, C.; Centeno, M.; Vos, S.B.; Trimmel, K.; Sidhu, M.K.; Thompson, P.J.; Winston, G.P.; et al. Abnormal hippocampal structure and function in juvenile myoclonic epilepsy and unaffected siblings. Brain 2019, 142, 2670–2687. [Google Scholar] [CrossRef]
- Bajic, D.; Kumlien, E.; Mattsson, P.; Lundberg, S.; Wang, C.; Raininko, R. Incomplete hippocampal inversion—Is there a relation to epilepsy? Eur. Radiol. 2009, 19, 2544–2550. [Google Scholar] [CrossRef]
- Dericioglu, N.; Oguz, K.K.; Soylemezoglu, F.; Akalan, N.; Saygi, S. Resective surgery is possible in patients with temporal lobe epilepsy due to bilateral isolated hippocampal malformation. Clin. Neurol. Neurosurg. 2009, 111, 554–557. [Google Scholar] [CrossRef]
- Sato, N.; Hatakeyama, S.; Shimizu, N.; Hikima, A.; Aoki, J.; Endo, K. MR evaluation of the hippocampus in patients with congenital malformations of the brain. Am. J. Neuroradiol. 2001, 22, 389–393. [Google Scholar] [PubMed]
- Yeghiazaryan, N.S.; Morana, G.; Veggiotti, P.; Savino, G.; Minetti, C.; Rossi, A.; Striano, P.; Giordano, L. Temporal lobe epilepsy and hippocampal malrotation: Is there a causal association? Epilepsy Behav. 2010, 18, 502–504. [Google Scholar] [CrossRef]
- Matsufuji, M.; Utsunomiya, H.; Inoue, T.; Yasumoto, S.; Takashima, S.; Mitsudome, A. Magnetic resonance imaging volumetry and clinical analysis of epilepsy patients with unilateral hippocampal abnormality. Pediatr. Int. 2011, 54, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Acay, M.B.; Koken, R.; Unlu, E.; Kacar, E.; Balcik, C.; Balçık, Ç. Evaluation of hippocampal infolding angle and incomplete hippocampal inversion in pediatric patients with epilepsy and febrile seizures. Diagn. Interv. Radiol. 2017, 23, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Bhoopathy, R.M.; Arthy, B.; Vignesh, S.S.; Srinivasan, A.V. Prevalence and clinical characteristics of malformations of cortical development and incomplete hippocampal inversion with medically intractable seizures in Chennai—A prospective study. Neurol. India 2019, 67, 442–447. [Google Scholar] [CrossRef]
- Voets, N.L.; Bernhardt, B.C.; Kim, H.; Yoon, U.; Bernasconi, N. Increased temporolimbic cortical folding complexity in temporal lobe epilepsy. Neurology 2010, 76, 138–144. [Google Scholar] [CrossRef]
- Stiers, P.; Fonteyne, A.; Wouters, H.; D’Agostino, E.; Sunaert, S.; Lagae, L. Hippocampal malrotation in pediatric patients with epilepsy associated with complex prefrontal dysfunction. Epilepsia 2010, 51, 546–555. [Google Scholar] [CrossRef] [PubMed]
- Cury, C.; Toro, R.; Cohen, F.; Fischer, C.; Mhaya, A.; Samper-González, J.; Hasboun, D.; Mangin, J.-F.; Banaschewski, T.; Bokde, A.L.W.; et al. Incomplete hippocampal inversion: A comprehensive MRI study of over 2000 subjects. Front. Neuroanat. 2015, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Leach, J.L.; Awwad, R.; Greiner, H.M.; Vannest, J.J.; Miles, L.; Mangano, F.T. Mesial temporal lobe morphology in intractable pediatric epilepsy: So-called hippocampal malrotation, associated findings, and relevance to presurgical assessment. J. Neurosurgery Pediatr. 2016, 17, 683–693. [Google Scholar] [CrossRef]
- Depondt, C.; Van Paesschen, W.; Matthijs, G.; Legius, E.; Martens, K.; Demaerel, P.; Wilms, G. Familial temporal lobe epilepsy with febrile seizures. Neurology 2002, 58, 1429–1433. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.; Bello, J.A.; Shinnar, S.; Hesdorffer, D.C.; Lewis, D.V.; MacFall, J.; Shinnar, R.C.; Gomes, W.; Litherland, C.; Xu, Y.; et al. Hippocampal malrotation is associated with prolonged febrile seizures: Results of the FEBSTAT study. Am. J. Roentgenol. 2015, 205, 1068–1074. [Google Scholar] [CrossRef]
- Kobayashi, E.; Facchin, D.; Steiner, C.E.; Leone, A.A.A.; Campos, N.L.V.; Cendes, F.; Lopes-Cendes, I. Mesial temporal lobe abnormalities in a family with 15q26qter trisomy. Arch. Neurol. 2002, 59, 1476–1479. [Google Scholar] [CrossRef]
- Pramparo, T.; De Gregori, M.; Gimelli, S.; Ciccone, R.; Frondizi, D.; Liehr, T.; Pellacani, S.; Masi, G.; Brovedani, P.; Zuffardi, O.; et al. A 7 Mb duplication at 22q13 in a girl with bipolar disorder and hippocampal malformation. Am. J. Med Genet. Part A 2008, 146A, 1754–1760. [Google Scholar] [CrossRef]
- Andrade, D.M.; Krings, T.; Chow, E.W.C.; Kiehl, T.-R.; Bassett, A.S. Hippocampal malrotation is associated with chromosome 22q11.2 microdeletion. Can. J. Neurol. Sci./J. Can. des Sci. Neurol. 2013, 40, 652–656. [Google Scholar] [CrossRef]
- Sisodiya, S.M.; Ragge, N.K.; Cavalleri, G.L.; Hever, A.; Lorenz, B.; Schneider, A.; Williamson, K.A.; Stevens, J.M.; Free, S.L.; Thompson, P.J.; et al. Role of SOX2 mutations in human hippocampal malformations and epilepsy. Epilepsia 2006, 47, 534–542. [Google Scholar] [CrossRef]
- Zhao, Y.; Sheng, H.Z.; Amini, R.; Grinberg, A.; Lee, E.; Huang, S.; Taira, M.; Westphal, H. Control of hippocampal morphogenesis and neuronal differentiation by the LIM homeobox gene Lhx5. Science 1999, 284, 1155–1158. [Google Scholar] [CrossRef]
- Lee, S.M.; Tole, S.; Grove, E.; McMahon, A.P. A local Wnt-3a signal is required for development of the mammalian hippocampus. Development 2000, 127, 457–467. [Google Scholar] [PubMed]
- Tole, S.; Goudreau, G.; Assimacopoulos, S.; Grove, E.A. Emx2 is required for growth of the hippocampus but not for hippocampal field specification. J. Neurosci. 2000, 20, 2618–2625. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Studies | Cohort | n | left | Right | Bilateral |
|---|---|---|---|---|---|
| Baulac et al., 1998 [3] | Epilepsy | 19 | 9 | 5 | 5 |
| Barsi et al., 2000 [17] | Epilepsy | 32 | 22 | 6 | 4 |
| Thom et al., 2002 [4] | Epilepsy | 1 | 0 | 0 | 1 |
| Sen et al., 2005 [6] | Epilepsy | 2 | 0 | 1 | 1 |
| Bajic et al., 2007 [19] | Controls | 19 | 13 | 0 | 6 |
| Bajic et al., 2009 [24] | Epilepsy | 60 | 40 | 4 | 16 |
| Bajic et al., 2009 [24] | Controls | 28 | 20 | 0 | 8 |
| Dericioglu et al., 2009 [25] | Epilepsy | 1 | 0 | 0 | 1 |
| Yeghiazaryan et al., 2010 [27] | Epilepsy | 2 | 2 | 0 | 0 |
| Matsufuji et al., 2012 [28] | Epilepsy | 5 | 2 | 3 | 0 |
| Tsai et al., 2016 [20] | Lesion-negative TLE (n = 155) and Healthy Controls (n = 103) | 50 | 26 | 8 | 21 |
| Caciagli et al., 2019 [23] | JME (n = 37), sibling (n = 16) and controls (n = 20) | 30 | 22 | 3 | 5 |
| Labate, Sammarra et al., 2020 [5] | MTLE (n = 187) and controls (n = 93) | 38 | 30 | 6 | 2 |
| Total | 287 | 186 (64.8%) | 36 (12.5%) | 70 (24.4%) |
| Studies | Subjects | Seizure Onset Side | Findings of HIMAL | Comments |
|---|---|---|---|---|
| Bernasconi et al., 2005 [18] | 13/30 TLE patients | The clinical decision from multiple types of investigations | 85% bilateral or contralateral versus 15% ipsilateral (p = 0.01) | HIMAL was not related to the side of the EEG focus |
| Bajic et al., 2009 [24] | 14/57 TLE patients (11 left, 2 right, and 1 bilateral) | Interictal EEG only | 1. 8 of 11 patients with left HIMAL had EEG focus on the left and 2 with bilateral EEG focus. 2. 2 of 2 patient with right HIMAL had left EEG focus 3. 2 patients (1 bilateral HIMAL, 1 left HIMAL) had undetermined EEG side | This study concluded that the laterality of EEG onset did not correlate with HIMAL. |
| Barsi et al., 2000 [17] | 32 epilepsy patients with HIMAL | Interictal EEG only | 8/32 (25%) contralateral 11/32 (34%) multifocal or bilateral 13/32 (45%) ipsilateral | Same as above |
| Thom et al., 2002 [4] | 1 TLE patient with left HIMAL | Clinical semiology suggested left-sided onset (ictal right head deviation) | Ipsilateral (n = 1) | Supports that HIMAL is epileptogenic but potential publication bias |
| Sen et al., 2005 [6] | 2 epilepsy patients (1 right, 1 bilateral HIMAL) | Left-sided onset based on Todd’s paralysis and interictal EEG, 1 non-localizing (bilateral, R > L HIMAL) | Ipsilateral in one patient (n = 1) | Supports that HIMAL is epileptogenic but potential publication bias |
| Yeghiazaryan et al., 2010 [27] | 2 TLE patients with left HIMAL | VEM and left ATL, both became seizure-free | 2 ipsilateral | Supports that HIMAL is epileptogenic but potential publication bias |
| Matsufuji et al., 2012 [28] | 5 HIMAL (2L, 3R) cases (3 BECTS, 1 FLE, 1 undetermined) | Interictal EEG only | 4 Ipsilateral, 1 uncertain (Diffuse spike and waves) | Supports that HIMAL is epileptogenic but potential publication bias |
| Tsai et al., 2016 [20] | 25 TLE patients with HIMAL from 155 lesion-negative TLE patients | Clinical semiology, electroencephalography, and VEM | 9 ipsilateral all on left side, 5 contralateral (2 right HIMAL and left-sided seizure onset, 3 left HIMAL and right-sided seizure onset), 11 bilateral HIMAL (9 left-sided seizure onset and 2 right-sided seizure onset) | Exact binomial test not significant, which suggests that the occurrence of HIMAL and seizure onset side did not differ from chance. HIMAL is not ictogenesis in lesion negative TLE and should not influence the surgical decision. |
| Caciagli et al., 2019 [23] | 37 JME, 16 unaffected siblings, 20 controls | Generalized | 22 left, 3 right, and 5 bilateral | HIMAL is not likely to be epileptogenic in JME. |
| Labate et al., 2020 [5] | 187 MTLE patients and 93 controls | Interictal EEG only | 11/19 patient with left HIMAL has left-sided EEG focus 3/4 patients with right HIMAL, EEG focus were on the left side 3/6 bilateral HIMAL, EEG focus on the left side | Concordance EEG focus with the side of HIMAL was presented in slightly more than half (52.2%) of the MTLE patients |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, T.-Y.; Ho, C.-R.; Lin, C.-H.; Lu, Y.-T.; Lin, W.-C.; Tsai, M.-H. Hippocampal Malrotation: A Genetic Developmental Anomaly Related to Epilepsy? Brain Sci. 2021, 11, 463. https://doi.org/10.3390/brainsci11040463
Fu T-Y, Ho C-R, Lin C-H, Lu Y-T, Lin W-C, Tsai M-H. Hippocampal Malrotation: A Genetic Developmental Anomaly Related to Epilepsy? Brain Sciences. 2021; 11(4):463. https://doi.org/10.3390/brainsci11040463
Chicago/Turabian StyleFu, Ting-Ying, Chen-Rui Ho, Chih-Hsiang Lin, Yan-Ting Lu, Wei-Che Lin, and Meng-Han Tsai. 2021. "Hippocampal Malrotation: A Genetic Developmental Anomaly Related to Epilepsy?" Brain Sciences 11, no. 4: 463. https://doi.org/10.3390/brainsci11040463
APA StyleFu, T.-Y., Ho, C.-R., Lin, C.-H., Lu, Y.-T., Lin, W.-C., & Tsai, M.-H. (2021). Hippocampal Malrotation: A Genetic Developmental Anomaly Related to Epilepsy? Brain Sciences, 11(4), 463. https://doi.org/10.3390/brainsci11040463