Memory Support System in Spanish: A Pilot Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Trial Registration
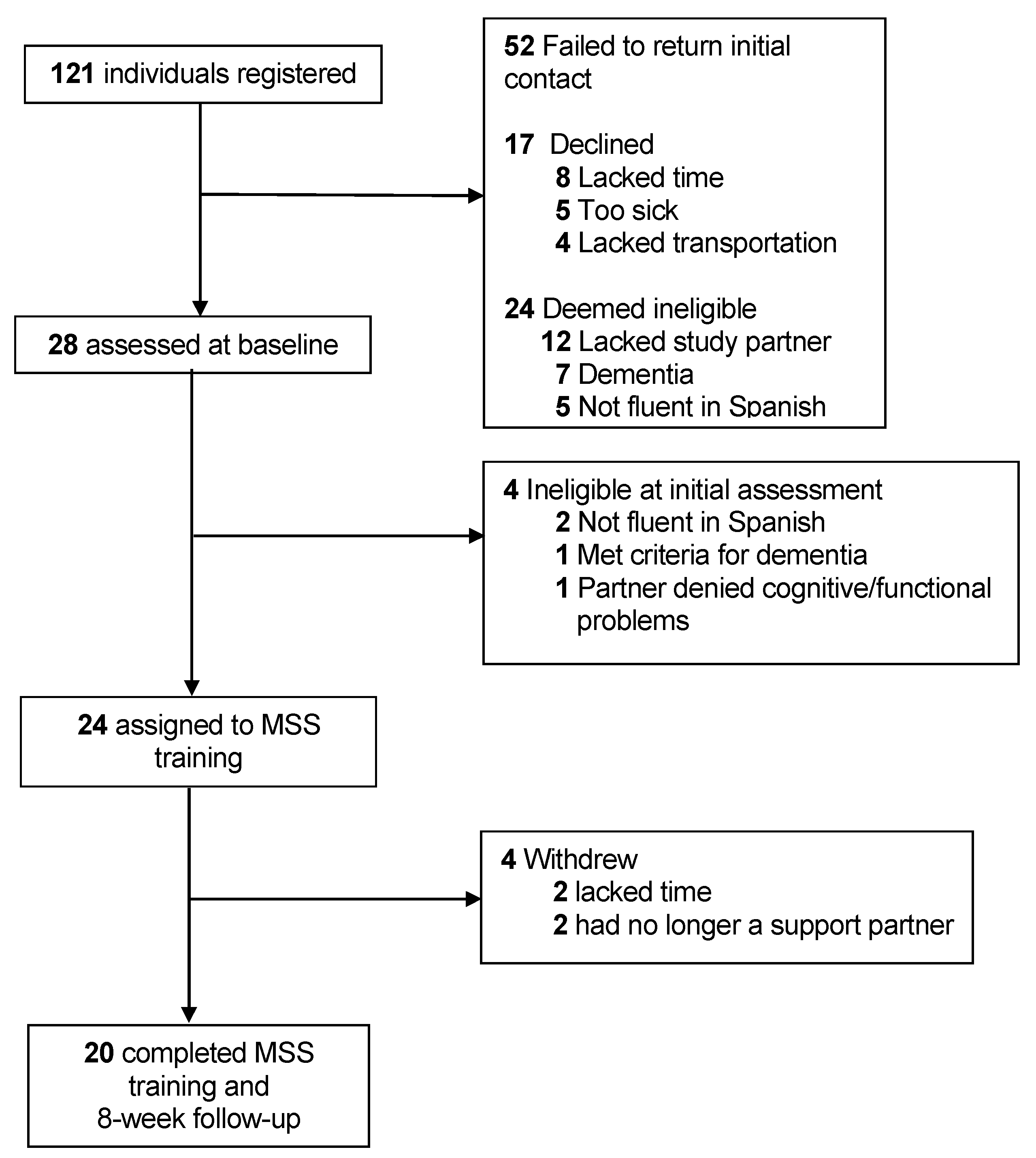
2.2. Participants
2.3. Procedure
2.3.1. Translation/Cultural Adaptation
2.3.2. MSS Training Paradigm
2.3.3. Treatment Adherence
2.3.4. Assessment Schedule and Outcome Measures
2.4. Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gunten, A.V. Subjective Memory Deficits in People with and without Dementia: Findings from the 10/66 Dementia Research Group Pilot Studies in Low- and Middle-Income Countries. J. Am. Geriatr. Soc. 2009, 57, 2118–2124. [Google Scholar] [CrossRef]
- Jessen, F.; Amariglio, R.E.; Buckley, R.F.; van der Flier, W.M.; Han, Y.; Molinuevo, J.L.; Rabin, L.; Rentz, D.M.; Rodriguez-Gomez, O.; Saykin, A.J.; et al. The characterisation of subjective cognitive decline. Lancet Neurol. 2020, 19, 271–278. [Google Scholar] [CrossRef]
- Petersen, R.C.; Lopez, O.; Armstrong, M.J.; Getchius, T.S.D.; Ganguli, M.; Gloss, D.; Gronseth, G.S.; Marson, D.; Pringsheim, T.; Day, G.S.; et al. Practice guideline update summary: Mild cognitive impairment. Neurology 2018, 90, 126–135. [Google Scholar] [CrossRef]
- Alzheimer’s Association. Alzheimer’s Association 2020 Facts and Figures Report. Available online: https://www.alz.org/media/Documents/alzheimers-facts-and-figures_1.pdf (accessed on 6 December 2019).
- Smart, C.M.; Karr, J.E.; Areshenkoff, C.N.; Rabin, L.A.; Hudon, C.; Gates, N.; Ali, J.I.; Arenaza-Urquijo, E.M.; Buckley, R.F.; Chetelat, G.; et al. Non-Pharmacologic Interventions for Older Adults with Subjective Cognitive Decline: Systematic Review, Meta-Analysis, and Preliminary Recommendations. Neuropsychol. Rev. 2017, 27, 245–257. [Google Scholar] [CrossRef] [PubMed]
- Chandler, M.J.; Locke, D.E.; Crook, J.E.; Fields, J.A.; Ball, C.T.; Phatak, V.S.; Dean, P.M.; Morris, M.; Smith, G.E. Comparative Effectiveness of Behavioral Interventions on Quality of Life for Older Adults With Mild Cognitive Impairment: A Randomized Clinical Trial. JAMA Netw. Open 2019, 2, e193016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenaway, M.C.; Hanna, S.M.; Lepore, S.W.; Smith, G.E. A behavioral rehabilitation intervention for amnestic mild cognitive impairment. Am. J. Alzheimer’s Dis. Other Demen. 2008, 23, 451–461. [Google Scholar] [CrossRef]
- Greenaway, M.C.; Duncan, N.L.; Smith, G.E. The memory support system for mild cognitive impairment: Randomized trial of a cognitive rehabilitation intervention. Int. J. Geriatr. Psychiatry 2013, 28, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Escobar, A.M.; Potowski, K. El español de Los Estados Unidos; Cambridge University Press: Cambridge, UK, 2015. [Google Scholar] [CrossRef]
- Hernández-Nieto, R.; Gutiérrez, M.C.; Moreno-Fernández, F. Hispanic Map of the United States 2017. 2017. Available online: https://doi.org/10.15427/OR035-11/2017EN (accessed on 6 December 2019).
- Roberts, A.W.; Ogunwole, S.U.; Blakeslee, L.; Rabe, M.A. The Population 65 Years and Older in the United States: 2016; American Community Survey Reports, ACS-38; US Census Bureau: Washington, DC, USA, 2018. [Google Scholar]
- Centers for Disease Control and Prevention. Hispanic Subjective Cognitive Decline in the United States. Available online: https://www.cdc.gov/aging/data/infographic/2017/hispanic-cognitive-decline.html (accessed on 6 December 2019).
- Alzheimer’s Association Hispanics and Latinos and Alzheimer’s Disease. Available online: https://www.alz.org/media/Documents/alzheimers-hispanics-latinos-r.pdf (accessed on 6 December 2019).
- Jessen, F.; Amariglio, R.E.; Van Boxtel, M.; Breteler, M.; Ceccaldi, M.; Chételat, G.; Dubois, B.; Dufouil, C.; Ellis, K.A.; Van Der Flier, W.M.; et al. A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer’s disease. Alzheimer’s Dement. 2014, 10, 844–852. [Google Scholar] [CrossRef] [Green Version]
- Petersen, R.C. Mild cognitive impairment as a diagnostic entity. J. Intern. Med. 2004, 256, 183–194. [Google Scholar] [CrossRef]
- Acevedo, A.; Krueger, K.R.; Navarro, E.; Ortiz, F.; Manly, J.J.; Padilla-Vélez, M.M.; Weintraub, S.; López, O.L.; Mungas, D. The Spanish translation and adaptation of the Uniform Data Set of the National Institute on Aging Alzheimer’s Disease Centers. Alzheimer Dis. Assoc. Disord. 2009, 23, 102–109. [Google Scholar] [CrossRef] [Green Version]
- Strutt, A.M.; Ayanegui, I.G.; Scott, B.M.; Mahoney, M.L.; York, M.K.; Montes, L.E.S.M. Influence of socio-demographic characteristics on DRS-2 performance in spanish-speaking older adults. Arch. Clin. Neuropsychol. 2012, 27, 545–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sohlberg, M.M.; Mateer, C.A. Training use of compensatory memory books: A three stage behavioral approach. J. Clin. Exp. Neuropsychol. 1989, 11, 871–891. [Google Scholar] [CrossRef] [PubMed]
- Zea, M.C.; Asner-Self, K.K.; Birman, D.; Buki, L.P. The abbreviated multidimensional acculturation scale: Empirical validation with two Latino/Latina samples. Cult. Divers. Ethn. Minor. Psychol. 2003, 9, 107–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sierra Sanjurjo, N.; Montañes, P.; Sierra Matamoros, F.A.; Burin, D. Estimating Intelligence in Spanish: Regression Equations with the Word Accentuation Test and Demographic Variables in Latin America. Appl. Neuropsychol. Adult 2015, 22, 252–261. [Google Scholar] [CrossRef]
- Losada, A.; de los Villareal, M.Á.; Nuevo, R.; Márquez-González, M.; Salazar, B.C.; Romero-Moreno, R.; Carrillo, A.L.; Fernández-Fernández, V. Cross-Cultural Confirmatory Factor Analysis of the CES-D in Spanish and Mexican Dementia Caregivers. Span. J. Psychol. 2012, 15, 783–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wisniewski, S.R.; Belle, S.H.; Marcus, S.M.; Burgio, L.D.; Coon, D.W.; Ory, M.G.; Burns, R.; Schulz, R. The Resources for Enhancing Alzheimer’s Caregiver Health (REACH): Project design and baseline characteristics. Psychol. Aging 2003, 18, 375–384. [Google Scholar] [CrossRef] [Green Version]
- Rosas-Carrasco, Ó.; Torres-Arreola, L.D.P.; Guerra-Silla, M.D.G.; Torres-Castro, S.; Gutiérrez-Robledo, L.M. Validación de la escala Quality of Life in Alzheimer’s Disease (QOL-AD) en pacientes mexicanos con demencia tipo Alzheimer, vascular y mixta. Rev. Neurol. 2010, 51, 72–80. [Google Scholar] [CrossRef]
- Lorig, K.; Stewart, A.; Ritter, P.; Gonzalez, V.; Laurent, D.; Lynch, J. Outcome Measures for Health Education and Other Health Care Interventions; SAGE Publications: Thousand Oaks, CA, USA, 1996; ISBN 0761900675. [Google Scholar]
- Russo, M.J.; Cohen, G.; Chrem Mendez, P.; Campos, J.; Martín, M.E.; Clarens, M.F.; Tapajoz, F.; Harris, P.; Sevlever, G.; Allegri, R.F. Utility of the Spanish version of the Everyday Cognition scale in the diagnosis of mild cognitive impairment and mild dementia in an older cohort from the Argentina-ADNI. Aging Clin. Exp. Res. 2018, 30, 1167–1176. [Google Scholar] [CrossRef]
- Zartman, A.L.; Hilsabeck, R.C.; Guarnaccia, C.A.; Houtz, A. The pillbox test: An ecological measure of executive functioning and estimate of medication management abilities. Arch. Clin. Neuropsychol. 2013, 28, 307–319. [Google Scholar] [CrossRef]
- Gort, A.M.; March, J.; Gómez, X.; De Miguel, M.; Mazarico, S.; Ballesté, J. Escala de Zarit reducida en cuidados paliativos. Med. Clin. 2005, 124, 651–653. [Google Scholar] [CrossRef]
- Siegel, J.S. Limited Language Proficiency and Its Consequences. In Demographic and Socioeconomic Basis of Ethnolinguistics; Springer: Cham, Switzerland, 2018. [Google Scholar]
- Amerian Psychiatric Association. Mental Health Disparities: Hispanics and Latinos. Available online: https://www.psychiatry.org/File%20Library/Psychiatrists/Cultural-Competency/Mental-Health-Disparities/Mental-Health-Facts-for-Hispanic-Latino.pdf (accessed on 6 December 2019).
- Gallagher-Thompson, D.; Solano, N.; Coon, D.; Arean, P. Recruitment and Retention of Latino Dementia Family Caregivers in Intervention Research: Issues to Face, Lessons to Learn. Gerontologist 2003, 43, 45–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristic | Participant with SCD (n = 20) Mean (SD) | Support Partner (n = 16) Mean (SD) |
|---|---|---|
| Age, years | 66.80 (10.29) | 49.44 (16.76) |
| Women, no. (%) | 16 (80) | 11 (68.75) |
| Education, years | 14.80 (3.59) | 15.94 (1.73) |
| Marital status, no. (%) | ||
| Married | 11 (55) | 13 (81.25) |
| Divorced/Separated | 4 (20) | 1 (6.25) |
| Widowed | 4 (20) | 0 (0) |
| Single/never married | 1 (5) | 2 (12.50) |
| Ethnicity, no. (%) | ||
| Hispanic/Latino | 20 (100) | 15 (93.75) |
| White | 0 (0) | 1 (6.25) |
| Primary language, no. (%) | ||
| Spanish | 19 (95) | 9 (56.25) |
| English | 0 (0) | 2 (12.50) |
| Both | 1 (5) | 5 (31,25) |
| Language proficiency a | ||
| Spanish | 6.26 (0.99) | 6.23 (1.13) |
| English | 3.95 (1.78) | 5.39 (1.84) |
| Acculturation b | ||
| American culture | 2.60 (0.68) | 3.03 (0.83) |
| Culture of origin | 3.30 (0.46) | 3.39 (0.44) |
| Test score results | ||
| WAT c | 34.20 (9.58) | 29.13 (11.22) |
| Participant’s memory functioning d | 4.8 (1.7) ^ | 4.19 (1.80) ^^ |
| MMSE e | 28.6 (1.4) | 29.56 (0.51) |
| ST-DRS-2 f | 133.2 (7.0) | |
| Place of birth, no. (%) | ||
| Puerto Rico | 9 (45) | 2 (12.50) |
| Colombia | 5 (25) | 1 (6.25) |
| Cuba | 3 (15) | 2 (12.50) |
| Argentina | 1 (5) | 3 (18.75) |
| Peru | 1 (5) | 1 (6.25) |
| Nicaragua | 1 (5) | 1 (6.25) |
| USA Mainland | 0 (0) | 6 (37.50) |
| Gross household annual income, no. (%) | ||
| <$25,000 | 6 (30) | 0 (0) |
| $25,000–49,999 | 6 (30) | 4 (25) |
| $50,000–74,999 | 3 (15) | 3 (18.75) |
| $75,000–99,999 | 2 (10) | 2 (12.50) |
| $100,000–149,000 | 1 (5) | 4 (25) |
| >$150,000 | 1 (5) | 1 (6.25) |
| Baseline (T1) Mean (SD) | Treatment End (T2) Mean (SD) | Follow-up (T3) Mean (SD) | T1–T2 Cohen’s d | T2–T3 Cohen’s d | T1–T3 Cohen’s d | |
|---|---|---|---|---|---|---|
| Participant with SCD | ||||||
| Adherence a | 1.20 (0.62) | 7.80 (1.47) | 7.45 (2.31) | −3.75 *** | 0.13 | −2.55 *** |
| Daily functioning | ||||||
| FAQ b | 2.65 (2.54) | 0.80 (1.40) | 1.10 (1.68) | 0.72 ** | −0.32 | 0.59 * |
| ECog Total c | 39.80 (13.64) | 35.80 (11.49) | 31.05 (7.89) | 0.28 | 0.54 * | 0.67 ** |
| ECog memory d | 13.65 (3.86) | 12.55 (4.39) | 11.50 (3.56) | 0.24 | 0.37 | 0.56 * |
| ECog planning e | 6.65 (2.08) | 6.60 (2.62) | 6.40 (2.04) | 0.02 | 0.08 | 0.13 |
| ECog organization f | 8.6 (3.22) | 7.30 (2.75) | 7.15 (2.03) | 0.66 ** | 0.07 | 0.61 * |
| ECog divided attention g | 7.30 (3.26) | 6.50 (2.40) | 6.00 (2.03) | 0.34 | 0.25 | 0.42 |
| Pillbox Test, no. (%) h | 10 (50) | 13 (65) | 13 (65) | |||
| Self-efficacy for memory i | 79.65 (14.17) | 82.35 (9.70) | 83.65 (6.50) | −0.29 | −0.21 | −0.40 |
| Quality of life j | 37.70 (5.62) | 39.30 (4.46) | 38.55 (5.48) | −0.44 | 0.19 | −0.18 |
| Depression k | 11.95 (12.38) | 7.85 (10.99) | 10.95 (11.34) | 0.99 *** | −0.52 * | 0.11 |
| Anxiety l | 20.10 (6.91) | 16.3 (5.78) | 18.5 (7.09) | 0.84 ** | −0.37 | 0.28 |
| Support partner | ||||||
| Caregiver burden m | 8.20 (6.83) | 6.80 (7.11) | 5.80 (6.68) | 0.39 | 0.3 | 0.65 ** |
| Quality of life j | 40.50 (6.58) | 40.56 (6.22) | 41.31 (5.85) | 41.31 (5.85) | −0.18 | −0.21 |
| Depression k | 8.06 (7.51) | 6.88 (7.24) | 6.06 (6.75) | 0.24 | 0.15 | 0.37 |
| Anxiety l | 19.50 (6.83) | 16.88 (6.35) | 17.5 (5.49) | 0.65 * | −0.11 | 0.32 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos, O.A.; Rios-Rosales, A.; Pedraza, O.; Bergeron, C.D.; Chandler, M. Memory Support System in Spanish: A Pilot Study. Brain Sci. 2021, 11, 1379. https://doi.org/10.3390/brainsci11111379
Santos OA, Rios-Rosales A, Pedraza O, Bergeron CD, Chandler M. Memory Support System in Spanish: A Pilot Study. Brain Sciences. 2021; 11(11):1379. https://doi.org/10.3390/brainsci11111379
Chicago/Turabian StyleSantos, Octavio A., Anapaula Rios-Rosales, Otto Pedraza, Caroline D. Bergeron, and Melanie Chandler. 2021. "Memory Support System in Spanish: A Pilot Study" Brain Sciences 11, no. 11: 1379. https://doi.org/10.3390/brainsci11111379
APA StyleSantos, O. A., Rios-Rosales, A., Pedraza, O., Bergeron, C. D., & Chandler, M. (2021). Memory Support System in Spanish: A Pilot Study. Brain Sciences, 11(11), 1379. https://doi.org/10.3390/brainsci11111379