
Against the Resilience of High-Grade Gliomas: The Immunotherapeutic Approach (Part I)



Abstract
1. Introduction
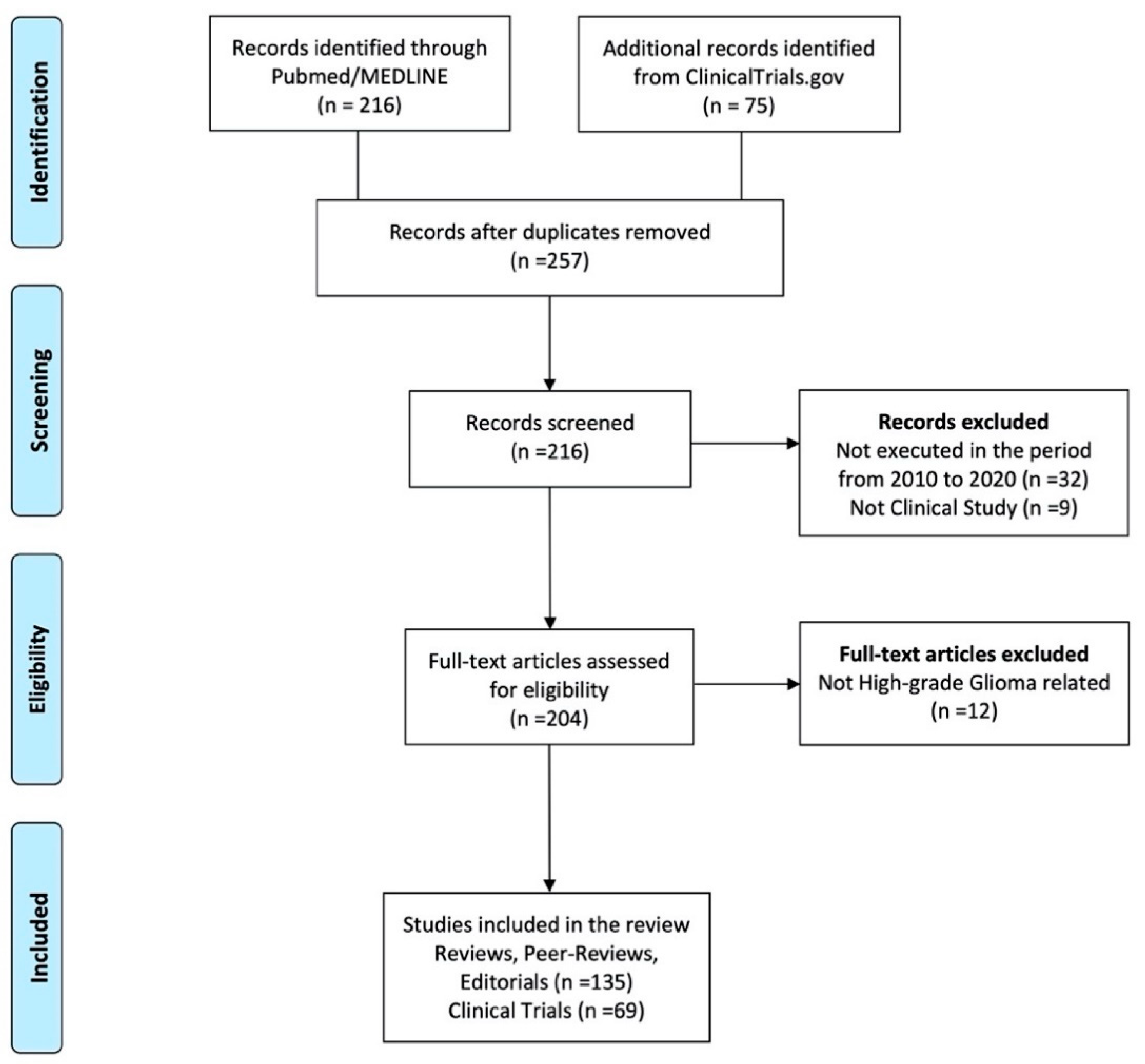
2. Materials and Methods
3. Results
3.1. Classification of Immunotherapies
3.2. Active Immunotherapies
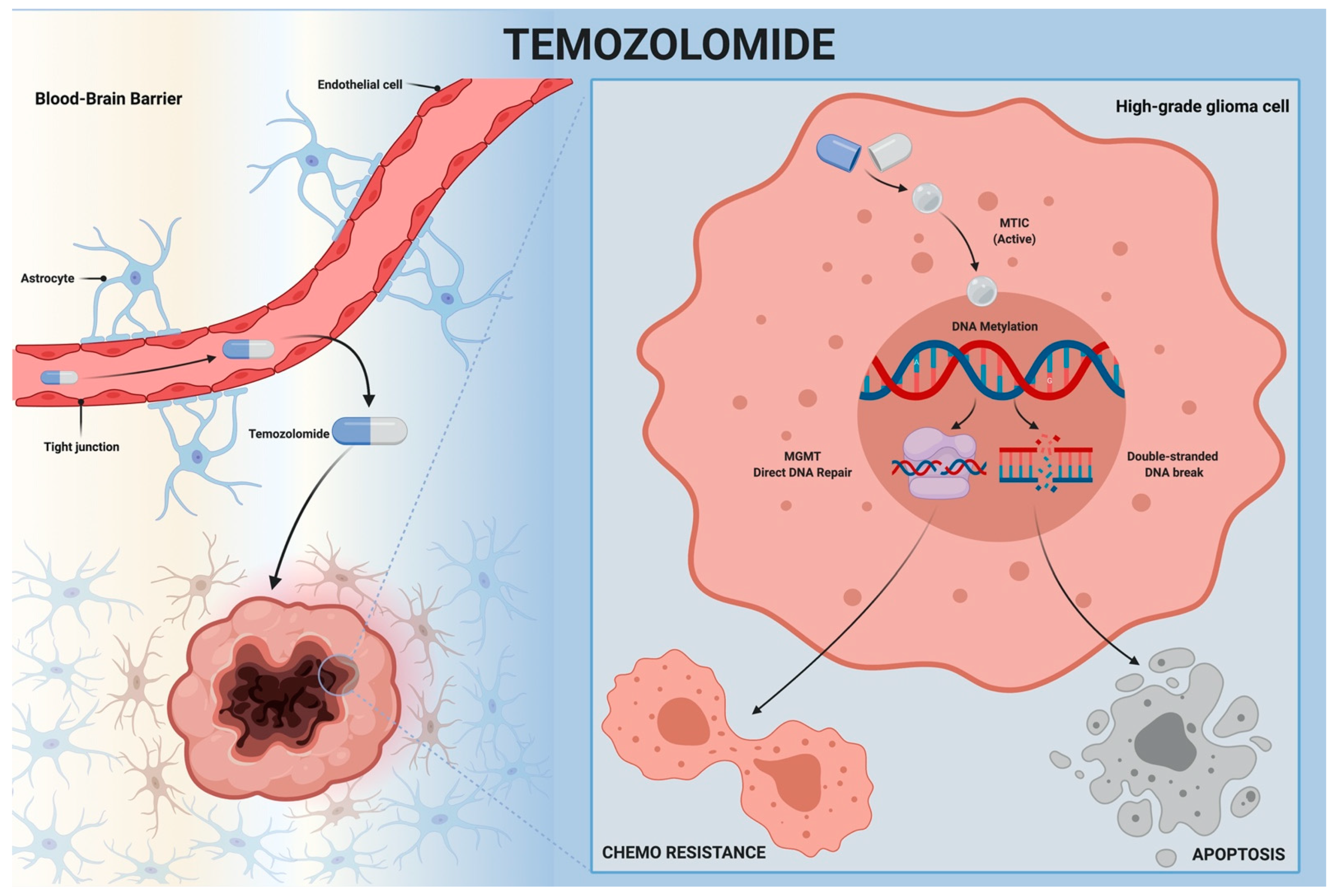
3.2.1. Alkylating Agents
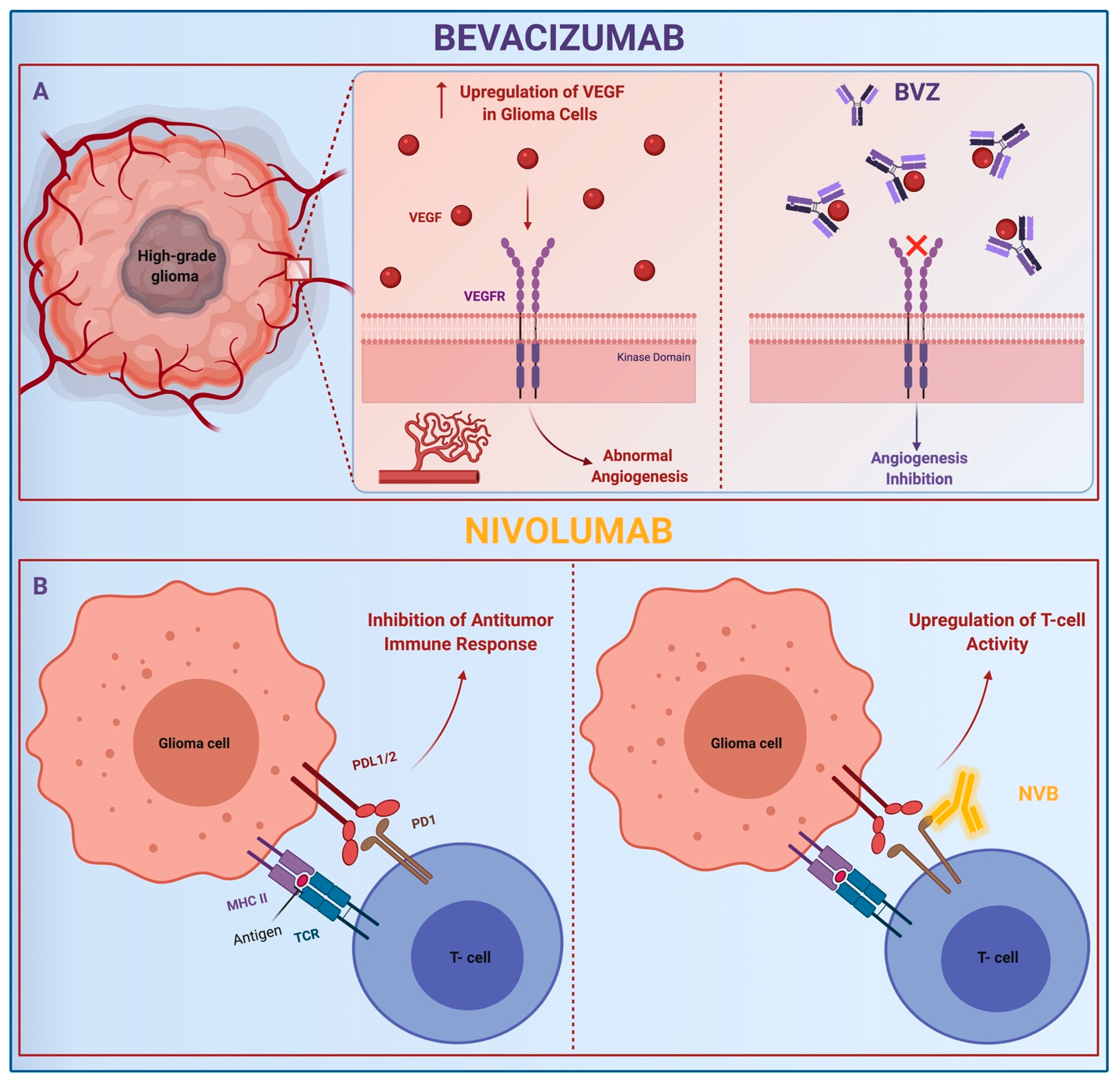
3.2.2. Monoclonal Antibodies
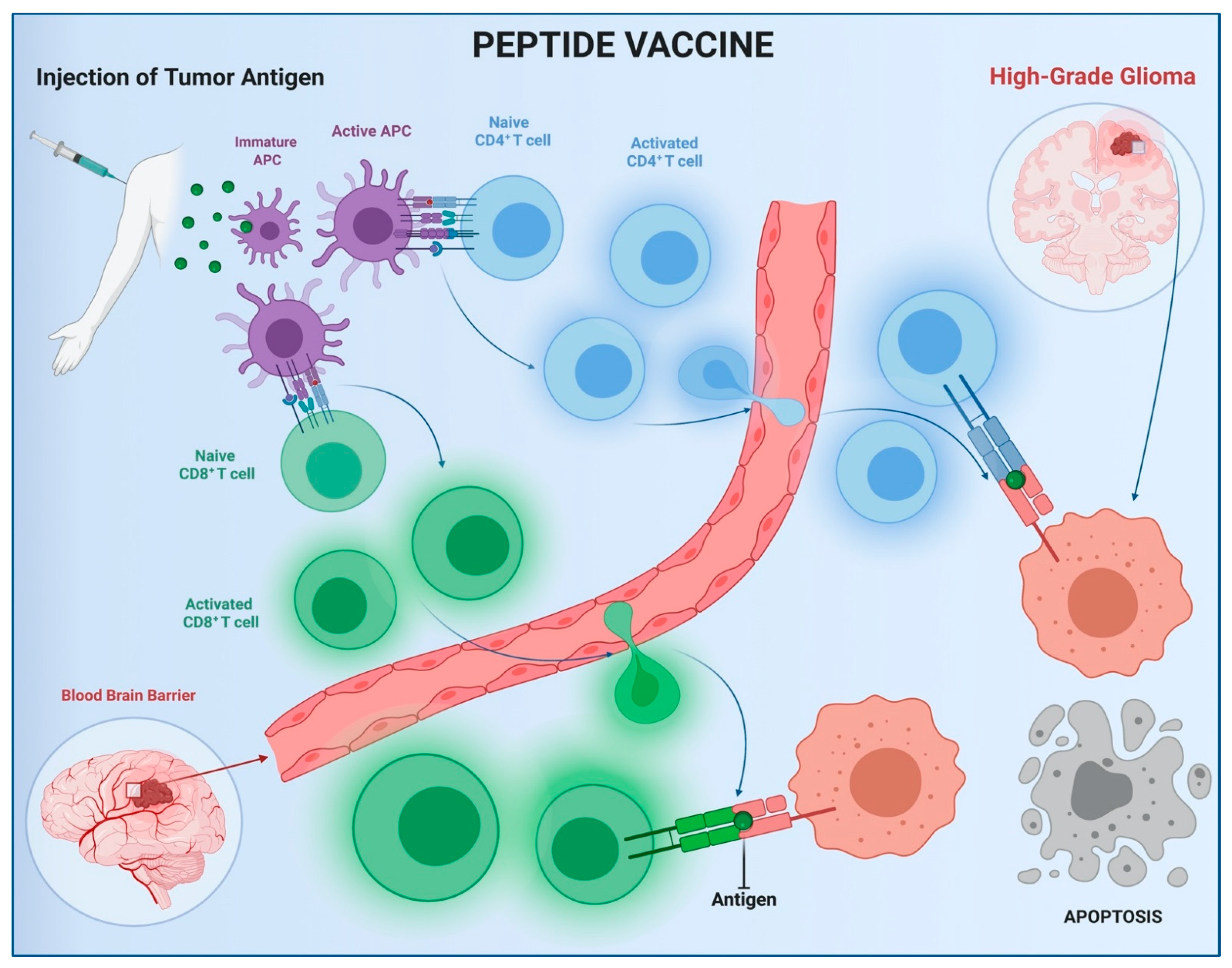
3.2.3. Vaccine
3.3. Adoptive Immunotherapies
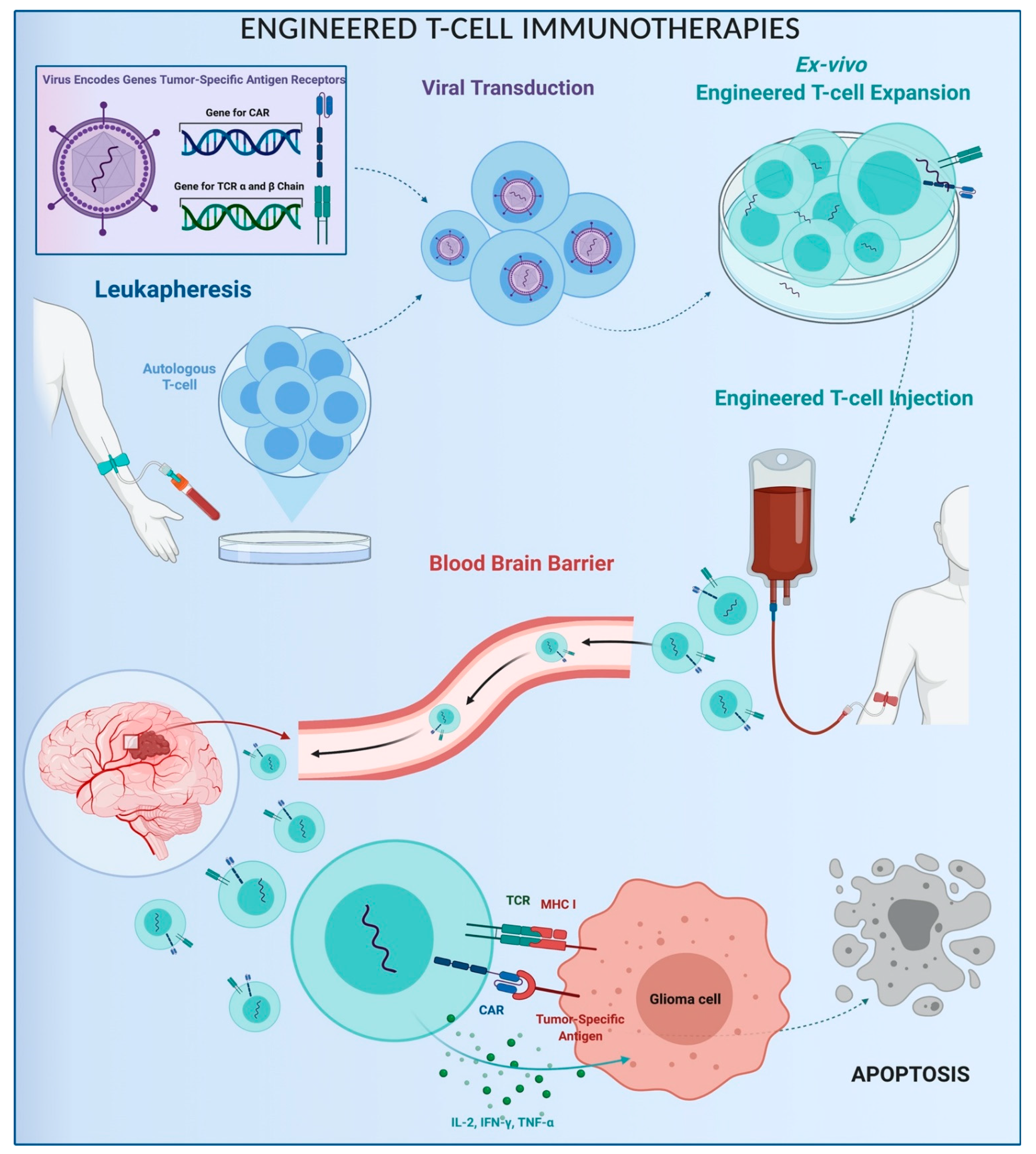
3.3.1. Engineered T Cells
3.3.2. NK Cells
3.3.3. NKT Cells and Hybrid Therapies
4. Discussion
Limitations and Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Ostrom, Q.T.; Gittleman, H.; Liao, P.; Rouse, C.; Chen, Y.; Dowling, J.; Wolinsky, Y.; Kruchko, C.; Barnholtz-Sloan, J. CBTRUS Statistical Report: Primary Brain and Central Nervous System Tumors Diagnosed in the United States in 2007–2011. Neuro-Oncology 2014, 16, iv1–iv63. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Steliarova-Foucher, E.; Lortet-Tieulent, J.; Rosso, S.; Coebergh, J.; Comber, H.; Forman, D.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries in 2012. Eur. J. Cancer 2013, 49, 1374–1403. [Google Scholar] [CrossRef] [PubMed]
- Soerjomataram, I.; Lortet-Tieulent, J.; Parkin, D.M.; Ferlay, J.; Mathers, C.; Forman, D.; Bray, F. Global burden of cancer in 2008: A systematic analysis of disability-adjusted life-years in 12 world regions. Lancet 2012, 380, 1840–1850. [Google Scholar] [CrossRef]
- Ladomersky, E.; Genet, M.; Zhai, L.; Gritsina, G.; Lauing, K.L.; Lulla, R.R.; Fangusaro, J.; Lenzen, A.; Kumthekar, P.; Raizer, J.J.; et al. Improving vaccine efficacy against malignant glioma. Onco Immunol. 2016, 5, e1196311. [Google Scholar] [CrossRef] [PubMed]
- Ostrom, Q.T.; Gittleman, H.; Stetson, L.; Virk, S.M.; Barnholtz-Sloan, J.S. Epidemiology of Gliomas. Cancer Treat. Res. 2014, 163, 1–14. [Google Scholar] [CrossRef]
- Stupp, R.; Hegi, M.E.; Mason, W.P.; Bent, M.J.V.D.; Taphoorn, M.J.B.; Janzer, R.C.; Ludwin, S.K.; Allgeier, A.; Fisher, B.; Belanger, K.; et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009, 10, 459–466. [Google Scholar] [CrossRef]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.B.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef]
- Johnson, D.R.; O’Neill, B.P. Glioblastoma survival in the United States before and during the temozolomide era. J. Neuro Oncol. 2012, 107, 359–364. [Google Scholar] [CrossRef]
- Eagan, R.T.; Scott, M. Evaluation of prognostic factors in chemotherapy of recurrent brain tumors. J. Clin. Oncol. 1983, 1, 38–44. [Google Scholar] [CrossRef]
- Wen, P.Y.; Kesari, S. Malignant Gliomas in Adults. N. Engl. J. Med. 2008, 359, 492–507. [Google Scholar] [CrossRef]
- Perry, J.R.; Laperriere, N.; O’Callaghan, C.J.; Brandes, A.A.; Menten, J.; Phillips, C.; Fay, M.; Nishikawa, R.; Cairncross, J.G.; Roa, W.; et al. Short-Course Radiation plus Temozolomide in Elderly Patients with Glioblastoma. N. Engl. J. Med. 2017, 376, 1027–1037. [Google Scholar] [CrossRef]
- Chen, R.; Smith-Cohn, M.; Cohen, A.L.; Colman, H. Glioma Subclassifications and Their Clinical Significance. Neurotherapeutics 2017, 14, 284–297. [Google Scholar] [CrossRef]
- Eckel-Passow, J.E.; Lachance, D.H.; Molinaro, A.M.; Walsh, K.M.; Decker, P.A.; Sicotte, H.; Pekmezci, M.; Rice, T.W.; Kosel, M.L.; Smirnov, I.V.; et al. Glioma Groups Based on 1p/19q, IDH, and TERT Promoter Mutations in Tumors. N. Engl. J. Med. 2015, 372, 2499–2508. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, K.; Kornblum, H.I. Molecular markers in glioma. J. Neuro-Oncol. 2017, 134, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.; Li, G.; Liu, H.; Zhao, Z.; Chai, R.; Liu, Y.; Jiang, H.; Zhai, Y.; Feng, Y.; Li, R.; et al. Molecular subtyping reveals immune alterations in IDH wild-type lower-grade diffuse glioma. J. Pathol. 2020, 251, 272–283. [Google Scholar] [CrossRef]
- Wesseling, P.; Capper, D. WHO 2016 Classification of gliomas. Neuropathol. Appl. Neurobiol. 2017, 44, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Reifenberger, G.; Von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef]
- Lucifero, A.G.; Luzzi, S.; Brambilla, I.; Guarracino, C.; Mosconi, M.; Foiadelli, T.; Savasta, S. Gene therapies for high-grade gliomas: From the bench to the bedside. Acta Biomed. 2020, 91, 32–50. [Google Scholar]
- Campanella, R.; Guarnaccia, L.; Cordiglieri, C.; Trombetta, E.; Caroli, M.; Carrabba, G.; La Verde, N.; Rampini, P.; Gaudino, C.; Costa, A.; et al. Tumor-Educated Platelets and Angiogenesis in Glioblastoma: Another Brick in the Wall for Novel Prognostic and Targetable Biomarkers, Changing the Vision from a Localized Tumor to a Systemic Pathology. Cells 2020, 9, 294. [Google Scholar] [CrossRef]
- Gieryng, A.; Pszczolkowska, D.; Walentynowicz, K.A.; Rajan, W.D.; Kaminska, B. Immune microenvironment of gliomas. Lab. Investig. 2017, 97, 498–518. [Google Scholar] [CrossRef]
- Wilcox, J.A.; Ramakrishna, R.; Magge, R. Immunotherapy in Glioblastoma. World Neurosurg. 2018, 116, 518–528. [Google Scholar] [CrossRef] [PubMed]
- Grabowski, M.M.; Sankey, E.W.; Ryan, K.J.; Chongsathidkiet, P.; Lorrey, S.J.; Wilkinson, D.S.; Fecci, P.E. Immune suppression in gliomas. J. Neuro Oncol. 2021, 151, 3–12. [Google Scholar] [CrossRef]
- Hanaei, S.; Afshari, K.; Hirbod-Mobarakeh, A.; Mohajer, B.; Dastmalchi, D.A.; Rezaei, N. Therapeutic efficacy of specific immunotherapy for glioma: A systematic review and meta-analysis. Rev. Neurosci. 2018, 29, 443–461. [Google Scholar] [CrossRef]
- Lucifero, A.G.; Luzzi, S.; Brambilla, I.; Trabatti, C.; Mosconi, M.; Savasta, S.; Foiadelli, T. Innovative therapies for malignant brain tumors: The road to a tailored cure. Acta Biomed. 2020, 91, 5–17. [Google Scholar]
- Dehcordi, S.R.; Ricci, A.; Di Vitantonio, H.; De Paulis, D.; Luzzi, S.; Palumbo, P.; Cinque, B.; Tempesta, D.; Coletti, G.; Cipolloni, G.; et al. Stemness Marker Detection in the Periphery of Glioblastoma and Ability of Glioblastoma to Generate Glioma Stem Cells: Clinical Correlations. World Neurosurg. 2017, 105, 895–905. [Google Scholar] [CrossRef]
- Campanella, R.; Guarnaccia, L.; Caroli, M.; Zarino, B.; Carrabba, G.; La Verde, N.; Gaudino, C.; Rampini, A.; Luzzi, S.; Riboni, L.; et al. Personalized and translational approach for malignant brain tumors in the era of precision medicine: The strategic contribution of an experienced neurosurgery laboratory in a modern neurosurgery and neuro-oncology department. J. Neurol. Sci. 2020, 417, 117083. [Google Scholar] [CrossRef] [PubMed]
- Luzzi, S.; Lucifero, A.G.; Brambilla, I.; Mantelli, S.S.; Mosconi, M.; Foiadelli, T.; Savasta, S. Targeting the medulloblastoma: A molecular-based approach. Acta Biomed. 2020, 91, 79–100. [Google Scholar]
- Luzzi, S.; Crovace, A.M.; Del Maestro, M.; Lucifero, A.G.; Elbabaa, S.K.; Cinque, B.; Palumbo, P.; Lombardi, F.; Cimini, A.; Cifone, M.G.; et al. The cell-based approach in neurosurgery: Ongoing trends and future perspectives. Heliyon 2019, 5, e02818. [Google Scholar] [CrossRef]
- Mount, N.M.; Ward, S.J.; Kefalas, P.; Hyllner, J. Cell-based therapy technology classifications and translational challenges. Philos. Trans. R. Soc. B Biol. Sci. 2015, 370, 20150017. [Google Scholar] [CrossRef]
- Everson, R.G.; Antonios, J.P.; Liau, L.M. Cell-Based Immunotherapy of Gliomas. Prog. Neurol. Surg. 2018, 32, 90–100. [Google Scholar] [CrossRef]
- Lucifero, A.G.; Luzzi, S.; Brambilla, I.; Schena, L.; Mosconi, M.; Foiadelli, T.; Savasta, S. Potential roads for reaching the summit: An overview on target therapies for high-grade gliomas. Acta Biomed. 2020, 91, 61–78. [Google Scholar]
- Han, S.J.; Zygourakis, C.; Lim, M.; Parsa, A.T. Immunotherapy for Glioma: Promises and challenges. Neurosurg. Clin. N. Am. 2012, 23, 357–370. [Google Scholar] [CrossRef]
- Luzzi, S.; Lucifero, A.G.; Brambilla, I.; Magistrali, M.; Mosconi, M.; Savasta, S.; Foiadelli, T. Adoptive immunotherapies in neuro-oncology: Classification, recent advances, and translational challenges. Acta Biomed. 2020, 91, 18–31. [Google Scholar] [PubMed]
- Wyatt, M.D.; Pittman, D.L. Methylating Agents and DNA Repair Responses: Methylated Bases and Sources of Strand Breaks. Chem. Res. Toxicol. 2006, 19, 1580–1594. [Google Scholar] [CrossRef] [PubMed]
- Friedman, H.S.; Kerby, T.; Calvert, H. Temozolomide and treatment of malignant glioma. Clin. Cancer Res. 2000, 6, 2585–2597. [Google Scholar] [PubMed]
- Schreck, K.C.; Grossman, S.A. Role of Temozolomide in the Treatment of Cancers Involving the Central Nervous System. Oncology 2018, 32, 555–560. [Google Scholar]
- Agarwala, S.S.; Kirkwood, J.M. Temozolomide, a Novel Alkylating Agent with Activity in the Central Nervous System, May Improve the Treatment of Advanced Metastatic Melanoma. Oncologist 2000, 5, 144–151. [Google Scholar] [CrossRef]
- Portnow, J.; Badie, B.; Chen, M.; Liu, A.; Blanchard, S.; Synold, T.W. The Neuropharmacokinetics of Temozolomide in Patients with Resectable Brain Tumors: Potential Implications for the Current Approach to Chemoradiation. Clin. Cancer Res. 2009, 15, 7092–7098. [Google Scholar] [CrossRef]
- Denny, B.J.; Wheelhouse, R.T.; Stevens, M.F.G.; Tsang, L.L.H.; Slack, J.A. NMR and Molecular Modeling Investigation of the Mechanism of Activation of the Antitumor Drug Temozolomide and Its Interaction with DNA. Biochemistry 1994, 33, 9045–9051. [Google Scholar] [CrossRef]
- Moody, C.L.; Wheelhouse, R.T. The Medicinal Chemistry of Imidazotetrazine Prodrugs. Pharmaceuticals 2014, 7, 797–838. [Google Scholar] [CrossRef]
- Strobel, H.; Baisch, T.; Fitzel, R.; Schilberg, K.; Siegelin, M.D.; Karpel-Massler, G.; Debatin, K.-M.; Westhoff, M.-A. Temozolomide and Other Alkylating Agents in Glioblastoma Therapy. Biomedicines 2019, 7, 69. [Google Scholar] [CrossRef]
- Hombach-Klonisch, S.; Mehrpour, M.; Shojaei, S.; Harlos, C.; Pitz, M.; Hamai, A.; Siemianowicz, K.; Likus, W.; Wiechec, E.; Toyota, B.D.; et al. Glioblastoma and chemoresistance to alkylating agents: Involvement of apoptosis, autophagy, and unfolded protein response. Pharmacol. Ther. 2018, 184, 13–41. [Google Scholar] [CrossRef]
- Zhang, J.; Stevens, M.F.; Bradshaw, T.D. Temozolomide: Mechanisms of Action, Repair and Resistance. Curr. Mol. Pharmacol. 2012, 5, 102–114. [Google Scholar] [CrossRef]
- Hegi, M.E.; Diserens, A.-C.; Gorlia, T.; Hamou, M.-F.; De Tribolet, N.; Weller, M.; Kros, J.M.; Hainfellner, J.A.; Mason, W.; Mariani, L.; et al. MGMTGene Silencing and Benefit from Temozolomide in Glioblastoma. N. Engl. J. Med. 2005, 352, 997–1003. [Google Scholar] [CrossRef]
- Rao, A.M.; Quddusi, A.; Shamim, M.S. The significance of MGMT methylation in Glioblastoma Multiforme prognosis. J. Pak. Med. Assoc. 2018, 68, 1137–1139. [Google Scholar] [PubMed]
- Binabaj, M.M.; Bahrami, A.; ShahidSales, S.; Joodi, M.; Mashhad, M.J.; Hassanian, S.M.; Anvari, K.; Avan, A. The prognostic value of MGMT promoter methylation in glioblastoma: A meta-analysis of clinical trials. J. Cell. Physiol. 2018, 233, 378–386. [Google Scholar] [CrossRef]
- Thon, N.; Kreth, S.; Kreth, F.W. Personalized treatment strategies in glioblastoma: MGMT promoter methylation status. OncoTargets Ther. 2013, 6, 1363–1372. [Google Scholar] [CrossRef]
- Hermisson, M.; Klumpp, A.; Wick, W.; Wischhusen, J.; Nagel, G.; Roos, W.; Kaina, B.; Weller, M. O6-methylguanine DNA methyltransferase and p53 status predict temozolomide sensitivity in human malignant glioma cells. J. Neurochem. 2006, 96, 766–776. [Google Scholar] [CrossRef] [PubMed]
- Wick, W.; Weller, M.; Bent, M.V.D.; Sanson, M.; Weiler, M.; Von Deimling, A.; Plass, C.; Hegi, M.E.; Platten, M.; Reifenberger, G. MGMT testing—The challenges for biomarker-based glioma treatment. Nat. Rev. Neurol. 2014, 10, 372–385. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.M.; Umemura, Y.; Leung, D. Bevacizumab and Glioblastoma: Past, Present, and Future Directions. Cancer J. 2018, 24, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Diaz, R.J.; Ali, S.; Qadir, M.G.; De La Fuente, M.I.; Ivan, M.E.; Komotar, R.J. The role of bevacizumab in the treatment of glioblastoma. J. Neuro Oncol. 2017, 133, 455–467. [Google Scholar] [CrossRef]
- Grill, J.; Massimino, M.; Bouffet, E.; Azizi, A.A.; McCowage, G.; Cañete, A.; Saran, F.; Le Deley, M.-C.; Varlet, P.; Morgan, P.S.; et al. Phase II, Open-Label, Randomized, Multicenter Trial (HERBY) of Bevacizumab in Pediatric Patients with Newly Diagnosed High-Grade Glioma. J. Clin. Oncol. 2018, 36, 951–958. [Google Scholar] [CrossRef]
- Salmaggi, A.; Gaviani, P.; Botturi, A.; Lamperti, E.; Simonetti, G.; Ferrari, D.; Silvani, A. Bevacizumab at recurrence in high-grade glioma. Neurol. Sci. 2011, 32, 251–253. [Google Scholar] [CrossRef] [PubMed]
- Bent, M.J.V.D.; Klein, M.; Smits, M.; Reijneveld, J.C.; French, P.J.; Clement, P.; De Vos, F.Y.F.; Wick, A.; Mulholland, P.J.; Taphoorn, M.J.B.; et al. Bevacizumab and temozolomide in patients with first recurrence of WHO grade II and III glioma, without 1p/19q co-deletion (TAVAREC): A randomised controlled phase 2 EORTC trial. Lancet Oncol. 2018, 19, 1170–1179. [Google Scholar] [CrossRef]
- Su, J.M.-F.; Murray, J.C.; McNall-Knapp, R.Y.; Bowers, D.C.; Shah, S.; Adesina, A.M.; Paulino, A.C.; Jo, E.; Mo, Q.; Baxter, P.A.; et al. A phase 2 study of valproic acid and radiation, followed by maintenance valproic acid and bevacizumab in children with newly diagnosed diffuse intrinsic pontine glioma or high-grade glioma. Pediatr. Blood Cancer 2020, 67, e28283. [Google Scholar] [CrossRef] [PubMed]
- Khasraw, M.; Simeonovic, M.; Grommes, C. Bevacizumab for the treatment of high-grade glioma. Expert Opin. Biol. Ther. 2012, 12, 1101–1111. [Google Scholar] [CrossRef] [PubMed]
- Khasraw, M.; Ameratunga, M.; Grommes, C. Bevacizumab for the treatment of high-grade glioma: An update after Phase III trials. Expert Opin. Biol. Ther. 2014, 14, 729–740. [Google Scholar] [CrossRef]
- Im, S.A.; Gomez-Manzano, C.; Fueyo, J.; Liu, T.J.; Ke, L.D.; Kim, J.S.; Lee, H.Y.; Steck, P.A.; Kyritsis, A.P.; Yung, W.K. Antiangiogenesis treatment for gliomas: Transfer of antisense-vascular endothelial growth factor inhibits tumor growth in vivo. Cancer Res. 1999, 59, 895–900. [Google Scholar] [PubMed]
- Von Baumgarten, L.; Brucker, D.; Tirniceru, A.; Kienast, Y.; Grau, S.; Burgold, S.; Herms, J.; Winkler, F. Bevacizumab Has Differential and Dose-Dependent Effects on Glioma Blood Vessels and Tumor Cells. Clin. Cancer Res. 2011, 17, 6192–6205. [Google Scholar] [CrossRef]
- Gabrilovich, D.I.; Chen, H.L.; Girgis, K.R.; Cunningham, H.T.; Meny, G.M.; Nadaf, S.; Kavanaugh, D.; Carbone, D.P. Production of vascular endothelial growth factor by human tumors inhibits the functional maturation of dendritic cells. Nat. Med. 1996, 2, 1096–1103. [Google Scholar] [CrossRef]
- Terme, M.; Pernot, S.; Marcheteau, E.; Sandoval, F.; Benhamouda, N.; Colussi, O.; Dubreuil, O.; Carpentier, A.F.; Tartour, E.; Taieb, J. VEGFA-VEGFR Pathway Blockade Inhibits Tumor-Induced Regulatory T-cell Proliferation in Colorectal Cancer. Cancer Res. 2013, 73, 539–549. [Google Scholar] [CrossRef]
- Shrimali, R.K.; Yu, Z.; Theoret, M.R.; Chinnasamy, D.; Restifo, N.P.; Rosenberg, S.A. Antiangiogenic Agents Can Increase Lymphocyte Infiltration into Tumor and Enhance the Effectiveness of Adoptive Immunotherapy of Cancer. Cancer Res. 2010, 70, 6171–6180. [Google Scholar] [CrossRef]
- Chinot, O.L.; Rouge, T.D.L.M.; Moore, N.; Zeaiter, A.; Das, A.; Phillips, H.; Modrusan, Z.; Cloughesy, T. AVAglio: Phase 3 trial of bevacizumab plus temozolomide and radiotherapy in newly diagnosed glioblastoma multiforme. Adv. Ther. 2011, 28, 334–340. [Google Scholar] [CrossRef]
- Gilbert, M.R.; Dignam, J.J.; Armstrong, T.S.; Wefel, J.S.; Blumenthal, D.T.; Vogelbaum, M.A.; Colman, H.; Chakravarti, A.; Pugh, S.; Won, M.; et al. A Randomized Trial of Bevacizumab for Newly Diagnosed Glioblastoma. N. Engl. J. Med. 2014, 370, 699–708. [Google Scholar] [CrossRef] [PubMed]
- Schalper, K.A.; Rodriguez-Ruiz, M.E.; Diez-Valle, R.; López-Janeiro, A.; Porciuncula, A.; Idoate, M.A.; Inogés, S.; De Andrea, C.; De Cerio, A.L.-D.; Tejada, S.; et al. Neoadjuvant nivolumab modifies the tumor immune microenvironment in resectable glioblastoma. Nat. Med. 2019, 25, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Chen, A.X.; Gartrell, R.D.; Silverman, A.M.; Aparicio, L.; Chu, T.; Bordbar, D.; Shan, D.; Samanamud, J.; Mahajan, A.; et al. Immune and genomic correlates of response to anti-PD-1 immunotherapy in glioblastoma. Nat. Med. 2019, 25, 462–469. [Google Scholar] [CrossRef]
- Ito, H.; Nakashima, H.; Chiocca, E.A. Molecular responses to immune checkpoint blockade in glioblastoma. Nat. Med. 2019, 25, 359–361. [Google Scholar] [CrossRef] [PubMed]
- Omuro, A.; Vlahovic, G.; Lim, M.; Sahebjam, S.; Baehring, J.; Cloughesy, T.; Voloschin, A.; Ramkissoon, S.H.; Ligon, K.L.; Latek, R.; et al. Nivolumab with or without ipilimumab in patients with recurrent glioblastoma: Results from exploratory phase I cohorts of CheckMate 143. Neuro Oncol. 2018, 20, 674–686. [Google Scholar] [CrossRef]
- Filley, A.C.; Henriquez, M.; Dey, M. Recurrent glioma clinical trial, CheckMate-143: The game is not over yet. Oncotarget 2017, 8, 91779–91794. [Google Scholar] [CrossRef] [PubMed]
- Reardon, D.A.; Brandes, A.A.; Omuro, A.; Mulholland, P.; Lim, M.; Wick, A.; Baehring, J.; Ahluwalia, M.S.; Roth, P.; Bähr, O.; et al. Effect of Nivolumab vs Bevacizumab in Patients with Recurrent Glioblastoma: The CheckMate 143 Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1003–1010. [Google Scholar] [CrossRef] [PubMed]
- Abrishami, M.; Zarei-Ghanavati, S.; Soroush, D.; Rouhbakhsh, M.; Jaafari, M.R.; Malaekeh-Nikouei, B. Preparation, characterization, and in vivo evaluation of nanoliposomes-encapsulated bevacizumab (avastin) for intravitreal administration. Retina 2009, 29, 699–703. [Google Scholar] [CrossRef]
- Burkhardt, J.-K.; Riina, H.; Shin, B.J.; Christos, P.; Kesavabhotla, K.; Hofstetter, C.P.; Tsiouris, A.J.; Boockvar, J.A. Intra-Arterial Delivery of Bevacizumab after Blood-Brain Barrier Disruption for the Treatment of Recurrent Glioblastoma: Progression-Free Survival and Overall Survival. World Neurosurg. 2012, 77, 130–134. [Google Scholar] [CrossRef]
- Wong, E.T.; Gautam, S.; Malchow, C.; Lun, M.; Pan, E.; Brem, S. Bevacizumab for recurrent glioblastoma multiforme: A meta-analysis. J. Natl. Compr. Cancer Netw. 2011, 9, 403–407. [Google Scholar] [CrossRef]
- Liu, Y.-X.; Liu, W.-J.; Zhang, H.-R.; Zhang, Z.-W. Delivery of bevacizumab by intracranial injection: Assessment in glioma model. OncoTargets Ther. 2018, 11, 2673–2683. [Google Scholar] [CrossRef] [PubMed]
- Del Vecchio, C.A.; Li, G.; Wong, A.J. Targeting EGF receptor variant III: Tumor-specific peptide vaccination for malignant gliomas. Expert Rev. Vaccines 2012, 11, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Mitra, S.; Wong, A.J. The Epidermal Growth Factor Variant III Peptide Vaccine for Treatment of Malignant Gliomas. Neurosurg. Clin. N. Am. 2010, 21, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Elsamadicy, A.A.; Chongsathidkiet, P.; Desai, R.; Woroniecka, K.; Farber, S.H.; Fecci, P.E.; Sampson, J.H. Prospect of rindopepimut in the treatment of glioblastoma. Expert Opin. Biol. Ther. 2017, 17, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Sampson, J.H.; Archer, G.E.; Mitchell, D.A.; Heimberger, A.B.; Bigner, D.D. Tumor-specific immunotherapy targeting the EGFRvIII mutation in patients with malignant glioma. Semin. Immunol. 2008, 20, 267–275. [Google Scholar] [CrossRef]
- Sampson, J.H.; Archer, G.E.; Mitchell, D.A.; Heimberger, A.B.; Herndon, J.E.; Lally-Goss, D.; McGehee-Norman, S.; Paolino, A.; Reardon, D.A.; Friedman, A.H.; et al. An epidermal growth factor receptor variant III–targeted vaccine is safe and immunogenic in patients with glioblastoma multiforme. Mol. Cancer Ther. 2009, 8, 2773–2779. [Google Scholar] [CrossRef]
- Swartz, A.M.; Batich, K.A.; Fecci, P.E.; Sampson, J.H. Peptide vaccines for the treatment of glioblastoma. J. Neuro Oncol. 2014, 123, 433–440. [Google Scholar] [CrossRef]
- Sampson, J.H.; Heimberger, A.B.; Archer, G.E.; Aldape, K.D.; Friedman, A.H.; Friedman, H.S.; Gilbert, M.R.; Ii, J.E.H.; McLendon, R.E.; Mitchell, D.A.; et al. Immunologic Escape After Prolonged Progression-Free Survival with Epidermal Growth Factor Receptor Variant III Peptide Vaccination in Patients with Newly Diagnosed Glioblastoma. J. Clin. Oncol. 2010, 28, 4722–4729. [Google Scholar] [CrossRef]
- Sampson, J.H.; Aldape, K.D.; Archer, G.E.; Coan, A.; Desjardins, A.; Friedman, A.H.; Friedman, H.S.; Gilbert, M.R.; Herndon, J.E.; McLendon, R.E.; et al. Greater chemotherapy-induced lymphopenia enhances tumor-specific immune responses that eliminate EGFRvIII-expressing tumor cells in patients with glioblastoma. Neuro Oncol. 2010, 13, 324–333. [Google Scholar] [CrossRef]
- Lai, R.; Recht, L.; Reardon, D.; Paleologos, N.; Groves, M.; Rosenfeld, M.; Davis, T.; Archer, G.; Green, J.; Heimberger, A.; et al. Long-term Follow-up of ACT III: A Phase II Trial of Rindopepimut (CDX-110) in Newly Diagnosed Glioblastoma. Neuro-Oncology 2011, 13, iii34–iii40. [Google Scholar]
- Gatson, N.T.N.; Weathers, S.-P.S.; De Groot, J.F. ReACT Phase II trial: A critical evaluation of the use of rindopepimut plus bevacizumab to treat EGFRvIII-positive recurrent glioblastoma (retracted). CNS Oncol. 2016, 5, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Platten, M. EGFRvIII vaccine in glioblastoma—InACT-IVe or not ReACTive enough? Neuro-Oncology 2017, 19, 1425–1426. [Google Scholar] [CrossRef] [PubMed]
- Lowenstein, P.R.; Castro, M.G. Multiple Expressed Endogenous Glioma Epitopes as Novel Vaccines for Gliomas. Clin. Cancer Res. 2016, 22, 4760–4762. [Google Scholar] [CrossRef][Green Version]
- Phuphanich, S.; Wheeler, C.J.; Rudnick, J.D.; Mazer, M.; Wang, H.; Nuño, M.A.; Richardson, J.E.; Fan, X.; Ji, J.; Chu, R.M.; et al. Phase I trial of a multi-epitope-pulsed dendritic cell vaccine for patients with newly diagnosed glioblastoma. Cancer Immunol. Immunother. 2012, 62, 125–135. [Google Scholar] [CrossRef]
- Polyzoidis, S.; Ashkan, K. DCVax®-L—Developed by Northwest Biotherapeutics. Hum. Vaccines Immunother. 2014, 10, 3139–3145. [Google Scholar] [CrossRef]
- Yan, Y.; Zeng, S.; Gong, Z.; Xu, Z. Clinical implication of cellular vaccine in glioma: Current advances and future prospects. J. Exp. Clin. Cancer Res. 2020, 39, 257. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, J.; Schüßler-Lenz, M.; Bondanza, A.; Buchholz, C.J. Clinical development of CAR T cells—challenges and opportunities in translating innovative treatment concepts. EMBO Mol. Med. 2017, 9, 1183–1197. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.; Riddell, S.R. Engineering CAR-T cells: Design concepts. Trends Immunol. 2015, 36, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-H.; Kim, C.H. Evolution of chimeric antigen receptor (CAR) T cell therapy: Current status and future perspectives. Arch. Pharmacal Res. 2019, 42, 607–616. [Google Scholar] [CrossRef] [PubMed]
- Petersen, C.T.; Krenciute, G. Next Generation CAR T Cells for the Immunotherapy of High-Grade Glioma. Front. Oncol. 2019, 9, 69. [Google Scholar] [CrossRef]
- Chuntova, P.; Downey, K.M.; Hegde, B.; Almeida, N.D.; Okada, H. Genetically Engineered T-Cells for Malignant Glioma: Overcoming the Barriers to Effective Immunotherapy. Front. Immunol. 2018, 9, 3062. [Google Scholar] [CrossRef] [PubMed]
- Choi, B.D.; Curry, W.T.; Carter, B.S.; Maus, M.V. Chimeric antigen receptor T-cell immunotherapy for glioblastoma: Practical insights for neurosurgeons. Neurosurg. Focus 2018, 44, E13. [Google Scholar] [CrossRef]
- Bagley, S.J.; Desai, A.S.; Linette, G.P.; June, C.H.; O’Rourke, D.M. CAR T-cell therapy for glioblastoma: Recent clinical advances and future challenges. Neuro Oncol. 2018, 20, 1429–1438. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.E.; Alizadeh, D.; Starr, R.; Weng, L.; Wagner, J.R.; Naranjo, A.; Ostberg, J.R.; Blanchard, M.S.; Kilpatrick, J.; Simpson, J.; et al. Regression of Glioblastoma after Chimeric Antigen Receptor T-Cell Therapy. N. Engl. J. Med. 2016, 375, 2561–2569. [Google Scholar] [CrossRef]
- Chow, K.K.H.; Naik, S.; Kakarla, S.; Brawley, V.S.; Shaffer, D.R.; Yi, Z.; Rainusso, N.; Wu, M.-F.; Liu, H.; Kew, Y.; et al. T Cells Redirected to EphA2 for the Immunotherapy of Glioblastoma. Mol. Ther. 2013, 21, 629–637. [Google Scholar] [CrossRef]
- O’Rourke, D.M.; Nasrallah, M.P.; Desai, A.; Melenhorst, J.J.; Mansfield, K.; Morrissette, J.J.D.; Martinez-Lage, M.; Brem, S.; Maloney, E.; Shen, A.; et al. A single dose of peripherally infused EGFRvIII-directed CAR T cells mediates antigen loss and induces adaptive resistance in patients with recurrent glioblastoma. Sci. Transl. Med. 2017, 9, eaaa0984. [Google Scholar] [CrossRef]
- Ahmed, N.; Brawley, V.; Hegde, M.; Bielamowicz, K.; Kalra, M.; Landi, D.; Robertson, C.; Gray, T.L.; Diouf, O.; Wakefield, A.; et al. HER2-Specific Chimeric Antigen Receptor–Modified Virus-Specific T Cells for Progressive Glioblastoma: A Phase 1 Dose-Escalation Trial. JAMA Oncol. 2017, 3, 1094–1101. [Google Scholar] [CrossRef]
- Kwatra, M.M. A Rational Approach to Target the Epidermal Growth Factor Receptor in Glioblastoma. Curr. Cancer Drug Targets 2017, 17, 290–296. [Google Scholar] [CrossRef]
- Padfield, E.; Ellis, H.P.; Kurian, K.M. Current Therapeutic Advances Targeting EGFR and EGFRvIII in Glioblastoma. Front. Oncol. 2015, 5, 5. [Google Scholar] [CrossRef] [PubMed]
- Ren, P.-P.; Li, M.; Li, T.-F.; Han, S.-Y. Anti-EGFRvIII Chimeric Antigen Receptor-Modified T Cells for Adoptive Cell Therapy of Glioblastoma. Curr. Pharm. Des. 2017, 23, 2113–2116. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.E.; Badie, B.; Barish, M.E.; Weng, L.; Ostberg, J.R.; Chang, W.-C.; Naranjo, A.; Starr, R.; Wagner, J.R.; Wright, C.; et al. Bioactivity and Safety of IL13Rα2-Redirected Chimeric Antigen Receptor CD8+ T Cells in Patients with Recurrent Glioblastoma. Clin. Cancer Res. 2015, 21, 4062–4072. [Google Scholar] [CrossRef]
- Brown, C.E.; Aguilar, B.; Starr, R.; Yang, X.; Chang, W.-C.; Weng, L.; Chang, B.; Sarkissian, A.; Brito, A.; Sanchez, J.F.; et al. Optimization of IL13Rα2-Targeted Chimeric Antigen Receptor T Cells for Improved Anti-tumor Efficacy against Glioblastoma. Mol. Ther. 2018, 26, 31–44. [Google Scholar] [CrossRef] [PubMed]
- Krenciute, G.; Prinzing, B.L.; Yi, Z.; Wu, M.-F.; Liu, H.; Dotti, G.; Balyasnikova, I.V.; Gottschalk, S. Transgenic Expression of IL15 Improves Antiglioma Activity of IL13Rα2-CAR T Cells but Results in Antigen Loss Variants. Cancer Immunol. Res. 2017, 5, 571–581. [Google Scholar] [CrossRef]
- Ahmed, N.; Salsman, V.S.; Kew, Y.; Shaffer, D.; Powell, S.; Zhang, Y.J.; Grossman, R.G.; Heslop, H.E.; Gottschalk, S. HER2-Specific T Cells Target Primary Glioblastoma Stem Cells and Induce Regression of Autologous Experimental Tumors. Clin. Cancer Res. 2010, 16, 474–485. [Google Scholar] [CrossRef] [PubMed]
- Heemskerk, M.H. T-cell receptor gene transfer for the treatment of leukemia and other tumors. Haematologica 2010, 95, 15–19. [Google Scholar] [CrossRef]
- Kessels, H.W.H.G.; Wolkers, M.C.; Boom, M.D.V.D.; Valk, M.A.V.D.; Schumacher, T.N.M. Immunotherapy through TCR gene transfer. Nat. Immunol. 2001, 2, 957–961. [Google Scholar] [CrossRef]
- Park, T.S.; Rosenberg, S.A.; Morgan, R.A. Treating cancer with genetically engineered T cells. Trends Biotechnol. 2011, 29, 550–557. [Google Scholar] [CrossRef]
- Smith, T.W.; Nishimura, M.I. Targeting Cancer with Genetically Engineered TCR T Cells. Methods Mol. Biol. 2019, 214, 129–151. [Google Scholar] [CrossRef]
- Sermer, D.; Brentjens, R. CAR T-cell therapy: Full speed ahead. Hematol. Oncol. 2019, 37, 95–100. [Google Scholar] [CrossRef]
- June, C.H.; O’Connor, R.S.; Kawalekar, O.U.; Ghassemi, S.; Milone, M.C. CAR T cell immunotherapy for human cancer. Science 2018, 359, 1361–1365. [Google Scholar] [CrossRef] [PubMed]
- Fesnak, A.D.; June, C.H.; Levine, B.L. Engineered T cells: The promise and challenges of cancer immunotherapy. Nat. Rev. Cancer 2016, 16, 566–581. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, R.; Chowdhury, C.R.; Arega, S.; Sen, P.; Ganguly, P.; Ganguly, N. CAR T cell therapy: A new era for cancer treatment (Review). Oncol. Rep. 2019, 42, 2183–2195. [Google Scholar] [CrossRef] [PubMed]
- Golán, I.; De La Fuente, L.R.; Costoya, J.A. NK Cell-Based Glioblastoma Immunotherapy. Cancers 2018, 10, 522. [Google Scholar] [CrossRef]
- Karantalis, V.; Schulman, I.H.; Balkan, W.; Hare, J.M. Allogeneic cell therapy: A new paradigm in therapeutics. Circ. Res. 2015, 116, 12–15. [Google Scholar] [CrossRef]
- Geller, M.A.; Miller, J.S. Use of allogeneic NK cells for cancer immunotherapy. Immunotherapy 2011, 3, 1445–1459. [Google Scholar] [CrossRef]
- Ruggeri, L.; Capanni, M.; Urbani, E.; Perruccio, K.; Shlomchik, W.D.; Tosti, A.; Posati, S.; Rogaia, D.; Frassoni, F.; Aversa, F.; et al. Effectiveness of Donor Natural Killer Cell Alloreactivity in Mismatched Hematopoietic Transplants. Science 2002, 295, 2097–2100. [Google Scholar] [CrossRef]
- Ishikawa, E.; Tsuboi, K.; Saijo, K.; Harada, H.; Takano, S.; Nose, T.; Ohno, T. Autologous natural killer cell therapy for human recurrent malignant glioma. Anticancer. Res. 2004, 24, 1861–1871. [Google Scholar]
- Navarro, A.G.; Kmiecik, J.; Leiss, L.; Zelkowski, M.; Engelsen, A.; Bruserud, Ø.; Zimmer, J.; Enger, P.; Chekenya, M. NK Cells with KIR2DS2 Immunogenotype Have a Functional Activation Advantage to Efficiently Kill Glioblastoma and Prolong Animal Survival. J. Immunol. 2014, 193, 6192–6206. [Google Scholar] [CrossRef] [PubMed]
- Yvon, E.S.; Burga, R.; Powell, A.; Cruz, C.R.; Fernandes, R.; Barese, C.; Nguyen, T.; Abdel-Baki, M.S.; Bollard, C.M. Cord blood natural killer cells expressing a dominant negative TGF-β receptor: Implications for adoptive immunotherapy for glioblastoma. Cytotherapy 2017, 19, 408–418. [Google Scholar] [CrossRef] [PubMed]
- Murakami, T.; Nakazawa, T.; Natsume, A.; Nishimura, F.; Nakamura, M.; Matsuda, R.; Omoto, K.; Tanaka, Y.; Shida, Y.; Park, Y.-S.; et al. Novel Human NK Cell Line Carrying CAR Targeting EGFRvIII Induces Antitumor Effects in Glioblastoma Cells. Anticancer. Res. 2018, 38, 5049–5056. [Google Scholar] [CrossRef]
- Kmiecik, J.; Navarro, A.G.; Poli, A.; Planagumà, J.P.; Zimmer, J.; Chekenya, M. Combining NK cells and mAb9.2.27 to combat NG2-dependent and anti-inflammatory signals in glioblastoma. OncoImmunology 2014, 3, e27185. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Oh, J.M.; Gangadaran, P.; Kalimuthu, S.; Baek, S.H.; Jeong, S.Y.; Lee, S.-W.; Lee, J.; Ahn, B.-C. Targeting and Therapy of Glioblastoma in a Mouse Model Using Exosomes Derived from Natural Killer Cells. Front. Immunol. 2018, 9, 824. [Google Scholar] [CrossRef]
- Seino, K.-I.; Motohashi, S.; Fujisawa, T.; Nakayama, T.; Taniguchi, M. Natural killer T cell-mediated antitumor immune responses and their clinical applications. Cancer Sci. 2006, 97, 807–812. [Google Scholar] [CrossRef]
- Dhodapkar, K.M.; Cirignano, B.; Chamian, F.; Zagzag, D.; Miller, D.C.; Finlay, J.L.; Steinman, R.M. Invariant natural killer T cells are preserved in patients with glioma and exhibit antitumor lytic activity following dendritic cell-mediated expansion. Int. J. Cancer 2004, 109, 893–899. [Google Scholar] [CrossRef]
- Giaccone, G.; Punt, C.J.A.; Ando, Y.; Ruijter, R.; Nishi, N.; Peters, M.; Von Blomberg, B.M.E.; Scheper, R.J.; Van Der Vliet, H.J.J.; Eertwegh, A.J.; et al. A phase I study of the natural killer T-cell ligand alpha-galactosylceramide (KRN7000) in patients with solid tumors. Clin. Cancer Res. 2002, 8, 3702–3709. [Google Scholar]
- Wenger, A.; Werlenius, K.; Hallner, A.; Thorén, F.B.; Farahmand, D.; Tisell, M.; Smits, A.; Rydenhag, B.; Jakola, A.S.; Carén, H. Determinants for Effective ALECSAT Immunotherapy Treatment on Autologous Patient-Derived Glioblastoma Stem Cells. Neoplasia 2018, 20, 25–31. [Google Scholar] [CrossRef]
- Harter, D.H.; Wilson, T.A.; Karajannis, M.A. Glioblastoma multiforme: State of the art and future therapeutics. Surg. Neurol. Int. 2014, 5, 64. [Google Scholar] [CrossRef]
- Giese, A.; Bjerkvig, R.; Berens, M.; Westphal, M. Cost of Migration: Invasion of Malignant Gliomas and Implications for Treatment. J. Clin. Oncol. 2003, 21, 1624–1636. [Google Scholar] [CrossRef]
- Bocangel, D.B.; Finkelstein, S.; Schold, S.C.; Bhakat, K.K.; Mitra, S.; Kokkinakis, D.M. Multifaceted resistance of gliomas to temozolomide. Clin. Cancer Res. 2002, 8, 2725–2734. [Google Scholar]
- Rabé, M.; Dumont, S.; Álvarez-Arenas, A.; Janati, H.; Belmonte-Beitia, J.; Calvo, G.F.; Thibault-Carpentier, C.; Séry, Q.; Chauvin, C.; Joalland, N.; et al. Identification of a transient state during the acquisition of temozolomide resistance in glioblastoma. Cell Death Dis. 2020, 11, 1–14. [Google Scholar] [CrossRef]
- Jiapaer, S.; Furuta, T.; Tanaka, S.; Kitabayashi, T.; Nakada, M. Potential Strategies Overcoming the Temozolomide Resistance for Glioblastoma. Neurol. Med. Chir. 2018, 58, 405–421. [Google Scholar] [CrossRef]
- Fang, C.; Wang, K.; Stephen, Z.R.; Mu, Q.; Kievit, F.M.; Chiu, D.T.; Press, O.W.; Zhang, M. Temozolomide Nanoparticles for Targeted Glioblastoma Therapy. ACS Appl. Mater. Interfaces 2015, 7, 6674–6682. [Google Scholar] [CrossRef]
- Sengupta, S.; Marrinan, J.; Frishman, C.; Sampath, P. Impact of Temozolomide on Immune Response during Malignant Glioma Chemotherapy. Clin. Dev. Immunol. 2012, 2012, 1–7. [Google Scholar] [CrossRef]
- Alvino, E.; Pepponi, R.; Pagani, E.; Lacal, P.M.; Nunziata, C.; Bonmassar, E.; D’Atri, S. O(6)-benzylguanine enhances the in vitro immunotoxic activity of temozolomide on natural or antigen-dependent immunity. J. Pharmacol. Exp. Ther. 1999, 291, 1292–1300. [Google Scholar] [PubMed]
- Heimberger, A.B.; Sun, W.; Hussain, S.F.; Dey, M.; Crutcher, L.; Aldape, K.; Gilbert, M.; Hassenbusch, S.J.; Sawaya, R.; Schmittling, B.; et al. Immunological responses in a patient with glioblastoma multiforme treated with sequential courses of temozolomide and immunotherapy: Case study. Neuro-Oncology 2008, 10, 98–103. [Google Scholar] [CrossRef]
- Fukushima, T.; Takeshima, H.; Kataoka, H. Anti-glioma therapy with temozolomide and status of the DNA-repair gene MGMT. Anticancer. Res. 2009, 29, 4845–4854. [Google Scholar] [PubMed]
- Bell, E.H.; Zhang, P.; Fisher, B.J.; Macdonald, D.R.; McElroy, J.P.; Lesser, G.J.; Fleming, J.; Chakraborty, A.R.; Liu, Z.; Becker, A.P.; et al. Association of MGMT Promoter Methylation Status with Survival Outcomes in Patients with High-Risk Glioma Treated with Radiotherapy and Temozolomide: An Analysis from the NRG Oncology/RTOG 0424 Trial. JAMA Oncol. 2018, 4, 1405–1409. [Google Scholar] [CrossRef] [PubMed]
- Friedman, H.S.; Prados, M.D.; Wen, P.Y.; Mikkelsen, T.; Schiff, D.; Abrey, L.E.; Yung, W.A.; Paleologos, N.; Nicholas, M.K.; Jensen, R.; et al. Bevacizumab Alone and in Combination With Irinotecan in Recurrent Glioblastoma. J. Clin. Oncol. 2009, 27, 4733–4740. [Google Scholar] [CrossRef] [PubMed]
- Arevalo, O.D.; Soto, C.; Rabiei, P.; Kamali, A.; Ballester, L.Y.; Esquenazi, Y.; Zhu, J.-J.; Riascos, R.F. Assessment of Glioblastoma Response in the Era of Bevacizumab: Longstanding and Emergent Challenges in the Imaging Evaluation of Pseudoresponse. Front. Neurol. 2019, 10, 460. [Google Scholar] [CrossRef] [PubMed]
- Castro, B.A.; Aghi, M.K. Bevacizumab for glioblastoma: Current indications, surgical implications, and future directions. Neurosurg. Focus 2014, 37, E9. [Google Scholar] [CrossRef]
- Kothari, P.; White, N.S.; Farid, N.; Chung, R.; Kuperman, J.M.; Girard, H.M.; Shankaranarayanan, A.; Kesari, S.; McDonald, C.R.; Dale, A.M. Longitudinal Restriction Spectrum Imaging Is Resistant to Pseudoresponse in Patients with High-Grade Gliomas Treated with Bevacizumab. Am. J. Neuroradiol. 2013, 34, 1752–1757. [Google Scholar] [CrossRef]
- Auer, T.A.; Breit, H.-C.; Marini, F.; Renovanz, M.; Ringel, F.; Sommer, C.J.; Brockmann, M.A.; Tanyildizi, Y. Evaluation of the apparent diffusion coefficient in patients with recurrent glioblastoma under treatment with bevacizumab with radiographic pseudoresponse. J. Neuroradiol. 2019, 46, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Swartz, A.M.; Li, Q.-J.; Sampson, J.H. Rindopepimut: A promising immunotherapeutic for the treatment of glioblastoma multiforme. Immunotherapy 2014, 6, 679–690. [Google Scholar] [CrossRef]
- Londhe, V.Y.; Date, V. Personalized neoantigen vaccines: A glimmer of hope for glioblastoma. Expert Rev. Vaccines 2020, 19, 407–417. [Google Scholar] [CrossRef]
- Neagu, M.R.; Reardon, D.A. An Update on the Role of Immunotherapy and Vaccine Strategies for Primary Brain Tumors. Curr. Treat. Options Oncol. 2015, 16, 54. [Google Scholar] [CrossRef]
- Ma, Q.; Long, W.; Xing, C.; Chu, J.; Luo, M.; Wang, H.Y.; Liu, Q.; Wang, R.-F. Cancer Stem Cells and Immunosuppressive Microenvironment in Glioma. Front. Immunol. 2018, 9, 2924. [Google Scholar] [CrossRef]
- Tamura, R.; Tanaka, T.; Akasaki, Y.; Murayama, Y.; Yoshida, K.; Sasaki, H. The role of vascular endothelial growth factor in the hypoxic and immunosuppressive tumor microenvironment: Perspectives for therapeutic implications. Med Oncol. 2019, 37, 2. [Google Scholar] [CrossRef]
- Luzzi, S.; Lucifero, A.G.; Brambilla, I.; Trabatti, C.; Mosconi, M.; Savasta, S.; Foiadelli, T. The impact of stem cells in neuro-oncology: Applications, evidence, limitations and challenges. Acta Biomed. 2020, 91, 51–60. [Google Scholar]
- Palumbo, P.; Lombardi, F.; Siragusa, G.; Dehcordi, S.R.; Luzzi, S.; Cimini, A.; Cifone, M.G.; Cinque, B. Involvement of NOS2 Activity on Human Glioma Cell Growth, Clonogenic Potential, and Neurosphere Generation. Int. J. Mol. Sci. 2018, 19, 2801. [Google Scholar] [CrossRef]
- Palumbo, P.; Lombardi, F.; Augello, F.R.; Giusti, I.; Luzzi, S.; Dolo, V.; Cifone, M.G.; Cinque, B. NOS2 inhibitor 1400W Induces Autophagic Flux and Influences Extracellular Vesicle Profile in Human Glioblastoma U87MG Cell Line. Int. J. Mol. Sci. 2019, 20, 3010. [Google Scholar] [CrossRef]
- Antonosante, A.; Brandolini, L.; D’Angelo, M.; Benedetti, E.; Castelli, V.; Del Maestro, M.; Luzzi, S.; Giordano, A.; Cimini, A.; Allegretti, M. Autocrine CXCL8-dependent invasiveness triggers modulation of actin cytoskeletal network and cell dynamics. Aging 2020, 12, 1928–1951. [Google Scholar] [CrossRef]
- Kwok, D.; Okada, H. T-Cell based therapies for overcoming neuroanatomical and immunosuppressive challenges within the glioma microenvironment. J. Neuro Oncol. 2020, 147, 281–295. [Google Scholar] [CrossRef]
- D’Amico, R.S.; Khatri, D.; Reichman, N.; Patel, N.V.; Wong, T.; Fralin, S.R.; Li, M.; Ellis, J.A.; Ortiz, R.; Langer, D.J.; et al. Super selective intra-arterial cerebral infusion of modern chemotherapeutics after blood–brain barrier disruption: Where are we now, and where we are going. J. Neuro Oncol. 2020, 147, 261–278. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, R.S.; Neira, J.A.; Yun, J.; Alexiades, N.G.; Banu, M.; Englander, Z.K.; Kennedy, B.C.; Ung, T.H.; Rothrock, R.J.; Romanov, A.; et al. Validation of an effective implantable pump-infusion system for chronic convection-enhanced delivery of intracerebral topotecan in a large animal model. J. Neurosurg. 2020, 133, 614–623. [Google Scholar] [CrossRef] [PubMed]
- Elleaume, H.; Barth, R.F.; Rousseau, J.; Bobyk, L.; Balosso, J.; Yang, W.; Huo, T.; Nakkula, R. Radiation therapy combined with intracerebral convection-enhanced delivery of cisplatin or carboplatin for treatment of the F98 rat glioma. J. Neuro-Oncol. 2020, 149, 193–208. [Google Scholar] [CrossRef]
- Sonabend, A.M.; Stuart, R.M.; Yun, J.; Yanagihara, T.; Mohajed, H.; Dashnaw, S.; Bruce, S.S.; Brown, T.; Romanov, A.; Sebastian, M.; et al. Prolonged intracerebral convection-enhanced delivery of topotecan with a subcutaneously implantable infusion pump. Neuro-Oncology 2011, 13, 886–893. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, S.; Filippi, C.G.; Wong, T.; Ray, A.; Fralin, S.; Tsiouris, A.J.; Praminick, B.; Demopoulos, A.; McCrea, H.J.; Bodhinayake, I.; et al. Superselective intraarterial cerebral infusion of cetuximab after osmotic blood/brain barrier disruption for recurrent malignant glioma: Phase I study. J. Neuro-Oncol. 2016, 128, 405–415. [Google Scholar] [CrossRef]
- Riina, H.; Knopman, J.; Greenfield, J.; Fralin, S.; Gobin, Y.P.; Tsiouris, A.; Souweidane, M.; Boockvar, J. Balloon-Assisted Superselective Intra-Arterial Cerebral Infusion of Bevacizumab for Malignant Brainstem Glioma: A Technical Note. Interv. Neuroradiol. 2010, 16, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Etame, A.B.; Diaz, R.J.; Smith, C.A.; Mainprize, T.G.; Hynynen, K.; Rutka, J.T. Focused ultrasound disruption of the blood-brain barrier: A new frontier for therapeutic delivery in molecular neurooncology. Neurosurg. Focus 2012, 32, E3. [Google Scholar] [CrossRef]
- Carpentier, A.; Canney, M.; Vignot, A.; Reina, V.; Beccaria, K.; Horodyckid, C.; Karachi, C.; Leclercq, D.; Lafon, C.; Chapelon, J.-Y.; et al. Clinical trial of blood-brain barrier disruption by pulsed ultrasound. Sci. Transl. Med. 2016, 8, 343re2. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.V.; Khatri, D.; D’Amico, R.; Abrams, M.; Reichman, N.; Filippi, C.G.; Anderson, T.; Ratzon, F.; Wong, T.; Fralin, S.; et al. Vascularized Temporoparietal Fascial Flap: A Novel Surgical Technique to Bypass the Blood-Brain Barrier in Glioblastoma. World Neurosurg. 2020, 143, 38–45. [Google Scholar] [CrossRef]
- Jiang, W.; Kim, B.Y.; Rutka, J.T.; Chan, W.C. Advances and challenges of nanotechnology-based drug delivery systems. Expert Opin. Drug Deliv. 2007, 4, 621–633. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, J.; Mizuno, M. Clinical gene therapy for brain tumors. Liposomal delivery of anticancer molecule to glioma. J. Neuro-Oncol. 2003, 65, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Lachmann, R.H. Herpes simplex virus-based vectors. Int. J. Exp. Pathol. 2004, 85, 177–190. [Google Scholar] [CrossRef]
- Jabir, N.R.; Tabrez, S.; Ashraf, G.M.; Shakil, S.; Damanhouri, G.A.; Kamal, M.A. Nanotechnology-based approaches in anticancer research. Int. J. Nanomed. 2012, 7, 4391. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Reviews, peer-reviews, editorials | Case reports, abstracts, and dissertations |
| Clinical, pre-clinical Trials | Withdrawn or abandoned clinical trials |
| English language, or translated | Non-English language |
| Publications from 2010–2020 | Studies not from 2010–2020 |
| Studies on humans or human products | Animal studies |
| Publications related to neuro-oncology | Publications not related to neuro-oncology |
| Publications related to high-grade glioma | Publications not related to high-grade glioma |
| Adult and pediatric patients |
| # | ClinicalTrials.gov Identifier | Title | Status | Phase | Diseases | # of Pts. Enrolled | Treatment | Locations |
|---|---|---|---|---|---|---|---|---|
| 1 | NCT03011671 | Study of Acetazolamide With Temozolomide in Adults With Newly Diagnosed or Recurrent Malignant Glioma | Suspended | I | Malignant Glioma of Brain | 24 | Acetazolamide, Temozolomide | USA |
| 2 | NCT02416999 | Ultra-low Dose Bevacizumab Plus Temozolomide for Recurrent High-grade Gliomas | Unknown | NA | Recurrent High-grade Glioma | 30 | Ultra-low dose Bevacizumab, Temozolomide | CHN |
| 3 | NCT01891747 | A Phase I Study of High-dose L-methylfolate in Combination With Temozolomide and Bevacizumab in Recurrent High Grade Glioma | Active, not recruiting | I | Malignant Glioma | 12 | Bevacizumab, Temozolomide, Vitamin C | USA |
| 4 | NCT04267146 | Nivolumab in Combination With Temozolomide and Radiotherapy in Children and Adolescents With Newly Diagnosed High-grade Glioma | Recruiting | I, II | High Grade Glioma | 40 | Nivolumab, Temozolomide, Radiotherapy | FR |
| 5 | NCT00782756 | Bevacizumab, Temozolomide and Hypofractionated Radiotherapy for Patients With Newly Diagnosed Malignant Glioma | Completed | II | Brain Cancer, Malignant Glioma | 40 | Radiotherapy, Temozolomide, Bevacizumab | USA |
| 6 | NCT04547621 | HSRT and IMRT Chemoradiotherapy for Newly Diagnosed GBM | Active, not recruiting | I, II | Glioma, Malignant | 50 | Radiation, Temozolomide | CHN |
| 7 | NCT01390948 | A Study of Bevacizumab (Avastin) in Combination With Temozolomide and Radiotherapy in Paediatric and Adolescent Participants With High-Grade Glioma | Completed | II | High Grade Glioma | 124 | Bevacizumab, Radiotherapy, Temozolomide | A |
| 8 | NCT00660621 | A Phase II Study Of Gliadel, Concomitant Temozolomide And Radiation, Followed By Dose Dense Therapy With Temozolomide Plus Bevacizumab For Newly Diagnosed Malignant High Grade Glioma | Unknown | II | Glioma | 40 | Temozolomide, Bevacizumab | USA |
| 9 | NCT03633552 | Efficacy of Two Temozolomide Regimens in Adjuvant Treatment of Patients With Brain High Grade Glioma | Recruiting | III | Glioblastoma Multiforme Anaplastic Astrocytoma | 62 | Temozolomide | IR |
| 10 | NCT01105702 | Temodar (Temozolomide), Bevacizumab, Lithium and Radiation for High Grade Glioma | Terminated | II | Brain Cancer | 28 | Temozolomide, Bevacizumab, Lithium Carbonate, Radiation | USA |
| 11 | NCT01740258 | Bevacizumab Beyond Progression (BBP) | Completed | II | Malignant Glioma, Glioblastoma, Gliosarcoma | 68 | Radiation Therapy, Temozolomide, Bevacizumab | USA |
| 12 | NCT01478321 | Efficacy of Hypofractionated XRT w/Bev. + Temozolomide for Recurrent Gliomas | Terminated | II | Adult Anaplastic Astrocytoma Ependymoma Oligodendroglioma/Glioblastoma | 54 | Temozolomide, Bevacizumab Hypofractionated radiation therapy | USA |
| 13 | NCT00943826 | A Study of Bevacizumab (Avastin®) in Combination With Temozolomide and Radiotherapy in Participants With Newly Diagnosed Glioblastoma | Completed | III | Glioblastoma | 921 | Bevacizumab, Temozolomide Radiation therapy | USA |
| 14 | NCT00884741 | Temozolomide and Radiation Therapy With or Without Bevacizumab in Treating Patients With Newly Diagnosed Glioblastoma | Completed | III | Glioblastoma, Gliosarcoma, Supratentorial Glioblastoma | 637 | Radiation Therapy, Temozolomide, Bevacizumab | USA |
| 15 | NCT01046279 | Hypertension Monitoring in Glioma Patients Treated With Bevacizumab | Terminated | NA | Glioma | 40 | Bevacizumab | ZH |
| 16 | NCT00271609 | Bevacizumab for Recurrent Malignant Glioma | Completed | II | Recurrent High-Grade Gliomas | 88 | Bevacizumab | USA |
| 17 | NCT02833701 | Bevacizumab and Ascorbic Acid in Patients Treating With Recurrent High Grade Glioma | Terminated | I | Glioblastoma, Glioma | 9 | Ascorbic Acid, Bevacizumab | USA |
| 18 | NCT00595322 | Bevacizumab in the Radiation Treatment of Recurrent Malignant Glioma | Completed | NA | Recurrent Malignant Gliomas, Primary Brain Tumor | 25 | Bevacizumab, Radiation | USA |
| 19 | NCT00337207 | Bevacizumab in Treating Patients With Recurrent or Progressive Glioma | Completed | II | Central Nervous System Tumors | 55 | Bevacizumab | USA |
| 20 | NCT01091792 | Exploratory Study of the Modulation of the Immune System by VEGF Blockade in Patients With Glioblastoma Multiforme (GBM) | Completed | I | Glioblastoma Multiforme | 13 | Bevacizumab | USA |
| 21 | NCT00883298 | Bi-weekly Temozolomide Plus Bevacizumab for Adult Patients With Recurrent Glioblastoma Multiforme | Completed | II | Recurrent Glioblastoma Multiforme Recurrent Gliosarcoma | 30 | Temozolomide, Bevacizumab | USA |
| 22 | NCT01811498 | Repeated Super-Selective Intraarterial Cerebral Infusion of Bevacizumab (Avastin) for Treatment of Newly Diagnosed GBM | Active, not recruiting | I, II | Glioblastoma Multiforme, Brain Tumor | 25 | Bevacizumab | USA |
| 23 | NCT01730950 | Bevacizumab With or Without Radiation Therapy in Treating Patients With Recurrent Glioblastoma | Active, not recruiting | II | Adult Giant Cell Glioblastoma, Glioblastoma, Adult Gliosarcoma Recurrent Adult Brain Tumor | 182 | Bevacizumab, Radiation therapy | USA |
| 24 | NCT02761070 | Bevacizumab Alone Versus Dose-dense Temozolomide Followed by Bevacizumab for Recurrent Glioblastoma, Phase III | Recruiting | III | Recurrent Glioblastoma | 146 | Temozolomide, Bevacizumab | J |
| 25 | NCT01209442 | Hypofractionated Intensity-Modulated Radiation Therapy With Temozolomide and Bevacizumab for Glioblastoma Multiforme | Completed | II | Glioblastoma Multiforme | 30 | Bevacizumab, Temozolomide Radiation Therapy | USA |
| 26 | NCT01125046 | Bevacizumab in Treating Patients With Recurrent or Progressive Meningiomas | Completed | II | Central Nervous System Tumors | 50 | Bevacizumab | USA |
| 27 | NCT01526837 | Bevacizumab (Avastin) Into the Tumor Resection Cavity in Subjects With Glioblastoma Multiforme at First Recurrence | Terminated | I | Glioblastoma Multiforme | 1 | Bevacizumab | USA |
| 28 | NCT01443676 | Avastin Plus Radiotherapy in Elderly Patients With Glioblastoma | Completed | II | Glioblastoma | 75 | Bevacizumab, Radiation therapy | USA |
| 29 | NCT00590681 | Bevacizumab and Temozolomide Following Radiation and Chemotherapy for Newly Diagnosed Glioblastoma Multiforme | Completed | II | Glioblastoma Multiforme | 62 | Bevacizumab, Temozolomide | USA |
| 30 | NCT03925246 | Efficacy of Nivolumab for Recurrent IDH Mutated High-Grade Gliomas | Active, not recruiting | II | High Grade Glioma, Brain Cancer | 43 | Nivolumab | FR |
| 31 | NCT00345163 | A Study to Evaluate Bevacizumab Alone or in Combination With Irinotecan for Treatment of Glioblastoma Multiforme (BRAIN) | Completed | II | Glioblastoma | 167 | Bevacizumab, Irinotecan | NA |
| 32 | NCT03890952 | Translational Study of Nivolumab in Combination With Bevacizumab for Recurrent Glioblastoma | Recruiting | II | Recurrent Adult Brain Tumor | 40 | Nivolumab, Bevacizumab | DNK |
| 33 | NCT01498328 | A Study of Rindopepimut/GM-CSF in Patients With Relapsed EGFRvIII-Positive Glioblastoma | Completed | II | Glioblastoma | 127 | Rindopepimut (CDX-110) with GM-CSF Bevacizumab, KLH | USA |
| 34 | NCT03743662 | Nivolumab With Radiation Therapy and Bevacizumab for Recurrent MGMT Methylated Glioblastoma | Recruiting | II | Glioblastoma | 94 | Re-irradiation, Bevacizumab Nivolumab, Re-resection | USA |
| 35 | NCT03452579 | Nivolumab Plus Standard Dose Bevacizumab Versus Nivolumab Plus Low Dose Bevacizumab in GBM | Active, not recruiting | II | Glioblastoma | 90 | Nivolumab, Standard/Reduced Dose Bevacizumab | USA |
| 36 | NCT02550249 | Neoadjuvant Nivolumab in Glioblastoma | Completed | II | Glioblastoma Multiforme | 29 | Nivolumab | ES |
| 37 | NCT04195139 | Nivolumab and Temozolomide Versus Temozolomide Alone in Newly Diagnosed Elderly Patients With GBM | Recruiting | II | Glioblastoma Multiforme | 102 | Nivolumab, Temozolomide | A |
| 38 | NCT02667587 | An Investigational Immuno-therapy Study of Temozolomide Plus Radiation Therapy With Nivolumab or Placebo, for Newly Diagnosed Patients With Glioblastoma (GBM, a Malignant Brain Cancer) | Active, not recruiting | III | Brain Neoplasms | 693 | Nivolumab, Temozolomide, Radiotherapy | USA |
| 39 | NCT02617589 | An Investigational Immuno-therapy Study of Nivolumab Compared to Temozolomide, Each Given With Radiation Therapy, for Newly-diagnosed Patients With Glioblastoma (GBM, a Malignant Brain Cancer) | Active, not recruiting | III | Brain Cancer | 560 | Nivolumab, Temozolomide, Radiotherapy | USA |
| 40 | NCT01213407 | Dendritic Cell Cancer Vaccine for High-grade Glioma | Completed | II | Glioblastoma Multiforme | 87 | Trivax, Temozolomide, Surgery, Radiotherapy | AU |
| 41 | NCT02529072 | Nivolumab With DC Vaccines for Recurrent Brain Tumors | Completed | I | Malignant Glioma, Astrocytoma | 6 | Nivolumab | USA |
| 42 | NCT03718767 | Nivolumab in Patients With IDH-Mutant Gliomas With and Without Hypermutator Phenotype | Recruiting | II | Malignant Glioma of Brain | 95 | Nivolumab | USA |
| 43 | NCT01480479 | Phase III Study of Rindopepimut/GM-CSF in Patients With Newly Diagnosed Glioblastoma | Completed | III | Malignant Glioma of Brain | 745 | Rindopepimut (CDX-110) with GM-CSF Temozolomide, KLH | USA |
| 44 | NCT01058850 | Phase I Rindopepimut After Conventional Radiation in Children w/Diffuse Intrinsic Pontine Gliomas | Terminated | I | Brain Cancer, Brain Stem Tumors | 3 | Rindopepimut | USA |
| 45 | NCT00045968 | Study of a Drug [DCVax®-L] to Treat Newly Diagnosed GBM Brain Cancer | Unknown | III | Glioblastoma | 348 | Dendritic cell immunotherapy | USA |
| 46 | NCT02808364 | Personalized Cellular Vaccine for Recurrent Glioblastoma (PERCELLVAC2) | Active, not recruiting | I | Glioblastoma | 10 | Personalized cellular vaccine | CHN |
| 47 | NCT02709616 | Personalized Cellular Vaccine for Glioblastoma (PERCELLVAC) | Active, not recruiting | 10 | Glioblastoma | 10 | Personalized cellular vaccine | CHN |
| 48 | NCT02209376 | Autologous T Cells Redirected to EGFRVIII-With a Chimeric Antigen Receptor in Patients With EGFRVIII+ Glioblastoma | Terminated | I | Patients With Residual or Reccurent EGFRvIII+ Glioma | 11 | CART-EGFRvIII T cells | USA |
| 49 | NCT03726515 | CART-EGFRvIII + Pembrolizumab in GBM | Active, not recruiting | I | Glioblastoma | 7 | CART-EGFRvIII T cells, Pembrolizumab | USA |
| 50 | NCT02664363 | EGFRvIII CAR T Cells for Newly-Diagnosed WHO Grade IV Malignant Glioma | Terminated | I | Glioblastoma, Gliosarcoma | 3 | EGFRvIII CAR T cells | USA |
| 51 | NCT01109095 | CMV-specific Cytotoxic T Lymphocytes Expressing CAR Targeting HER2 in Patients With GBM | Completed | I | Glioblastoma Multiforme | 16 | HER.CAR CMV-specific CTLs | USA |
| 52 | NCT02208362 | Genetically Modified T-cells in Treating Patients With Recurrent or Refractory Malignant Glioma | Recruiting | I | Glioblastoma, Recurrent Malignant Glioma | 92 | IL13Ralpha2-specific Hinge-optimized 41BB-co-stimulatory CAR Truncated CD19-expressing Autologous T-Lymphocytes | USA |
| 53 | NCT04003649 | IL13Ralpha2-Targeted Chimeric Antigen Receptor (CAR) T Cells With or Without Nivolumab and Ipilimumab in Treating Patients With Recurrent or Refractory Glioblastoma | Recruiting | I | Recurrent/Refractory Glioblastoma | 60 | IL13Ralpha2-specific Hinge-optimized 4-1BB-co-stimulatory CAR/Truncated CD19-expressing Autologous TN/MEM Cells, Ipilimumab, Nivolumab | USA |
| 54 | NCT03383978 | Intracranial Injection of NK-92/5.28.z Cells in Patients With Recurrent HER2-positive Glioblastoma | Recruiting | I | Glioblastoma | 30 | NK-92/5.28.z | DE |
| 55 | NCT03392545 | Combination of Immunization and Radiotherapy for Malignant Gliomas (InSituVac1) | Recruiting | I | High Grade Glioma, Glioblastoma, Glioma of Brainstem | 30 | Combined immune adjuvants and radiation | CHN |
| 56 | NCT03389230 | Memory-Enriched T Cells in Treating Patients With Recurrent or Refractory Grade III-IV Glioma | Recruiting | I | High Grade Glioma, Glioblastoma | 42 | HER2(EQ)BBζ/CD19t+ Tcm | USA |
| 57 | NCT03347097 | Adoptive Cell Therapy of Autologous TIL and PD1-TIL Cells for Patients With Glioblastoma Multiforme | Active, not recruiting | I | Glioblastoma Multiforme | 40 | TIL | CHN |
| 58 | NCT03344250 | Phase I EGFR BATs in Newly Diagnosed Glioblastoma | Recruiting | I | Glioblastoma Multiforme | 18 | EGFR BATs with SOC RT and TMZ | USA |
| 59 | NCT03170141 | Immunogene-modified T (IgT) Cells Against Glioblastoma Multiforme | Enrolling by invitation | I | Glioblastoma Multiforme | 20 | Antigen-specific IgT cells | CHN |
| 60 | NCT02937844 | Pilot Study of Autologous Chimeric Switch Receptor Modified T Cells in Recurrent Glioblastoma Multiforme | Unknown | I | Glioblastoma Multiforme | 20 | Anti-PD-L1 CSR T cells, Cyclophosphamide, Fludarabine | CHN |
| 61 | NCT02799238 | Autologuos Lymphoid Effector Cells Specific Against Tumour (ALECSAT) as Add on to Standard of Care in Patients With Glioblastoma | Completed | II | Glioblastoma | 62 | ALECSAT, Radiotherapy, Temozolomide | SE |
| 62 | NCT02060955 | Randomized Phase 2 Study to Investigate Efficacy of ALECSAT in Patients With GBM Measured Compared to Avastin/Irinotecan | Terminated | II | Glioblastoma Multiforme | 25 | ALECSAT, Bevacizumab/Irinotecan | DK |
| 63 | NCT01588769 | A Phase I Study to Investigate Tolerability and Efficacy of ALECSAT Administered to Glioblastoma Multiforme Patients | Completed | I | Glioblastoma Multiforme | 23 | ALECSAT cell based immunotherapy | DK |
| 64 | NCT01454596 | CAR T Cell Receptor Immunotherapy Targeting EGFRvIII for Patients With Malignant Gliomas Expressing EGFRvIII | Completed | I, II | Malignant Glioma, Glioblastoma, Gliosarcoma | 18 | Epidermal growth factor receptor(EGFRv)III Chimeric antigen receptor (CAR) transduced PBL, Aldesleukin, Fludarabine, Cyclophosphamide | USA |
| 65 | NCT01144247 | Cellular Immunotherapy Study for Brain Cancer | Completed | I | Malignant Glioma of Brain | 10 | Alloreactive CTL | USA |
| 66 | NCT01082926 | Phase I Study of Cellular Immunotherapy for Recurrent/Refractory Malignant Glioma Using Intratumoral Infusions of GRm13Z40-2, An Allogeneic CD8+ Cytolytic T-Cell Line Genetically Modified to Express the IL 13-Zetakine and HyTK and to be Resistant to Glucocorticoids, in Combination With Interleukin-2 | Completed | I | Malignant Glioma of Brain | 6 | Therapeutic allogeneic lymphocytes, Aldesleukin | USA |
| 67 | NCT00730613 | Cellular Adoptive Immunotherapy Using Genetically Modified T-Lymphocytes in Treating Patients With Recurrent or Refractory High-Grade Malignant Glioma | Completed | I | Central Nervous System Tumors | 3 | Therapeutic autologous lymphocytes | NA |
| 68 | NCT00331526 | Cellular Adoptive Immunotherapy in Treating Patients With Glioblastoma Multiforme | Completed | II | Central Nervous System Tumors | 83 | Aldesleukin, Therapeutic autologous lymphocytes, Adjuvant therapy, Surgery | USA |
| 69 | NCT00004024 | Biological Therapy Following Surgery and Radiation Therapy in Treating Patients With Primary or Recurrent Astrocytoma or Oligodendroglioma | Completed | II | Central Nervous System Tumors | 60 | Aldesleukin, Autologous tumor cell vaccine, Muromonab-CD3, Sargramostim, Therapeutic autologous lymphocytes, Surgical procedure, Radiation therapy | USA |
| Immunotherapies | |||
|---|---|---|---|
| Active | Checkpoint Inhibitors | Alkylating agent | TMZ |
| MAbs | BVZ, Nivolumab | ||
| Vaccine | Rindopepimut DCVax-Brain PerCellVac2 | ||
| Adoptive | T cell | TCR transgenic T | |
| CAR T | EGFRIII IL-13Ra2 HER2 EphA2 | ||
| NK cell | Allogenic NK | ||
| Anti-KIR Abs | |||
| ADCC | |||
| DNRII | |||
| NK exosomes | |||
| NKT | Autologous NKT, autologous mature DC cultured with NKT ligand α-galactosyl ceramide | ||
| Hybrid | ALECSAT | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giotta Lucifero, A.; Luzzi, S. Against the Resilience of High-Grade Gliomas: The Immunotherapeutic Approach (Part I). Brain Sci. 2021, 11, 386. https://doi.org/10.3390/brainsci11030386
Giotta Lucifero A, Luzzi S. Against the Resilience of High-Grade Gliomas: The Immunotherapeutic Approach (Part I). Brain Sciences. 2021; 11(3):386. https://doi.org/10.3390/brainsci11030386
Chicago/Turabian StyleGiotta Lucifero, Alice, and Sabino Luzzi. 2021. "Against the Resilience of High-Grade Gliomas: The Immunotherapeutic Approach (Part I)" Brain Sciences 11, no. 3: 386. https://doi.org/10.3390/brainsci11030386
APA StyleGiotta Lucifero, A., & Luzzi, S. (2021). Against the Resilience of High-Grade Gliomas: The Immunotherapeutic Approach (Part I). Brain Sciences, 11(3), 386. https://doi.org/10.3390/brainsci11030386