
Relationships between Freezing of Gait Severity and Cognitive Deficits in Parkinson’s Disease


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants and Identification of PDFOG+
2.2. Clinical, Motor, and Cognitive Assessments
2.3. Statistical Analysis
3. Results
3.1. Differences in Demographic and Clinical Assessments
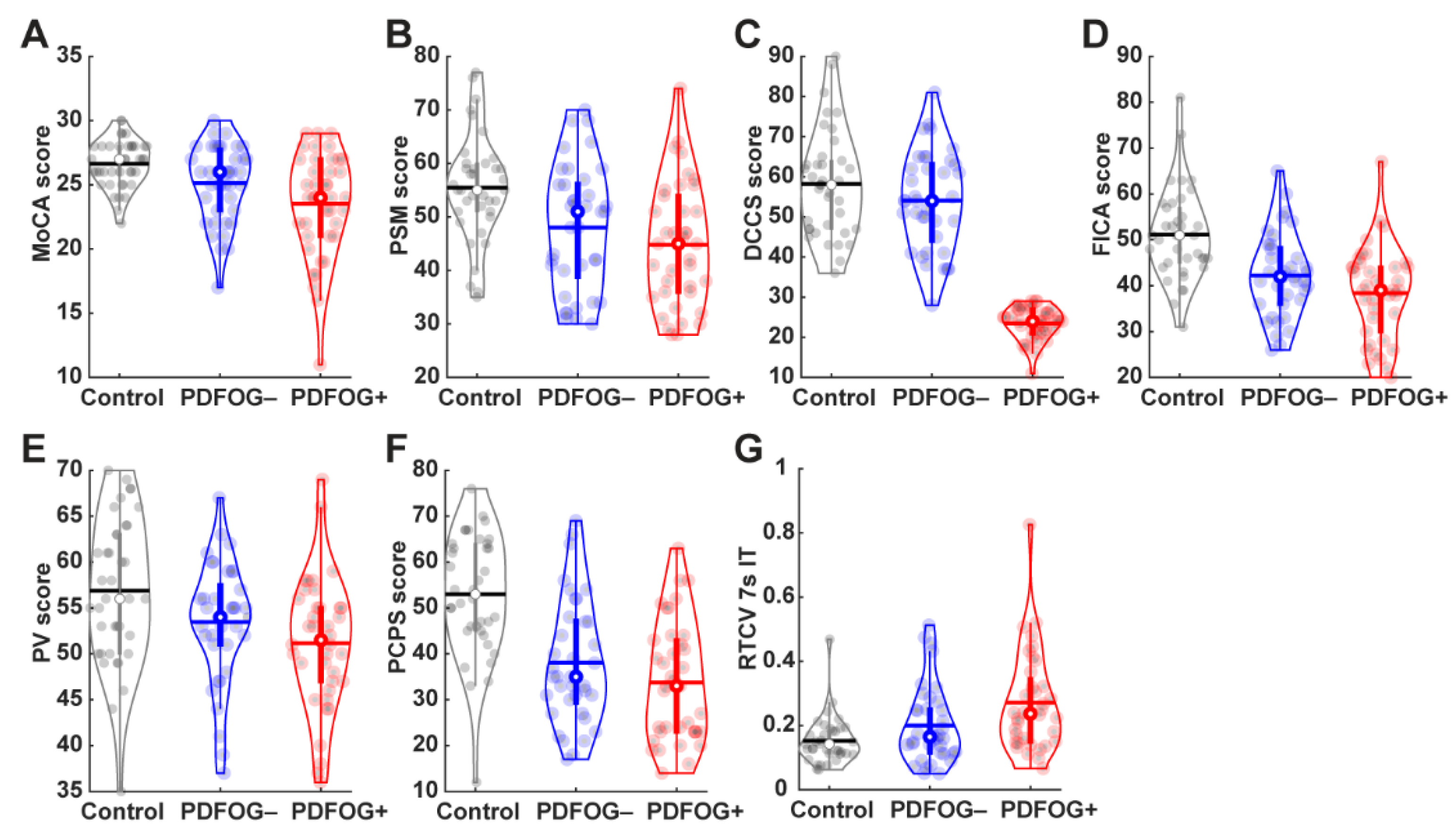
3.2. Differences in Cognitive Measurements
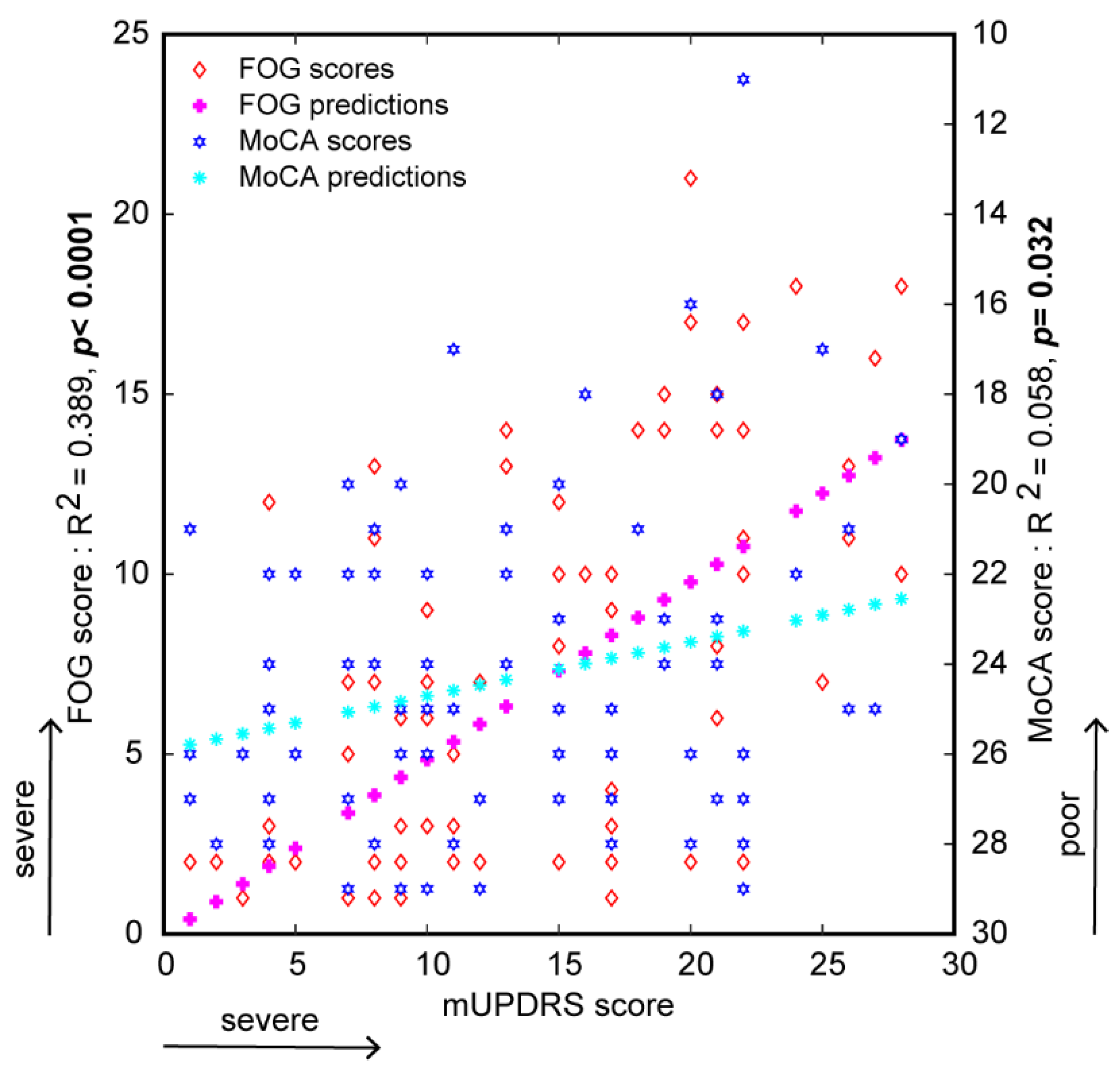
3.3. Relationship between FOG Severity and Cognitive Measurements
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bloem, B.R.; Hausdorff, J.M.; Visser, J.E.; Giladi, N. Falls and freezing of gait in Parkinson’s disease: A review of two interconnected, episodic phenomena. Mov. Disord. 2004, 19, 871–884. [Google Scholar] [CrossRef]
- Lewis, S.J.; Barker, R.A. A pathophysiological model of freezing of gait in Parkinson’s disease. Parkinsonism Relat. Disord. 2009, 15, 333–338. [Google Scholar] [CrossRef]
- Huang, Y.F.; Cherng, Y.G.; Hsu, S.P.; Yeh, C.C.; Chou, Y.C.; Wu, C.H.; Chen, T.L.; Liao, C.C. Risk and adverse outcomes of fractures in patients with Parkinson’s disease: Two nationwide studies. Osteoporos. Int. 2015, 26, 1723–1732. [Google Scholar] [CrossRef]
- Giladi, N.; McDermott, M.P.; Fahn, S.; Przedborski, S.; Jankovic, J.; Stern, M.; Tanner, C.; Parkinson Study Group. Freezing of gait in PD: Prospective assessment in the DATATOP cohort. Neurology 2001, 56, 1712–1721. [Google Scholar] [CrossRef]
- Singh, A. Oscillatory activity in the cortico-basal ganglia-thalamic neural circuits in Parkinson’s disease. Eur. J. Neurosci. 2018, 48, 2869–2878. [Google Scholar] [CrossRef]
- Singh, A.; Plate, A.; Kammermeier, S.; Mehrkens, J.H.; Ilmberger, J.; Bötzel, K. Freezing of gait-related oscillatory activity in the human subthalamic nucleus. Basal Ganglia 2013, 3, 25–32. [Google Scholar] [CrossRef]
- Elble, R.J. Gait and dementia: Moving beyond the notion of gait apraxia. J. Neural. Transm 2007, 114, 1253–1258. [Google Scholar] [CrossRef]
- Alster, P.; Madetko, N.; Koziorowski, D.; Friedman, A. Progressive Supranuclear Palsy-Parkinsonism Predominant (PSP-P)-A Clinical Challenge at the Boundaries of PSP and Parkinson’s Disease (PD). Front. Neurol. 2020, 11, 180. [Google Scholar] [CrossRef]
- Osaki, Y.; Morita, Y.; Miyamoto, Y.; Furuta, K.; Furuya, H. Freezing of gait is an early clinical feature of progressive supranuclear palsy. Neurol. Clin. Neurosci. 2017, 5, 86–90. [Google Scholar] [CrossRef] [Green Version]
- Gurevich, T.; Giladi, N. Freezing of gait in multiple system atrophy (MSA). Parkinsonism Relat. Disord. 2003, 9, 169–174. [Google Scholar] [CrossRef]
- Macht, M.; Kaussner, Y.; Moller, J.C.; Stiasny-Kolster, K.; Eggert, K.M.; Kruger, H.P.; Ellgring, H. Predictors of freezing in Parkinson’s disease: A survey of 6620 patients. Mov. Disord. 2007, 22, 953–956. [Google Scholar] [CrossRef]
- Martens, K.A.E.; Shine, J.M.; Walton, C.C.; Georgiades, M.J.; Gilat, M.; Hall, J.M.; Muller, A.J.; Szeto, J.Y.Y.; Lewis, S.J.G. Evidence for subtypes of freezing of gait in Parkinson’s disease. Mov. Disord. 2018, 33, 1174–1178. [Google Scholar] [CrossRef]
- Kelly, V.E.; Eusterbrock, A.J.; Shumway-Cook, A. A review of dual-task walking deficits in people with Parkinson’s disease: Motor and cognitive contributions, mechanisms, and clinical implications. Parkinsons Dis. 2012, 2012, 918719. [Google Scholar] [CrossRef] [Green Version]
- Morris, R.; Lord, S.; Lawson, R.A.; Coleman, S.; Galna, B.; Duncan, G.W.; Khoo, T.K.; Yarnall, A.J.; Burn, D.J.; Rochester, L. Gait Rather Than Cognition Predicts Decline in Specific Cognitive Domains in Early Parkinson’s Disease. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 1656–1662. [Google Scholar] [CrossRef] [Green Version]
- Morris, R.; Smulders, K.; Peterson, D.S.; Mancini, M.; Carlson-Kuhta, P.; Nutt, J.G.; Horak, F.B. Cognitive function in people with and without freezing of gait in Parkinson’s disease. NPJ Parkinsons Dis. 2020, 6, 9. [Google Scholar] [CrossRef]
- Amboni, M.; Cozzolino, A.; Longo, K.; Picillo, M.; Barone, P. Freezing of gait and executive functions in patients with Parkinson’s disease. Mov. Disord. 2008, 23, 395–400. [Google Scholar] [CrossRef]
- Singh, A.; Cole, R.C.; Espinoza, A.I.; Brown, D.; Cavanagh, J.F.; Narayanan, N.S. Frontal theta and beta oscillations during lower-limb movement in Parkinson’s disease. Clin. Neurophysiol. 2020, 131, 694–702. [Google Scholar] [CrossRef]
- Horta-Barba, A.; Pagonabarraga, J.; Martinez-Horta, S.; Busteed, L.; Pascual-Sedano, B.; Illan-Gala, I.; Marin-Lahoz, J.; Aracil-Bolanos, I.; Perez-Perez, J.; Sampedro, F.; et al. Cognitive and behavioral profile of progressive supranuclear palsy and its phenotypes. J. Neurol. 2021, 268, 3400–3408. [Google Scholar] [CrossRef]
- Giagkou, N.; Hoglinger, G.U.; Stamelou, M. Progressive supranuclear palsy. Int. Rev. Neurobiol. 2019, 149, 49–86. [Google Scholar] [CrossRef]
- Rezvanian, S.; Litvan, I.; Standaert, D.; Jankovic, J.; Reich, S.G.; Hall, D.; Shprecher, D.R.; Bordelon, Y.; Dubinsky, R.; Kluger, B. Understanding the relationship between freezing of gait and other progressive supranuclear palsy features. Parkinsonism Relat. Disord. 2020, 78, 56–60. [Google Scholar] [CrossRef]
- Walton, C.C.; Shine, J.M.; Mowszowski, L.; Naismith, S.L.; Lewis, S.J. Freezing of gait in Parkinson’s disease: Current treatments and the potential role for cognitive training. Restor. Neurol. Neurosci. 2014, 32, 411–422. [Google Scholar] [CrossRef]
- Snijders, A.H.; Leunissen, I.; Bakker, M.; Overeem, S.; Helmich, R.C.; Bloem, B.R.; Toni, I. Gait-related cerebral alterations in patients with Parkinson’s disease with freezing of gait. Brain 2011, 134, 59–72. [Google Scholar] [CrossRef]
- Cohen, R.G.; Klein, K.A.; Nomura, M.; Fleming, M.; Mancini, M.; Giladi, N.; Nutt, J.G.; Horak, F.B. Inhibition, executive function, and freezing of gait. J. Parkinsons Dis. 2014, 4, 111–122. [Google Scholar] [CrossRef] [Green Version]
- Yao, Z.; Shao, Y.; Han, X. Freezing of gait is associated with cognitive impairment in patients with Parkinson disease. Neurosci. Lett. 2017, 656, 126–130. [Google Scholar] [CrossRef]
- Giladi, N.; Tal, J.; Azulay, T.; Rascol, O.; Brooks, D.J.; Melamed, E.; Oertel, W.; Poewe, W.H.; Stocchi, F.; Tolosa, E. Validation of the freezing of gait questionnaire in patients with Parkinson’s disease. Mov. Disord. 2009, 24, 655–661. [Google Scholar] [CrossRef]
- Movement Disorder Society Task Force on Rating Scales for Parkinson’s Disease. The Unified Parkinson’s Disease Rating Scale (UPDRS): Status and recommendations. Mov. Disord. 2003, 18, 738–750. [Google Scholar] [CrossRef]
- Singh, A.; Cole, R.; Espinoza, A.I.; Evans, A.; Cao, S.; Cavanagh, J.F.; Narayanan, N.S. Timing variability and midfrontal~ 4 Hz rhythms correlate with cognition in Parkinson’s disease. npj Parkinsons Dis. 2021, 7, 14. [Google Scholar] [CrossRef]
- Weintraub, S.; Dikmen, S.S.; Heaton, R.K.; Tulsky, D.S.; Zelazo, P.D.; Slotkin, J.; Carlozzi, N.E.; Bauer, P.J.; Wallner-Allen, K.; Fox, N.; et al. The cognition battery of the NIH toolbox for assessment of neurological and behavioral function: Validation in an adult sample. J. Int. Neuropsychol. Soc. 2014, 20, 567–578. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.; Trapp, N.T.; De Corte, B.; Cao, S.; Kingyon, J.; Boes, A.D.; Parker, K.L. Cerebellar Theta Frequency Transcranial Pulsed Stimulation Increases Frontal Theta Oscillations in Patients with Schizophrenia. Cerebellum 2019, 18, 489–499. [Google Scholar] [CrossRef]
- Ge, H.L.; Chen, X.Y.; Lin, Y.X.; Ge, T.J.; Yu, L.H.; Lin, Z.Y.; Wu, X.Y.; Kang, D.Z.; Ding, C.Y. The prevalence of freezing of gait in Parkinson’s disease and in patients with different disease durations and severities. Chin. Neurosurg. J. 2020, 6, 17. [Google Scholar] [CrossRef]
- Roheger, M.; Kalbe, E.; Liepelt-Scarfone, I. Progression of Cognitive Decline in Parkinson’s Disease. J. Parkinsons Dis. 2018, 8, 183–193. [Google Scholar] [CrossRef] [Green Version]
- Vercruysse, S.; Devos, H.; Munks, L.; Spildooren, J.; Vandenbossche, J.; Vandenberghe, W.; Nieuwboer, A.; Heremans, E. Explaining freezing of gait in Parkinson’s disease: Motor and cognitive determinants. Mov. Disord. 2012, 27, 1644–1651. [Google Scholar] [CrossRef]
- Singh, A.; Kammermeier, S.; Plate, A.; Mehrkens, J.H.; Ilmberger, J.; Botzel, K. Pattern of local field potential activity in the globus pallidus internum of dystonic patients during walking on a treadmill. Exp. Neurol. 2011, 232, 162–167. [Google Scholar] [CrossRef]
- Wang, D.D.; Choi, J.T. Brain Network Oscillations during Gait in Parkinson’s Disease. Front. Hum. Neurosci. 2020, 14, 568703. [Google Scholar] [CrossRef]
- Singh, A.; Richardson, S.P.; Narayanan, N.; Cavanagh, J.F. Mid-frontal theta activity is diminished during cognitive control in Parkinson’s disease. Neuropsychologia 2018, 117, 113–122. [Google Scholar] [CrossRef]
- Lewis, S.J.; Slabosz, A.; Robbins, T.W.; Barker, R.A.; Owen, A.M. Dopaminergic basis for deficits in working memory but not attentional set-shifting in Parkinson’s disease. Neuropsychologia 2005, 43, 823–832. [Google Scholar] [CrossRef]
- Garcia-Ruiz, P.J. Gait disturbances in Parkinson disease. Did freezing of gait exist before levodopa? Historical review. J. Neurol. Sci. 2011, 307, 15–17. [Google Scholar] [CrossRef]
- Huang, C.; Chu, H.; Zhang, Y.; Wang, X. Deep Brain Stimulation to Alleviate Freezing of Gait and Cognitive Dysfunction in Parkinson’s Disease: Update on Current Research and Future Perspectives. Front. Neurosci. 2018, 12, 29. [Google Scholar] [CrossRef]
- Mori, F.; Okada, K.; Nomura, T.; Kobayashi, Y. The Pedunculopontine Tegmental Nucleus as a Motor and Cognitive Interface between the Cerebellum and Basal Ganglia. Front. Neuroanat. 2016, 10, 109. [Google Scholar] [CrossRef] [Green Version]
- Thevathasan, W.; Pogosyan, A.; Hyam, J.A.; Jenkinson, N.; Foltynie, T.; Limousin, P.; Bogdanovic, M.; Zrinzo, L.; Green, A.L.; Aziz, T.Z.; et al. Alpha oscillations in the pedunculopontine nucleus correlate with gait performance in parkinsonism. Brain 2012, 135, 148–160. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Measure | Control (n = 41) | PD (n = 80) | PDFOG− (n = 39) | PDFOG+ (n = 41) | Control vs. PD | PDFOG– vs. PDFOG+ |
|---|---|---|---|---|---|---|
| Independent t-Test | Independent t-Test | |||||
| Gender (M/F) $ | 23/18 | 56/24 | 26/13 | 30/11 | 0.12 | 0.52 |
| Age (years) | 71.3 ± 7.6 | 68.7 ± 8.0 | 68.4 ± 7.7 | 68.9 ± 8.3 | 1.77 (0.079) | −0.26 (0.795) |
| Education (years) | 16.6 ± 2.2 | 15.8 ± 3.2 | 15.6 ± 3.4 | 16.0 ± 3.1 | 1.35 (0.179) | −0.49 (0.623) |
| BAI | 1.8 ± 2.1 | 14.7 ± 11.0 | 9.5 ± 7.4 | 19.8 ± 11.6 | −7.46 (<0.001) *** | −4.7 (<0.001) *** |
| GDS | 0.7 ± 1.1 | 3.7 ± 3.2 | 2.7 ± 2.4 | 4.6 ± 3.6 | −5.64 (<0.001) *** | −2.73 (0.008) ** |
| Total FOG | - | 6.5 ± 5.7 | 1.6 ± 1.3 | 11.2 ± 4.1 | - | −13.71 (<0.001) *** |
| DD (years) | - | 5.15 ± 4.0 | 4.3 ± 3.2 | 5.9 ± 4.4 | - | −1.83 (0.072) |
| LEDD (mg) | - | 860.5 ± 450.3 | 710.6 ± 392.9 | 1003.0 ± 459.3 | - | −3.05 (0.003) ** |
| mUPDRS | - | 13.4 ± 7.2 | 9.4 ± 5.6 | 17.2 ± 6.6 | - | −5.71 (<0.001) *** |
| H and Y | - | 2.07 ± 0.9 | 1.5 ± 0.7 | 2.5 ± 0.8 | - | −4.89 (<0.001) *** |
| PDSS | - | 17.5 ± 10.0 | 13.1 ± 7.7 | 21.7 ± 10.3 | - | −4.26 (<0.001) *** |
| Control (n = 41) | PD (n = 80) | PDFOG− (n = 39) | PDFOG+ (n = 41) | Control vs. PD | PDFOG− vs. PDFOG+ | |||
|---|---|---|---|---|---|---|---|---|
| Independent t-Test | a ANCOVA | Independent t-Test | a ANCOVA | b ANCOVA | ||||
| Cognitive function: MoCA | ||||||||
| 26.6 ± 1.8 | 24.3 ± 3.6 | 25.1 ± 3 | 23.5 ± 4 | 3.9 (<0.001) *** | 14.53 (<0.001) *** | 2.05 (0.044) * | 4.55 (0.034) * | 4.7 (0.034) * |
| Episodic memory: PSM | ||||||||
| 55.5 ± 9.9 | 46.4 ± 11.7 | 48 ± 11.8 | 44.8 ± 11.6 | 4.11 (<0.001) *** | 23.74 (<0.001) *** | 1.2 (0.234) | 0.049 (0.487) | 0.43 (0.515) |
| Executive function/Attention: DCCS | ||||||||
| 58.2 ± 13.2 | 50.1 ± 12.3 | 54.1 ± 12.2 | 46.1 ± 11.1 | 3.26 (0.001) ** | 12.66 (0.001) *** | 2.94 (0.004) ** | 7.78 (0.007) ** | 7.44 (0.008) ** |
| Executive function/Attention: FICA | ||||||||
| 51.1 ± 9.8 | 40.3 ± 9.8 | 42.2 ± 9.1 | 38.4 ± 10.1 | 5.55 (<0.001) *** | 30.74 (<0.001) *** | 1.74 (0.087) | 1.64 (0.205) | 1.07 (0.304) |
| Language: PV | ||||||||
| 56.9 ± 7.9 | 52.3 ± 6.9 | 53.5 ± 6.5 | 51.2 ± 7.2 | 3.16 (0.002) ** | 7.76 (0.006) ** | 1.45 (0.151) | 1.21 (0.276) | 1.28 (0.262) |
| Processing speed: PCPS | ||||||||
| 53 ± 13 | 35.9 ± 13.3 | 38.1 ± 13.5 | 33.7 ± 12.9 | 6.49 (<0.001) *** | 44.87 (<0.001) *** | 1.44 (0.155) | 1.46 (0.232) | 1.53 (0.22) |
| Temporal processing/Working memory: RTCV | ||||||||
| 0.15 ± 0.07 | 0.23 ± 0.14 | 0.20 ± 0.12 | 0.27 ± 0.16 | −3.31 (0.001) ** | 14.34 (<0.001) *** | 2.2 (0.031) * | 2.98 (0.089) | 2.36 (0.129) |
| Variable | Spearman Correlation | Spearman Partial Correlation | |
|---|---|---|---|
| a Age, Gender, Education | b Age, Gender, Education, Disease Duration | ||
| Cognitive function | |||
| MoCA | −0.27 (0.015) * | −0.27 (0.021) * | −0.29 (0.01) ** |
| Episodic memory | |||
| PSM | −0.11 (0.33) | −0.05 (0.69) | −0.02 (0.852) |
| Executive function/Attention | |||
| DCCS | −0.28 (0.014) * | −0.26 (0.032) * | −0.25 (0.044) * |
| FICA | −0.20 (0.093) | −0.13 (0.313) | −0.09 (0.472) |
| Language | |||
| PV | −0.14 (0.22) | −0.07 (0.567) | −0.10 (0.439) |
| Processing speed | |||
| PCPS | −0.28 (0.015) * | −0.24 (0.05) * | −0.25 (0.043) * |
| Temporal processing/Working memory | |||
| RTCV | 0.36 (0.002) ** | 0.32 (0.009) ** | 0.29 (0.018) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scholl, J.L.; Espinoza, A.I.; Rai, W.; Leedom, M.; Baugh, L.A.; Berg-Poppe, P.; Singh, A. Relationships between Freezing of Gait Severity and Cognitive Deficits in Parkinson’s Disease. Brain Sci. 2021, 11, 1496. https://doi.org/10.3390/brainsci11111496
Scholl JL, Espinoza AI, Rai W, Leedom M, Baugh LA, Berg-Poppe P, Singh A. Relationships between Freezing of Gait Severity and Cognitive Deficits in Parkinson’s Disease. Brain Sciences. 2021; 11(11):1496. https://doi.org/10.3390/brainsci11111496
Chicago/Turabian StyleScholl, Jamie L., Arturo I. Espinoza, Wijdan Rai, Matt Leedom, Lee A. Baugh, Patti Berg-Poppe, and Arun Singh. 2021. "Relationships between Freezing of Gait Severity and Cognitive Deficits in Parkinson’s Disease" Brain Sciences 11, no. 11: 1496. https://doi.org/10.3390/brainsci11111496
APA StyleScholl, J. L., Espinoza, A. I., Rai, W., Leedom, M., Baugh, L. A., Berg-Poppe, P., & Singh, A. (2021). Relationships between Freezing of Gait Severity and Cognitive Deficits in Parkinson’s Disease. Brain Sciences, 11(11), 1496. https://doi.org/10.3390/brainsci11111496