
Paediatricians’ Views on Pain in Children with Profound Intellectual and Multiple Disabilities



Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Population
2.3. Survey Development and Content
2.4. Data Collection
2.5. Data Analysis
3. Results
3.1. Survey Population
3.2. Survey Responses
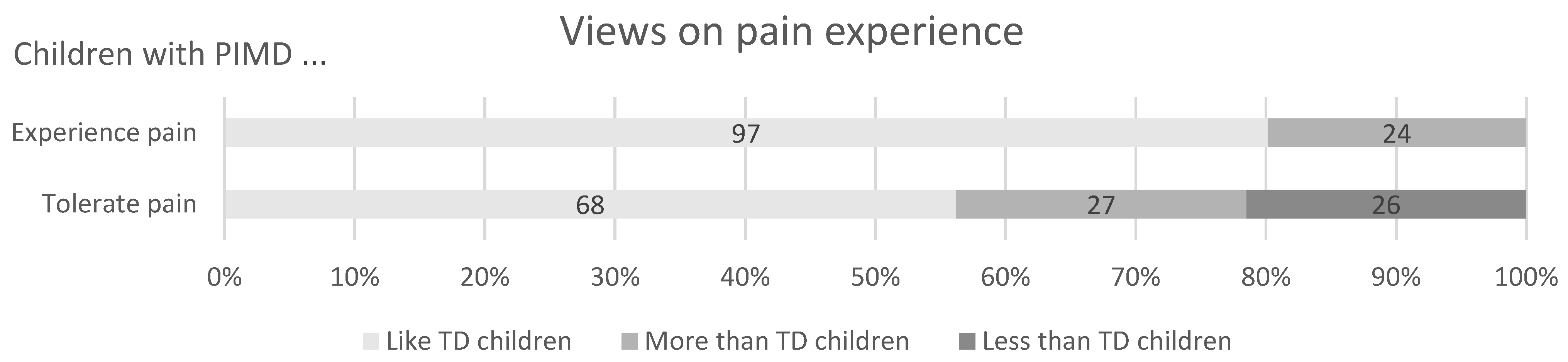
3.2.1. The Experience of Pain in Children with PIMD
3.2.2. Pain Assessment
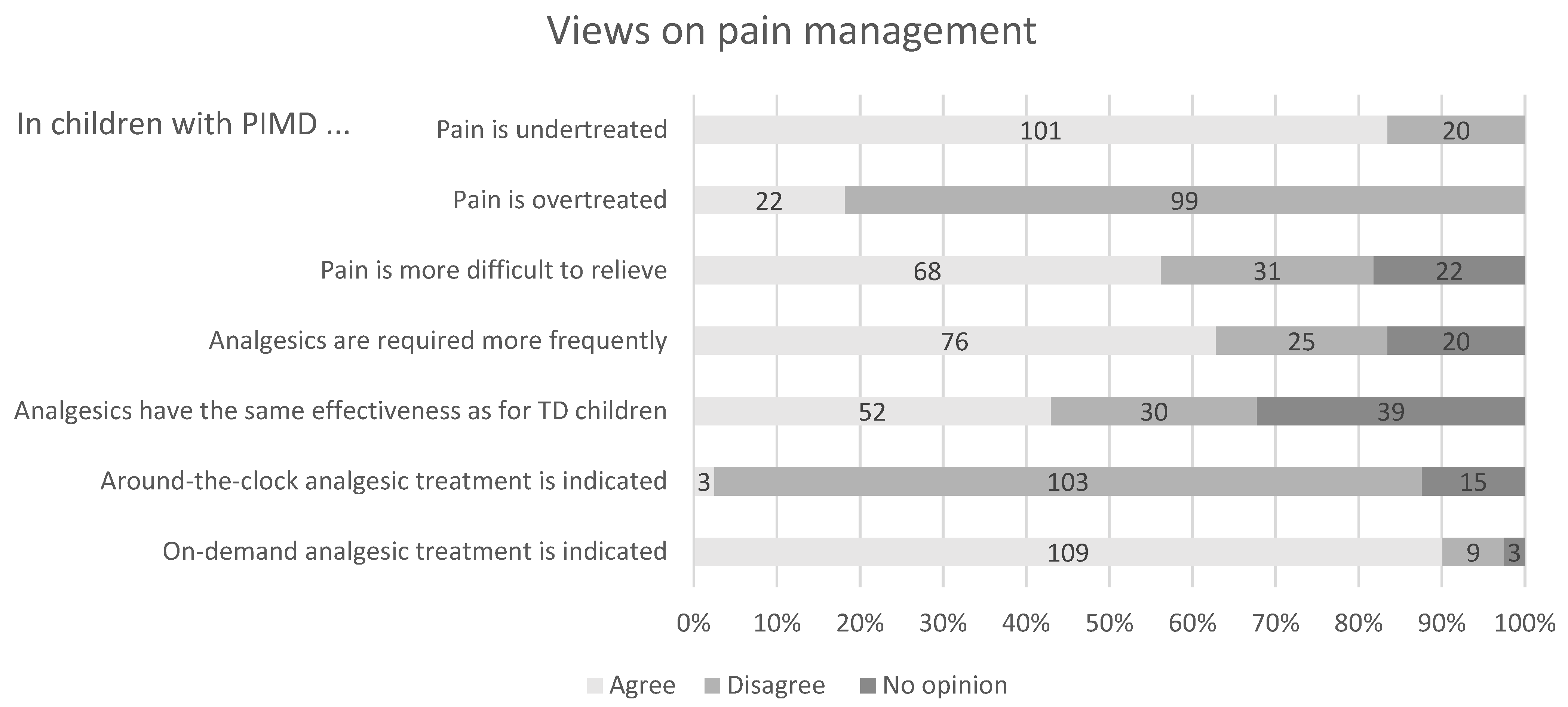
3.2.3. Pain Management
3.2.4. Barriers to the Appropriate Medical Care of Children with PIMD
3.2.5. Barriers to Treating Pain with Medication in Children with PIMD
3.2.6. Association Analyses of Non-Consensual Responses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arvio, M.; Sillanpaa, M. Prevalence, aetiology and comorbidity of severe and profound intellectual disability in Finland. J. Intellect. Disabil. Res. 2003, 47, 108–112. [Google Scholar] [CrossRef]
- Hogg, J.; Juhlberg, K.; Lambe, L. Policy, service pathways and mortality: A 10-year longitudinal study of people with profound intellectual and multiple disabilities. J. Intellect. Disabil. Res. 2007, 51, 366–376. [Google Scholar] [CrossRef]
- Bellamy, G.; Croot, L.; Bush, A.; Berry, H.; Smith, A. A study to define: Profound and multiple learning disabilities (PMLD). J. Intellect. Disabil. 2010, 14, 221–235. [Google Scholar] [CrossRef]
- Malviya, S.; Voepel-Lewis, T.; Merkel, S.; Tait, A.R. Difficult pain assessment and lack of clinician knowledge are ongoing barriers to effective pain management in children with cognitive impairment. Acute Pain 2005, 7, 27–32. [Google Scholar] [CrossRef]
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, F.J.; Mogil, J.S.; Ringkamp, M.; Sluka, K.A.; et al. The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef]
- Lumley, M.A.; Cohen, J.L.; Borszcz, G.S.; Cano, A.; Radcliffe, A.M.; Porter, L.S.; Schubiner, H.; Keefe, F.J. Pain and emotion: A biopsychosocial review of recent research. J. Clin. Psychol. 2011, 67, 942–968. [Google Scholar] [CrossRef] [PubMed]
- Samuel, J.; Pritchard, M. The ignored minority: Meeting the needs of people with profound learning disability. Tizard Learn. Disabil. Rev. 2001, 6, 34–44. [Google Scholar] [CrossRef]
- Van der Putten, A.; Vlaskamp, C. Pain assessment in people with profound intellectual and multiple disabilities; a pilot study into the use of the Pain Behaviour Checklist in everyday practice. Res. Dev. Disabil. 2011, 32, 1677–1684. [Google Scholar] [CrossRef]
- Houx, L.; Pons, C.; Saudreau, H.; Dubois, A.; Creusat, M.; Le Moine, P.; Rémy-Néris, O.; Ropars, J.; LeReste, J.Y.; Brochard, S. No pain, no gain? Children with cerebral palsy and their experience with physiotherapy. Ann. Phys. Rehabil. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Warlow, T.A.; Hain, R.D.W. ‘Total Pain’ in Children with Severe Neurological Impairment. Children 2018, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Breau, L.M.; Camfield, C.S.; McGrath, P.J.; Finley, G.A. The incidence of pain in children with severe cognitive impairments. Arch. Pediatrics Adolesc. Med. 2003, 157, 1219–1226. [Google Scholar] [CrossRef] [PubMed]
- Westbom, L.; Rimstedt, A.; Nordmark, E. Assessments of pain in children and adolescents with cerebral palsy: A retrospective population-based registry study. Dev. Med. Child Neurol. 2017, 59, 858–863. [Google Scholar] [CrossRef] [PubMed]
- Tedroff, K.; Gyllensvärd, M.; Löwing, K. Prevalence, identification, and interference of pain in young children with cerebral palsy: A population-based study. Disabil. Rehabil. 2019, 10, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Carter, B.; McArthur, E.; Cunliffe, M. Dealing with uncertainty: Parental assessment of pain in their children with profound special needs. J. Adv. Nurs. 2002, 38, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Valkenburg, A.J.; van der Kreeft, S.M.; de Leeuw, T.G.; Stolker, R.J.; Tibboel, D.; van Dijk, M. Pain management in intellectually disabled children: A survey of perceptions and current practices among Dutch anesthesiologists. Paediatr. Anaesth. 2012, 22, 682–689. [Google Scholar] [CrossRef] [PubMed]
- Kankkunen, P.; Janis, P.; Vehvilainen-Julkunen, K. Pain assessment among non-communicating intellectually disabled people described by nursing staff. Open Nurs. J. 2010, 4, 55–59. [Google Scholar] [CrossRef]
- Federal Act on Research involving Human Beings. Available online: https://www.admin.ch/opc/en/classified-compilation/20061313/index.html (accessed on 1 December 2020).
- Hsu, C.; Sandford, B. The Delphi technique: Making sense of consensus—Practical assessment, research & evaluation. Pract. Assess. Res. Eval. 2007, 12, 10. [Google Scholar]
- Malviya, S.; Voepel-Lewis, T.; Burke, C.; Merkel, S.; Tait, A.R. The revised FLACC observational pain tool: Improved reliability and validity for pain assessment in children with cognitive impairment. Paediatr. Anaesth. 2006, 16, 258–265. [Google Scholar] [CrossRef]
- Collignon, P.; Giusiano, B. Validation of a pain evaluation scale for patients with severe cerebral palsy. Eur. J. Pain 2001, 5, 433–442. [Google Scholar] [CrossRef]
- Barney, C.C.; Andersen, R.D.; Defrin, R.; Genik, L.M.; McGuire, B.E.; Symons, F.J. Challenges in pain assessment and management among individuals with intellectual and developmental disabilities. Pain Rep. 2020, 5, e821. [Google Scholar] [CrossRef]
- Biersdorff, K.K. Incidence of significantly altered pain experience among individuals with developmental disabilities. Am. J. Ment. Retard. Ajmr. 1994, 98, 619–631. [Google Scholar]
- De Araújo Vitor, C.A.; Ortega, A.D.O.L.; Ferreira, A.C.F.M.; da Silva, C.A.; Gallottini, M.H.C.; Santos, M.T.B.R. Pressure pain threshold of masticatory muscles in children and adolescents with and without intellectual disability: A pilot study. Eur. Arch. Paediatr. Dent. 2021, 1–7. [Google Scholar] [CrossRef]
- Blankenburg, M.; Junker, J.; Hirschfeld, G.; Michel, E.; Aksu, F.; Wager, J.; Zernikow, B. Quantitative sensory testing profiles in children, adolescents and young adults (6–20 years) with cerebral palsy: Hints for a neuropathic genesis of pain syndromes. Eur. J. Paediatr. Neurol. 2018, 22, 470–481. [Google Scholar] [CrossRef] [PubMed]
- Riquelme, I.; Padrón, I.; Cifre, I.; González-Roldán, A.M.; Montoya, P. Differences in somatosensory processing due to dominant hemispheric motor impairment in cerebral palsy. BMC Neurosci. 2014, 15, 10. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal Dutta, R.; Salamon, K.S. Risk and Resilience Factors Impacting Treatment Compliance and Functional Impairment among Adolescents Participating in an Outpatient Interdisciplinary Pediatric Chronic Pain Management Program. Children 2020, 7, 247. [Google Scholar] [CrossRef]
- Pascolo, P.; Peri, F.; Montico, M.; Funaro, M.; Parrino, R.; Vanadia, F.; Rusalen, F.; Vecchiato, L.; Benini, F.; Congedi, S.; et al. Needle-related pain and distress management during needle-related procedures in children with and without intellectual disability. Eur. J. Pediatrics 2018, 177, 1753–1760. [Google Scholar] [CrossRef] [PubMed]
- Bembich, S.; Morabito, G.; Simeon, V.; Strajn, T.; Rutigliano, R.; Di Rocco, P.; Cont, G.; Risso, F.M.; Peri, F.; Barbi, E. Venipuncture activates the cerebral cortex in children with intellectual disability. Arch. Dis. Child. 2021, 106, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Craig, K.D. Social communication model of pain. Pain 2015, 156, 1198–1199. [Google Scholar] [CrossRef]
- Hunt, A.; Mastroyannopoulou, K.; Goldman, A.; Seers, K. Not knowing--the problem of pain in children with severe neurological impairment. Int. J. Nurs. Stud. 2003, 40, 171–183. [Google Scholar] [CrossRef]
- Barbi, E.; Massaro, M.; Badina, L. Measuring pain in children with cognitive impairment and cerebral palsy: A multiregional survey in the use of specific pain scales. Pediatr. Emerg. Care 2011, 27, 1216. [Google Scholar] [CrossRef]
- Hauer, J.; Houtrow, A.J. Pain Assessment and Treatment in Children with Significant Impairment of the Central Nervous System. Pediatrics 2017, 139, e20171002. [Google Scholar] [CrossRef]
- Hauer, J. Improving comfort in children with severe neurological impairment. Prog. Palliat. Care 2012, 20, 349–356. [Google Scholar] [CrossRef]
- Massaro, M.; Pastore, S.; Ventura, A.; Barbi, E. Pain in cognitively impaired children: A focus for general pediatricians. Eur. J. Pediatr. 2013, 172, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Sheppard, M.E.; Vitalone-Raccaro, N. How physicians support children with disabilities and their families: Roles, responsibilities and collaborative partnerships. Disabil. Health J. 2016, 9, 692–704. [Google Scholar] [CrossRef]
- Sneed, R.C.; May, W.L.; Stencel, C.S. Training of pediatricians in care of physical disabilities in children with special health needs: Results of a two-state survey of practicing pediatricians and national resident training programs. Pediatrics 2000, 105, 554–561. [Google Scholar] [CrossRef]
- Wilkinson, J.; Dreyfus, D.; Cerreto, M.; Bokhour, B. “Sometimes I feel overwhelmed”: Educational needs of family physicians caring for people with intellectual disability. Intellect. Dev. Disabil. 2012, 50, 243–250. [Google Scholar] [CrossRef]
- Clarke, Z.J.; Thompson, A.R.; Buchan, L.; Combes, H. Parents’ experiences of pain and discomfort in people with learning disabilities. Br. J. Learn. Disabil. 2008, 36, 84–90. [Google Scholar] [CrossRef]
- Principal Relevant Objectives and a Framework for Integrative Learning and Education in Switzerland (PROFILES). Available online: https://www.profilesmed.ch/ssps/1-general-complaints-and-symptoms?s=pain (accessed on 3 March 2021).
- Hauer, J.M.; Solodiuk, J.C. Gabapentin for management of recurrent pain in 22 nonverbal children with severe neurological impairment: A retrospective analysis. J. Palliat. Med. 2015, 18, 453–456. [Google Scholar] [CrossRef]
- Friedrichsdorf, S.J.; Kang, T.I. The management of pain in children with life-limiting illnesses. Pediatric Clin. N. Am. 2007, 54, 645–672. [Google Scholar] [CrossRef]
- Swiss Medical Federation Medical Statistics. Available online: https://aerztestatistik.myfmh2.fmh.ch/ (accessed on 3 March 2021).
- Carter, B.; Simons, J.; Bray, L.; Arnott, J. Navigating Uncertainty: Health Professionals’ Knowledge, Skill, and Confidence in Assessing and Managing Pain in Children with Profound Cognitive Impairment. Pain Res. Manag. 2016, 2016, 8617182. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Demographic and Professional Characteristics n (%) | ||||||
|---|---|---|---|---|---|---|
| Gender | Male 39 (32.2%) | Female 82 (67.8%) | ||||
| Age range (years) | 25–34 | 35–44 | 45–54 | >55 | ||
| 39 (32.2%) | 36 (29.8%) | 31 (25.9%) | 15 (12.4%) | |||
| Country of origin | Switzerland | Europe | Other | |||
| 89 (73.5%) | 29 (23.9%) | 5 (4.1%) | ||||
| Country of study | Switzerland | Europe | Other | |||
| 96 (79.3%) | 22 (18.2%) | 4 (3.3%) | ||||
| Current activity | General paediatricians | Neuropaediatricians | Other paediatric specialists | |||
| 87 (71.9%) | 12 (9.9%) | 22 (18.2%) | ||||
| Experience in paediatrics (years) | 0–5 | 6–10 | 11–20 | >20 | ||
| 33 (27.3%) | 17 (14%) | 44 (36.4%) | 27 (22.3%) | |||
| Current activity (years) | 0–5 | 6–10 | 11–20 | >20 | ||
| 52 (43%) | 30 (24.8%) | 28 (23.1%) | 11 (9.1%) | |||
| Place of work | Hospital | Community | ||||
| 81 (66.9%) | 40 (33.1%) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petigas, L.; Newman, C.J. Paediatricians’ Views on Pain in Children with Profound Intellectual and Multiple Disabilities. Brain Sci. 2021, 11, 408. https://doi.org/10.3390/brainsci11030408
Petigas L, Newman CJ. Paediatricians’ Views on Pain in Children with Profound Intellectual and Multiple Disabilities. Brain Sciences. 2021; 11(3):408. https://doi.org/10.3390/brainsci11030408
Chicago/Turabian StylePetigas, Lucie, and Christopher J. Newman. 2021. "Paediatricians’ Views on Pain in Children with Profound Intellectual and Multiple Disabilities" Brain Sciences 11, no. 3: 408. https://doi.org/10.3390/brainsci11030408
APA StylePetigas, L., & Newman, C. J. (2021). Paediatricians’ Views on Pain in Children with Profound Intellectual and Multiple Disabilities. Brain Sciences, 11(3), 408. https://doi.org/10.3390/brainsci11030408