
Endoscopic Bilateral Optic Nerve Decompression for Treatment of Idiopathic Intracranial Hypertension


Abstract
:1. Introduction
2. Materials and Methods
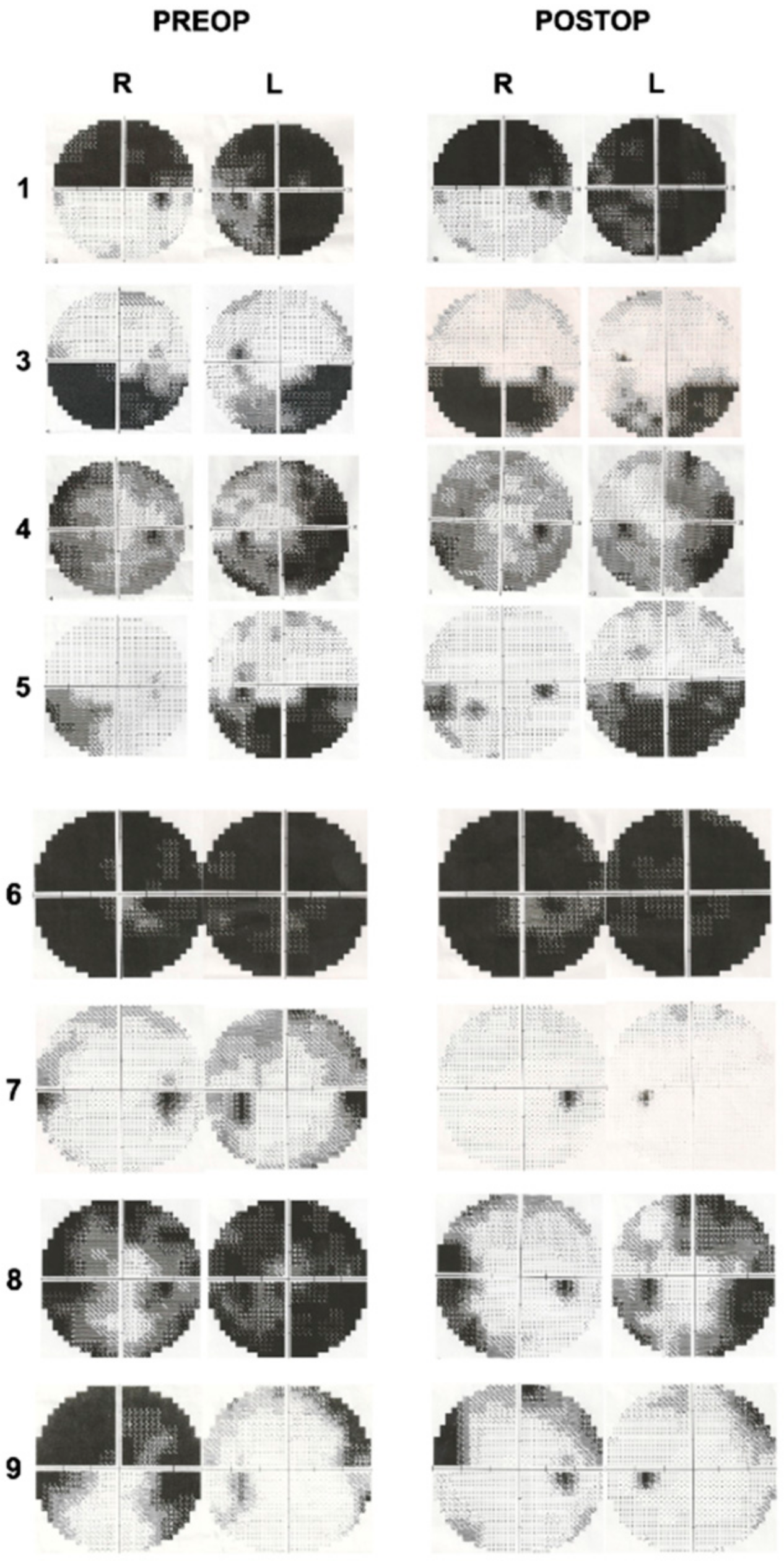
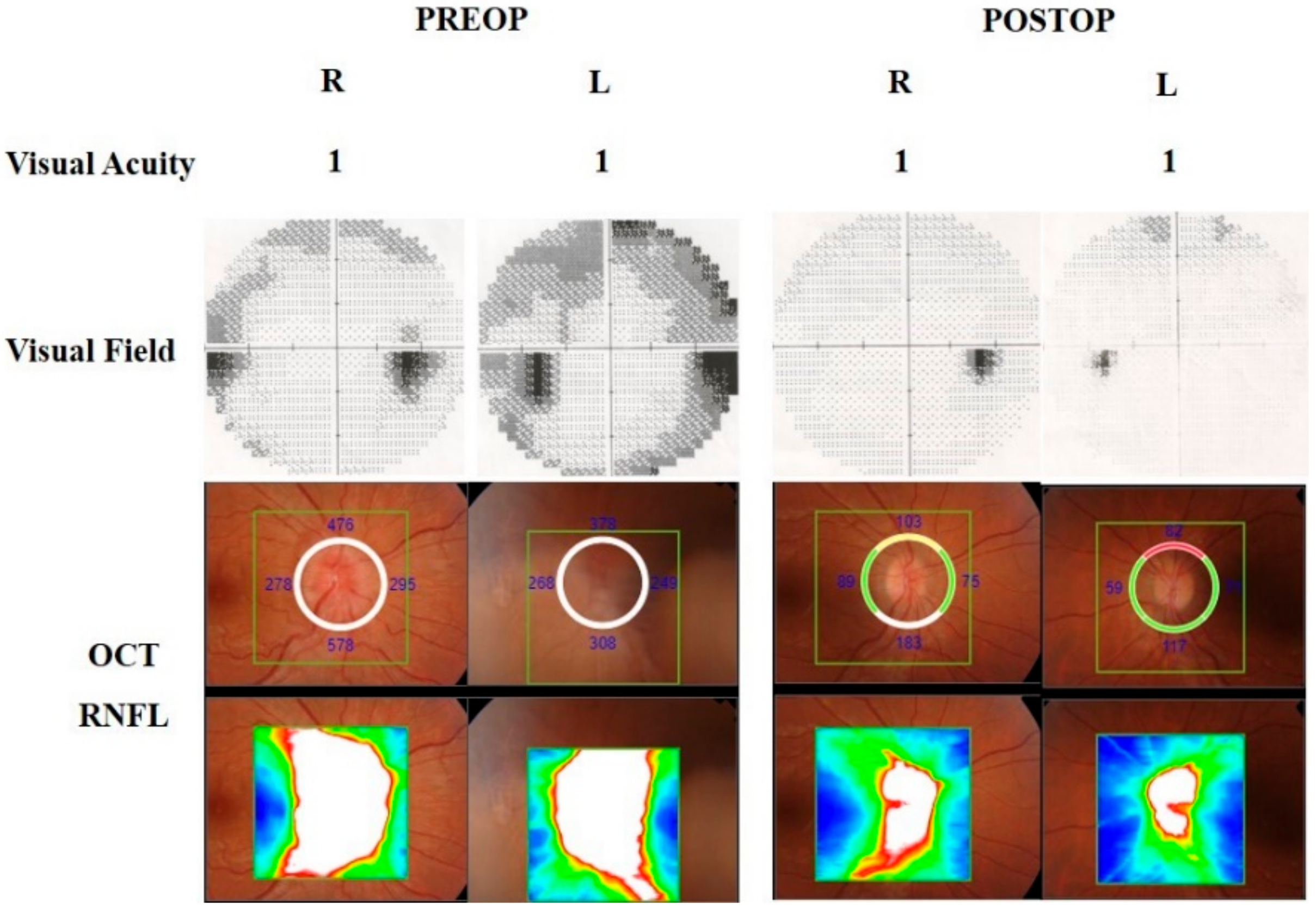
2.1. Ophthalmological Examinations
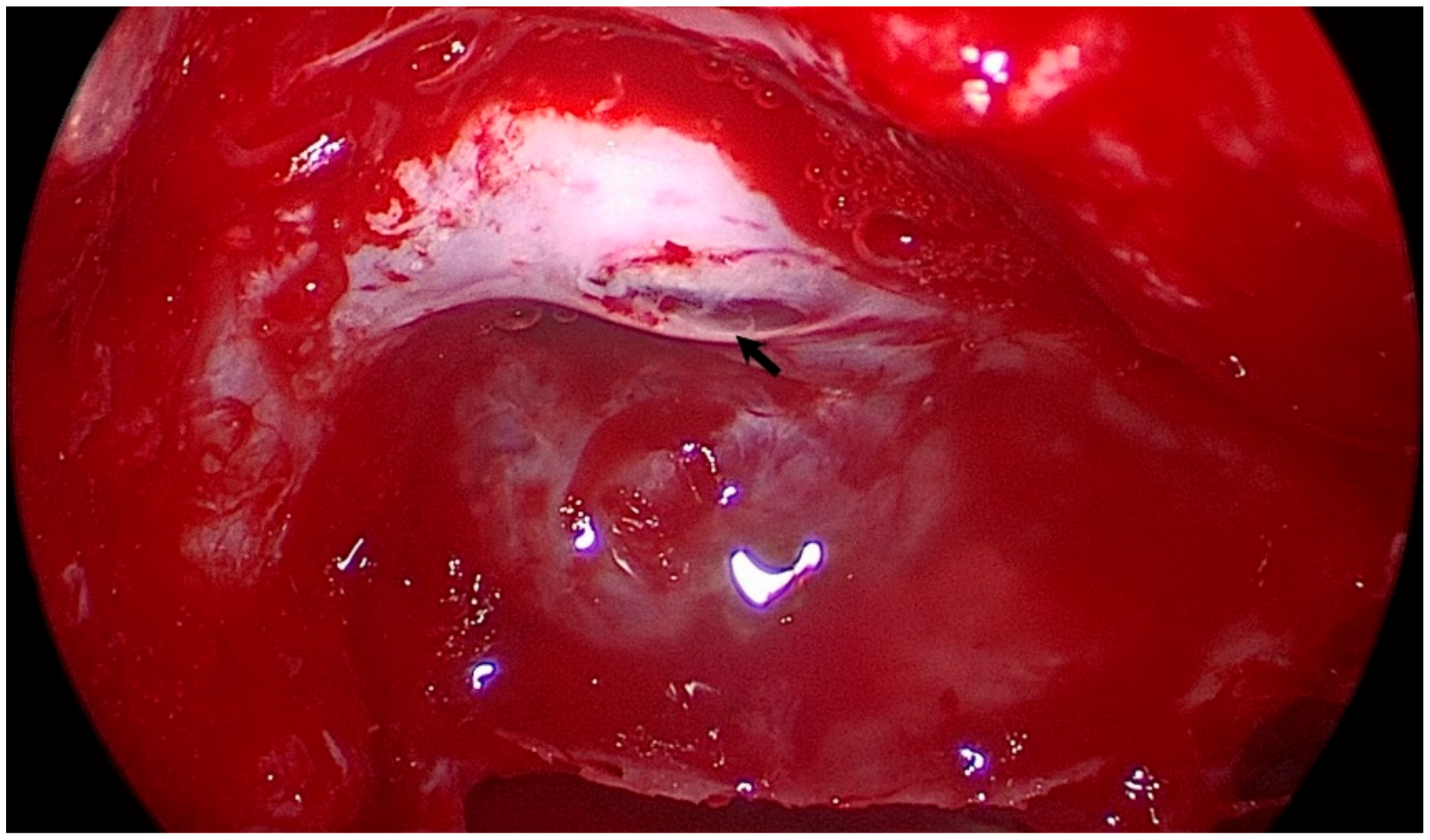
2.2. Surgical Technique
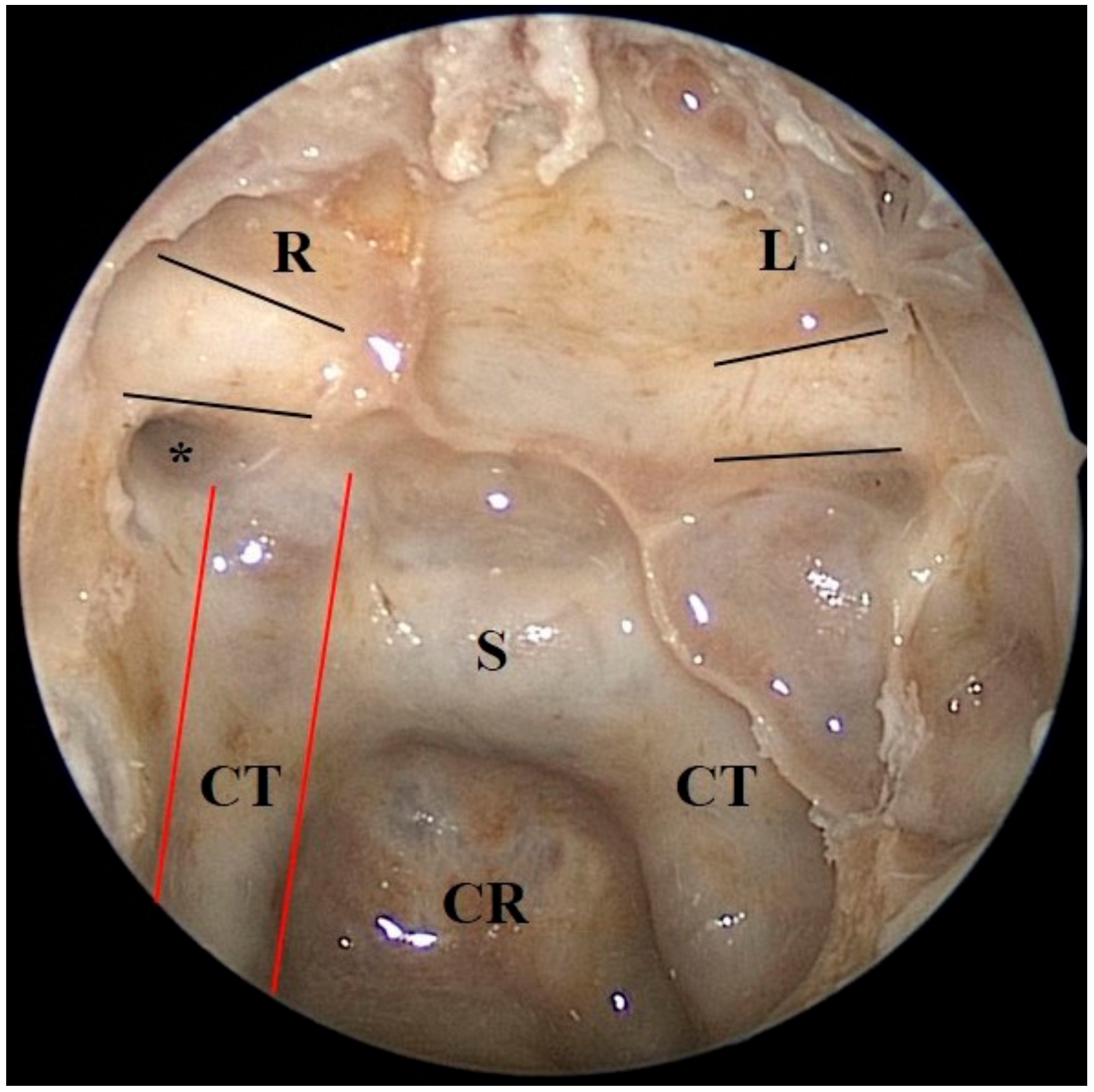
2.3. Cadaveric Demonstration
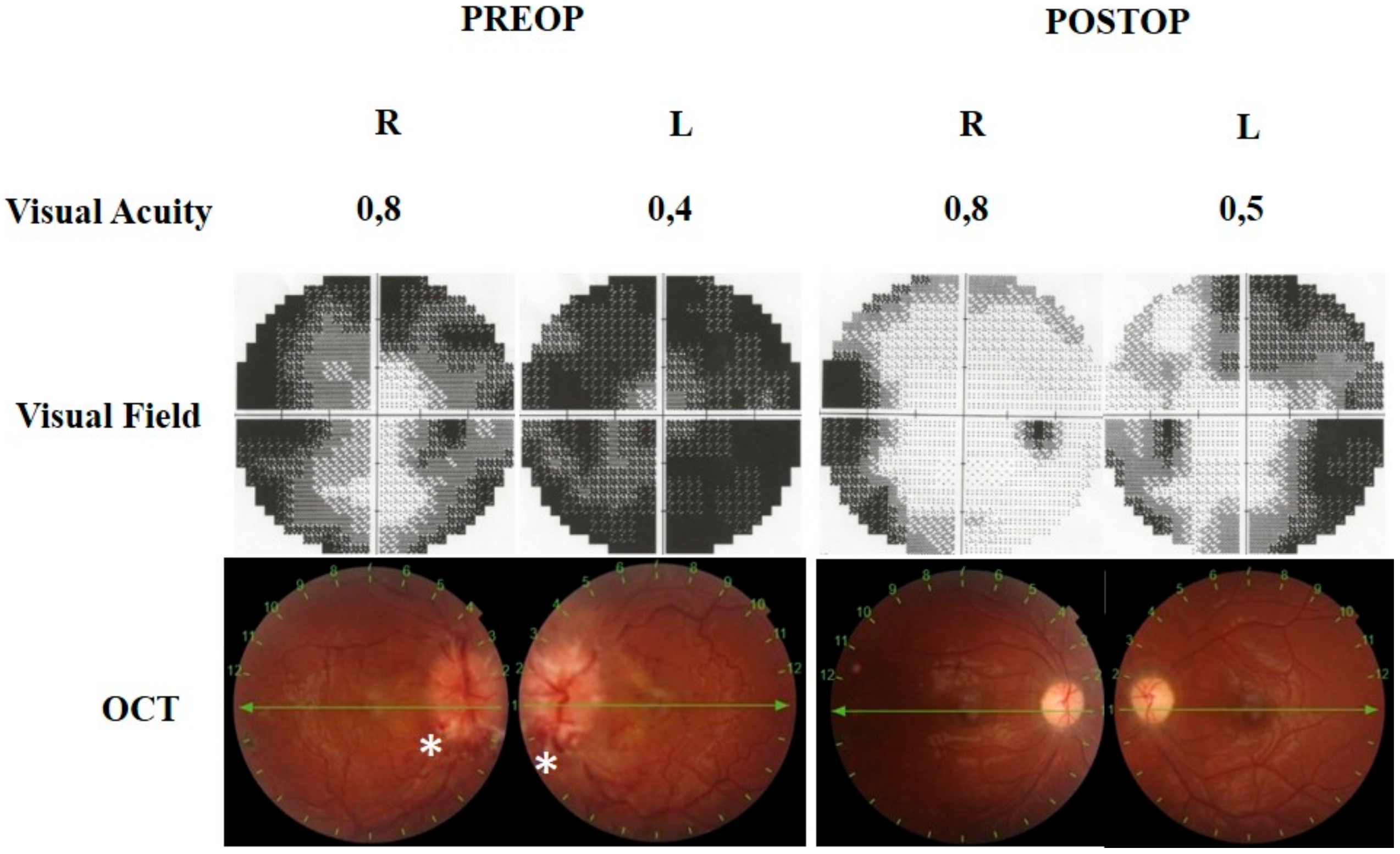
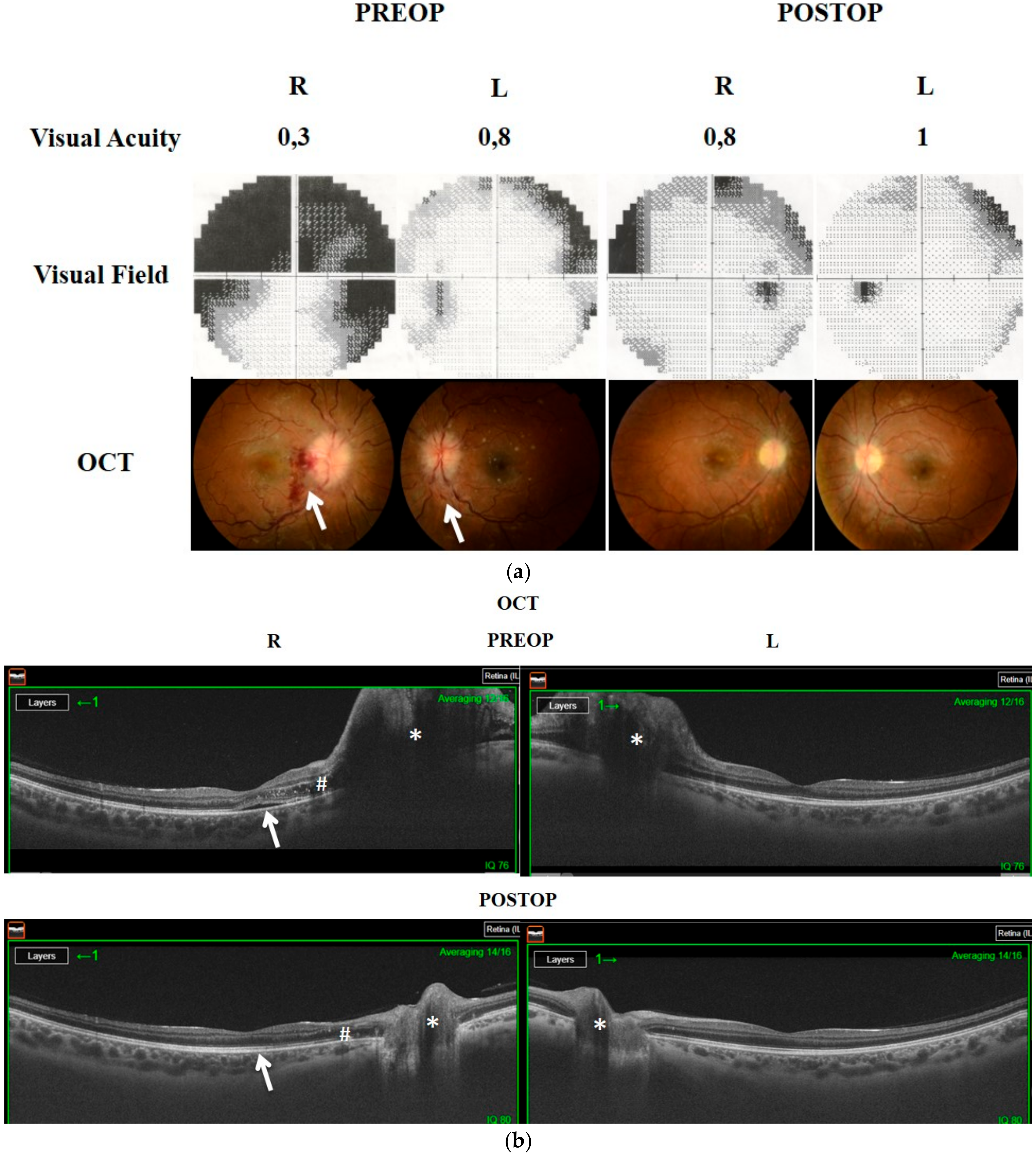
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Gilbert, A.L.; Chwalisz, B.; Mallery, R. Complications of Optic Nerve Sheath Fenestration as a Treatment for Idiopathic Intracranial Hypertension. Semin. Ophthalmol. 2018, 33, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Durcan, F.J.; Corbett, J.J.; Wall, M. The incidence of pseudotumor cerebri. Population studies in Iowa and Louisiana. Arch. Neurol. 1988, 45, 875–877. [Google Scholar] [CrossRef]
- Eggenberger, E.R.; Miller, N.R.; Vitale, S. Lumboperitoneal shunt for the treatment of pseudotumor cerebri. Neurology 1996, 46, 1524–1530. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K.; Gupta, A.; Kumar, S.; Lal, V. Endoscopic endonasal management of pseudotumor cerebri: Is it effective? Laryngoscope 2007, 117, 1138–1142. [Google Scholar] [CrossRef]
- Digre, K.B. Imaging characteristics of IIH: Are they reliable? Cephalalgia 2013, 33, 1067–1069. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, J.; Huppertz, H.J.; Schmidt, C.; Kunte, H.; Harms, L.; Klingebiel, R.; Wiener, E. Morphometric and volumetric MRI changes in idiopathic intracranial hypertension. Cephalalgia 2013, 33, 1075–1084. [Google Scholar] [CrossRef] [PubMed]
- Radhakrishnan, K.; Ahlskog, J.E.; Cross, S.A.; Kurland, L.T.; O’Fallon, W.M. Idiopathic intracranial hypertension (pseudotumor cerebri). Descriptive epidemiology in Rochester, Minn, 1976 to 1990. Arch. Neurol. 1993, 50, 78–80. [Google Scholar] [CrossRef] [PubMed]
- Portelli, M.; Papageorgiou, P.N. An update on idiopathic intracranial hypertension. Acta Neurochir. 2017, 159, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Tarrats, L.; Hernandez, G.; Busquets, J.M.; Portela, J.C.; Serrano, L.A.; Gonzalez-Sepulveda, L.; Sanchez-Perez, J.R. Outcomes of endoscopic optic nerve decompression in patients with idiopathic intracranial hypertension. Int. Forum Allergy Rhinol. 2017, 7, 615–623. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, A.K.; Singh, S.; Khatri, D.; Jaiswal, A.K.; Sankar, R.; Paliwal, V.K.; Neyaz, Z.; Sharma, K.; Behari, S. Endoscopic Endonasal Optic Nerve Decompression with Durotomy: Pis Aller in the Mind of a Blind. Neurol. India 2020, 68, 54–60. [Google Scholar] [CrossRef]
- McGeeney, B.E.; Friedman, D.I. Pseudotumor cerebri pathophysiology. Headache 2014, 54, 445–458. [Google Scholar] [CrossRef]
- Burgett, R.A.; Purvin, V.A.; Kawasaki, A. Lumboperitoneal shunting for pseudotumor cerebri. Neurology 1997, 49, 734–739. [Google Scholar] [CrossRef]
- Sinclair, A.J.; Kuruvath, S.; Sen, D.; Nightingale, P.G.; Burdon, M.A.; Flint, G. Is cerebrospinal fluid shunting in idiopathic intracranial hypertension worthwhile? A 10-year review. Cephalalgia 2011, 31, 1627–1633. [Google Scholar] [CrossRef] [PubMed]
- Mudumbai, R.C. Optic nerve sheath fenestration: Indications, techniques, mechanisms and, results. Int. Ophthalmol. Clin. 2014, 54, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Sencer, A.; Akcakaya, M.O.; Basaran, B.; Yorukoglu, A.G.; Aydoseli, A.; Aras, Y.; Sencan, F.; Satana, B.; Aslan, I.; Unal, O.F.; et al. Unilateral endoscopic optic nerve decompression for idiopathic intracranial hypertension: A series of 10 patients. World Neurosurg. 2014, 82, 745–750. [Google Scholar] [CrossRef] [PubMed]
- Kalyvas, A.; Neromyliotis, E.; Skandalakis, G.S.; Koutsarnakis, C.; Komaitis, S.; Zadeh, G.; Gentili, F.; Gobin, P.Y.; Stranjalis, G.; Patsalides, A. A Systematic Review of Surgical Treatments of Idiopathic Intracranial Hypertension (IIH): Should VSS Be Regarded as the First Line Surgical Modality? Neurosurgery 2020, 67 (Suppl. S1), nyaa447_315. [Google Scholar]
- Gupta, A.K.; Ganth, M.G.; Gupta, A. Modified endoscopic optic nerve decompression in idiopathic intracranial hypertension. J. Laryngol. Otol. 2003, 117, 501–502. [Google Scholar] [CrossRef] [PubMed]
- Keltner, J.L. Optic nerve sheath decompression. How does it work? Has its time come? Arch. Ophthalmol. 1988, 106, 1365–1369. [Google Scholar] [CrossRef] [PubMed]
- Pircher, A.; Montali, M.; Pircher, J.; Berberat, J.; Remonda, L.; Killer, H.E. Perioptic Cerebrospinal Fluid Dynamics in Idiopathic Intracranial Hypertension. Front. Neurol. 2018, 9, 506. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Age | Sex | BMI | Headache | Visual Acuity (BCVA) R/L | Visual Field Defect | Fundoscopic Examination (Papilledema/OA) |
|---|---|---|---|---|---|---|---|
| 1 | 72 | Male | >30 | − | 0.4/0.2 | + | −/+ |
| 2 | 54 | Female | >30 | + | LP/FC | NA | −/+ |
| 3 | 37 | Female | >30 | − | 0.5/0.6 | + | +/+ |
| 4 | 54 | Female | >30 | − | 0.7/1 | + | −/+ |
| 5 | 47 | Female | >30 | + | 0.9/0.9 | + | +/+ |
| 6 | 23 | Female | >30 | + | 0.6/0.6 | + | +/+ |
| 7 | 32 | Female | <30 | + | 1/1 | + | +/− |
| 8 | 21 | Male | <30 | + | 0.8/0.4 | + | +/− |
| 9 | 28 | Female | >30 | + | 0.3/0.8 | + | +/− |
| Patient | Headache | Visual Acuity (BCVA) | Visual Field Defect | Fundoscopic Examination |
|---|---|---|---|---|
| R/L | Papilledema/OA | |||
| 1 | − | 0.5/0.2 | Unchanged | Unchanged |
| 2 | Improved | LP/0.05 | NA | Unchanged |
| 3 | − | 0.7/0.8 | Unchanged | Resolved/+ |
| 4 | − | 0.7/1 | Improved | Unchanged |
| 5 | Improved | 1/0.9 | Improved | Resolved/+ |
| 6 | Improved | 0.9/0.9 | Unchanged | Resolved/+ |
| 7 | Improved | 1/1 | Improved | Resolved/− |
| 8 | Improved | 0.8/0.5 | Improved | Resolved/− |
| 9 | Improved | 0.8/1 | Improved | Resolved/− |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Göksu, E.; Bozkurt, B.; İlhan, D.; Özak, A.; Çırak, M.; Yağmurlu, K. Endoscopic Bilateral Optic Nerve Decompression for Treatment of Idiopathic Intracranial Hypertension. Brain Sci. 2021, 11, 324. https://doi.org/10.3390/brainsci11030324
Göksu E, Bozkurt B, İlhan D, Özak A, Çırak M, Yağmurlu K. Endoscopic Bilateral Optic Nerve Decompression for Treatment of Idiopathic Intracranial Hypertension. Brain Sciences. 2021; 11(3):324. https://doi.org/10.3390/brainsci11030324
Chicago/Turabian StyleGöksu, Ethem, Baran Bozkurt, Deniz İlhan, Ahmet Özak, Musa Çırak, and Kaan Yağmurlu. 2021. "Endoscopic Bilateral Optic Nerve Decompression for Treatment of Idiopathic Intracranial Hypertension" Brain Sciences 11, no. 3: 324. https://doi.org/10.3390/brainsci11030324
APA StyleGöksu, E., Bozkurt, B., İlhan, D., Özak, A., Çırak, M., & Yağmurlu, K. (2021). Endoscopic Bilateral Optic Nerve Decompression for Treatment of Idiopathic Intracranial Hypertension. Brain Sciences, 11(3), 324. https://doi.org/10.3390/brainsci11030324