
Cerebrospinal Fluid IgM and Oligoclonal IgG Bands in Multiple Sclerosis: A Meta-Analysis of Prevalence and Prognosis

 , , ,
, , , {kind=link}
{kind=link}
Abstract
:1. Introduction
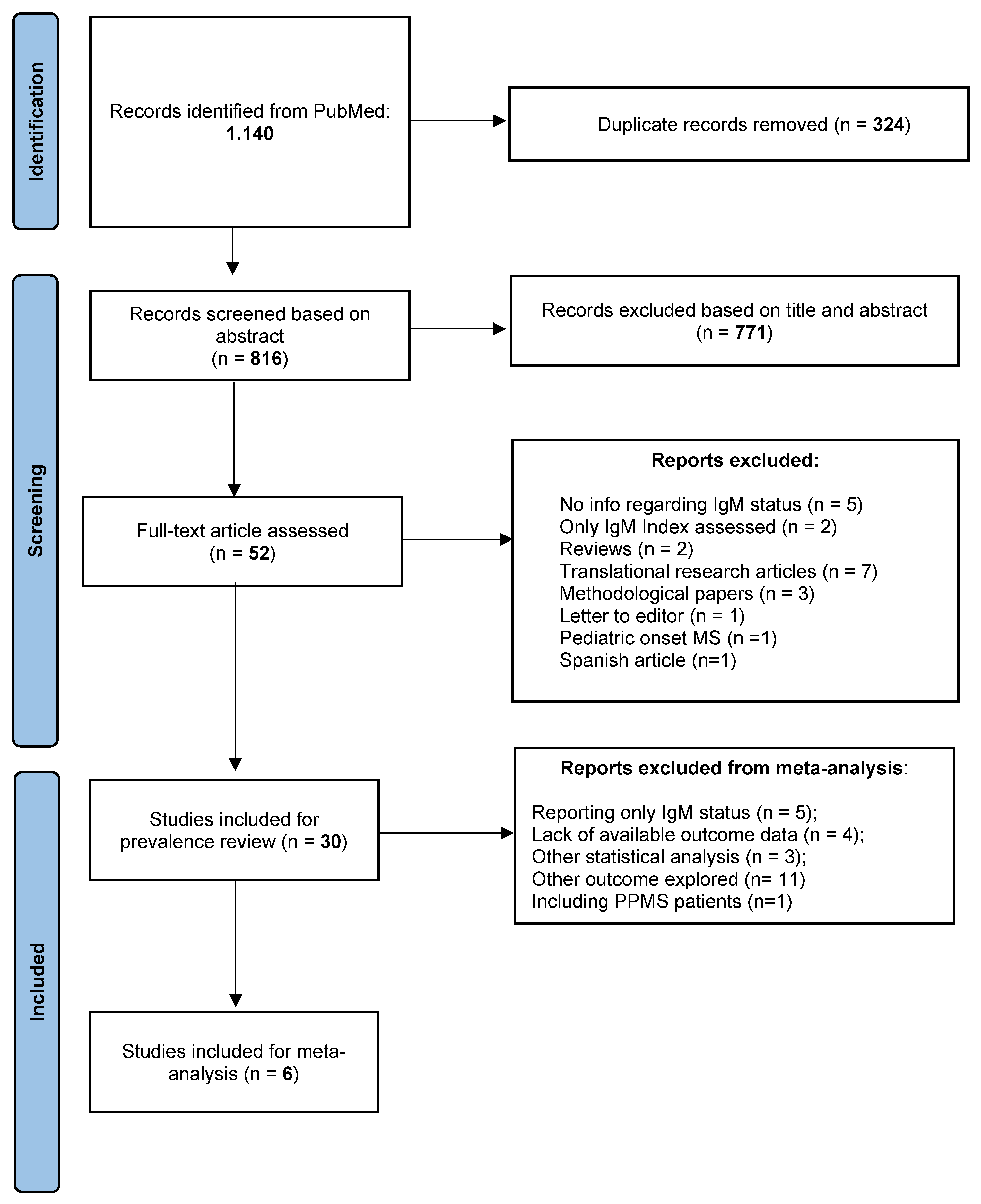
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Prevalence of ITMS in CIS, RRMS, and PPMS Patients
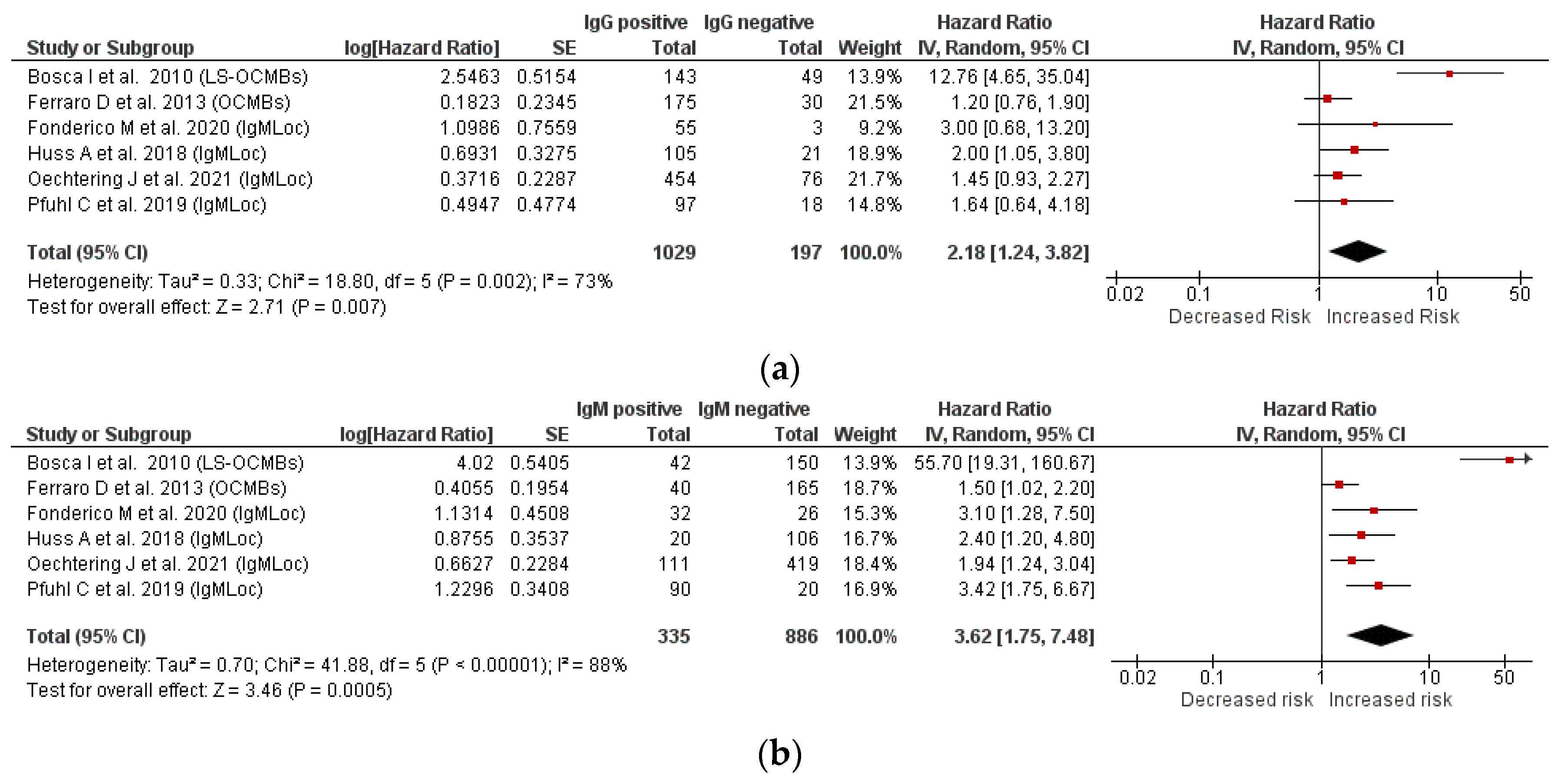
3.2. Relationship between IgM and IgG Status and Second Relapse
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- He, A.; Merkel, B.; Brown, W.; Ryerson, L.Z.; Kister, I.; Malpas, C.B.; Sharmin, S.; Horakova, D.; Havrdova, E.K.; Spelman, T.; et al. Timing of high-efficacy therapy for multiple sclerosis: A retrospective observational cohort study. Lancet Neurol. 2020, 19, 307–316. [Google Scholar] [CrossRef]
- Simpson, A.; Mowry, E.M.; Newsome, S.D. Early aggressive treatment approaches for multiple sclerosis. Curr. Treat. Options Neurol. 2021, 23, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Tur, C.; Moccia, M.; Barkhof, F.; Chataway, J.; Garriga, J.S.; Thompson, A.; Ciccarelli, O. Assessing treatment outcomes in multiple sclerosis trials and in the clinical setting. Nat. Rev. Neurol. 2018, 14, 75–93. [Google Scholar] [CrossRef] [PubMed]
- Ziemssen, T.; Derfuss, T.; de Stefano, N.; Giovannoni, G.; Palavra, F.; Tomic, D.; Vollmer, T.; Schippling, S. Optimizing treatment success in multiple sclerosis. J. Neurol. 2016, 263, 1053–1065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dobson, R.; Ramagopalan, S.; Davis, A.; Giovannoni, G. Cerebrospinal fluid oligoclonal bands in multiple sclerosis and clinically isolated syndromes: A meta-analysis of prevalence, prognosis and effect of latitude. J. Neurol. Neurosurg. Psychiatry 2013, 84, 909–914. [Google Scholar] [CrossRef] [PubMed]
- Tintore, M.; Rovira, À.; Rio, J.; Otero-Romero, S.; Arrambide, G.; Tur, C.; Comabella, M.; Nos, C.; Arevalo, M.J.; Negrotto, L.; et al. Defining high, medium and low impact prognostic factors for developing multiple sclerosis. Brain 2015, 138, 1863–1874. [Google Scholar] [CrossRef] [Green Version]
- Pfuhl, C.; Grittner, U.; Gieß, R.M.; Scheel, M.; Behrens, J.R.; Rasche, L.; Pache, F.C.; Wenzel, R.; Brandt, A.U.; Bellmann-Strobl, J.; et al. Intrathecal IgM production is a strong risk factor for early conversion to multiple sclerosis. Neurology 2019, 93, e1439–e1451. [Google Scholar] [CrossRef]
- Fonderico, M.; Biagioli, T.; Lanzilao, L.; Bellinvia, A.; Fratangelo, R.; Pastò, L.; Prestipino, E.; Razzolini, L.; Tudisco, L.; Ginestroni, A.; et al. Prognostic role of intrathecal IgM synthesis in multiple sclerosis: Results from a clinical series. Mult. Scler. J. 2021, 27, 198–207. [Google Scholar] [CrossRef]
- Sharief, M.K.; Thompson, E.J. Intrathecal immunoglobulin M synthesis in multiple sclerosis relationship with clinical and cerebrospinal fluid parameters. Brain 1991, 114, 181–195. [Google Scholar] [CrossRef]
- Villar, L.M.; Masjuan, J.; Gonzalez-Porqué, P.; Plaza, J.; Sábada, M.C.; Roldán, E.; Pootello, A.; Alvarez-Cermeño, J.C. Intrathecal IgM synthesis in neurologic diseases: Relationship with disability in MS. Neurology 2002, 58, 824–826. [Google Scholar] [CrossRef]
- Villar, L.M.; Masjuan, J.; Gonzalez-Porque, P.; Plaza, J.; Sadaba, M.C.; Roldan, E.; Bootello, A.; Alvarez-Cermeno, J.C. Intrathecal IgM synthesis predicts the onset of new relapses and a worse disease course in MS. Neurology 2002, 59, 555–559. [Google Scholar] [CrossRef]
- Villar, L.M.; Masjuan, J.; González-Porqué, P.; Plaza, J.; Sádaba, M.C.; Roldán, E.; Bootello, A.; Alvarez-Cermeño, J.C. Intrathecal IgM synthesis is a prognostic factor in multiple sclerosis. Ann. Neurol. 2002, 53, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Villar, L.M.; Casanova, B.; Ouamara, N.; Comabella, M.; Jalili, F.; Leppert, D.; de Andrés, C.; Izquierdo, G.; Arroyo, R.; Avşar, T.; et al. Immunoglobulin M oligoclonal bands: Biomarker of targetable inflammation in primary progressive multiple sclerosis. Ann. Neurol. 2014, 76, 231–240. [Google Scholar] [CrossRef]
- Schneider, R.; Euler, B.; Rauer, S. Intrathecal IgM-synthesis does not correlate with the risk of relapse in patients with a primary demyelinating event. Eur. J. Neurol. 2007, 14, 907–911. [Google Scholar] [CrossRef] [PubMed]
- Gasperi, C.; Salmen, A.; Antony, G.; Bayas, A.; Heesen, C.; Kümpfel, T.; Linker, R.A.; Paul, F.; Stangel, M.; Tackenberg, B.; et al. Association of intrathecal immunoglobulin G synthesis with disability worsening in multiple sclerosis. JAMA Neurol. 2019, 76, 841–849. [Google Scholar] [CrossRef]
- Frau, J.; Villar, L.M.; Sardu, C.; Secci, M.A.; Schirru, L.; Ferraro, D.; Coghe, G.; Lorefice, L.; Fenu, G.; Bedin, R.; et al. Intrathecal oligoclonal bands synthesis in multiple sclerosis: Is it always a prognostic factor? J. Neurol. 2017, 265, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Stauch, C.; Reiber, H.; Rauchenzauner, M.; Strasak, A.; Pohl, D.; Hanefeld, F.; Gärtner, J.; Rostásy, K. Intrathecal IgM synthesis in pediatric MS is not a negative prognostic marker of disease progression: Quantitative versus qualitative IgM analysis. Mult. Scler. J. 2010, 17, 327–334. [Google Scholar] [CrossRef]
- Annunziata, P.; Pluchino, S.; Martino, T.; Guazzi, G. High levels of cerebrospinal fluid IgM binding to myelin basic protein are associated with early benign course in multiple sclerosis. J. Neuroimmunol. 1997, 77, 128–133. [Google Scholar] [CrossRef]
- Freedman, M.S.; Thompson, E.J.; Deisenhammer, F.; Giovannoni, G.; Grimsley, G.; Keir, G.; Öhman, S.; Racke, M.K.; Sharief, M.; Sindic, C.J.M.; et al. Recommended standard of cerebrospinal fluid analysis in the diagnosis of multiple sclerosis. Arch. Neurol. 2005, 62, 865–870. [Google Scholar] [CrossRef] [Green Version]
- Link, H. Qualitative changes in immunoglobulin g in multiple sclerosis-cerebrospinal fluid. Acta Neurol. Scand. 2009, 43, 180–181. [Google Scholar] [CrossRef]
- Öhman, S.; Ernerudh, J.; Forsberg, P.; Henriksson, A.; von Schenck, H.; Vrethem, M. Comparison of seven formulae and isoelectrofocusing for determination of intrathecally produced IgG in neurological diseases. Ann. Clin. Biochem. Int. J. Lab. Med. 1992, 29, 405–410. [Google Scholar] [CrossRef]
- Reiber, H. Cerebrospinal fluid—Physiology, analysis and interpretation of protein patterns for diagnosis of neurological diseases. Mult. Scler. J. 1998, 4, 99–107. [Google Scholar] [CrossRef]
- Auer, M.; Hegen, H.; Zeileis, A.; Deisenhammer, F. Quantitation of intrathecal immunoglobulin synthesis—A new empirical formula. Eur. J. Neurol. 2016, 23, 713–721. [Google Scholar] [CrossRef]
- Reiber, H.; Peter, J.B. Cerebrospinal fluid analysis: Disease-related data patterns and evaluation programs. J. Neurol. Sci. 2001, 184, 101–122. [Google Scholar] [CrossRef]
- Giovannoni, G. Cerebrospinal Fluid Analysis; Elsevier: Amsterdam, The Netherlands, 2014; Volume 122, pp. 681–702. [Google Scholar]
- Espiño, M.; Abraira, V.; Arroyo, R.; Bau, L.; Cámara, C.; Campos-Ruiz, L.; Casanova, B.; Espejo, C.; Fernández, O.; García-Merino, A.; et al. Assessment of the reproducibility of oligoclonal IgM band detection for its application in daily clinical practice. Clin. Chim. Acta 2015, 438, 67–69. [Google Scholar] [CrossRef]
- Zeman, D.; Kušnierová, P.; Všianský, F.; Reguliová, K.; Škutová, M.; Woznicová, I.; Zapletalová, O.; Hradílek, P. Cerebrospinal fluid oligoclonal IgM test in routine practice: Comparison with quantitative assessment of intrathecal IgM synthesis. Clin. Chim. Acta 2020, 508, 137–145. [Google Scholar] [CrossRef]
- Cabrera, C.M.; Gosis, A. Semi-automated methodology for detection of IgM oligoclonal bands in cerebrospinal fluid and serum samples. J. Immunol. Methods 2020, 487, 112898. [Google Scholar] [CrossRef] [PubMed]
- Villar, L.M.; Sádaba, M.C.; Roldán, E.; Masjuan, J.; González-Porqué, P.; Villarrubia, N.; Espiño, M.; García-Trujillo, J.A.; Bootello, A.; Álvarez-Cermeño, J.C. Intrathecal synthesis of oligoclonal IgM against myelin lipids predicts an aggressive disease course in MS. J. Clin. Investig. 2005, 115, 187–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tejeda-Velarde, A.; Costa-Frossard, L.; de la Maza, S.S.; Carrasco, Á.; Espiño, M.; Picón, C.; Toboso, I.; Walo, P.E.; Lourido, D.; Muriel, A.; et al. Clinical usefulness of prognostic biomarkers in optic neuritis. Eur. J. Neurol. 2018, 25, 614–618. [Google Scholar] [CrossRef] [PubMed]
- Bosca, I.; Magraner, M.; Coret, F.; Alvarez-Cermeño, J.; Simó-Castelló, M.; Villar, L.M.; Casanova, B. The risk of relapse after a clinically isolated syndrome is related to the pattern of oligoclonal bands. J. Neuroimmunol. 2010, 226, 143–146. [Google Scholar] [CrossRef]
- Bosca, I.; Villar, L.M.; Coret, F.; Magraner, M.J.; Simó-Castelló, M.; Alvarez-Cermeño, J.C.; Casanova, B. Response to interferon in multiple sclerosis is related to lipid-specific oligoclonal IgM bands. Mult. Scler. J. 2010, 16, 810–815. [Google Scholar] [CrossRef] [PubMed]
- Berek, K.; Bsteh, G.; Auer, M.; di Pauli, F.; Zinganell, A.; Berger, T.; Deisenhammer, F.; Hegen, H. Cerebrospinal fluid findings in 541 patients with clinically isolated syndrome and multiple sclerosis: A monocentric study. Front. Immunol. 2021, 12, 675307. [Google Scholar] [CrossRef]
- Oechtering, J.; Schaedelin, S.; Benkert, P.; Müller, S.; Achtnichts, L.; Vehoff, J.; Disanto, G.; Findling, O.; Fischer-Barnicol, B.; Orleth, A.; et al. Intrathecal immunoglobulin M synthesis is an independent biomarker for higher disease activity and severity in multiple sclerosis. Ann. Neurol. 2021, 90, 477–489. [Google Scholar] [CrossRef]
- Gil-Perotin, S.; Castillo-Villalba, J.; Cubas-Nuñez, L.; Gasque, R.; Hervas, D.; Gomez-Mateu, J.; Alcala, C.; Pérez-Miralles, F.; Gascon, F.; Dominguez, J.A.; et al. Combined cerebrospinal fluid neurofilament light chain protein and chitinase-3 like-1 levels in defining disease course and prognosis in multiple sclerosis. Front. Neurol. 2019, 10, 1008. [Google Scholar] [CrossRef] [PubMed]
- Monreal, E.; de la Maza, S.S.; Costa-Frossard, L.; Walo-Delgado, P.; Zamora, J.; Fernández-Velasco, J.I.; Villarrubia, N.; Espiño, M.; Lourido, D.; Lapuente, P.; et al. Predicting aggressive multiple sclerosis with intrathecal IgM synthesis among patients with a clinically isolated syndrome. Neurol. Neuroimmunol. Neuroinflamm. 2021, 8, e1047. [Google Scholar] [CrossRef]
- Lucchinetti, C.F.; Brück, W.; Rodriguez, M.; Lassmann, H. Distinct patterns of multiple sclerosis pathology indicates heterogeneity in pathogenesis. Brain Pathol. 1996, 6, 259–274. [Google Scholar] [CrossRef]
- Metz, I.; Weigand, S.D.; Popescu, B.F.G.; Frischer, J.; Parisi, J.E.; Guo, Y.; Lassmann, H.; Brück, W.; Lucchinetti, C.F. Pathologic heterogeneity persists in early active multiple sclerosis lesions. Ann. Neurol. 2014, 75, 728–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stork, L.; Ellenberger, D.; Ruprecht, K.; Reindl, M.; Beißbarth, T.; Friede, T.; Kümpfel, T.; Gerdes, L.A.; Gloth, M.; Liman, T.; et al. Antibody signatures in patients with histopathologically defined multiple sclerosis patterns. Acta Neuropathol. 2020, 139, 547–564. [Google Scholar] [CrossRef] [Green Version]
- Muñoz, U.; Sebal, C.; Escudero, E.; Esiri, M.; Tzartos, J.; Sloan, C.; Sadaba, M.C. Main role of antibodies in demyelination and axonal damage in multiple sclerosis. Cell. Mol. Neurobiol. 2021, 1–19. [Google Scholar] [CrossRef]
- Boes, M. Role of natural and immune IgM antibodies in immune responses. Mol. Immunol. 2000, 37, 1141–1149. [Google Scholar] [CrossRef]
- Rosenbluth, J.; Schiff, R.; Liang, W.-L.; Dou, W. Antibody-mediated CNS demyelination II. Focal spinal cord lesions induced by implantation of an IgM antisulfatide-secreting hybridoma. J. Neurocytol. 2003, 32, 265–276. [Google Scholar] [CrossRef]
- Beltrán, E.; Obermeier, B.; Moser, M.; Coret, F.; Simó-Castelló, M.; Boscá, I.; Pérez-Miralles, F.; Villar, L.M.; Senel, M.; Tumani, H.; et al. Intrathecal somatic hypermutation of IgM in multiple sclerosis and neuroinflammation. Brain 2014, 137, 2703–2714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sospedra, M.; Martin, R. Immunology of multiple sclerosis. Annu. Rev. Immunol. 2005, 23, 683–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, M.J.; Tourtellotte, W.W. Temporal invariance and clonal uniformity of brain and cerebrospinal IgG, IgA, and IgM in multiple sclerosis. J. Exp. Med. 1986, 163, 41–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gastaldi, M.; Zardini, E.; Franciotta, D. An update on the use of cerebrospinal fluid analysis as a diagnostic tool in multiple sclerosis. Expert Rev. Mol. Diagn. 2016, 17, 31–46. [Google Scholar] [CrossRef]
- Álvarez-Cermeño, J.C.; Muñoz-Negrete, F.J.; Costa-Frossard, L.; de la Maza, S.S.; Villar, L.M.; Rebolleda, G. Intrathecal lipid-specific oligoclonal IgM synthesis associates with retinal axonal loss in multiple sclerosis. J. Neurol. Sci. 2016, 360, 41–44. [Google Scholar] [CrossRef]
- Jarius, S.; Lechner, C.; Wendel, E.M.; Baumann, M.; Breu, M.; Schimmel, M.; Karenfort, M.; Della Marina, A.; Merkenschlager, A.; Thiels, C.; et al. Cerebrospinal fluid findings in patients with myelin oligodendrocyte glycoprotein (MOG) antibodies. Part 2: Results from 108 lumbar punctures in 80 pediatric patients. J. Neuroinflamm. 2020, 17, 262. [Google Scholar] [CrossRef]
- Schlüter, M.; Oswald, E.; Winklmeier, S.; Meinl, I.; Havla, J.; Eichhorn, P.; Meinl, E.; Kümpfel, T. Effects of natalizumab therapy on intrathecal immunoglobulin G production indicate targeting of plasmablasts. Neurol. Neuroimmunol. Neuroinflamm. 2021, 8, e1030. [Google Scholar] [CrossRef]
- Larsson, D.; Åkerfeldt, T.; Carlson, K.; Burman, J. Intrathecal immunoglobulins and neurofilament light after autologous haematopoietic stem cell transplantation for multiple sclerosis. Mult. Scler. J. 2020, 26, 1351–1359. [Google Scholar] [CrossRef]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Comi, G.; Filippi, M.; Barkhof, F.; Durelli, L.; Edan, G.; Fernández, O.; Hartung, H.-P.; Seeldrayers, P.; Sorensen, P.S.; Rovaris, M.; et al. Effect of early interferon treatment on conversion to definite multiple sclerosis: A randomised study. Lancet 2001, 357, 1576–1582. [Google Scholar] [CrossRef]
- Kappos, L.; Polman, C.H.; Freedman, M.S.; Edan, G.; Hartung, H.P.; Miller, D.H.; Montalban, X.; Barkhof, F.; Bauer, L.; Jakobs, P.; et al. Treatment with interferon beta-1b delays conversion to clinically definite and McDonald MS in patients with clinically isolated syndromes. Neurology 2006, 67, 1242–1249. [Google Scholar] [CrossRef] [PubMed]
- Gout, O.; Bouchareine, A.; Moulignier, A.; Deschamps, R.; Papeix, C.; Gorochov, G.; Héran, F.; Bastuji-Garin, S. Prognostic value of cerebrospinal fluid analysis at the time of a first demyelinating event. Mult. Scler. J. 2010, 17, 164–172. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fonderico, M.; Portaccio, E.; Razzolini, L.; Pastò, L.; Bellinvia, A.; Addazio, I.; Betti, M.; Aprea, M.G.; Ballerini, C.; Biagioli, T.; et al. Cerebrospinal Fluid IgM and Oligoclonal IgG Bands in Multiple Sclerosis: A Meta-Analysis of Prevalence and Prognosis. Brain Sci. 2021, 11, 1444. https://doi.org/10.3390/brainsci11111444
Fonderico M, Portaccio E, Razzolini L, Pastò L, Bellinvia A, Addazio I, Betti M, Aprea MG, Ballerini C, Biagioli T, et al. Cerebrospinal Fluid IgM and Oligoclonal IgG Bands in Multiple Sclerosis: A Meta-Analysis of Prevalence and Prognosis. Brain Sciences. 2021; 11(11):1444. https://doi.org/10.3390/brainsci11111444
Chicago/Turabian StyleFonderico, Mattia, Emilio Portaccio, Lorenzo Razzolini, Luisa Pastò, Angelo Bellinvia, Ilaria Addazio, Matteo Betti, Maria Grazia Aprea, Clara Ballerini, Tiziana Biagioli, and et al. 2021. "Cerebrospinal Fluid IgM and Oligoclonal IgG Bands in Multiple Sclerosis: A Meta-Analysis of Prevalence and Prognosis" Brain Sciences 11, no. 11: 1444. https://doi.org/10.3390/brainsci11111444
APA StyleFonderico, M., Portaccio, E., Razzolini, L., Pastò, L., Bellinvia, A., Addazio, I., Betti, M., Aprea, M. G., Ballerini, C., Biagioli, T., & Amato, M. P. (2021). Cerebrospinal Fluid IgM and Oligoclonal IgG Bands in Multiple Sclerosis: A Meta-Analysis of Prevalence and Prognosis. Brain Sciences, 11(11), 1444. https://doi.org/10.3390/brainsci11111444